
Exploring Acceptability Drivers of Oral Antibiotics in Children: Findings from an International Observational Study

 , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Objective and Setting
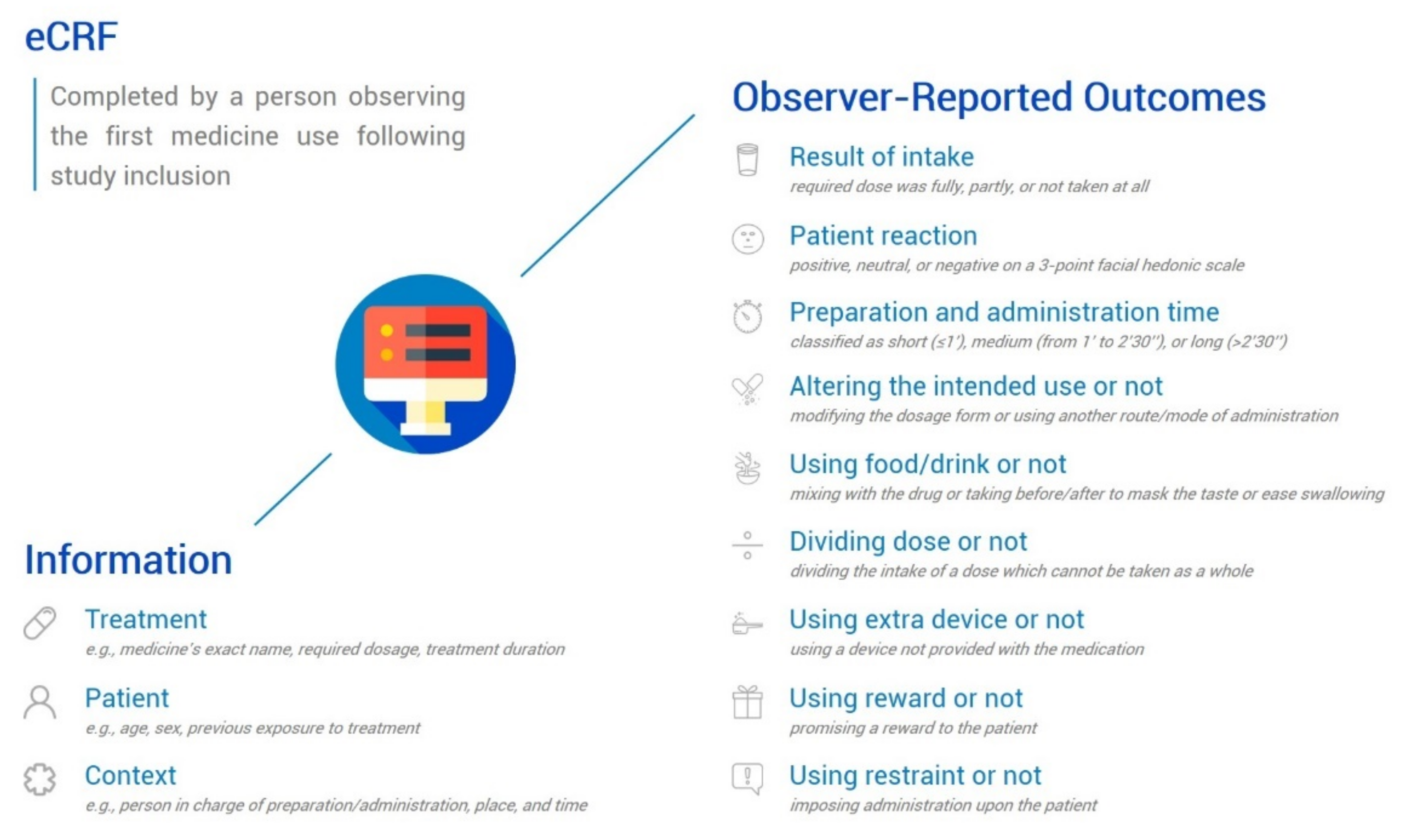
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Patients and Medicines
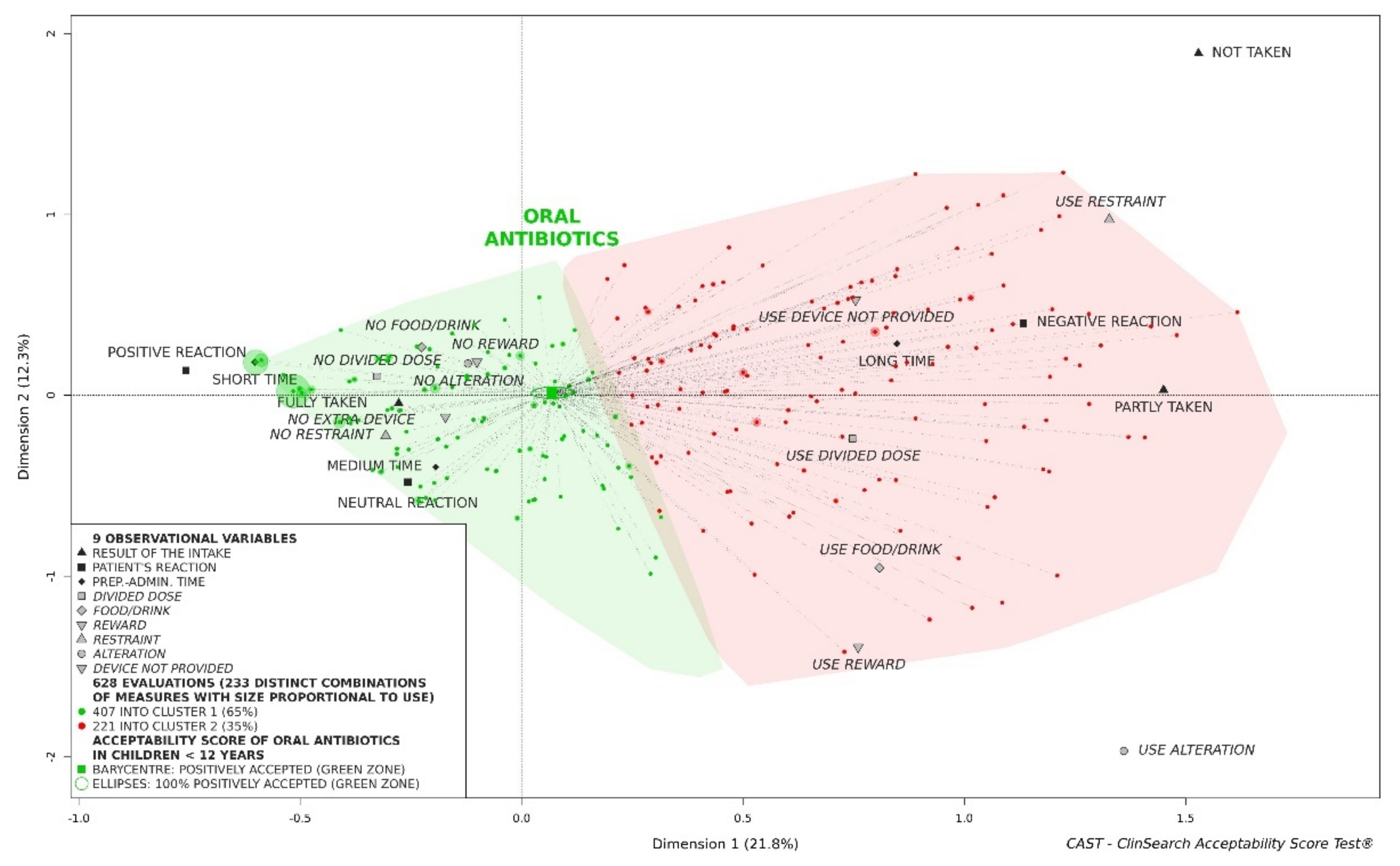
3.2. Acceptability Drivers
3.2.1. Influence of Age of Children on Acceptability of Oral Antibiotics
3.2.2. Influence of Dosage Form on Acceptability of Oral Antibiotics
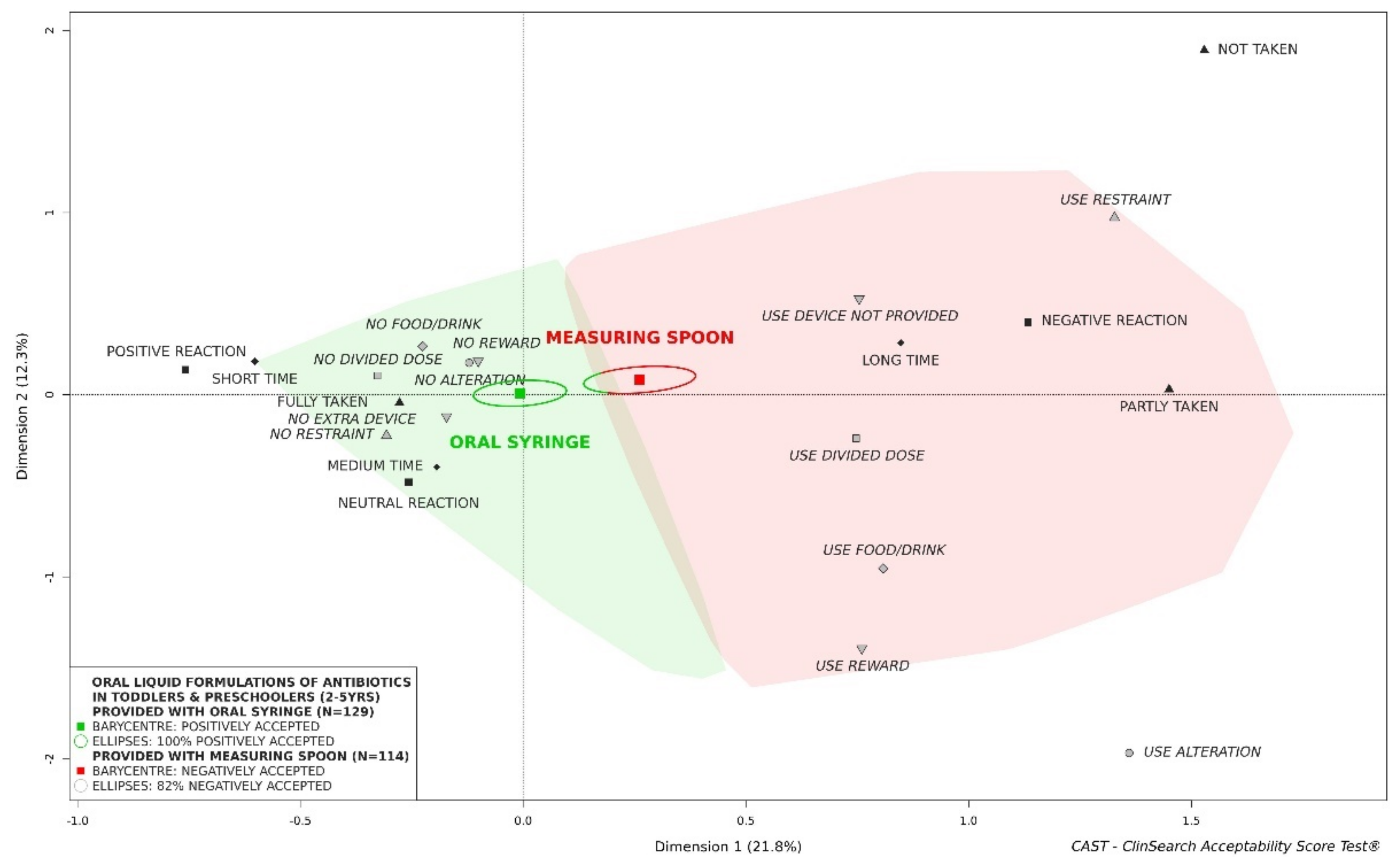
3.2.3. Influence of Administration Device Provided with the Medicine on Acceptability of Oral Liquid Formulations of Antibiotics
