Better Medicines for Older Patients: Considerations between Patient Characteristics and Solid Oral Dosage Form Designs to Improve Swallowing Experience


Abstract
:1. Introduction
2. Swallowing Problems in the Older Patient Population
2.1. Prevalence of Dysphagia
2.2. Factors Contributing to Dysphagia
2.2.1. Age-Related Dysphagia
2.2.2. Disease-Related Dysphagia
2.2.3. Drug-Related Dysphagia
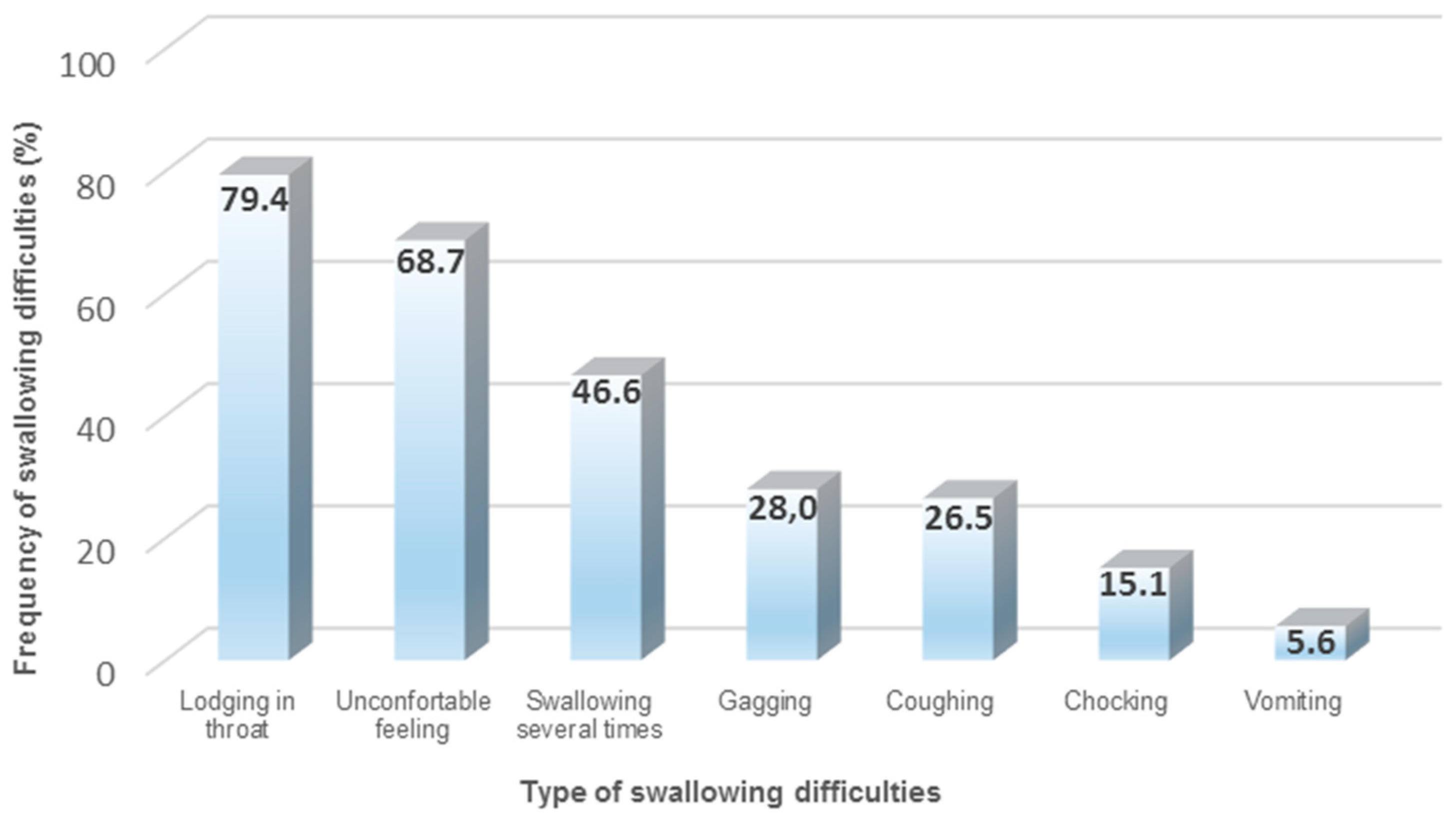
2.3. Perception of Dysphagia by Older Patients
3. Administration of SODF by Older Patients
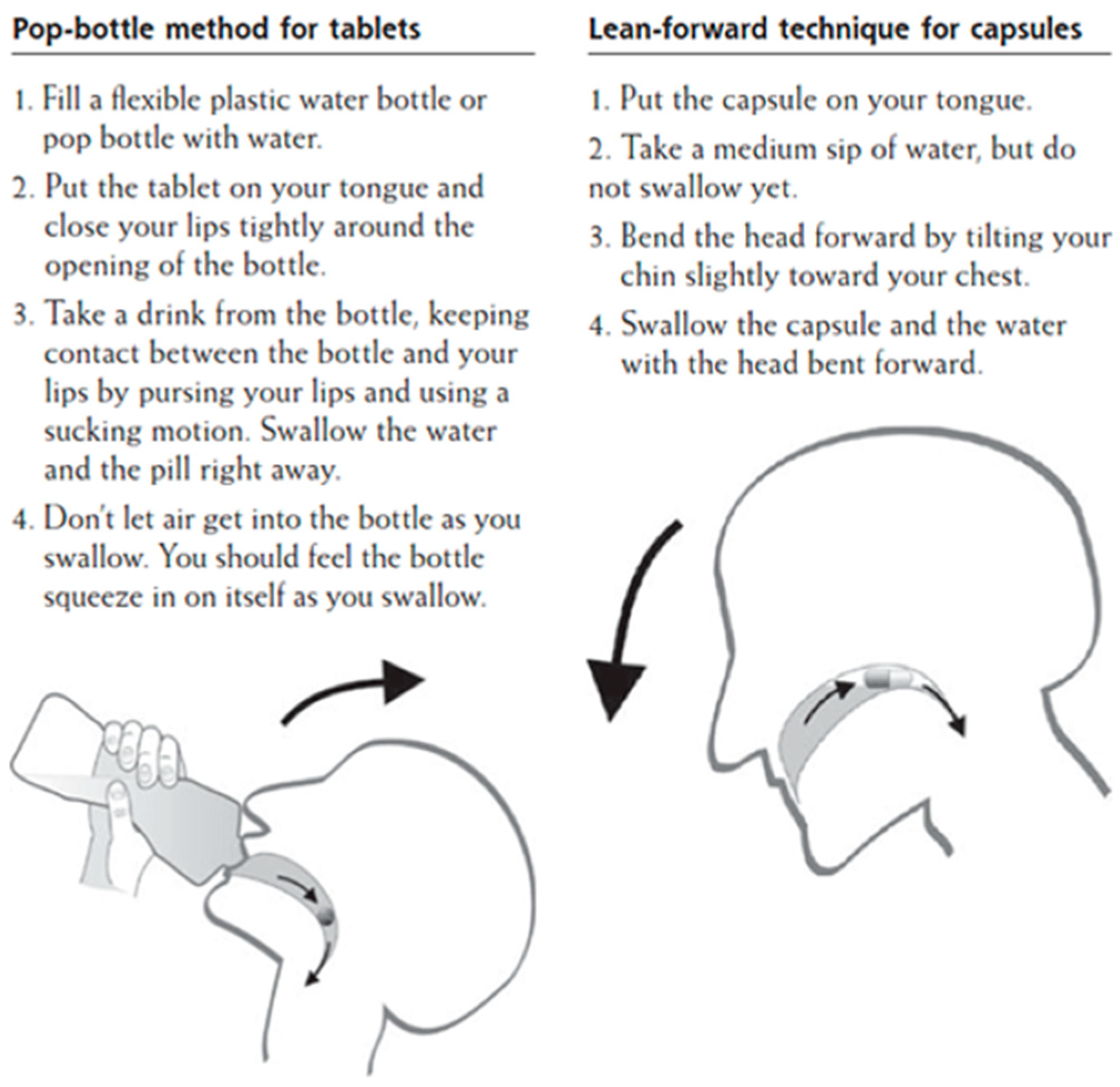
3.1. Conventional Administration Techniques to Improve Swallowability
3.2. Application of Administration Aids and Devices to Improve Swallowability
3.2.1. Oral Jellies
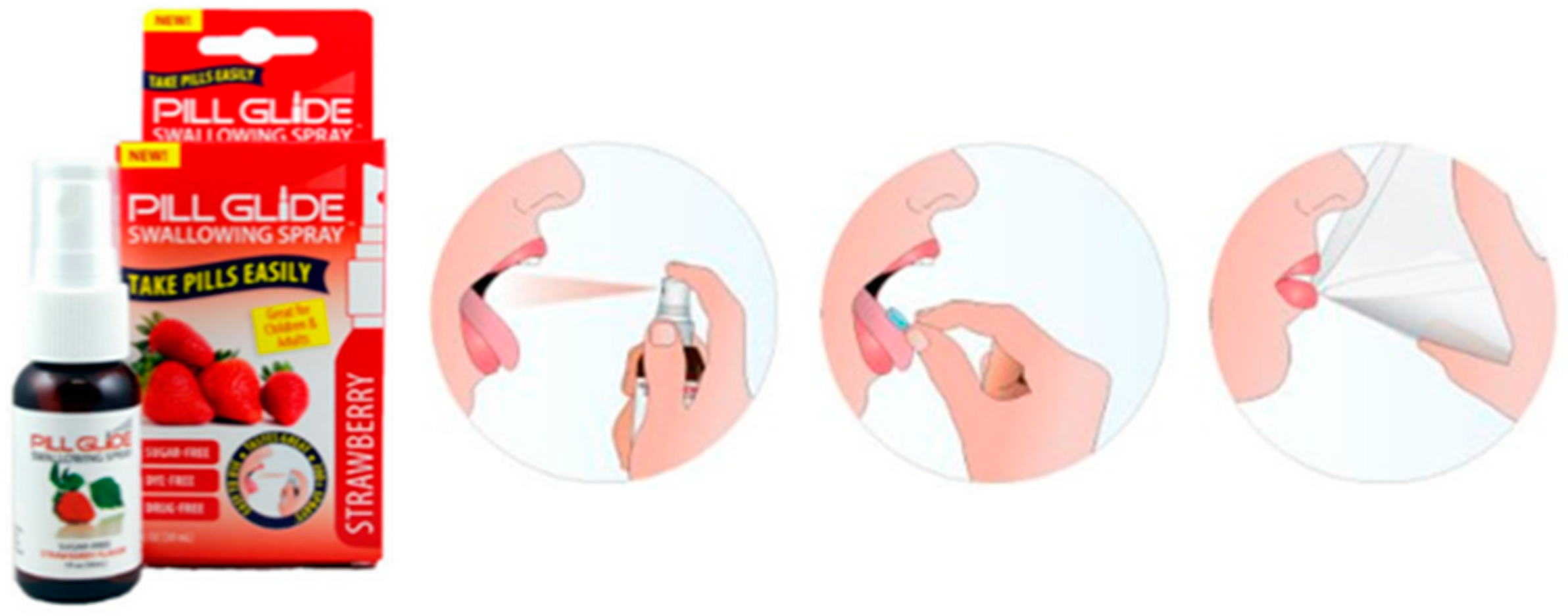
3.2.2. Pill Glide®
3.2.3. SODF Coating Devices
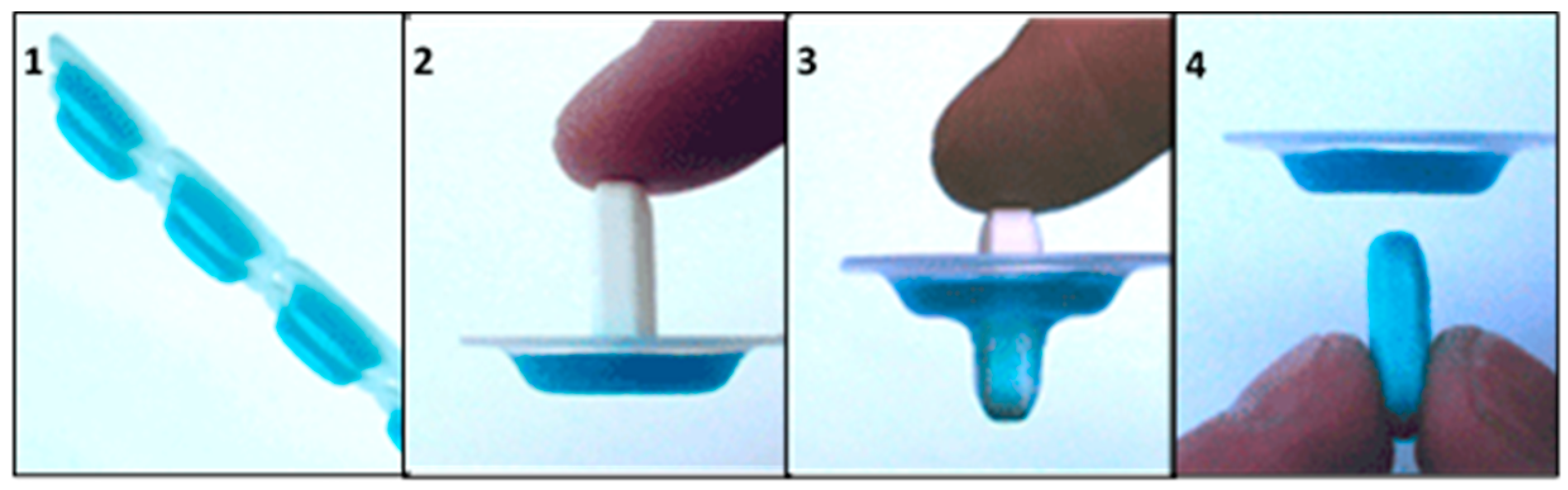
MedCoat®
Coating Container
3.3. Influence of SODF Design on Patients’ Adherence and Swallowing Experience
3.3.1. Color
3.3.2. Size
3.3.3. Shape
3.3.4. Taste and Smell
3.3.5. Density
3.3.6. Surface Characteristics
4. Development of SODF for Older Patients Requires a Patient Centric Drug Product Design Approach
5. Film Coating Materials Designed to Enhance SODF Swallowing Experience
5.1. Selection Process and Obtained Results
5.1.1. Polyvinyl Alcohol-Based Coatings (PVA)
5.1.2. Cellulose-Based Coatings
5.1.3. Gum-Based Coatings
5.1.4. Gelatin-Based Coatings
5.1.5. Sodium Alginate-Based Coatings
5.1.6. Wax-Based Coatings
5.1.7. Shellac-Based Coatings
5.1.8. Polyacrylate-Based Coatings
5.1.9. Polyethylene Oxide-Based Coatings
5.1.10. Carrageenan-Based Coatings
5.1.11. Polysaccharide-Based Coatings
5.2. Clinical Evidence of Proposed Coating Compositions for Enhanced Swallowability
6. Reflections on Available Administration Aids and Devices to Enhance SODF Swallowability in Older Patient Populations
7. Reflections on Identified Film Coating Materials to Enhance SODF Swallowability in Older Patient Populations
8. Concluding Remarks
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stegemann, S.; Gosch, M.; Breitkreutz, J. Swallowing dysfunction and dysphagia is an unrecognized challenge for oral drug therapy. Int. J. Pharm. 2012, 430, 197–206. [Google Scholar] [CrossRef]
- Perrie, Y.; Badhan, R.K.S.; Kirby, D.; Lowry, D.; Mohammed, A.R.; Ouyang, D. The impact of ageing on the barriers to drug delivery. J. Control. Release 2012, 161, 389–398. [Google Scholar] [CrossRef]
- Galato, D.; Da Silva, E.S.; Tiburcio, L.D.S. Study of the use of medicine in elderly living in a city in the South of Santa Catarina (Brazil): A look at the polymedication. Cien. Saude Colet. 2010, 15, 2899–2905. [Google Scholar] [CrossRef] [PubMed]
- Husson, N.; Watfa, G.; Laurain, M.-C.; Perret-Guillaume, C.; Niemier, J.-Y.; Miget, P.; Benetos, A. Characteristics of polymedicated (≥4) elderly: A survey in a community-dwelling population aged 60 years and over. J. Nutr. Heal. Aging 2014, 18, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, M.; Taylor, D. Solid oral dosage forms. Prof. Nurse 1993, 8, 313–317. [Google Scholar] [PubMed]
- Domb, A.J.; Khan, W. Focal Controlled Drug Delivery; Springer: New York, NY, USA, 2014. [Google Scholar]
