
Posterior Segment Ophthalmic Drug Delivery: Role of Muco-Adhesion with a Special Focus on Chitosan

 , , and
, , and
Abstract
:1. Introduction
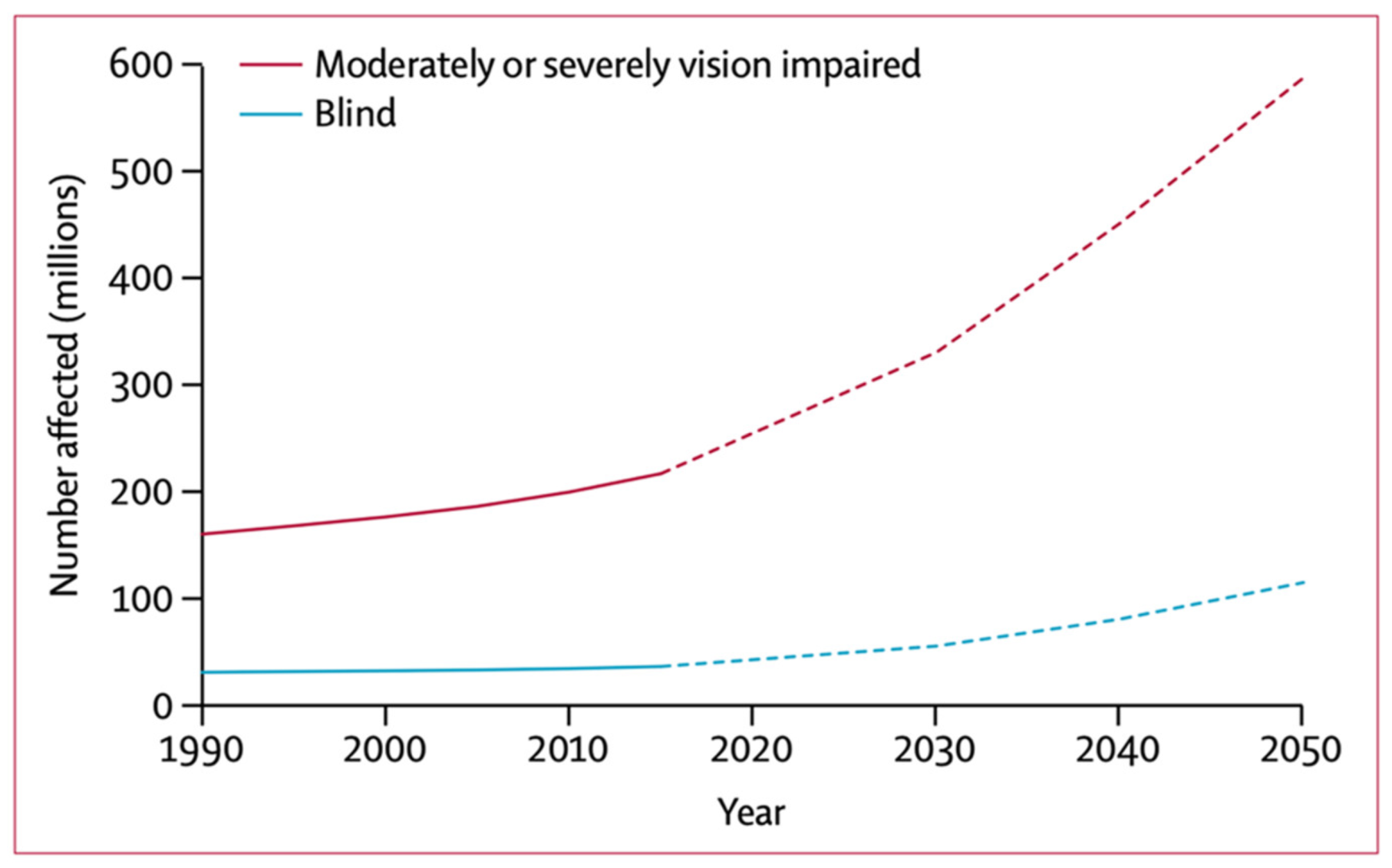
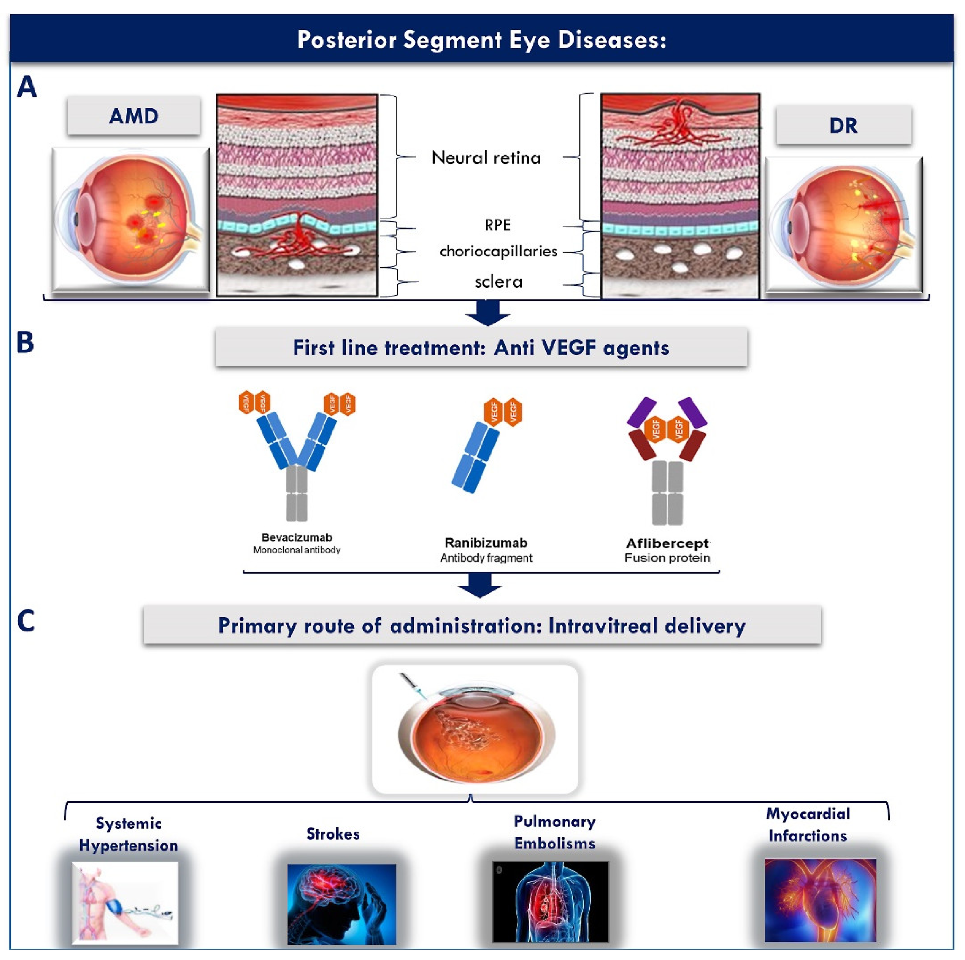
2. Posterior Segment Eye Diseases: A Global Health Crisis
2.1. Posterior Segment Eye Diseases
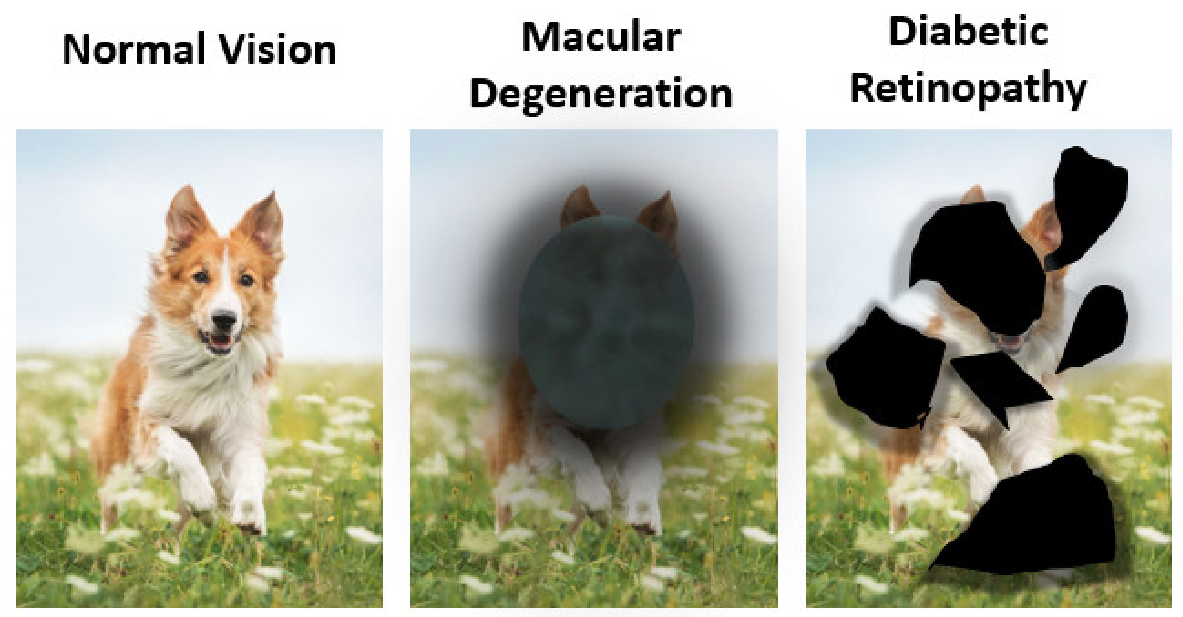
2.1.1. Age Related Macular Degeneration (AMD)
2.1.2. Diabetic Retinopathy (DR)
2.2. Conventional Therapies and Their Drawbacks
2.2.1. Anti-VEGF Agents
2.2.2. Corticosteroids
3. Topical Drug Delivery to the Posterior Eye Segment
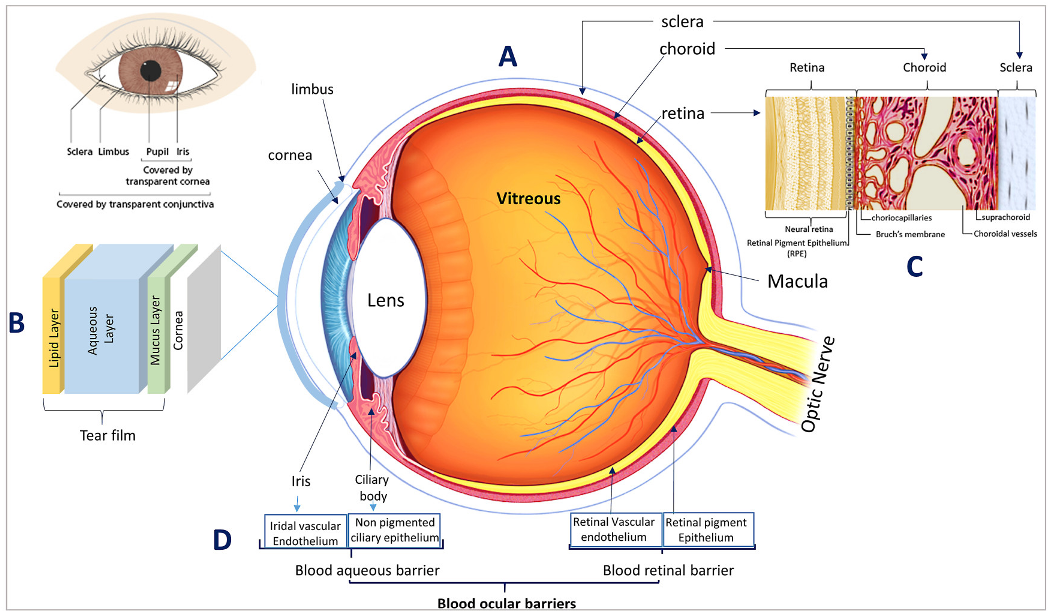
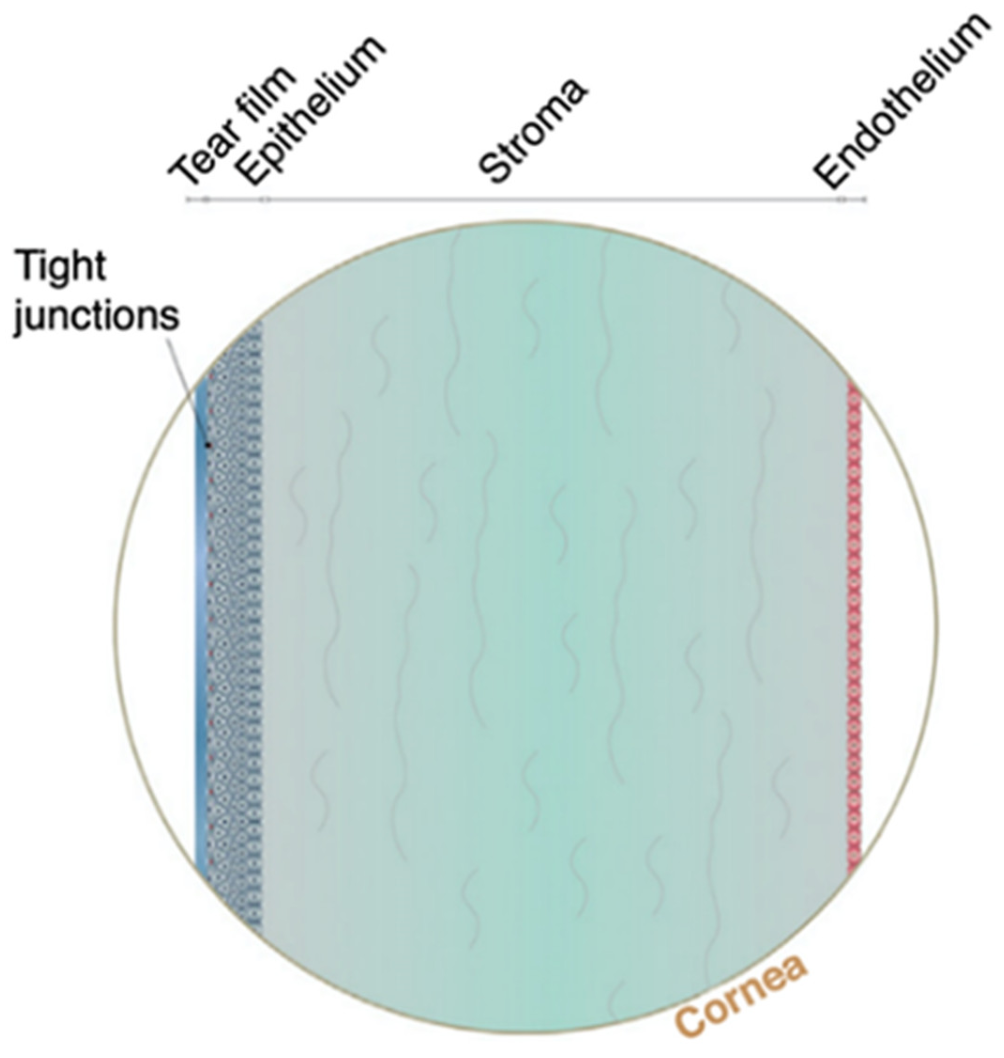
3.1. Eye Anatomy and Hurdles of Topical Drug Delivery to the Posterior Eye Segment
3.2. Pathways of Topical Drug Absorption into the Posterior Eye Segment
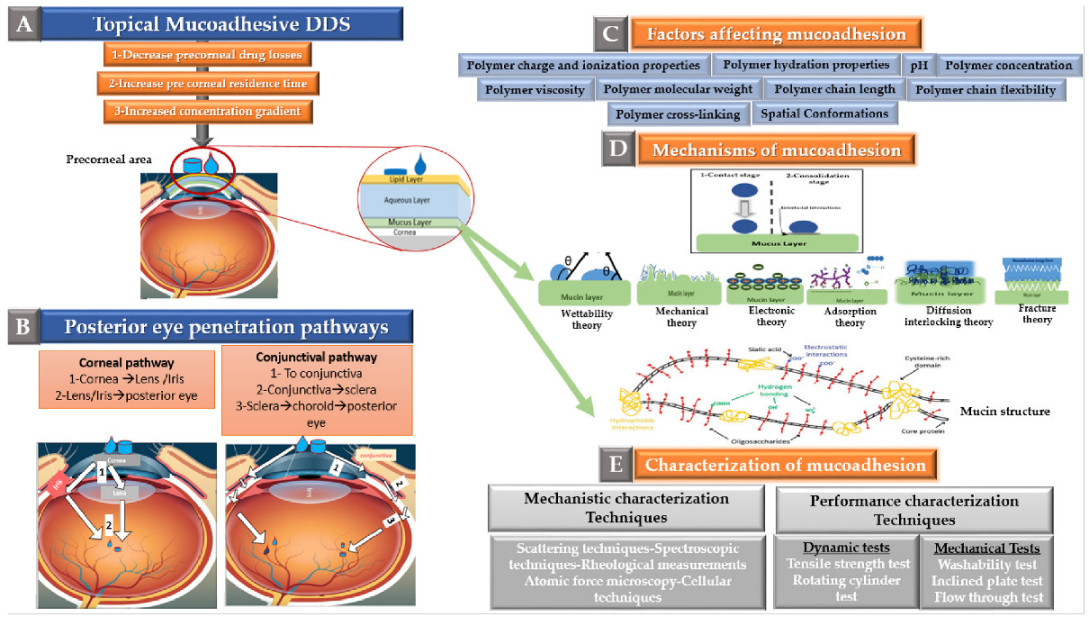
- The corneal pathway: The corneal pathway has been reported to be the primary route of hydrophobic drugs absorption to the posterior eye segment [95]. Following corneal absorption, drugs can then reach the posterior segment using one of two ways as follows:
- The drugs absorbed through the cornea can also undergo lateral diffusion to the sclera, from where they can be distributed to the various ocular tissues including the posterior segment tissues [15].
- The conjunctival pathway: This pathway is reported to be the major pathway for the absorption of hydrophilic drugs (e.g., Inulin) to the posterior eye segment tissues [95]. In this pathway, the anterior chamber is bypassed and drug distribution occurs predominantly in the uveal tract and vitreous humour. Through the conjunctival pathway, drugs are reported to access the posterior eye tissues through one of the following:
- Diffusion across the conjunctiva, choroid, and sclera to reach the retina (this is the major pathway) [15].
- Conjunctival absorbed drugs can also diffuse laterally to the iris, cornea, and ciliary body, i.e., diffuse to the anterior chamber with other intraocular tissue [15].
- The conjunctival blood vessels can drain drugs to the systemic circulation, from where they distribute to various body organs, including the retina [15].

4. Mucoadhesion for Posterior Eye Segment Delivery
4.1. Theory of Mucoadhesion
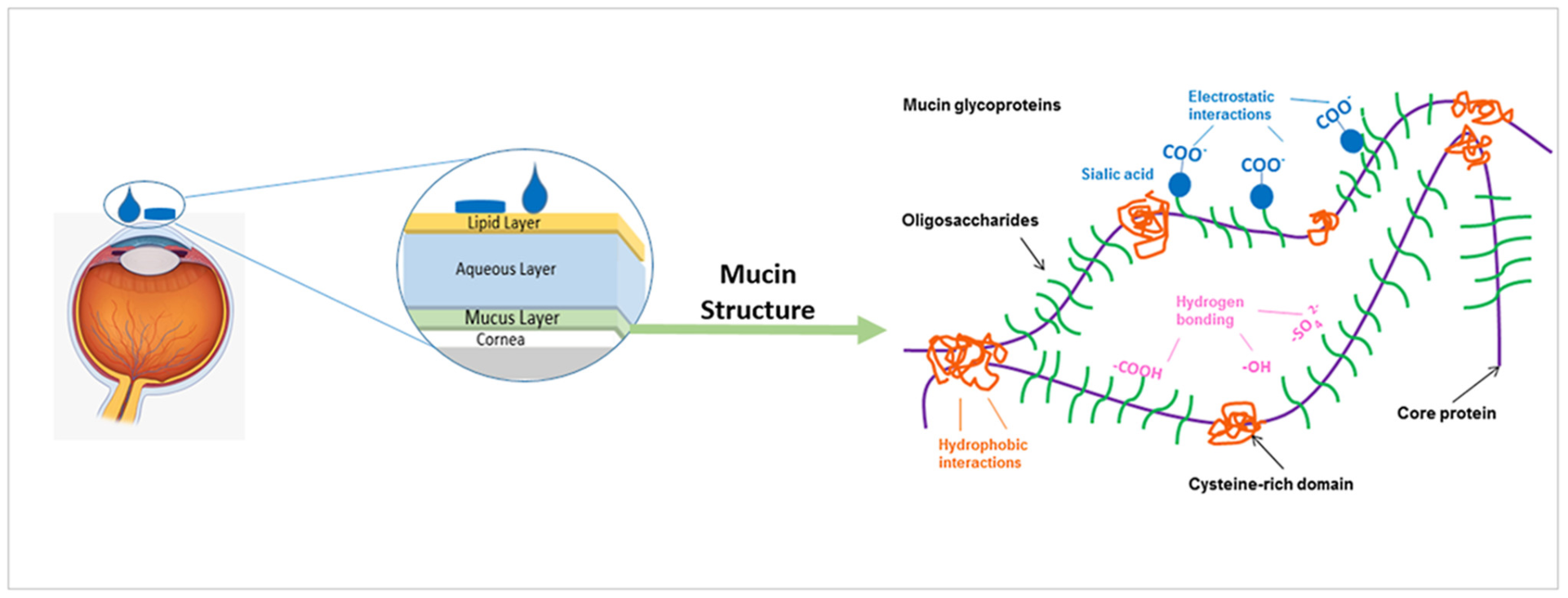
Ocular Mucins

4.2. Factors Affecting Mucoadhesion
4.3. Characterization of Mucoadhesion
4.3.1. Mechanistic Characterization Techniques
4.3.2. Performance Characterization Techniques
4.4. Considerations for Mucoadhesion in Ocular Drug Delivery
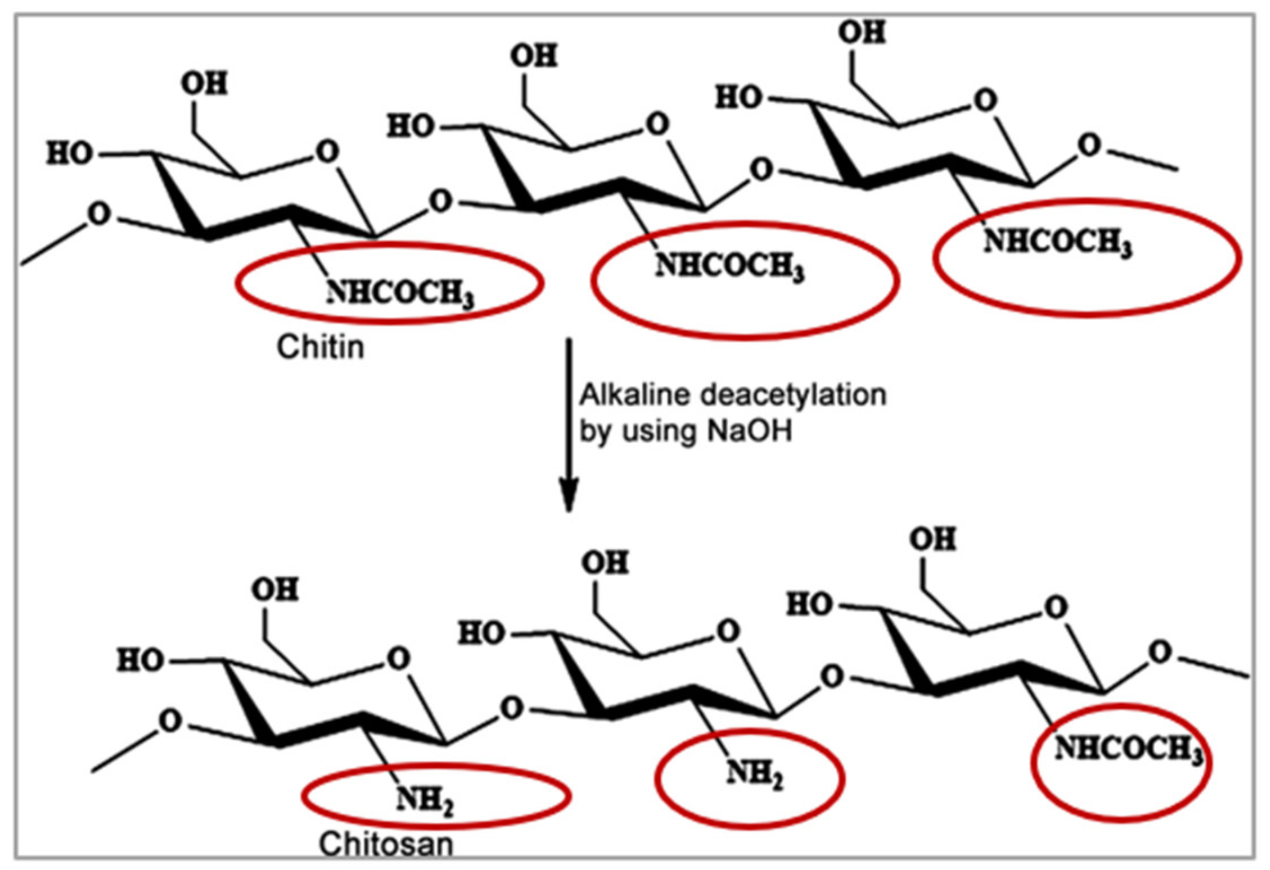
5. Chitosan-Based Mucosal Delivery
5.1. Chitosan Nanoparticles
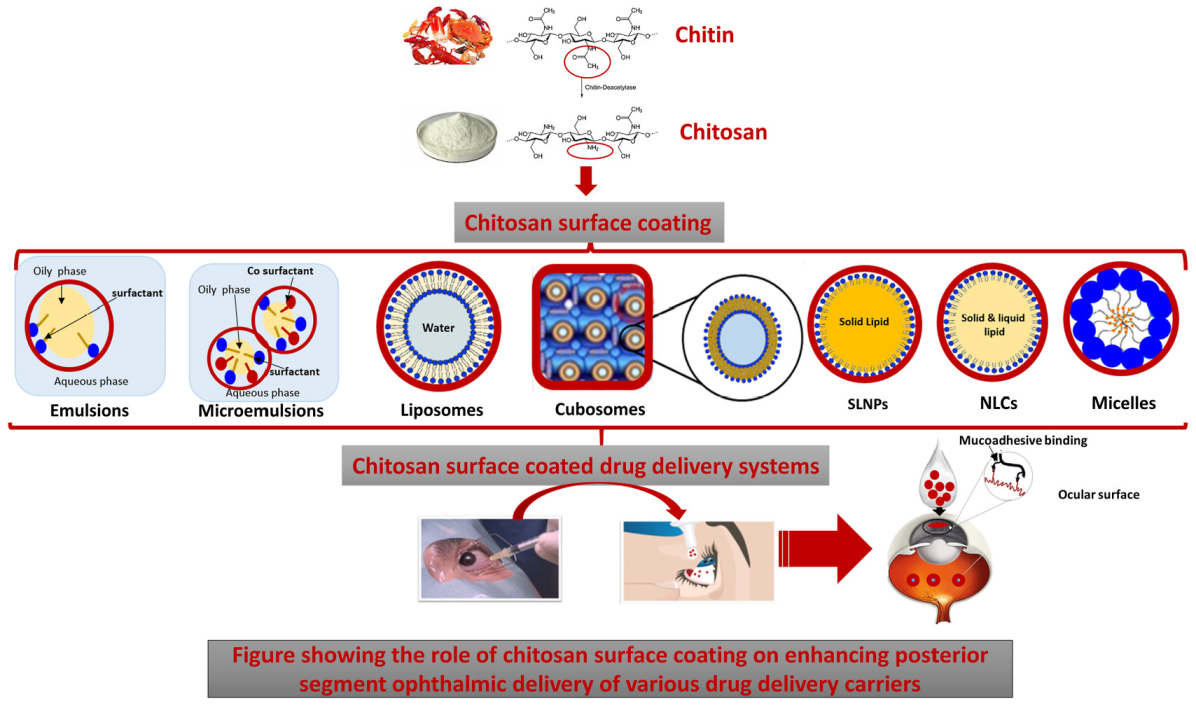
5.2. Chitosan Coated Drug Delivery Systems
5.2.1. Chitosan Coated Emulsions
Emulsions
Microemulsions (MEs)
5.2.2. Chitosan Coated Liposomes
5.2.3. Chitosan Coated Cubosomes
5.2.4. Chitosan Coated Lipid Particles SLNPs and NLCs
5.2.5. Chitosan Coated Nanomicelles
5.2.6. Chitosan Coated Nanocomposites

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Delivery System | Loaded Drug | Ref. |
|---|---|---|
| Chitosan-hyalouronic acid nanoparticles | Erythropoeitin | [131] |
| Emulsion | Coumarin-6 | [135] |
| Microemulsion | TA/coumarin-6 for PK studies | [137] |
| Liposomes | TA | [105] |
| Liposomes | TA | [145] |
| Liposomes | Coumarin-6 | [146] |
| Cubosomes | Voriconazole | [156] |
| SLNPs/NLCs | Indomethacin | [157] |
| NLCs | Itraconazole | [158] |
| Nanomicelles | Dexamethasone | [5,160] |
| Nanocomposites | DEXP | [161,164] |
6. Other Mucoadhesives
6.1. Mucoadhesion Using Poly Vinyl Alcohol
6.2. Hyalouronic Acid Based Mucoadhesion