3.2.4. Influence of Administration Setting on Acceptability of Oral Liquid Formulations of Antibiotics
3.2.5. Influence of Previous Exposure to Treatment on Acceptability of Oral Liquid Formulations of Antibiotics
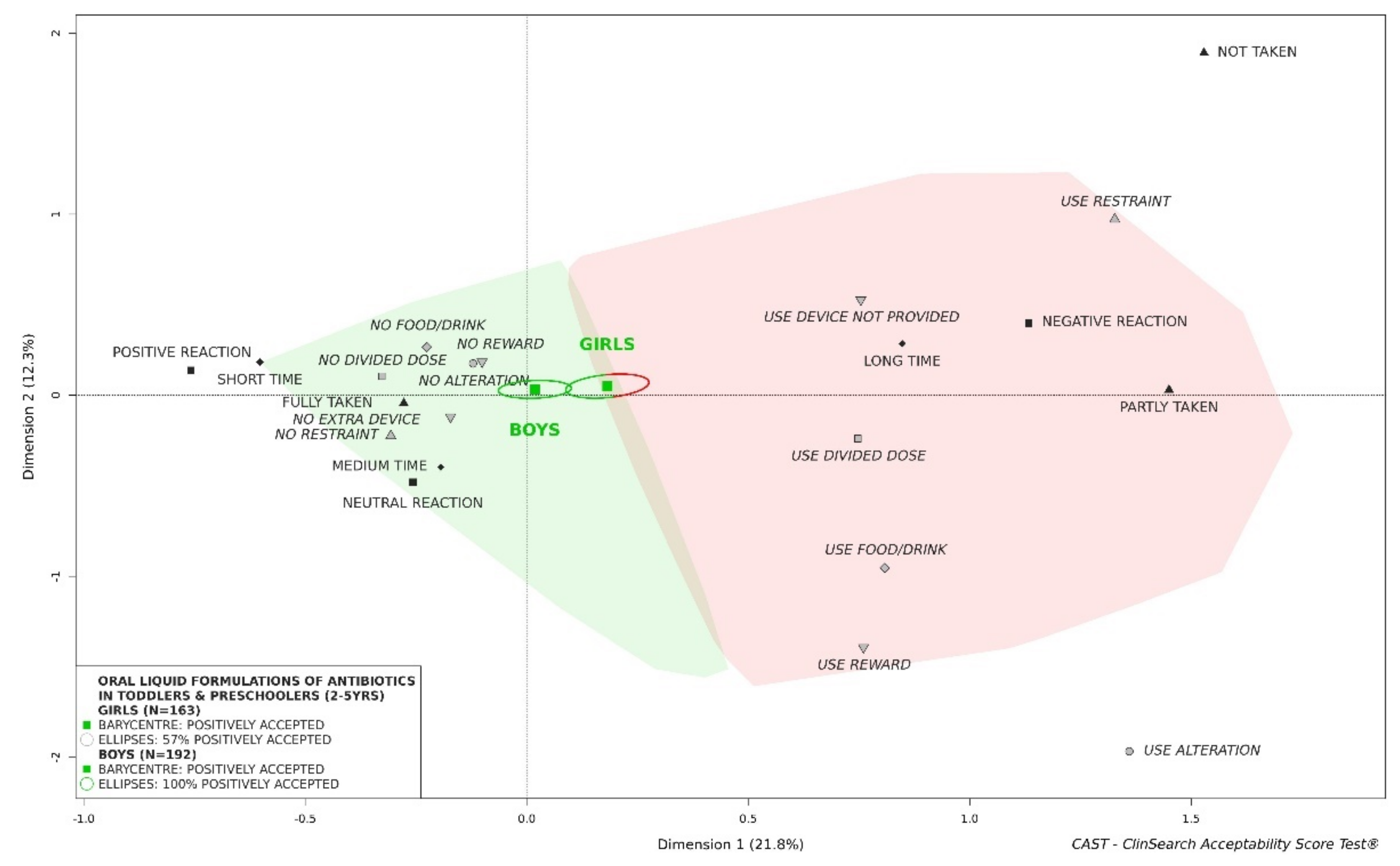
3.2.6. Influence of Sex of Children on Acceptability of Oral Liquid Formulations of Antibiotics
3.2.7. Influence of Flavor on Acceptability of Oral Liquid Formulations of Antibiotics
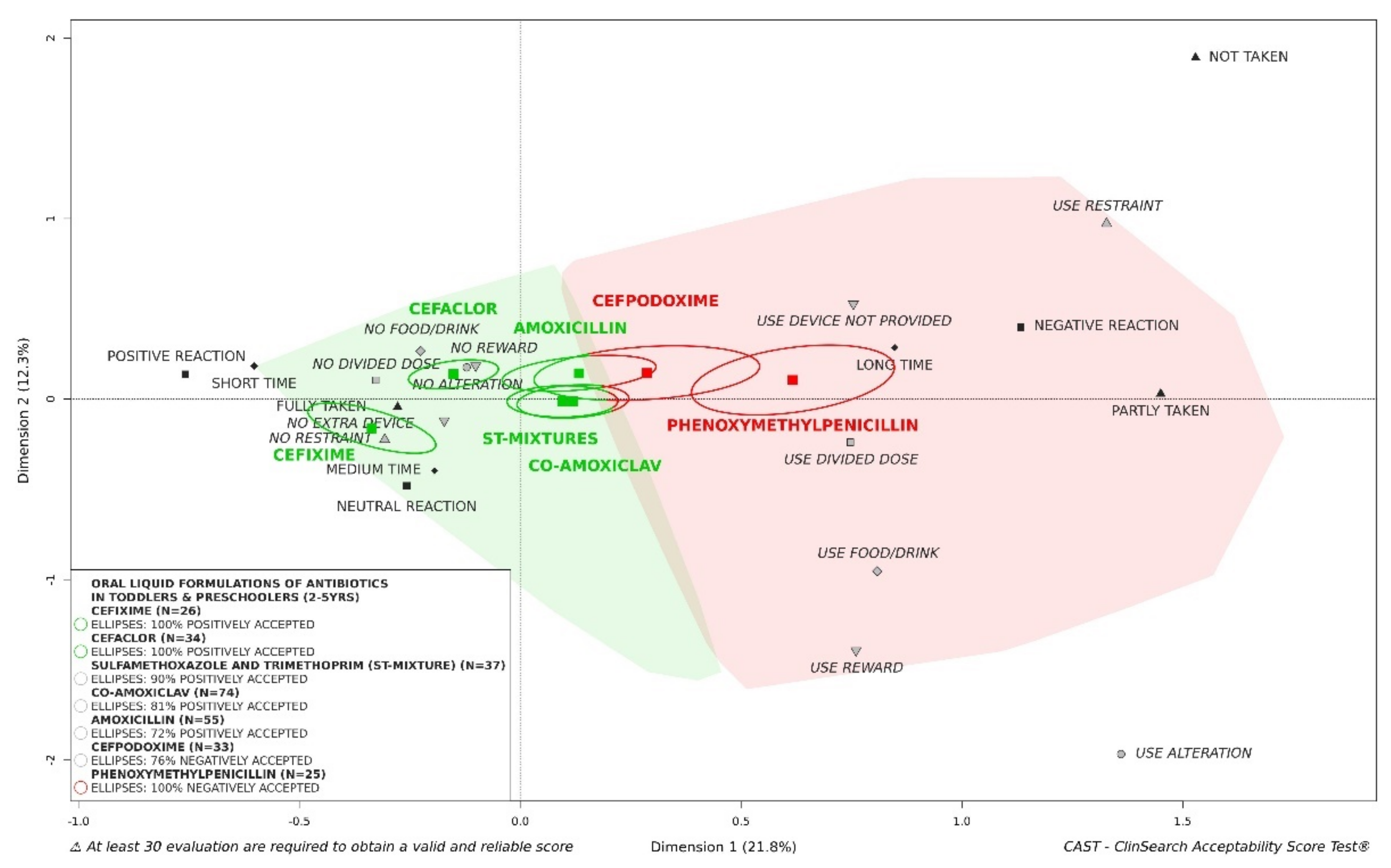
3.2.8. Influence of Active Pharmaceutical Ingredient on Acceptability of Oral Liquid Formulations of Antibiotics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan on Antimicrobial Resistance; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/feature-stories/ten-threats-to-global-health-in-2019 (accessed on 23 May 2021).