- Forough, A.S.; Lau, E.T.; Steadman, K.J.; Cichero, J.A.; Kyle, G.J.; Santos, J.M.S.; Nissen, L. A spoonful of sugar helps the medicine go down? A review of strategies for making pills easier to swallow. Patient Prefer. Adherence 2018, 12, 1337–1346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, F.; Ghaffur, A.; Bains, J.; Hamdy, S. Acceptability of oral solid medicines in older adults with and without dysphagia: A nested pilot validation questionnaire based observational study. Int. J. Pharm. 2016, 512, 374–381. [Google Scholar] [CrossRef] [Green Version]
- Barczi, S.R.; Sullivan, P.A.; Robbins, J. How Should Dysphagia Care of Older Adults Differ? Establishing Optimal Practice Patterns. Semin. Speech Lang. 2000, 21, 347–364. [Google Scholar] [CrossRef]
- Leder, S.B.; Suiter, D.M. An Epidemiologic Study on Aging and Dysphagia in the Acute Care Hospitalized Population: 2000–2007. Gerontology 2009, 55, 714–718. [Google Scholar] [CrossRef]
- Nicosia, M.A.; Hind, J.A.; Roecker, E.B.; Carnes, M.; Doyle, J.; Dengel, G.A.; Robbins, J. Age Effects on the Temporal Evolution of Isometric and Swallowing Pressure. J. Gerontol. Ser. A Biol. Sci. Med Sci. 2000, 55, M634–M640. [Google Scholar] [CrossRef]
- Ekberg, O.; Olsson, R.; Hindfelt, B. Quantitative aspects of swallowing in an elderly nondysphagic population. Dysphagia 1996, 11, 180–184. [Google Scholar] [CrossRef]
- Barer, D.H. The natural history and functional consequences of dysphagia after hemispheric stroke. J. Neurol. Neurosurg. Psychiatry 1989, 52, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Calcagno, P.; Ruoppolo, G.; Grasso, M.G.; De Vincentiis, M.; Paolucci, S. Dysphagia in multiple sclerosis—prevalence and prognostic factors. Acta Neurol. Scand. 2002, 105, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Coates, C.; Bakheit, A.M. Dysphagia in Parkinson’s disease. Eur. Neurol. 1997, 38, 49–52. [Google Scholar] [CrossRef]
- De Pauw, A.; Dejaeger, E.; D’Hooghe, B.; Carton, H. Dysphagia in multiple sclerosis. Clin. Neurol. Neurosurg. 2002, 104, 345–351. [Google Scholar] [CrossRef]
- Gordon, C.; Hewer, R.L.; Wade, D.T. Dysphagia in acute stroke. Br. Med. J. 1987, 295, 411–414. [Google Scholar] [CrossRef] [Green Version]
- Mann, G.; Hankey, G.J.; Cameron, D. Swallowing function after stroke: Prognostic factors at months. Stroke 1999, 30, 744–748. [Google Scholar] [CrossRef]
- Spechler, S.J. AGA technical review on treatment of patients with dysphagia caused by benign disorders of the distal esophagus. Gastroenterology 1999, 117, 233–254. [Google Scholar] [CrossRef]
- Daniels, S.K. Neurological disorders affecting oral, pharyngeal swallowing. GI Motil. Online 2006. [Google Scholar] [CrossRef]
- Alvarenga, K.D.F.; Vicente, L.C.; Lopes, R.C.F.; Ventura, L.M.P.; Bevilacqua, M.C.; Moret, A.L.M.; Bassi, D.; Furkim, A.M.; Silva, C.A.; Coelho, M.S.P.H.; et al. Identification of risk groups for oropharyngeal dysphagia in hospitalized patients in a university hospital. CoDAS 2014, 26, 17–27. [Google Scholar] [CrossRef]
- Kendall, K.A.; Leonard, R.J.; McKenzie, S. Common medical conditions in the elderly: Impact on pharyngeal bolus transit. Dysphagia 2004, 19, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.B.; Drennan, J.C.; Baba, M. Evaluation and treatment of swallowing impairments. Am. Fam. Physician 2000, 61, 2453–2462. [Google Scholar] [PubMed]
- Balzer, K.M. Drug-Induced Dysphagia. Int. J. MS Care 2000, 2, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Page, S.; Coupe, A.; Barrett, A. An industrial perspective on the design and development of medicines for older patients. Int. J. Pharm. 2016, 512, 352–354. [Google Scholar] [CrossRef] [PubMed]