6.3. Alginate Based Mucoadhesion
7. Challenges of Preclinical to Clinical Translation
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AFM | Atomic force microscopy |
| AMD | Age Macular Degeneration |
| Anti-VEGFs | Anti-vascular endothelial growth factors agents |
| ATR–FTIR | Fourier transform infrared spectral analysis |
| β-CD | β-cyclodextrin |
| CCB | Celecoxib |
| CCCs | Chitosan coated cubosomes |
| CCLs | chitosan coated liposomes |
| CDs | Cyclodextrins |
| CMCS | Carboxymethyl chitosan |
| CNV | Choroidal neovascularization (CNV) |
| Cs | Chitosan |
| CSO | Chitosan oligosaccharide |
| CVS | Chitosan oligosaccharide-valylvaline-steric acid |
| DEX | Dexamethasone |
| DR | Diabetic Retinopathy |
| DDS | Drug Delivery System |
| %EE | % Entrapment Efficiency |
| FITC | Fluorescein isothiocyanate isomer |
| GIT | Gastrointestinal tract |
| HConEpiC | Human conjunctival epithelial primary cells |
| HCEpiC | Human Corneal Epithelial Primary Cells |
| HP-β-CD | Hydroxypropyl β-cyclodextrin |
| HPMC | Hydroxypropyl methylcellulose |
| IVT | Intravitreal |
| LDH | Inorganic materials of hydroxide |
| MEs | microemulsions |
| MLVs | multilamellar vesicles |
| NF | Nepafenac |
| NLCs | Nanostructured lipid carriers |
| NMR | Nuclear magnetic resonance |
| OC-40 | Octoxynol-40 |
| OcDD | Ocular drug delivery |
| PDT | Photodynamic therapy |
| PEG | Poly (ethylene glycol) |
| PepT-1 | Peptide transporter-1 |
| PGF | Placental Growth Factors |
| P-gp | P-glycoprotein |
| PLGA | poly (lactic-co-glycolic acid) |
| PDS | port delivery system |
| PS | Particle size |
| PSEDs | Posterior segment eye diseases |
| PVA | Polyvinyl alcohol |
| PVA-R | Polyvinyl alcohol derivatives bearing a hydrophobic anchor at the terminate molecule |
| SA | Steric acid |
| TA | Triamcinolone aetonide |
| TER | Transepithelial electrical resistance |
| TPP | Sodium tripolyphosphate |
| ULVs | Unilamellar vesicles |
| VEGF | Vascular Endothelial Growth Factors |
| VV | Valyl valine |
| ZP | Zeta potential |
References
- Burton, M.J.; Ramke, J.; Marques, A.P.; Bourne, R.R.A.; Congdon, N.; Jones, I.; Ah Tong, B.A.M.; Arunga, S.; Bachani, D.; Bascaran, C.; et al. The Lancet Global Health Commission on Global Eye Health: Vision beyond 2020. Lancet Glob. Health 2021, 9, e489–e551. [Google Scholar] [CrossRef]
- Li, J.Q.; Welchowski, T.; Schmid, M.; Mauschitz, M.M.; Holz, F.G.; Finger, R.P. Prevalence and incidence of age-related macular degeneration in Europe: A systematic review and meta-analysis. Br. J. Ophthalmol. 2020, 104, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.R.A.; Flaxman, S.R.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; Leasher, J.; Limburg, H.; et al. Magnitude, temporal trends, and projections of the global prevalence of blindness and distance and near vision impairment: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e888–e897. [Google Scholar] [CrossRef] [Green Version]
- Gorantla, S.; Rapalli, V.K.; Waghule, T.; Singh, P.P.; Dubey, S.K.; Saha, R.N.; Singhvi, G. Nanocarriers for ocular drug delivery: Current status and translational opportunity. RSC Adv. 2020, 10, 27835–27855. [Google Scholar] [CrossRef]
- Xu, X.; Sun, L.; Zhou, L.; Cheng, Y.; Cao, F. Functional chitosan oligosaccharide nanomicelles for topical ocular drug delivery of dexamethasone. Carbohydr. Polym. 2020, 227, 115356. [Google Scholar] [CrossRef]
- Urtti, A. Challenges and obstacles of ocular pharmacokinetics and drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1131–1135. [Google Scholar] [CrossRef]
- Ali, M.; Byrne, M. Challenges and solutions in topical ocular drug-delivery systems. Expert Rev. Clin. Pharmacol. 2008, 1, 145–161. [Google Scholar] [CrossRef]