- Okeke, I.N.; Laxminarayan, R.; Bhutta, Z.A.; Duse, A.G.; Jenkins, P.; O’Brien, T.F.; Pablos-Mendez, A.; Klugman, K.P. Antimicrobial resistance in developing countries. Part I: Recent trends and current status. Lancet Infect. Dis. 2005, 5, 481–493. [Google Scholar] [CrossRef]
- Matteelli, A.; Roggi, A.; Carvalho, A.C. Extensively drug-resistant tuberculosis: Epidemiology and management. Clin. Epidemiol. 2014, 6, 111. [Google Scholar] [CrossRef] [Green Version]
- Ayukekbong, J.A.; Ntemgwa, M.; Atabe, A.N. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control 2017, 6, 47. [Google Scholar] [CrossRef]
- Cervino, G.; Cicciù, M.; Biondi, A.; Bocchieri, S.; Herford, A.S.; Laino, L.; Fiorillo, L. Antibiotic prophylaxis on third molar extraction: Systematic review of recent data. Antibiotics 2019, 8, 53. [Google Scholar] [CrossRef] [Green Version]
- Vaz, L.E.; Kleinman, K.P.; Raebel, M.A.; Nordin, J.D.; Lakoma, M.D.; Dutta-Linn, M.M.; Finkelstein, J.A. Recent trends in outpatient antibiotic use in children. Pediatrics 2014, 133, 375–385. [Google Scholar] [CrossRef] [Green Version]
- Youngster, I.; Avorn, J.; Belleudi, V.; Cantarutti, A.; Díez-Domingo, J.; Kirchmayer, U.; Park, B.-J.; Peiró, S.; Sanfélix-Gimeno, G.; Schröder, H. Antibiotic use in children—A cross-national analysis of 6 countries. J. Pediatr. 2017, 182, 239–244.e231. [Google Scholar] [CrossRef]
- Pottegård, A.; Broe, A.; Aabenhus, R.; Bjerrum, L.; Hallas, J.; Damkier, P. Use of antibiotics in children: A Danish nationwide drug utilization study. Pediatr. Infect. Dis. J. 2015, 34, e16–e22. [Google Scholar] [CrossRef] [Green Version]
- Hsia, Y.; Sharland, M.; Jackson, C.; Wong, I.C.; Magrini, N.; Bielicki, J.A. Consumption of oral antibiotic formulations for young children according to the WHO Access, Watch, Reserve (AWaRe) antibiotic groups: An analysis of sales data from 70 middle-income and high-income countries. Lancet Infect. Dis. 2019, 19, 67–75. [Google Scholar] [CrossRef]
- Iannelli, V.; Garbi, L. 30 Most Commonly Prescribed Pediatric Medications. Available online: https://www.verywellhealth.com/the-30-most-prescribed-drugs-in-pediatrics-2633435 (accessed on 17 September 2017).