- Vallet, T.; Michelon, H.; Orlu, M.; Jani, Y.; Leglise, P.; Laribe-Caget, S.; Piccoli, M.; Le Fur, A.; Liu, F.; Ruiz, F.; et al. Acceptability in the Older Population: The Importance of an Appropriate Tablet Size. Pharmaceutics 2020, 12, 746. [Google Scholar] [CrossRef] [PubMed]
- Forster, A.; Samaras, N.; Gold, G.; Samaras, D. Oropharyngeal dysphagia in older adults: A review. Eur. Geriatr. Med. 2011, 2, 356–362. [Google Scholar] [CrossRef]
- Crary, M.A.; Sura, L.; Madhavan, A.; Carnaby-Mann, G. Dysphagia in the elderly: Management and nutritional considerations. Clin. Interv. Aging 2012, 7, 287–298. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.L.; Park, G.-Y.; Kwon, D.R.; Kwon, D.Y.; Kwak, S.G.; Cho, H.K. Airway invasion in non-neurologically ill patients with dysphagia: Contributing factors and associated problems during swallowing process. A retrospective observational study. Medicine 2020, 99, e22977. [Google Scholar] [CrossRef]
- Wilkins, T.; Gillies, R.A.; Thomas, A.M.; Wagner, P.J. The Prevalence of Dysphagia in Primary Care Patients: A HamesNet Research Network Study. J. Am. Board Fam. Med. 2007, 20, 144–150. [Google Scholar] [CrossRef]
- Masilamoney, M.; Dowse, R. Knowledge and practice of healthcare professionals relating to oral medicine use in swallowing-impaired patients: A scoping review. Int. J. Pharm. Pr. 2018, 26, 199–209. [Google Scholar] [CrossRef] [Green Version]
- Sestili, M.; Logrippo, S.; Cespi, M.; Bonacucina, G.; Ferrara, L.; Busco, S.; Grappasonni, I.; Palmieri, G.F.; Ganzetti, R.; Blasi, P. Potentially Inappropriate Prescribing of Oral Solid Medications in Elderly Dysphagic Patients. Pharmaceutics 2018, 10, 280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marquis, J.; Schneider, M.-P.; Payot, V.; Cordonier, A.-C.; Bugnon, O.; Hersberger, K.E.; Arnet, I. Swallowing difficulties with oral drugs among polypharmacy patients attending community pharmacies. Int. J. Clin. Pharm. 2013, 35, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Schiele, J.T.; Quinzler, R.; Klimm, H.-D.; Pruszydlo, M.G.; Haefeli, W.E. Difficulties swallowing solid oral dosage forms in a general practice population: Prevalence, causes, and relationship to dosage forms. Eur. J. Clin. Pharmacol. 2013, 69, 937–948. [Google Scholar] [CrossRef] [PubMed]
- Ekberg, O.; Hamdy, S.; Woisard, V.; Wuttge-Hannig, A.; Ortega, P. Social and Psychological Burden of Dysphagia: Its Impact on Diagnosis and Treatment. Dysphagia 2002, 17, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, N. The Prevalence of Dysphagia among Adults in the United States. Otolaryngol. Neck Surg. 2014, 151, 765–769. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Kaplan, D. Aspiration Pneumonia and Dysphagia in the Elderly. Chest 2003, 124, 328–336. [Google Scholar] [CrossRef]
- Pauloski, B.R.; Rademaker, A.; Logemann, J.A.; Lazarus, C.; Newman, L.; Ma, A.H.; Ms, E.M.; Gaziano, J.; Ms, L.S. Swallow function and perception of dysphagia in patients with head and neck cancer. Head Neck 2002, 24, 555–565. [Google Scholar] [CrossRef]
- Starmer, H.M.; Riley, L.H.; Hillel, A.T.; Akst, L.M.; Best, S.R.; Gourin, C.G. Dysphagia, Short-Term Outcomes, and Cost of Care After Anterior Cervical Disc Surgery. Dysphagia 2013, 29, 68–77. [Google Scholar] [CrossRef]
- Sengupta, J. Esophageal sensory physiology. GI Motil. Online. 2006. [Google Scholar] [CrossRef]
- Stoschus, B.; Allescher, H.-D. Drug-induced dysphagia. Dysphagia 1993, 8, 154–159. [Google Scholar] [CrossRef]