- Varela-Fernández, R.; Díaz-Tomé, V.; Luaces-Rodríguez, A.; Conde-Penedo, A.; García-Otero, X.; Luzardo-Álvarez, A.; Fernández-Ferreiro, A.; Otero-Espinar, F.J. Drug Delivery to the Posterior Segment of the Eye: Biopharmaceutic and Pharmacokinetic Considerations. Pharmaceutics 2020, 12, 269. [Google Scholar] [CrossRef] [Green Version]
- Kaji, H.; Nagai, N.; Nishizawa, M.; Abe, T. Drug delivery devices for retinal diseases. Adv. Drug Deliv. Rev. 2018, 128, 148–157. [Google Scholar] [CrossRef]
- Costagliola, C.; Agnifili, L.; Arcidiacono, B.; Duse, S.; Fasanella, V.; Mastropasqua, R.; Verolino, M.; Semeraro, F. Systemic thromboembolic adverse events in patients treated with intravitreal anti-VEGF drugs for neovascular age-related macular degeneration. Expert Opin. Biol. Ther. 2012, 12, 1299–1313. [Google Scholar] [CrossRef]
- Wang, Y.; Xu, X.; Gu, Y.; Cheng, Y.; Cao, F. Recent advance of nanoparticle-based topical drug delivery to the posterior segment of the eye. Expert Opin. Drug Deliv. 2018, 15. [Google Scholar] [CrossRef]
- Thareja, A.; Hughes, H.; Alvarez-Lorenzo, C.; Hakkarainen, J.J.; Ahmed, Z. Penetration Enhancers for Topical Drug Delivery to the Ocular Posterior Segment—A Systematic Review. Pharmaceutics 2021, 13, 276. [Google Scholar] [CrossRef]
- Johannsdottir, S.; Jansook, P.; Stefansson, E.; Kristinsdottir, I.M.; Asgrimsdottir, G.M.; Loftsson, T. Topical drug delivery to the posterior segment of the eye: The effect of benzalkonium chloride on topical dexamethasone penetration into the eye in vivo. J. Drug Deliv. Sci. Technol. 2018, 48, 125–127. [Google Scholar] [CrossRef]
- Di Prima, G.; Saladino, S.; Bongiovì, F.; Adamo, G.; Ghersi, G.; Pitarresi, G.; Giammona, G. Novel inulin-based mucoadhesive micelles loaded with corticosteroids as potential transcorneal permeation enhancers. Eur. J. Pharm. Biopharm. 2017, 117, 385–399. [Google Scholar] [CrossRef]
- Boddu, S.H.; Gupta, H.; Patel, S. Drug delivery to the back of the eye following topical administration: An update on research and patenting activity. Recent Pat. Drug Deliv. 2014, 8, 27–36. [Google Scholar] [CrossRef]
- Kumar, A.; Vimal, A.; Kumar, A. Why Chitosan? From properties to perspective of mucosal drug delivery. Int. J. Biol. Macromol. 2016, 91, 615–622. [Google Scholar] [CrossRef]
- Benediktsdóttir, B.E.; Baldursson, Ó.; Másson, M. Challenges in evaluation of chitosan and trimethylated chitosan (TMC) as mucosal permeation enhancers: From synthesis to in vitro application. J. Control. Release 2014, 173, 18–31. [Google Scholar] [CrossRef]
- M Ways, T.M.; Lau, W.M.; Khutoryanskiy, V.V. Chitosan and Its Derivatives for Application in Mucoadhesive Drug Delivery Systems. Polymers 2018, 10, 267. [Google Scholar] [CrossRef] [Green Version]
- Bernkop-Schnürch, A.; Dünnhaupt, S. Chitosan-based drug delivery systems. Eur. J. Pharm. Biopharm. 2012, 81, 463–469. [Google Scholar] [CrossRef]
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Moiseev, R.V.; Morrison, P.W.J.; Steele, F.; Khutoryanskiy, V.V. Penetration Enhancers in Ocular Drug Delivery. Pharmaceutics 2019, 11, 321. [Google Scholar] [CrossRef] [Green Version]
- Al-Zamil, W.M.; Yassin, S.A. Recent developments in age-related macular degeneration: A review. Clin. Interv. Aging 2017, 12, 1313–1330. [Google Scholar] [CrossRef] [Green Version]
- Kijlstra, A.; La Heij, E.C.; Hendrikse, F. Review Article, Immunological Factors in the Pathogenesis and Treatment of Age-Related Macular Degeneration. Ocul. Immunol. Inflamm. 2005, 13, 3–11. [Google Scholar] [CrossRef]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.-Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef] [Green Version]