- Hales, C.M.; Kit, B.K.; Gu, Q.; Ogden, C.L. Trends in prescription medication use among children and adolescents—United States, 1999–2014. JAMA 2018, 319, 2009–2020. [Google Scholar] [CrossRef] [PubMed]
- Matuz, M.; Benko, R.; Elseviers, M.; Hajdu, E.; Doro, P.; Viola, R.; Soos, G. Dosage form data used for estimating pediatric antibiotic use. Sci. Pharm. 2015, 83, 511–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Jackson, C.; Bielicki, J.; Ellis, S.; Hsia, Y.; Sharland, M. Estimates of global consumption of child-appropriate antibiotic formulations. Bull. World Health Organ. 2020, 98, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Wollner, A.; Lecuyer, A.; De La Rocque, F.; Sedletzki, G.; Derkx, V.; Boucherat, M.; Elbez, A.; Gelbert-Baudino, N.; Levy, C.; Corrard, F.; et al. Acceptability, compliance and schedule of administration of oral antibiotics in outpatient children. Arch. Pediatr. 2011, 18, 611–616. [Google Scholar] [CrossRef] [PubMed]
- European Medicine Agency. Guideline on Pharmaceutical Development of Medicines for Paediatric Use; EMA/CHMP/QWP/805880/2012 Rev. 2; EMA: London, UK, 2013. [Google Scholar]
- Sjövall, J.; Fogh, A.; Huitfeldt, B.; Karlsson, G.; Nylen, O. Methods for evaluating the taste of paediatric formulations in children: A comparison between the facial hedonic method and the patients’ own spontaneous verbal judgement. Eur. J. Pediatr. 1984, 141, 243–247. [Google Scholar] [CrossRef]
- Uhari, M.; Eskelinen, L.; Jokisalo, J. Acceptance of antibiotic mixtures by infants and children. Eur. J. Clin. Pharm. 1986, 30, 503–504. [Google Scholar] [CrossRef]
- Jahnsen, T.; Thorn, P. An acceptability study of two pivampicillin mixtures in children in general practice. Scand. J. Prim. Health Care 1987, 5, 241–243. [Google Scholar] [CrossRef]
- El-Chaar, G.M.; Mardy, G.; Wehlou, K.; Rubin, L.G. Randomized, double blind comparison of brand and generic antibiotic suspensions: II. A study of taste and compliance in children. Pediatr. Infect. Dis. J. 1996, 15, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; de La Rocque, F.; Lecuyer, A.; Wollner, C.; Bodin, M.J.; Wollner, A. Study of the acceptability of antibiotic syrups, suspensions, and oral solutions prescribed to pediatric outpatients. Eur. J. Pediatr. 2009, 168, 851–857. [Google Scholar] [CrossRef] [PubMed]
- Bagger-Sjoback, D.; Bondesson, G. Taste evaluation and compliance of two paediatric formulations of phenoxymethylpenicillin in children. Scand. J. Prim. Health Care 1989, 7, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Baguley, D.; Lim, E.; Bevan, A.; Pallet, A.; Faust, S.N. Prescribing for children-taste and palatability affect adherence to antibiotics: A review. Arch. Dis. Child. 2012, 97, 293–297. [Google Scholar] [CrossRef]
- Tuleu, C.; Hughes, D.A.; Clapham, D.; Vallet, T.; Ruiz, F. Acceptability of generic versus innovator oral medicines: Not only a matter of taste. Drug Discov. Today 2020, 26, 329–343. [Google Scholar] [CrossRef]
- Ruiz, F.; Vallet, T.; Pense-Lheritier, A.M.; Aoussat, A. Standardized method to assess medicines’ acceptability: Focus on paediatric population. J. Pharm. Pharmacol. 2017, 69, 406–416. [Google Scholar] [CrossRef]
- Vallet, T.; Ruiz, F.; Lavarde, M.; Pense-Lheritier, A.M.; Aoussat, A. Standardized evaluation of medicine acceptability in paediatric population: Reliability of a model. J. Pharm. Pharmacol. 2018, 70, 42–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, F.; Vallet, T.; Dufay Wojcicki, A.; Belissa, É.; Fontan, J.-E.; de Pontual, L.; Nathanson, S.; Chevallier, A.; Laribe-Caget, S.; Boudy, V. Dosage form suitability in vulnerable populations: A focus on paracetamol acceptability from infants to centenarians. PLoS ONE 2019, 14, e0221261. [Google Scholar] [CrossRef]