- Fields, J.; Go, J.T.; Schulze, K.S. Pill Properties that Cause Dysphagia and Treatment Failure. Curr. Ther. Res. 2015, 77, 79–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bott, S.; Prakash, C.; McCallum, R.W. Medication-induced esophageal injury: Survey of the literature. Am. J. Gastroenterol. 1987, 82, 758–763. [Google Scholar] [PubMed]
- Jaspersen, D. Drug-induced oesophageal disorders: Pathogenesis, incidence, prevention and management. Drug Saf. 2000, 22, 237–249. [Google Scholar] [CrossRef]
- Bálint, A.; Balázs, P.; Bátorfi, J.; Fazekas, T.; Réfi, M.; Ihász, M. Study on dysphagia after proximal selective vagotomy. Acta Chir. Hung. 1991, 32, 341–345. [Google Scholar] [PubMed]
- Newton, H.B.; Newton, C.; Pearl, D.; Davidson, T. Swallowing assessment in primary brain tumor patients with dysphagia. Neurol. 1994, 44, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- Witterick, I.J.; Gullane, P.J.; Yeung, E. Outcome analysis of Zenker’s diverticulectomy and cricopharyngeal myotomy. Head Neck 1995, 17, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Anselmino, M.; Zaninotto, G.; Costantini, M.; Ostuni, P.; Ianniello, A.; Boccú, C.; Doria, A.; Todesco, S.; Ancona, E. Esophageal motor function in primary Sjögren’s syndrome: Correlation with dysphagia and xerostomia. Dig. Dis. Sci. 1997, 42, 113–118. [Google Scholar] [CrossRef]
- Nathadwarawala, K.M.; McGroary, A.; Wiles, C.M. Swallowing in neurological outpatients: Use of a timed test. Dysphagia 1994, 9, 120–129. [Google Scholar] [CrossRef]
- Rhodus, N.L.; Colby, S.; Moller, K.; Bereuter, J. Quantitative assessment of dysphagia in patients with primary and secondary Sjögren’s syndrome. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 1995, 79, 305–310. [Google Scholar] [CrossRef]
- Rogus-Pulia, N.; Pierce, M.C.; Mittal, B.B.; Zecker, S.G.; Logemann, J.A. Changes in Swallowing Physiology and Patient Perception of Swallowing Function Following Chemoradiation for Head and Neck Cancer. Dysphagia 2014, 29, 223–233. [Google Scholar] [CrossRef]
- Heppner, H.J.; Sieber, C.C.; Esslinger, A.S.; Trögner, J. Drug administration and dosage forms in geriatric patients. Ther. Umsch. 2006, 63, 419–422. [Google Scholar] [CrossRef]
- Nunn, T.; Williams, J. Formulation of medicines for children. Br. J. Clin. Pharmacol. 2005, 59, 674–676. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Philip, A.K.; Pathak, K. Optimization Studies on Design and Evaluation of Orodispersible Pediatric Formulation of Indomethacin. AAPS PharmSciTech 2008, 9, 60–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logrippo, S.; Ricci, G.; Sestili, M.; Cespi, M.; Ferrara, L.; Palmieri, G.F.; Ganzetti, R.; Bonacucina, G.; Blasi, P. Oral drug therapy in elderly with dysphagia: Between a rock and a hard place. Clin. Interv. Aging 2017, 12, 241–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahaineh, L.M.; Al-Wazaify, M. Difficulties in swallowing oral medications in Jordan. Int. J. Clin. Pharm. 2017, 39, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Carnaby-Mann, G.; Crary, M. Pill Swallowing by Adults with Dysphagia. Arch. Otolaryngol. Head Neck Surg. 2005, 131, 970–975. [Google Scholar] [CrossRef] [Green Version]
- Andersen, O.; Zweidorff, O.K.; Hjelde, T.; Rødland, E.A. Problems when swallowing tablets. A questionnaire study from general practice. Tidsskr. Den Nor. Legeforening 1995, 115, 947–949. [Google Scholar]