- Skalicky, S.E. Ocular and Visual Physiology Clinical Application; Springer: Berlin/Heidelberg, Germany, 2015; p. 366. [Google Scholar] [CrossRef]
- Age-Related Eye Diseases. Available online: https://www.eyecentersofnwo.com/newsletters/september-2019 (accessed on 15 February 2021).
- Lim, L.S.; Mitchell, P.; Seddon, J.M.; Holz, F.G.; Wong, T.Y. Age-related macular degeneration. Lancet 2012, 379, 1728–1738. [Google Scholar] [CrossRef]
- Hood, D.C.; Raza, A.S.; de Moraes, C.G.V.; Liebmann, J.M.; Ritch, R. Glaucomatous damage of the macula. Prog. Retin. Eye Res. 2013, 32, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Gerster, H. Review: Antioxidant Protection of The Ageing Macula. Age Ageing 1991, 20, 60–69. [Google Scholar] [CrossRef]
- Gerritsen, M.E. Chapter 8—Angiogenesis. In Microcirculation, 2nd ed.; Tuma, R.F., Durán, W.N., Ley, K., Eds.; Academic Press: San Diego, CA, USA, 2008; pp. 351–383. [Google Scholar] [CrossRef]
- Ribatti, D. Angiogenesis. In Brenner’s Encyclopedia of Genetics, 2nd ed.; Maloy, S., Hughes, K., Eds.; Academic Press: San Diego, CA, USA, 2013; pp. 130–132. [Google Scholar] [CrossRef]
- Grossniklaus, H.E.; Green, W.R. Choroidal neovascularization. Am. J. Ophthalmol. 2004, 137, 496–503. [Google Scholar] [CrossRef]
- Flaxman, S.R.; Bourne, R.R.A.; Resnikoff, S.; Ackland, P.; Braithwaite, T.; Cicinelli, M.V.; Das, A.; Jonas, J.B.; Keeffe, J.; Kempen, J.H.; et al. Global causes of blindness and distance vision impairment 1990-2020: A systematic review and meta-analysis. Lancet Glob. Health 2017, 5, e1221–e1234. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; He, M.; Congdon, N. The worldwide epidemic of diabetic retinopathy. Indian J. Ophthalmol. 2012, 60, 428–431. [Google Scholar] [CrossRef]
- Duh, E.J.; Sun, J.K.; Stitt, A.W. Diabetic retinopathy: Current understanding, mechanisms, and treatment strategies. JCI Insight 2017, 2, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Zhang, L.; Weinreb, R.N. Ophthalmic drug discovery: Novel targets and mechanisms for retinal diseases and glaucoma. Nat. Rev. Drug Discov. 2012, 11, 541–559. [Google Scholar] [CrossRef] [PubMed]
- Avery, R.L.; Pieramici, D.J.; Rabena, M.D.; Castellarin, A.A.; Ma’an, A.N.; Giust, M.J. Intravitreal bevacizumab (Avastin) for neovascular age-related macular degeneration. Ophthalmology 2006, 113, 363–372.e365. [Google Scholar] [CrossRef] [PubMed]
- Jyothi, S.; Chowdhury, H.; Elagouz, M.; Sivaprasad, S. Intravitreal bevacizumab (Avastin) for age-related macular degeneration: A critical analysis of literature. Eye 2010, 24, 816–824. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, P.J.; Brown, D.M.; Heier, J.S.; Boyer, D.S.; Kaiser, P.K.; Chung, C.Y.; Kim, R.Y. Ranibizumab for neovascular age-related macular degeneration. N. Engl. J. Med. 2006, 355, 1419–1431. [Google Scholar] [CrossRef] [Green Version]
- Blick, S.K.; Keating, G.M.; Wagstaff, A.J. Ranibizumab. Drugs 2007, 67, 1199–1206. [Google Scholar] [CrossRef]
- Heier, J.S.; Brown, D.M.; Chong, V.; Korobelnik, J.-F.; Kaiser, P.K.; Nguyen, Q.D.; Kirchhof, B.; Ho, A.; Ogura, Y.; Yancopoulos, G.D. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology 2012, 119, 2537–2548. [Google Scholar] [CrossRef]
- Trichonas, G.; Kaiser, P.K. Aflibercept for the treatment of age-related macular degeneration. Ophthalmol. Ther. 2013, 2, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Pharmaceuticals. Regeneron, “Eylea (Aflibercept) Injection”. 2021. Available online: https://www.regeneron.com/medicines/eylea-injection (accessed on 15 March 2021).