- Vallet, T.; Elhamdaoui, O.; Berraho, A.; Cherkaoui, L.O.; Kriouile, Y.; Mahraoui, C.; Mouane, N.; Pense-Lheritier, A.-M.; Ruiz, F.; Bensouda, Y. Medicines Acceptability in Hospitalized Children: An Ongoing Need for Age-Appropriate Formulations. Pharmaceutics 2020, 12, 766. [Google Scholar] [CrossRef]
- Emeryk, A.; Vallet, T.; Wawryk-Gawda, E.; Jędrzejewski, A.; Durmont, F.; Ruiz, F. Acceptability of a Sublingual Drug Formulation for Respiratory Tract Infections in Children Aged 3 to 5 Years. Pharmaceutics 2021, 13, 294. [Google Scholar] [CrossRef]
- Saito, J.; Miyamoto, S.; Yamada, M.; Yamatani, A.; Ruiz, F.; Vallet, T. Adherence and Acceptability of an Oral Antibiotic Used for the Prevention of Pediatric Urinary Tract Infection in Japan. Pharmaceutics 2021, 13, 345. [Google Scholar] [CrossRef]
- Le, S.; Josse, J.; Husson, F. FactoMineR: An R package for multivariate analysis. J. Stat. Softw. 2008, 25, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Josse, J.; Husson, F. missMDA: A package for handling missing values in multivariate data analysis. J. Stat. Softw. 2016, 70, 1–31. [Google Scholar] [CrossRef]
- Vallet, T. Conception D’un Outil D’évaluation de L’acceptabilité des Médicaments; Génie Industriel École Nationale Supérieure d’Arts et Métiers (ENSAM); Arts et Métiers ParisTech: Paris, France, 2017. [Google Scholar]
- Dovey, T.M.; Staples, P.A.; Gibson, E.L.; Halford, J.C. Food neophobia and ‘picky/fussy’eating in children: A review. Appetite 2008, 50, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Belissa, E.; Vallet, T.; Laribe-Caget, S.; Chevallier, A.; Chedhomme, F.X.; Abdallah, F.; Bachalat, N.; Belbachir, S.A.; Boulaich, I.; Bloch, V.; et al. Acceptability of oral liquid pharmaceutical products in older adults: Palatability and swallowability issues. BMC Geriatr. 2019, 19, 344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruiz, F.; Keeley, A.; Léglise, P.; Tuleu, C.; Lachuer, C.; Rwabihama, J.-P.; Bachalat, N.; Boulaich, I.; Abdallah, F.; Rabus, M.; et al. Sex Differences in Medicine Acceptability: A New Factor to Be Considered in Medicine Formulation. Pharmaceutics 2019, 11, 368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Riet-Nales, D.A.; Ferreira, J.A.; Schobben, A.F.; de Neef, B.J.; Egberts, T.C.; Rademaker, C.M. Methods of administering oral formulations and child acceptability. Int. J. Pharm. 2015, 491, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Walsh, J.; Math, M.-C.; Breitkreutz, J.; Zerback, T.; Wachtel, H.; Initiative, E.P.F. Devices for oral and respiratory paediatric medicines: What do healthcare professionals think? Int. J. Pharm. 2015, 492, 304–315. [Google Scholar] [CrossRef]
- Walsh, J.; Bickmann, D.; Breitkreutz, J.; Chariot-Goulet, M.; Initiative, E.P.F. Delivery devices for the administration of paediatric formulations: Overview of current practice, challenges and recent developments. Int. J. Pharm. 2011, 415, 221–231. [Google Scholar] [CrossRef]
- Toscani, M.; Drehobl, M.; Freed, J.; Stool, S. A multicenter, randomized, comparative assessment in healthy pediatric volunteers of the palatability of oral antibiotics effective in the therapy of otitis media. Curr. Ther. Res. 2000, 61, 278–285. [Google Scholar] [CrossRef]
- Angelilli, M.L.; Toscani, M.; Matsui, D.M.; Rieder, M.J. Palatability of oral antibiotics among children in an urban primary care center. Arch. Pediatr. Adolesc. Med. 2000, 154, 267–270. [Google Scholar] [CrossRef] [Green Version]