- Kikendall, J.W. Pill-induced esophageal injury. Gastroenterol. Clin. N. Am. 1991, 20, 835–846. [Google Scholar] [CrossRef]
- Llorca, P.M. Discussion of prevalence and management of discomfort when swallowing pills: Orodispersible tablets expand treatment options in patients with depression. Ther. Deliv. 2011, 2, 611–622. [Google Scholar] [CrossRef]
- Simpson, S.H.; Eurich, D.T.; Majumdar, S.R.; Padwal, R.S.; Tsuyuki, R.T.; Varney, J.; Johnson, J.A. A meta-analysis of the association between adherence to drug therapy and mortality. BMJ 2006, 333, 15. [Google Scholar] [CrossRef] [Green Version]
- Kirkevold, Ø.; Engedal, K. What is the matter with crushing pills and opening capsules? Int. J. Nurs. Pr. 2010, 16, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Paradiso, L.M.; Roughead, E.; Gilbert, A.L.; Cosh, D.; Nation, R.L.; Barnes, L.; Cheek, J.; Ballantyne, A. Crushing or altering medications: What’s happening in residential aged-care facilities? Australas. J. Ageing 2002, 21, 123–127. [Google Scholar] [CrossRef]
- Van Welie, S.; Wijma, L.; Beerden, T.; Van Doormaal, J.; Taxis, K. Effect of warning symbols in combination with education on the frequency of erroneously crushing medication in nursing homes: An uncontrolled before and after study. BMJ Open 2016, 6, e012286. [Google Scholar] [CrossRef] [PubMed]
- Oberoi, R.K.; Zhao, W.; Sidhu, D.S.; Viani, R.M.; Trinh, R.; Liu, W. A Phase 1 Study to Evaluate the Effect of Crushing, Cutting Into Half, or Grinding of Glecaprevir/Pibrentasvir Tablets on Exposures in Healthy Subjects. J. Pharm. Sci. 2018, 107, 1724–1730. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.T.L.; Steadman, K.J.; Cichero, J.A.; Nissen, L. Dosage form modification and oral drug delivery in older people. Adv. Drug Deliv. Rev. 2018, 135, 75–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, J.; D’Cruz, G.; Wright, D. Patients with dysphagia: Experiences of taking medication. J. Adv. Nurs. 2010, 66, 82–91. [Google Scholar] [CrossRef] [PubMed]
- Schier, J.G.; Howland, M.A.; Hoffman, R.S.; Nelson, L. Fatality from Administration of Labetalol and Crushed Extended-Release Nifedipine. Ann. Pharmacother. 2003, 37, 1420–1423. [Google Scholar] [CrossRef]
- Griffith, R.; Tengnah, C. A guideline for managing medication related dysphagia. Br. J. Community Nurs. 2007, 12, 426–429. [Google Scholar] [CrossRef]
- Fowler, J.F. A helpful aid for pill swallowing: The pop-bottle method. Cutis 1986, 37, 461. [Google Scholar]
- MacLeod, A.D.; Vella-Brincat, J.; Frampton, C. Swallowing capsules. Palliat. Med. 2003, 17, 559. [Google Scholar] [CrossRef]
- Schiele, J.T.; Schneider, H.; Quinzler, R.; Reich, G.; Haefeli, W.E. Two Techniques to Make Swallowing Pills Easier. Ann. Fam. Med. 2014, 12, 550–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakuma, T.; Kida, I. Relationship between Ease of Swallowing and Deglutition-Related Muscle Activity in Various Postures. J. Oral Rehabil. 2010, 37, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.H.; Zafar, H.; Al-Eisa, E.S.; Iqbal, Z.A. Effect of posture on swallowing. Afr. Health Sci. 2017, 17, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Channer, K.S.; Virjee, J.P. The effect of formulation on oesophageal transit. J. Pharm. Pharmacol. 1985, 37, 126–129. [Google Scholar] [CrossRef]
- Channer, K.S.; Virjee, J.P. The Effect of Size and Shape of Tablets on Their Esophageal Transit. J. Clin. Pharmacol. 1986, 26, 141–146. [Google Scholar] [CrossRef]