- Dugel, P.U.; Koh, A.; Ogura, Y.; Jaffe, G.J.; Schmidt-Erfurth, U.; Brown, D.M.; Gomes, A.V.; Warburton, J.; Weichselberger, A.; Holz, F.G. HAWK and HARRIER: Phase 3, multicenter, randomized, double-masked trials of brolucizumab for neovascular age-related macular degeneration. Ophthalmology 2020, 127, 72–84. [Google Scholar] [CrossRef]
- Sharma, A.; Kumar, N.; Parachuri, N.; Sharma, R.; Bandello, F.; Kuppermann, B.D.; Loewenstein, A. Brolucizumab and immunogenicity. Eye 2020, 34, 1726–1728. [Google Scholar] [CrossRef]
- Gaudreault, J.; Gunde, T.; Floyd, H.S.; Ellis, J.; Tietz, J.; Binggeli, D.; Keller, B.; Schmidt, A.; Escher, D. Preclinical pharmacology and safety of ESBA1008, a single-chain antibody fragment, investigated as potential treatment for age related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2012, 53, 3025. [Google Scholar]
- Nimz, E.L.; Van’t Land, C.W.; Yáñez, J.A.; Chastain, J.E. Intraocular and systemic pharmacokinetics of brolucizumab (RTH258) in nonhuman primates. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4996. [Google Scholar]
- Ren, X.; Bu, S.; Zhang, X.; Jiang, Y.; Tan, L.; Zhang, H.; Li, X. Safety and efficacy of intravitreal conbercept injection after vitrectomy for the treatment of proliferative diabetic retinopathy. Eye 2019, 33, 1177–1183. [Google Scholar] [CrossRef]
- Li, X.; Xu, G.; Wang, Y.; Xu, X.; Liu, X.; Tang, S.; Zhang, F.; Zhang, J.; Tang, L.; Wu, Q.; et al. Safety and Efficacy of Conbercept in Neovascular Age-Related Macular Degeneration: Results from a 12-Month Randomized Phase 2 Study: AURORA Study. Ophthalmology 2014, 121, 1740–1747. [Google Scholar] [CrossRef] [Green Version]
- Cui, J.; Sun, D.; Lu, H.; Dai, R.; Xing, L.; Dong, H.; Wang, L.; Wei, D.; Jiang, B.; Jiao, Y. Comparison of effectiveness and safety between conbercept and ranibizumab for treatment of neovascular age-related macular degeneration. A retrospective case-controlled non-inferiority multiple center study. Eye 2018, 32, 391–399. [Google Scholar] [CrossRef] [Green Version]
- Dugel, P.U.; Jaffe, G.J.; Sallstig, P.; Warburton, J.; Weichselberger, A.; Wieland, M.; Singerman, L. Brolucizumab versus aflibercept in participants with neovascular age-related macular degeneration: A randomized trial. Ophthalmology 2017, 124, 1296–1304. [Google Scholar] [CrossRef]
- Tietz, J.; Spohn, G.; Schmid, G.; Konrad, J.; Jampen, S.; Maurer, P.; Schmidt, A.; Escher, D. Affinity and potency of RTH258 (ESBA1008), a novel inhibitor of vascular endothelial growth factor a for the treatment of retinal disorders. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1501. [Google Scholar]
- Lu, X.; Sun, X. Profile of conbercept in the treatment of neovascular age-related macular degeneration. Drug Des. Dev. Ther. 2015, 9, 2311–2320. [Google Scholar]
- Li, H.; Lei, N.; Zhang, M.; Li, Y.; Xiao, H.; Hao, X. Pharmacokinetics of a long-lasting anti-VEGF fusion protein in rabbit. Exp. Eye Res. 2012, 97, 154–159. [Google Scholar] [CrossRef]
- Sinapis, C.I.; Routsias, J.G.; Sinapis, A.I.; Sinapis, D.I.; Agrogiannis, G.D.; Pantopoulou, A.; Theocharis, S.E.; Baltatzis, S.; Patsouris, E.; Perrea, D. Pharmacokinetics of intravitreal bevacizumab (Avastin®) in rabbits. Clin. Ophthalmol. 2011, 5, 697–704. [Google Scholar] [CrossRef] [Green Version]
- Gao, L.; Tao, Y.; Liu, M.; Li, L.; Zhang, P.; Wang, H.; Zhang, L. Different conbercept injection strategies for the treatment of exudative age-related macular degeneration: A retrospective cohort study. Medicine 2020, 1–5. [Google Scholar] [CrossRef]
- Bai, Y.; Nie, H.; Wei, S.; Lu, X.; Ke, X.; Ouyang, X.; Feng, S. Efficacy of intravitreal conbercept injection in the treatment of retinopathy of prematurity. Br. J. Ophthalmol. 2019, 103, 494–498. [Google Scholar] [CrossRef]
- Campochiaro, P.A.; Marcus, D.M.; Awh, C.C.; Regillo, C.; Adamis, A.P.; Bantseev, V.; Chiang, Y.; Ehrlich, J.S.; Erickson, S.; Hanley, W.D. The port delivery system with ranibizumab for neovascular age-related macular degeneration: Results from the randomized phase 2 ladder clinical trial. Ophthalmology 2019, 126, 1141–1154. [Google Scholar] [CrossRef] [Green Version]
- Xie, B.; Jin, L.; Luo, Z.; Yu, J.; Shi, S.; Zhang, Z.; Shen, M.; Chen, H.; Li, X.; Song, Z. An injectable thermosensitive polymeric hydrogel for sustained release of Avastin® to treat posterior segment disease. Int. J. Pharm. 2015, 490, 375–383. [Google Scholar] [CrossRef]
- Yu, Y.; Lau, L.C.M.; Lo, A.C.-Y.; Chau, Y. Injectable chemically crosslinked hydrogel for the controlled release of bevacizumab in vitreous: A 6-month in vivo study. Transl. Vis. Sci. Technol. 2015, 4, 5. [Google Scholar] [CrossRef] [Green Version]
- Badiee, P.; Varshochian, R.; Rafiee-Tehrani, M.; Abedin Dorkoosh, F.; Khoshayand, M.R.; Dinarvand, R. Ocular implant containing bevacizumab-loaded chitosan nanoparticles intended for choroidal neovascularization treatment. J. Biomed. Mater. Res. Part A 2018, 106, 2261–2271. [Google Scholar] [CrossRef]
- Kim, J.; Kudisch, M.; Mudumba, S.; Asada, H.; Aya-Shibuya, E.; Bhisitkul, R.B.; Desai, T.A. Biocompatibility and pharmacokinetic analysis of an intracameral polycaprolactone drug delivery implant for glaucoma. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4341–4346. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.I.; Wolitz, R.A.; Dowling, A.H.; Bloom, H.R.; Irvine, A.R.; Schwartz, D.M. Visual and anatomic outcomes associated with posterior segment complications after ganciclovir implant procedures in patients with AIDS and cytomegalovirus retinitis. Am. J. Ophthalmol. 1999, 127, 288–293. [Google Scholar] [CrossRef]
- Wang, Y.-S.; Friedrichs, U.; Eichler, W.; Hoffmann, S.; Wiedemann, P. Inhibitory effects of triamcinolone acetonide on bFGF-induced migration and tube formation in choroidal microvascular endothelial cells. Graefe’s Arch. Clin. Exp. Ophthalmol. 2002, 240, 42–48. [Google Scholar] [CrossRef]
- Durairaj, C.; Shah, J.C.; Senapati, S.; Kompella, U.B. Prediction of vitreal half-life based on drug physicochemical properties: Quantitative structure–pharmacokinetic relationships (QSPKR). Pharm. Res. 2009, 26, 1236–1260. [Google Scholar] [CrossRef] [PubMed]
- Carnahan, M.C.; Goldstein, D.A. Ocular complications of topical, peri-ocular, and systemic corticosteroids. Curr. Opin. Ophthalmol. 2000, 11, 478–483. [Google Scholar] [CrossRef] [PubMed]
- Abdelkader, H.; Alany, R.G.; Pierscionek, B. Age-related cataract and drug therapy: Opportunities and challenges for topical antioxidant delivery to the lens. J. Pharm. Pharmacol. 2015, 67, 537–550. [Google Scholar] [CrossRef] [PubMed]
- Simaroj, P.; Sinsawad, P.; Lekhanont, K. Effects of intracameral triamcinolone and gentamicin injections following cataract surgery. J. Med. Assoc. Thail. 2011, 94, 819–825. [Google Scholar]
- Schmit-Eilenberger, V.K. A novel intravitreal fluocinolone acetonide implant (Iluvien®) in the treatment of patients with chronic diabetic macular edema that is insufficiently responsive to other medical treatment options: A case series. Clin. Ophthalmol. 2015, 9, 801–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakri, S.J.; Couch, S.M.; McCannel, C.A.; Edwards, A.O. Same-day triple therapy with photodynamic therapy, intravitreal dexamethasone, and bevacizumab in wet age-related macular degeneration. Retina 2009, 29, 573–578. [Google Scholar] [CrossRef]
- Augustin, A.J.; Puls, S.; Offermann, I. Triple therapy for choroidal neovascularization due to age-related macular degeneration: Verteporfin PDT, bevacizumab, and dexamethasone. Retina 2007, 27, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Francis, B.A.; Chang, E.L.; Haik, B.G. Particle size and drug interactions of injectable corticosteroids used in ophthalmic practice. Ophthalmology 1996, 103, 1884–1888. [Google Scholar] [CrossRef]
- Kuppermann, B.D.; Zacharias, L.C.; Kenney, M.C. Steroid differentiation: The safety profile of various steroids on retinal cells in vitro and their implications for clinical use (an American Ophthalmological Society thesis). Trans. Am. Ophthalmol. Soc. 2014, 112, 116–141. [Google Scholar]
- Chaudhary, V.; Mao, A.; Hooper, P.L.; Sheidow, T.G. Triamcinolone acetonide as adjunctive treatment to verteporfin in neovascular age-related macular degeneration: A prospective randomized trial. Ophthalmology 2007, 114, 2183–2189. [Google Scholar] [CrossRef]
- Gaudana, R.; Ananthula, H.K.; Parenky, A.; Mitra, A.K. Ocular drug delivery. AAPS J. 2010, 12, 348–360. [Google Scholar] [CrossRef]
- Subrizi, A.; Del Amo, E.M.; Korzhikov-Vlakh, V.; Tennikova, T.; Ruponen, M.; Urtti, A. Design principles of ocular drug delivery systems: Importance of drug payload, release rate, and material properties. Drug Discov. Today 2019, 24, 1446–1457. [Google Scholar] [CrossRef]
- Patel, A.; Cholkar, K.; Agrahari, V.; Mitra, A.K. Ocular drug delivery systems: An overview. World J. Pharmacol. 2013, 2, 47–64. [Google Scholar] [CrossRef]
- Atchison, E.A.; Omar, A.F.; Iezzi, R.; Barkmeier, A.J.; Bakri, S.J. Outcomes of an Intravitreal Injection Clinic. Retina 2017, 37, 1371–1376. [Google Scholar] [CrossRef]
- Nettey, H.; Darko, Y.; Bamiro, O.A.; Addo, R.T. Ocular barriers. In Ocular Drug Delivery: Advances, Challenges and Applications; Springer: Berlin/Heidelberg, Germany, 2016; pp. 27–36. [Google Scholar]