- Gooch, W.; Philips, A.; Rhoades, R.; Rosenberg, R.; Schaten, R.; Starobin, S. Comparison of the efficacy, safety and acceptability of cefixime and amoxicillin/clavulanate in acute otitis media. Pediatr. Infect. Dis. J. 1997, 16, S21–S24. [Google Scholar] [CrossRef]
- Dagan, R.; Shvartzman, P.; Liss, Z. Variation in acceptance of common oral antibiotic suspensions. Pediatr. Infect. Dis. J. 1994, 13, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Pichichero, M.; Aronovitz, G.; Gooch, W.M.; McLinn, S.; Maddern, B.; Johnson, C.; Darden, P. Comparison of cefuroxime axetil, cefaclor, and amoxicillin-clavulanate potassium suspensions in acute otitis media in infants and children. South. Med. J. 1990, 83, 1174–1177. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patient Age | Statistical Test | ||
|---|---|---|---|---|
| Newborns and Infants 0–1 Year (n = 92) | Toddlers and Preschoolers 2–5 Years (n = 372) | Grade-Schoolers 6–11 Years (n = 164) | ||
| Sex | χ2 b: p = 0.77 | |||
| Female | 48 (53) a | 199 (54) | 79 (50) | |
| Male | 43 (47) | 171 (46) | 78 (50) | |
| missing data | 1 | 2 | 7 | |
| Treatment exposure | χ2: p < 0.001 | |||
| Previous exposure | 20 (22) | 155 (42) | 88 (54) | |
| First exposure | 72 (78) | 217 (58) | 76 (46) | |
| Setting | χ2: p = 0.007 | |||
| Community | 31 (34) | 160 (43) | 48 (29) | |
| Hospital | 61 (66) | 212 (57) | 116 (71) | |
| Country | χ2: p < 0.001 | |||
| France | 32 (35) | 135 (36) | 39 (24) | |
| Morocco | 23 (25) | 68 (18) | 42 (26) | |
| Japan | 18 (20) | 71 (19) | 36 (22) | |
| Norway | 2 (2) | 36 (10) | 12 (7) | |
| India | 2 (2) | 25 (7) | 23 (14) | |
| Germany | 10 (11) | 21 (6) | 3 (2) | |
| England | 5 (5) | 16 (4) | 9 (5) | |
| 5th level (chemical substance) of the Anatomical Therapeutic Chemical (ATC) classification system | χ2: p < 0.001 | |||
| Amoxicillin and clavulanic acid (co-amoxiclav) | 20 (22) | 75 (20) | 25 (15) | |
| Amoxicillin | 17 (18) | 57 (15) | 20 (12) | |
| Sulfamethoxazole and trimethoprim (ST-mixture) | 19 (21) | 41 (11) | 25 (15) | |
| Cefpodoxime | 7 (8) | 36 (10) | 14 (9) | |
| Cefaclor | 2 (2) | 34 (9) | 17 (10) | |
| Josamycin | 20 (22) | 23 (6) | 6 (4) | |
| Cefixime | 3 (3) | 26 (7) | 15 (9) | |
| Fusidic acid | 3 (3) | 21 (6) | 16 (10) | |
| Phenoxymethylpenicillin | 0 (0) | 25 (7) | 9 (5) | |
| Other (<5%) | 1 (1) | 34 (9) | 17 (10) | |
| Pharmaceutical form categories | χ2: p < 0.001 | |||
| Oral liquids c | 92 (100) | 357 (96) | 137 (84) | |
| Solid oral dosage form | 0 (0) | 15 (4) | 27 (16) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallet, T.; Bensouda, Y.; Saito, J.; Mathiesen, L.; Pokharkar, V.; Klingmann, V.; Peak, M.; Elhamdaoui, O.; Yamatani, A.; Ivanovic, I.; et al. Exploring Acceptability Drivers of Oral Antibiotics in Children: Findings from an International Observational Study. Pharmaceutics 2021, 13, 1721. https://doi.org/10.3390/pharmaceutics13101721
Vallet T, Bensouda Y, Saito J, Mathiesen L, Pokharkar V, Klingmann V, Peak M, Elhamdaoui O, Yamatani A, Ivanovic I, et al. Exploring Acceptability Drivers of Oral Antibiotics in Children: Findings from an International Observational Study. Pharmaceutics. 2021; 13(10):1721. https://doi.org/10.3390/pharmaceutics13101721
Chicago/Turabian StyleVallet, Thibault, Yahya Bensouda, Jumpei Saito, Liv Mathiesen, Varsha Pokharkar, Viviane Klingmann, Matthew Peak, Omar Elhamdaoui, Akimasa Yamatani, Ivana Ivanovic, and et al. 2021. "Exploring Acceptability Drivers of Oral Antibiotics in Children: Findings from an International Observational Study" Pharmaceutics 13, no. 10: 1721. https://doi.org/10.3390/pharmaceutics13101721