- Manrique, Y.J.; Sparkes, A.M.; Cichero, J.A.; Stokes, J.R.; Nissen, L.; Steadman, K.J. Oral medication delivery in impaired swallowing: Thickening liquid medications for safe swallowing alters dissolution characteristics. Drug Dev. Ind. Pharm. 2016, 42, 1537–1544. [Google Scholar] [CrossRef] [Green Version]
- Malouh, M.A.; Cichero, J.A.; Manrique, Y.J.; Crino, L.; Lau, E.T.L.; Nissen, L.; Steadman, K.J. Are Medication Swallowing Lubricants Suitable for Use in Dysphagia? Consistency, Viscosity, Texture, and Application of the International Dysphagia Diet Standardization Initiative (IDDSI) Framework. Pharmaceutics 2020, 12, 924. [Google Scholar] [CrossRef]
- Oh, E.; Jee, S.; Kim, B.K.; Lee, J.S.; Cho, K.; Ahn, S.Y. A new swallowing supplement for dysphagia in patients with Parkinson’s disease. Neurol. Sci. 2020. [Google Scholar] [CrossRef]
- Patel, S.; Scott, N.; Patel, K.; Mohylyuk, V.; McAuley, W.J.; Liu, F. Easy to Swallow “Instant” Jelly Formulations for Sustained Release Gliclazide Delivery. J. Pharm. Sci. 2020, 109, 2474–2484. [Google Scholar] [CrossRef]
- Harada, T.; Yasuoka, K.; Sakurai, M.; Murase, T.; Owaki, T. Development of a Novel Oral Jelly Formulation for Elderly Patients. Yakugaku Zasshi 2015, 135, 249–254. [Google Scholar] [CrossRef] [Green Version]
- Satyanarayana, D.A.; Kulkarni, P.K.; Shivakumar, H.G. Gels and Jellies as a Dosage Form for Dysphagia Patients: A Review. Curr. Drug Ther. 2011, 6, 79–86. [Google Scholar] [CrossRef]
- Sadamoto, K.; Mizoguchi, M.; Yamanouchi, T.; Morimoto, S.; Kubota, K. Innovative Tool for Taking Large Pills for the Elderly and Patients with Swallowing Difficulties. Pharma Innov. 2012, 1, 1–6. [Google Scholar]
- Guomin, Y.; Bao, Q.R.; Xia, Z.; Fa-Ming, Z.; Jingfang, X.; Rong, Q.; ZhengYu, T.; Gang, D.; MingHui, W. Gel for Assisting Swallow of Oral Solid Medicinal Preparation. CN103721264A, 16 April 2014. [Google Scholar]
- Morimoto, S.; Sakuma, Y. Device for Oral Drug Administration. WO2014064840A1, 1 May 2014. [Google Scholar]
- Craig, D.; Wright, D.; Mencarelli, G.; Rogerson, M. Composition and Method for Assisting Swallowing. WO2009098520A2, 13 August 2009. [Google Scholar]
- Diamond, S.; Lavallee, D.C. Experience With a Pill-Swallowing Enhancement Aid. Clin. Pediatr. 2010, 49, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Uloza, V.; Uloziene, I.; Gradauskiene, E. A randomized cross-over study to evaluate the swallow-enhancing and taste-masking properties of a novel coating for oral tablets. Pharm. World Sci. 2010, 32, 420–423. [Google Scholar] [CrossRef]
- Lenk, L.A. Anti-Stick Formula Delivered by Spray Process to Facilitate Swallowing of Solid Object, such as Pill, Tablet, Capsule, or Caplet. US2007275053A1, 26 May 2007. [Google Scholar]
- Axelsson, J.; Lilieblad, F. A New Coating Composition and Use Thereo. WO2010085195A2, 29 July 2010. [Google Scholar]
- Nappi, B. Pill Coating Apparatus and Method. US2018311108A1, 2 August 2018. [Google Scholar]
- Gaskell, C. Use of Pill Glide to Encourage Transition from Liquid to Solid Dosage Formulations. Arch. Dis. Child. 2016, 101, e2. [Google Scholar] [CrossRef]
- Jagani, M.; Legay, H.; Ranmal, S.R.; Bertrand, J.; Ooi, K.; Tuleu, C. Can a Flavored Spray (Pill Glide) Help Children Swallow Their Medicines? A Pilot Study. Pediatrics 2016, 138, e20160680. [Google Scholar] [CrossRef] [Green Version]
- Pill Glide, Swallowing Spray, FAQ. 2009. Available online: http://pillglide.com/faq.asp (accessed on 15 December 2020).