- Shen, J.; Wang, Y.; Ping, Q.; Xiao, Y.; Huang, X. Mucoadhesive effect of thiolated PEG stearate and its modified NLC for ocular drug delivery. J. Control. Release 2009, 137, 217–223. [Google Scholar] [CrossRef]
- Barbault-Foucher, S.; Gref, R.; Russo, P.; Guechot, J.; Bochot, A. Design of poly-ε-caprolactone nanospheres coated with bioadhesive hyaluronic acid for ocular delivery. J. Control. Release 2002, 83, 365–375. [Google Scholar] [CrossRef]
- Kapoor, Y.; Thomas, J.C.; Tan, G.; John, V.T.; Chauhan, A. Surfactant-laden soft contact lenses for extended delivery of ophthalmic drugs. Biomaterials 2009, 30, 867–878. [Google Scholar] [CrossRef]
- Del Amo, E.M.; Urtti, A. Current and future ophthalmic drug delivery systems: A shift to the posterior segment. Drug Discov. Today 2008, 13, 135–143. [Google Scholar] [CrossRef]
- Naderan, M. Ocular changes during pregnancy. J. Curr. Ophthalmol. 2018, 30, 202–210. [Google Scholar] [CrossRef]
- Ali, Y.; Lehmussaari, K. Industrial perspective in ocular drug delivery. Adv. Drug Deliv. Rev. 2006, 58, 1258–1268. [Google Scholar] [CrossRef]
- Prosperi-Porta, G.; Kedzior, S.; Muirhead, B.; Sheardown, H. Phenylboronic-acid-based polymeric micelles for mucoadhesive anterior segment ocular drug delivery. Biomacromolecules 2016, 17, 1449–1457. [Google Scholar] [CrossRef]
- Yu, A.; Shi, H.; Liu, H.; Bao, Z.; Dai, M.; Lin, D.; Lin, D.; Xu, X.; Li, X.; Wang, Y. Mucoadhesive dexamethasone-glycol chitosan nanoparticles for ophthalmic drug delivery. Int. J. Pharm. 2020, 575, 118943. [Google Scholar] [CrossRef]
- Daull, P.; Lallemand, F.; Philips, B.; Lambert, G.; Buggage, R.; Garrigue, J.-S. Distribution of cyclosporine A in ocular tissues after topical administration of cyclosporine A cationic emulsions to pigmented rabbits. Cornea 2013, 32, 345–354. [Google Scholar] [CrossRef]
- Bagnis, A.; Papadia, M.; Scotto, R.; Traverso, C.E. Current and emerging medical therapies in the treatment of glaucoma. Expert Opin. Emerg. Drugs 2011, 16, 293–307. [Google Scholar] [CrossRef]
- Cholkar, K.; Dasari, S.R.; Pal, D.; Mitra, A.K. 1–Eye: Anatomy, Physiology and Barriers to Drug Delivery. In Ocular Transporters and Receptors; Mitra, A.K., Ed.; Woodhead Publishing: Cambridge, UK, 2013; pp. 1–36. [Google Scholar] [CrossRef]
- Agrahari, V.; Mandal, A.; Agrahari, V.; Trinh, H.M.; Joseph, M.; Ray, A.; Hadji, H.; Mitra, R.; Pal, D.; Mitra, A.K. A comprehensive insight on ocular pharmacokinetics. Drug Deliv. Transl. Res. 2016, 6, 735–754. [Google Scholar] [CrossRef]
- Willcox, M.D.P.; Argüeso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- Tsai, C.-H.; Wang, P.-Y.; Lin, I.; Huang, H.; Liu, G.-S.; Tseng, C.-L. Ocular drug delivery: Role of degradable polymeric nanocarriers for ophthalmic application. Int. J. Mol. Sci. 2018, 19, 2830. [Google Scholar] [CrossRef] [Green Version]
- Sunkara, G.; Kompella, U.B. Membrane transport processes in the eye. Drugs Pharm. Sci. 2003, 130, 13–58. [Google Scholar]
- Ahmed, I.; Patton, T.F. Disposition of timolol and inulin in the rabbit eye following corneal versus non-corneal absorption. Int. J. Pharm. 1987, 38, 9–21. [Google Scholar] [CrossRef]
- Nickla, D.L.; Wallman, J. The multifunctional choroid. Prog. Retin. Eye Res. 2010, 29, 144–168. [Google Scholar] [CrossRef] [Green Version]
- Cunha-Vaz, J.; Bernardes, R.; Lobo, C. Blood-retinal barrier. Eur. J. Ophthalmol. 2011, 21 (Suppl. S6), S3–S9. [Google Scholar] [CrossRef]
- Chen, M.-S.; Hou, P.-K.; Tai, T.-Y.; Lin, B.J. Blood-Ocular Barriers. Tzu Chi Med. J. 2008, 20, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Acheampong, A.A.; Shackleton, M.; John, B.; Burke, J.; Wheeler, L.; Tang-Liu, D. Distribution of brimonidine into anterior and posterior tissues of monkey, rabbit, and rat eyes. Drug Metab. Dispos. 2002, 30, 421–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koevary, S.B.; Nussey, J.; Lake, S. Accumulation of Topically Applied Porcine Insulin in the Retina and Optic Nerve in Normal and Diabetic Rats. Investig. Ophthalmol. Vis. Sci. 2002, 43, 797–804. [Google Scholar]
- Kent, A.R.; Nussdorf, J.D.; David, R.; Tyson, F.; Small, D.; Fellows, D. Vitreous concentration of topically applied brimonidine tartrate 0.2%. Ophthalmology 2001, 108, 784–787. [Google Scholar] [CrossRef]
- Gu, Y.; Xu, C.; Wang, Y.; Zhou, X.; Fang, L.; Cao, F. Multifunctional Nanocomposites Based on Liposomes and Layered Double Hydroxides Conjugated with Glycylsarcosine for Efficient Topical Drug Delivery to the Posterior Segment of the Eye. Mol. Pharm. 2019, 16, 2845–2857. [Google Scholar] [CrossRef] [PubMed]
- de Cogan, F.; Hill, L.J.; Lynch, A.; Morgan-Warren, P.J.; Lechner, J.; Berwick, M.R.; Peacock, A.F.A.; Chen, M.; Scott, R.A.H.; Xu, H.; et al. Topical Delivery of Anti-VEGF Drugs to the Ocular Posterior Segment Using Cell-Penetrating Peptides. Investig. Ophthalmol. Vis. Sci. 2017, 58, 2578–2590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Gonzalez-De la Rosa, A.; Armendariz-Borunda, J.; Castro-Castaneda, C.R.; Santos, A. Safety and Tolerability of Topical Ophthalmic Triamcinolone Acetonide-Loaded Liposomes Formulation and Evaluation of Its Biologic Activity in Patients with Diabetic Macular Edema. Pharmaceutics 2021, 13, 322. [Google Scholar] [CrossRef] [PubMed]
- Khalil, M.; Hashmi, U.; Riaz, R.; Rukh Abbas, S. Chitosan coated liposomes (CCL) containing triamcinolone acetonide for sustained delivery: A potential topical treatment for posterior segment diseases. Int. J. Biol. Macromol. 2020, 143, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, D.P. Mucoadhesive Microspheres: A Short Review. Asian J. Pharm. Clin. Res. 2012, 5, 24–27. [Google Scholar]
- Smart, J.D. The basics and underlying mechanisms of mucoadhesion. Adv. Drug Deliv. Rev. 2005, 57, 1556–1568. [Google Scholar] [CrossRef]
- Shaikh, R.; Raj Singh, T.; Garland, M.; Woolfson, A.; Donnelly, R. Mucoadhesive drug delivery systems. J. Pharm. Bioallied Sci. 2011, 3, 89–100. [Google Scholar] [CrossRef]
- Mackie, A.R.; Goycoolea, F.M.; Menchicchi, B.; Caramella, C.M.; Saporito, F.; Lee, S.; Stephansen, K.; Chronakis, I.S.; Hiorth, M.; Adamczak, M.; et al. Innovative Methods and Applications in Mucoadhesion Research. Macromol. Biosci. 2017, 17, 1600534. [Google Scholar] [CrossRef] [Green Version]
- Mansuri, S.; Kesharwani, P.; Jain, K.; Tekade, R.K.; Jain, N.K. Mucoadhesion: A promising approach in drug delivery system. React. Funct. Polym. 2016, 100, 151–172. [Google Scholar] [CrossRef]
- Khutoryanskiy, V.V. Advances in mucoadhesion and mucoadhesive polymers. Macromol. Biosci. 2011, 11, 748–764. [Google Scholar] [CrossRef]
- Leal, J.; Smyth, H.D.C.; Ghosh, D. Physicochemical properties of mucus and their impact on transmucosal drug delivery. Int. J. Pharm. 2017, 532, 555–572. [Google Scholar] [CrossRef]
- Georgiev, G.A.; Eftimov, P.; Yokoi, N. Contribution of Mucins towards the Physical Properties of the Tear Film: A Modern Update. Int. J. Mol. Sci. 2019, 20, 6132. [Google Scholar] [CrossRef] [Green Version]
- Yang, X.; Forier, K.; Steukers, L.; Van Vlierberghe, S.; Dubruel, P.; Braeckmans, K.; Glorieux, S. Immobilization of Pseudorabies Virus in Porcine Tracheal Respiratory Mucus Revealed by Single Particle Tracking. PLoS ONE 2012, 7, e51054. [Google Scholar] [CrossRef] [Green Version]
- Duggan, S.; Cummins, W.; O’Donovan, O.; Hughes, H.; Owens, E. Thiolated polymers as mucoadhesive drug delivery systems. Eur. J. Pharm. Sci. 2017, 100, 64–78. [Google Scholar] [CrossRef]
- Grewal, H.S.; Nam Kim, H.; Cho, I.-J.; Yoon, E.-S. Role of Viscous Dissipative Processes on the Wetting of Textured Surfaces. Sci. Rep. 2015, 5, 14159. [Google Scholar] [CrossRef] [Green Version]
- Sandri, S.R.G.; Bonferoni, M.C.; Ferrari, F.; Mori, M.; Caramella, C. The role of chitosan as a mucoadhesive agent in mucosal drug delivery. J. Drug Deliv. Sci. Technol. 2012, 22, 275–284. [Google Scholar] [CrossRef]
- Sandri, G.; Rossi, S.; Ferrari, F.; Bonferoni, M.C.; Zerrouk, N.; Caramella, C. Mucoadhesive and penetration enhancement properties of three grades of hyaluronic acid using porcine buccal and vaginal tissue, Caco-2 cell lines, and rat jejunum. J. Pharm. Pharmacol. 2004, 56, 1083–1090. [Google Scholar] [CrossRef]
- Choy, Y.B.; Park, J.-H.; Prausnitz, M.R. Mucoadhesive microparticles engineered for ophthalmic drug delivery. J. Phys. Chem. Solids 2008, 69, 1533–1536. [Google Scholar] [CrossRef] [Green Version]
- Chaiyasan, W.; Srinivas, S.P.; Tiyaboonchai, W. Mucoadhesive chitosan-dextran sulfate nanoparticles for sustained drug delivery to the ocular surface. J. Ocul. Pharm. 2013, 29, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Kandile, N.; Zaky, H.; Ismail, M.; Nasr, A.; Ali, Y.; Saleh, Y. Extraction and Characterization of Chitosan from Shrimp Shells. Open J. Org. Polym. Mater. 2018, 8, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Muxika, A.; Etxabide, A.; Uranga, J.; Guerrero, P.; de la Caba, K. Chitosan as a bioactive polymer: Processing, properties and applications. Int. J. Biol. Macromol. 2017, 105, 1358–1368. [Google Scholar] [CrossRef]
- Zamboulis, A.; Nanaki, S.; Michailidou, G.; Koumentakou, I.; Lazaridou, M.; Ainali, N.M.; Xanthopoulou, E.; Bikiaris, D.N. Chitosan and its Derivatives for Ocular Delivery Formulations: Recent Advances and Developments. Polymers 2020, 12, 1519. [Google Scholar] [CrossRef]