- Axelsson, J. MedCoat AB, Products. 2002. Available online: http://www.medcoat.com/indexCor.htm (accessed on 15 December 2020).
- McDonald, H.P.; Garg, A.X.; Haynes, R.B. Interventions to enhance patient adherence to medication prescriptions: Scientific review. JAMA 2002, 288, 2868–2879. [Google Scholar] [CrossRef]
- Brotherman, D.P.; Bayraktaroglu, T.O.; Garofalo, R.J. Comparison of ease of swallowing of dietary supplement products for age-related eye disease. J. Am. Pharm. Assoc. 2004, 44, 587–593. [Google Scholar] [CrossRef]
- Tucker, C.; Fennell, R.S.; Pedersen, T.; Higley, B.P.; Wallack, C.E.; Peterson, S. Associations with medication adherence among ethnically different pediatric patients with renal transplants. Pediatr. Nephrol. 2002, 17, 251–256. [Google Scholar] [CrossRef]
- Yoder, S.; Rajabi, J.; Miller, C.; Oza, K. Physical Appearance Preferences for Oral Solid Dosage Formulations. 2014. Available online: https://www.colorcon.com/search/download/348/633/34?method=view (accessed on 15 December 2020).
- U.S. Department of Health and Human Services Food; Drug Administration (CDER). Guidance for Industry. Size, Shape and Other Physical Attributes of Generic Tablets and Capsules. 2013. Available online: https://www.fda.gov/media/87344/download (accessed on 15 December 2020).
- Yamamoto, S.; Taniguchi, H.; Hayashi, H.; Hori, K.; Tsujimura, T.; Nakamura, Y.; Sato, H.; Inoue, M. How do tablet properties influence swallowing behaviors? J. Pharm. Pharmacol. 2014, 66, 32–39. [Google Scholar] [CrossRef]
- Srivastava, R.; More, A.T. Some aesthetic considerations for over the-counter (OTC) pharmaceutical products. Int. J. Biotechnol. 2010, 11, 267. [Google Scholar] [CrossRef]
- Kesselheim, A.S.; Misono, A.S.; Shrank, W.H.; Greene, J.A.; Doherty, M.; Avorn, J.; Choudhry, N.K. Variations in Pill Appearance of Antiepileptic Drugs and the Risk of Nonadherence. JAMA Intern. Med. 2013, 173, 202–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hey, H.; Jorgensen, F.; Sorensen, K.; Hasselbalch, H.; Wamberg, T. Oesophageal transit of six commonly used tablets and capsules. BMJ 1982, 285, 1717–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mangoni, A.A.; Jackson, S.H.D. Age-related changes in pharmacokinetics and pharmacodynamics: Basic principles and practical applications. Br. J. Clin. Pharmacol. 2004, 57, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Overgaard, A.; Møller-Sonnergaard, J.; Christrup, L.L.; Højsted, J.; Hansen, R. Patients’ evaluation of shape, size and colour of solid dosage forms. Pharm. World Sci. 2001, 23, 185–188. [Google Scholar] [CrossRef]
- Miura, H.; Kariyasu, M. Effect of size of tablets on easiness of swallowing and handling among the frail elderly. Nippon. Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2007, 44, 627–633. [Google Scholar] [CrossRef] [Green Version]
- Becker, K.; Saurugger, E.-M.; Kienberger, D.; Lopes, D.; Haack, D.; Köberle, M.; Stehr, M.; Lochmann, D.; Zimmer, A.; Salar-Behzadi, S. Advanced stable lipid-based formulations for a patient-centric product design. Int. J. Pharm. 2016, 497, 136–149. [Google Scholar] [CrossRef]
- Stegemann, S. Towards better understanding of patient centric drug product development in an increasingly older patient population. Int. J. Pharm. 2016, 512, 334–342. [Google Scholar] [CrossRef]
- Du Plessis, D.; Sake, J.-K.; Halling, K.; Morgan, J.; Georgieva, A.; Bertelsen, N. Patient Centricity and Pharmaceutical Companies: Is It Feasible? Ther. Innov. Regul. Sci. 2017, 51, 460–467. [Google Scholar] [CrossRef]
- Liu, F.; Ranmal, S.; Batchelor, H.K.; Orlu-Gul, M.; Ernest, T.B.; Thomas, I.W.; Flanagan, T.; Tuleu, C. Patient-Centered Pharmaceutical Design to Improve Acceptability of Medicines: Similarities and Differences in Paediatric and Geriatric Populations. Drugs 2014, 74, 1871–1889. [Google Scholar] [CrossRef] [Green Version]
- European Medicines Agency. Reflection Paper on the Pharmaceutical Development of Medicines for Use in the Older Population. Available online: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2017/08/WC500232782.pdf (accessed on 15 December 2020).