- Calvo, P.; Remuñan-López, C.; Vila-Jato, J.L.; Alonso, M.J. Chitosan and Chitosan/Ethylene Oxide-Propylene Oxide Block Copolymer Nanoparticles as Novel Carriers for Proteins and Vaccines. Pharm. Res. 1997, 14, 1431–1436. [Google Scholar] [CrossRef]
- Verheul, R.J.; van der Wal, S.; Hennink, W.E. Tailorable thiolated trimethyl chitosans for covalently stabilized nanoparticles. Biomacromolecules 2010, 11, 1965–1971. [Google Scholar] [CrossRef]
- Li, M.F.; Chen, L.; Xu, M.Z.; Zhang, J.L.; Wang, Q.; Zeng, Q.Z.; Wei, X.C.; Yuan, Y. The formation of zein-chitosan complex coacervated particles: Relationship to encapsulation and controlled release properties. Int. J. Biol. Macromol. 2018, 116, 1232–1239. [Google Scholar] [CrossRef]
- Cruz-Cazarim, E.L.C.; Cazarim, M.S.; Ogunjimi, A.T.; Petrilli, R.; Rocha, E.M.; Lopez, R.F.V. Prospective insulin-based ophthalmic delivery systems for the treatment of dry eye syndrome and corneal injuries. Eur. J. Pharm. Biopharm. 2019, 140, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rosca, I.D.; Watari, F.; Uo, M. Microparticle formation and its mechanism in single and double emulsion solvent evaporation. J. Control. Release 2004, 99, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Chen, X.G.; Li, Y.Y.; Liu, C.S. Self-assembled nanoparticles based on hydrophobically modified chitosan as carriers for doxorubicin. Nanomedicine 2007, 3, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Vichare, R.; Garner, I.; Paulson, R.J.; Tzekov, R.; Sahiner, N.; Panguluri, S.K.; Mohapatra, S.; Mohapatra, S.S.; Ayyala, R.; Sneed, K.B.; et al. Biofabrication of Chitosan-Based Nanomedicines and Its Potential Use for Translational Ophthalmic Applications. Appl. Sci. 2020, 10, 4189. [Google Scholar] [CrossRef]
- Silva, B.; Marto, J.; Braz, B.S.; Delgado, E.; Almeida, A.J.; Gonçalves, L. New nanoparticles for topical ocular delivery of erythropoietin. Int. J. Pharm. 2020, 576, 119020. [Google Scholar] [CrossRef]
- Bugnicourt, L.; Ladavière, C. A close collaboration of chitosan with lipid colloidal carriers for drug delivery applications. J. Control. Release 2017, 256, 121–140. [Google Scholar] [CrossRef]
- Peng, C.C.; Bengani, L.C.; Jung, H.J.; Leclerc, J.; Gupta, C.; Chauhan, A. Emulsions and microemulsions for ocular drug delivery. J. Drug Deliv. Sci. Technol. 2011, 21, 111–121. [Google Scholar] [CrossRef]
- Su, M.; Zhao, M.; Luo, Y.; Lin, X.; Xu, L.; He, H.; Xu, H.; Tang, X. Evaluation of the efficacy, toxicity and safety of vinorelbine incorporated in a lipid emulsion. Int. J. Pharm. 2011, 411, 188–196. [Google Scholar] [CrossRef]
- Ying, L.; Tahara, K.; Takeuchi, H. Drug delivery to the ocular posterior segment using lipid emulsion via eye drop administration: Effect of emulsion formulations and surface modification. Int. J. Pharm. 2013, 453, 329–335. [Google Scholar] [CrossRef]
- Üstündağ Okur, N.; Çağlar, E.Ş.; Siafaka, P.I. Novel Ocular Drug Delivery Systems: An Update on Microemulsions. J. Ocul. Pharmacol. Ther. 2020, 36, 342–354. [Google Scholar] [CrossRef]
- Raval, N.; Khunt, D.; Misra, M. Microemulsion-based delivery of triamcinolone acetonide to posterior segment of eye using chitosan and butter oil as permeation enhancer: An in vitro and in vivo investigation. J. Microencapsul. 2018, 35, 62–77. [Google Scholar] [CrossRef]
- Agarwal, R.; Iezhitsa, I.; Agarwal, P.; Abdul Nasir, N.A.; Razali, N.; Alyautdin, R.; Ismail, N.M. Liposomes in topical ophthalmic drug delivery: An update. Drug Deliv. 2016, 23, 1075–1091. [Google Scholar] [CrossRef]
- Daraee, H.; Etemadi, A.; Kouhi, M.; Alimirzalu, S.; Akbarzadeh, A. Application of liposomes in medicine and drug delivery. Artif. Cells Nanomed. Biotechnol. 2016, 44, 381–391. [Google Scholar] [CrossRef]
- Allen, T.M.; Cullis, P.R. Liposomal drug delivery systems: From concept to clinical applications. Adv. Drug Deliv. Rev. 2013, 65, 36–48. [Google Scholar] [CrossRef]
- Schwendener, R.A. Liposomes as vaccine delivery systems: A review of the recent advances. Ther. Adv. Vaccines 2014, 2, 159–182. [Google Scholar] [CrossRef]
- Hironaka, K.; Inokuchi, Y.; Tozuka, Y.; Shimazawa, M.; Hara, H.; Takeuchi, H. Design and evaluation of a liposomal delivery system targeting the posterior segment of the eye. J. Control. Release 2009, 136, 247–253. [Google Scholar] [CrossRef]
- Altamirano-Vallejo, J.C.; Navarro-Partida, J.; Gonzalez-De la Rosa, A.; Hsiao, J.H.; Olguín-Gutierrez, J.S.; Gonzalez-Villegas, A.C.; Keller, B.C.; Bouzo-Lopez, L.; Santos, A. Characterization and Pharmacokinetics of Triamcinolone Acetonide-Loaded Liposomes Topical Formulations for Vitreoretinal Drug Delivery. J. Ocul. Pharm. 2018, 34, 416–425. [Google Scholar] [CrossRef]
- Inokuchi, Y.; Hironaka, K.; Fujisawa, T.; Tozuka, Y.; Tsuruma, K.; Shimazawa, M.; Takeuchi, H.; Hara, H. Physicochemical Properties Affecting Retinal Drug/Coumarin-6 Delivery from Nanocarrier Systems via Eyedrop Administration. Investig. Ophthalmol. Vis. Sci. 2010, 51, 3162–3170. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Cheng, T.; Tian, Q.; Cheng, Y.; Zhao, L.; Zhang, X.; Qu, Y. A more efficient ocular delivery system of triamcinolone acetonide as eye drop to the posterior segment of the eye. Drug Deliv. 2019, 26, 188–198. [Google Scholar] [CrossRef] [Green Version]
- Cheng, T.; Li, J.; Cheng, Y.; Zhang, X.; Qu, Y. Triamcinolone acetonide-chitosan coated liposomes efficiently treated retinal edema as eye drops. Exp. Eye Res. 2019, 188, 107805. [Google Scholar] [CrossRef]
- Li, N.; Zhuang, C.-Y.; Wang, M.; Sui, C.-G.; Pan, W.-S. Low molecular weight chitosan-coated liposomes for ocular drug delivery: In vitro and in vivo studies. Drug Deliv. 2012, 19, 28–35. [Google Scholar] [CrossRef]
- Karami, Z.; Hamidi, M. Cubosomes: Remarkable drug delivery potential. Drug Discov. Today 2016, 21, 789–801. [Google Scholar] [CrossRef]
- Gregoriadis, G. Engineering liposomes for drug delivery: Progress and problems. Trends Biotechnol. 1995, 13, 527–537. [Google Scholar] [CrossRef]
- Gregoriadis, G.; Florence, A.T. Liposomes in Drug Delivery. Drugs 1993, 45, 15–28. [Google Scholar] [CrossRef]
- El-Gendy, M.A.; Mansour, M.; El-Assal, M.I.A.; Ishak, R.A.H.; Mortada, N.D. Delineating penetration enhancer-enriched liquid crystalline nanostructures as novel platforms for improved ophthalmic delivery. Int. J. Pharm. 2020, 582, 119313. [Google Scholar] [CrossRef]
- Han, S.; Shen, J.-Q.; Gan, Y.; Geng, H.-M.; Zhang, X.-X.; Zhu, C.-L.; Gan, L. Novel vehicle based on cubosomes for ophthalmic delivery of flurbiprofen with low irritancy and high bioavailability. Acta Pharmacol. Sin. 2010, 31, 990–998. [Google Scholar] [CrossRef]
- Ali, Z.; Sharma, P.; Warsi, M. Fabrication and Evaluation of Ketorolac Loaded Cubosome for Ocular Drug Delivery. J. Appl. Pharm. Sci. 2016, 6, 204–208. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.; Peng, T.; Li, Y.; Zhan, Z.; Zeng, Y.; Huang, Y.; Pan, X.; Wu, C.Y.; Wu, C. Ocular Cubosome Drug Delivery System for Timolol Maleate: Preparation, Characterization, Cytotoxicity, Ex Vivo, and In Vivo Evaluation. AAPS PharmSciTech 2017, 18, 2919–2926. [Google Scholar] [CrossRef]
- Eldeeb, A.E.; Salah, S.; Ghorab, M. Formulation and evaluation of cubosomes drug delivery system for treatment of glaucoma: Ex-vivo permeation and in-vivo pharmacodynamic study. J. Drug Deliv. Sci. Technol. 2019, 52, 236–247. [Google Scholar] [CrossRef]
- Said, M.; Aboelwafa, A.; Elshafeey, A.; Elsayed, I. Central composite optimization of ocular mucoadhesive cubosomes for enhanced bioavailability and controlled delivery of voriconazole. J. Drug Deliv. Sci. Technol. 2020. [Google Scholar] [CrossRef]
- Balguri, S.P.; Adelli, G.R.; Majumdar, S. Topical ophthalmic lipid nanoparticle formulations (SLN, NLC) of indomethacin for delivery to the posterior segment ocular tissues. Eur. J. Pharm. Biopharm. 2016, 109, 224–235. [Google Scholar] [CrossRef] [Green Version]
- Selvaraj, K.; Kuppusamy, G.; Krishnamurthy, J.; Mahalingam, R.; Singh, S.K.; Gulati, M. Repositioning of Itraconazole for the Management of Ocular Neovascularization Through Surface-Modified Nanostructured Lipid Carriers. ASSAY Drug Dev. Technol. 2019, 17, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Owen, S.C.; Chan, D.P.; Shoichet, M.S. Polymeric micelle stability. Nano Today 2012, 7, 53–65. [Google Scholar] [CrossRef]
- Gukasyan, H.J.; Hailu, S.; Karami, T.K.; Graham, R. Ocular biopharmaceutics: Impact of modeling and simulation on topical ophthalmic formulation development. Drug Discov. Today 2019, 24, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- Chi, J.; Jiang, Z.; Qiao, J.; Peng, Y.; Liu, W.; Han, B. Synthesis and anti-metastasis activities of norcantharidin-conjugated carboxymethyl chitosan as a novel drug delivery system. Carbohydr. Polym. 2019, 214, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Chi, H.; Gu, Y.; Xu, T.; Cao, F. Multifunctional organic–inorganic hybrid nanoparticles and nanosheets based on chitosan derivative and layered double hydroxide: Cellular uptake mechanism and application for topical ocular drug delivery. Int. J. Nanomed. 2017, 12, 1607–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Xu, X.; Gu, Y.; Fang, L.; Cao, F. Functional intercalated nanocomposites with chitosan-glutathione-glycylsarcosine and layered double hydroxides for topical ocular drug delivery. Int. J. Nanomed. 2018, 13, 917–937. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Zhou, L.; Fang, L.; Cao, F. Multifunctional carboxymethyl chitosan derivatives-layered double hydroxide hybrid nanocomposites for efficient drug delivery to the posterior segment of the eye. Acta Biomater. 2020, 104, 104–114. [Google Scholar] [CrossRef]
- Fujisawa, T.; Miyai, H.; Hironaka, K.; Tsukamoto, T.; Tahara, K.; Tozuka, Y.; Ito, M.; Takeuchi, H. Liposomal diclofenac eye drop formulations targeting the retina: Formulation stability improvement using surface modification of liposomes. Int. J. Pharm. 2012, 436, 564–567. [Google Scholar] [CrossRef]
- Saettone, M.F.; Giannaccini, B.; Ravecca, S.; La Marca, F.; Tota, G. Polymer effects on ocular bioavailability—the influence of different liquid vehicles on the mydriatic response of tropicamide in humans and in rabbits. Int. J. Pharm. 1984, 20, 187–202. [Google Scholar] [CrossRef]
- Jansook, P.; Kulsirachote, P.; Loftsson, T. Cyclodextrin solubilization of celecoxib: Solid and solution state characterization. J. Incl. Phenom. Macrocycl. Chem. 2018, 90, 75–88. [Google Scholar] [CrossRef]
- Lorenzo-Veiga, B.; Diaz-Rodriguez, P.; Alvarez-Lorenzo, C.; Loftsson, T.; Sigurdsson, H.H. In vitro and ex vivo evaluation of Nepafenac-based cyclodextrin microparticles for treatment of eye inflammation. Nanomaterials 2020, 10, 709. [Google Scholar] [CrossRef] [Green Version]
- Anderson, D.; Brydon, W.; Eastwood, M.; Sedgwick, D. Dietary effects of sodium alginate in humans. Food Addit. Contam. 1991, 8, 237–248. [Google Scholar] [CrossRef]
- Shelley, H.; Rodriguez-Galarza, R.M.; Duran, S.H.; Abarca, E.M.; Babu, R.J. In situ gel formulation for enhanced ocular delivery of nepafenac. J. Pharm. Sci. 2018, 107, 3089–3097. [Google Scholar] [CrossRef]
- Kumar, A.; Naik, P.K.; Pradhan, D.; Ghosh, G.; Rath, G. Mucoadhesive formulations: Innovations, merits, drawbacks, and future outlook. Pharm. Dev. Technol. 2020, 25, 797–814. [Google Scholar] [CrossRef]
- Alruwaili, N.K.; Zafar, A.; Imam, S.S.; Alharbi, K.S.; Alotaibi, N.H.; Alshehri, S.; Alhakamy, N.A.; Alzarea, A.I.; Afzal, M.; Elmowafy, M. Stimulus Responsive Ocular Gentamycin-Ferrying Chitosan Nanoparticles Hydrogel: Formulation Optimization, Ocular Safety and Antibacterial Assessment. Int. J. Nanomed. 2020, 15, 4717–4737. [Google Scholar] [CrossRef]
- de Campos, A.M.; Diebold, Y.; Carvalho, E.L.S.; Sánchez, A.; José Alonso, M. Chitosan Nanoparticles as New Ocular Drug Delivery Systems: In Vitro Stability, in Vivo Fate, and Cellular Toxicity. Pharm. Res. 2004, 21, 803–810. [Google Scholar] [CrossRef]
- de Salamanca, A.E.Q.; Diebold, Y.; Calonge, M.; García-Vazquez, C.; Callejo, S.; Vila, A.; Alonso, M.J. Chitosan Nanoparticles as a Potential Drug Delivery System for the Ocular Surface: Toxicity, Uptake Mechanism and In Vivo Tolerance. Investig. Ophthalmol. Vis. Sci. 2006, 47, 1416–1425. [Google Scholar] [CrossRef]
- Diebold, Y.; Jarrín, M.; Sáez, V.; Carvalho, E.L.S.; Orea, M.; Calonge, M.; Seijo, B.; Alonso, M.J. Ocular drug delivery by liposome–chitosan nanoparticle complexes (LCS-NP). Biomaterials 2007, 28, 1553–1564. [Google Scholar] [CrossRef]
- Silva, M.M.; Calado, R.; Marto, J.; Bettencourt, A.; Almeida, A.J.; Gonçalves, L.M.D. Chitosan Nanoparticles as a Mucoadhesive Drug Delivery System for Ocular Administration. Mar. Drugs 2017, 15, 370. [Google Scholar] [CrossRef] [Green Version]
- de la Fuente, M.; Raviña, M.; Paolicelli, P.; Sanchez, A.; Seijo, B.; Alonso, M.J. Chitosan-based nanostructures: A delivery platform for ocular therapeutics. Adv. Drug Deliv. Rev. 2010, 62, 100–117. [Google Scholar] [CrossRef]
- Inmaculada, A.; Marian, M.; Ruth, H.; Beatriz, M.; Niuris, A.; Laura, C.; Angela, S.; Angeles, H. Role of Physicochemical Properties of Chitin and Chitosan on their Functionality. Curr. Chem. Biol. 2014, 8, 27–42. [Google Scholar] [CrossRef]







| Drugs | Molecular Weight | IVT Injection Dosage Regimen | Mechanism of Action | Reported Side Effects |
|---|---|---|---|---|
| Bevacizumab (Avastin®) | 149 kDa | 1.25 mg q 4 weeks [37] | Humanized anti-VEGF-A antibody binding all isoforms and biologically active degradation products [38] | Blurred vision, vitreous floaters and swelling of the cornea [37] |
| Ranibizumab (Lucentis®) | 48 kDa | 0.3 or 0.5 mg q 4 weeks [39] | Humanized anti-VEGF-A antibody binding fragment targeting all isoforms and biologically active degradation products [40] | Endopthalmitis, vitreous floaters and eye pain [39] |
| Aflibercept (Eylea®) | 96.6 kDa | 2 mg at weeks 0, 4 and 8 then q 8 weeks [41] | Chimeric protein binding all isomers of the VEGF-A family, VEGF-B and PGF [42] | Conjunctival haemorrhage, eye pain, vitreous detachment and floaters and ocular hypertension [41,43] |
| Brolucizumab (Beovu®) | 26 kDa | 6 mg q 12 weeks [44] | Single-chain antibody fragment inhibitor of VEGF-A isoforms [44,45] | Blurred vision, cataract, conjunctival hemorrhage, vitreous floaters and eye pain [44,46,47] |
| Conbercept (Lumitin®) | 142 kDa | 0.5 mg at weeks 1, 4, 12 and 24 [48] | Recombinant fusion protein targeting multiple VEGF isoforms (VEGF-B, PIGF and VEGF-A) [49] | Eye pain, intraocular pressure and conjunctival haemorrhage [49,50] |
| Theory | Mechanism | Illustration |
|---|---|---|
| Wettability theory | Used to describe the mucoadhesive interactions in case of liquid formulations based on their spreadability on mucosal membranes. Interfacial tension is the main determinant of wettability and spreadability of liquid formulations. In addition, other secondary factors including viscosity, disjoining pressure, and contact line friction effects are also reported to affect the wetting of surfaces [116]. The better the spreadability, the higher the chances for mucoadhesion. Spreadability can be assessed through the measurement of the liquid formulations’ contact angles with the mucosal surface using the equation (γ SG = γ SL + γ LG cos (θ C), where γ SG is the surface tensions of the solid, γ LG is the surface tension of the liquid, γ SL represents the interfacial tension between them, and θ is the contact angle formed when they come into contact. The lower the value of the contact angle, the higher the spreadability and vice versa, and hence the higher the chances of mucosal interactions [110]. |  |
| Mechanical theory | Used to describe mucoadhesion of liquids, it attributes mucoadhesion to the interlocking of the liquid mucoadhseive into the rough mucosal surface irregularities. Surface roughness increases the interaction area as well as viscoelastic and plastic dissipation of energy in case of joint failure. These later factors are considered more critical for mucoadhesion than the mechanical effect alone [107] |  |
| Electronic theory | Mucoadhesive interactions are attributed to the formation of electrostatic interactions between oppositely charged surfaces, as in the electrostatic interaction between the negatively charged mucin and positively charged polymers such as chitosan [110] |  |
| Adsorption theory | Mucoadhesion is a result of covalent bonding between the formulation and the mucus surface via hydrogen bonds and van der waal’s forces [110] |  |
| Diffusion interlocking theory | In this theory, mucoadhesion is attributed to time and concentration gradient dependent inter diffusion of polymer chains and mucus glycoprotein chains across the mucoadhesive interface. Following diffusion, sufficient interpenetration depth and chain entanglements induce semi-permanent mucoadhesive bond formation. This process is governed by several factors including temperature, polymer molecular weight, molecular chain length, cross-linking density, molecular chain mobility and flexibility, as well as expansion capacity [107,110] |  |
| Fracture theory | It differs from the other theories in relating the strength of mucoadhesion between two surfaces to the force required for their separation and detachment. It is assumed that the mucoadhesive bond failure occurs at the interface; however, failure typically occurs at the weakest point which could be any of the adhering surfaces as well [107,110] |  |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burhan, A.M.; Klahan, B.; Cummins, W.; Andrés-Guerrero, V.; Byrne, M.E.; O’Reilly, N.J.; Chauhan, A.; Fitzhenry, L.; Hughes, H. Posterior Segment Ophthalmic Drug Delivery: Role of Muco-Adhesion with a Special Focus on Chitosan. Pharmaceutics 2021, 13, 1685. https://doi.org/10.3390/pharmaceutics13101685
Burhan AM, Klahan B, Cummins W, Andrés-Guerrero V, Byrne ME, O’Reilly NJ, Chauhan A, Fitzhenry L, Hughes H. Posterior Segment Ophthalmic Drug Delivery: Role of Muco-Adhesion with a Special Focus on Chitosan. Pharmaceutics. 2021; 13(10):1685. https://doi.org/10.3390/pharmaceutics13101685
Chicago/Turabian StyleBurhan, Ayah Mohammad, Butsabarat Klahan, Wayne Cummins, Vanessa Andrés-Guerrero, Mark E. Byrne, Niall J. O’Reilly, Anuj Chauhan, Laurence Fitzhenry, and Helen Hughes. 2021. "Posterior Segment Ophthalmic Drug Delivery: Role of Muco-Adhesion with a Special Focus on Chitosan" Pharmaceutics 13, no. 10: 1685. https://doi.org/10.3390/pharmaceutics13101685