- Van Riet-Nales, D.A.; Hussain, N.; Sundberg, K.A.; Eggenschwyler, D.; Ferris, C.; Robert, J.-L.; Cerreta, F. Regulatory incentives to ensure better medicines for older people: From ICH E7 to the EMA reflection paper on quality aspects. Int. J. Pharm. 2016, 512, 343–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, M.D.; Keeney, M.; Kleinberg, R.; Burlage, R. Challenges and Opportunities for Patient Centric Drug Product Design: Industry Perspectives. Pharm. Res. 2019, 36, 85. [Google Scholar] [CrossRef] [PubMed]
- Stegemann, S. Patient centric drug product design in modern drug delivery as an opportunity to increase safety and effectiveness. Expert Opin. Drug Deliv. 2018, 15, 619–627. [Google Scholar] [CrossRef] [PubMed]
- Radhakrishnan, A.; Kuppusamy, G.; Ponnusankar, S.; Shanmukhan, N.K. Pharmacogenomic phase transition from personalized medicine to patient-centric customized delivery. Pharm. J. 2019, 20, 1–18. [Google Scholar] [CrossRef]
- Hannan, P.A.; Khan, J.A.; Safiullah, S. Oral dispersible system: A new approach in drug delivery system. Indian J. Pharm. Sci. 2016, 78, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Rehman, A.; Bushra, R.; Beg, A.E.; Ali, H.; Zafar, F.; Ashfaq, M.; Alam, S.; Mustapha, O.; Shafique, S. Effects of superdisintegrants in oral dissolving formulation of cinitapride tablets. Pak. J. Pharm. Sci. 2018, 31, 643–650. [Google Scholar]
- Hesari, Z.; Shafiee, A.; Hooshfar, S.; Mobarra, N.; Mortazavi, S.A. Formulation and Taste Masking of Ranitidine Orally Disintegrating Tablet. Iran. J. Pharm. Res. 2016, 15, 677–686. [Google Scholar]
- Aslani, A.; Beigi, M. Design, formulation, and physicochemical evaluation of montelukast orally disintegrating tablet. Int. J. Prev. Med. 2016, 7, 120. [Google Scholar] [CrossRef]
- Chandrasekaran, P.; Kandasamy, R. Development of Oral Flexible Tablet (OFT) Formulation for Pediatric and Geriatric Patients: A Novel Age-Appropriate Formulation Platform. AAPS PharmSciTech 2016, 18, 1972–1986. [Google Scholar] [CrossRef]
- Sotoyama, M.; Uchida, S.; Kamiya, C.; Tanaka, S.; Kashiwagura, Y.; Hakamata, A.; Odagiri, K.; Inui, N.; Watanabe, H.; Namiki, N. Ease of Taking and Palatability of Fixed-Dose Orally Disintegrating Mitiglinide/Voglibose Tablets. Chem. Pharm. Bull. 2019, 67, 540–545. [Google Scholar] [CrossRef]
- Glezer on Behalf of the Optimum Program Participants MG. Evaluation of Antihypertensive Efficacy and Patient Adherence to Treatment with the New Formulation Perindopril Arginine (Orally Disintegrating Tablet) in General Clinical Practice: OPTIMUM Program. Kardiologiia 2016, 56, 36–41. [Google Scholar]
- Rustemkyzy, C.; Belton, P.; Qi, S. Preparation and Characterization of Ultrarapidly Dissolving Orodispersible Films for Treating and Preventing Iodine Deficiency in the Pediatric Population. J. Agric. Food Chem. 2015, 63, 9831–9838. [Google Scholar] [CrossRef] [PubMed]
- Schiele, J.T.; Penner, H.; Schneider, H.; Quinzler, R.; Reich, G.; Wezler, N.; Micol, W.; Oster, P.; Haefeli, W.E. Swallowing Tablets and Capsules Increases the Risk of Penetration and Aspiration in Patients with Stroke-Induced Dysphagia. Dysphagia 2015, 30, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Drumond, N. Future Perspectives for Patient-Centric Pharmaceutical Drug Product Design with Regard to Solid Oral Dosage Forms. J. Pharm. Innov. 2019, 15, 318–324. [Google Scholar] [CrossRef] [Green Version]
- Curtis, J.A.; Seikaly, Z.N.; Dakin, A.E.; Troche, M.S. Detection of Aspiration, Penetration, and Pharyngeal Residue During Flexible Endoscopic Evaluation of Swallowing (FEES): Comparing the Effects of Color, Coating, and Opacity. Dysphagia 2020. [Google Scholar] [CrossRef] [PubMed]
- Marconati, M.; Raut, S.; Burbidge, A.; Engmann, J.; Ramaioli, M. An in vitro experiment to simulate how easy tablets are to swallow. Int. J. Pharm. 2018, 535, 27–37. [Google Scholar] [CrossRef]
- Maalouf, N. Developing patient-centric drug formulations to meet patient needs. Business Dev Licens J. 2013, 20. [Google Scholar]
- Reeve, B.B.; Wyrwich, K.W.; Wu, A.W.; Velikova, G.; Terwee, C.; Snyder, C.F.; Schwartz, C.; Revicki, D.A.; Moinpour, C.M.; McLeod, L.D.; et al. ISOQOL recommends minimum standards for patient-reported outcome measures used in patient-centered outcomes and comparative effectiveness research. Qual. Life Res. 2013, 22, 1889–1905. [Google Scholar] [CrossRef]
- Hanning, S.M.; Lopez, F.; Wong, I.C.; Ernest, T.B.; Tuleu, C.; Orlu-Gul, M. Patient centric formulations for paediatrics and geriatrics: Similarities and differences. Int. J. Pharm. 2016, 512, 355–359. [Google Scholar] [CrossRef]
- Menditto, E.; Orlando, V.; De Rosa, G.; Minghetti, P.; Musazzi, U.M.; Cahir, C.; Kurczewska-Michalak, M.; Kardas, P.; Costa, E.; Sousa-Lobo, J.M.; et al. Patient Centric Pharmaceutical Drug Product Design—The Impact on Medication Adherence. Pharmaceutics 2020, 12, 44. [Google Scholar] [CrossRef] [Green Version]
- Timpe, C.; Stegemann, S.; Barrett, A.; Mujumdar, S. Challenges and opportunities to include patient-centric product design in industrial medicines development to improve therapeutic goals. Br. J. Clin. Pharmacol. 2020, 86, 2020–2027. [Google Scholar] [CrossRef] [PubMed]
- Goyanes, A.; Scarpa, M.; Kamlow, M.; Gaisford, S.; Basit, A.W.; Orlu, M. Patient acceptability of 3D printed medicines. Int. J. Pharm. 2017, 530, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Duggan, J.M.; Akpanudo, B.; Shukla, V.; Gutterson, G.; Eitniear, L.; Sahloff, E.G. Alternative antiretroviral therapy formulations for patients unable to swallow solid oral dosage forms. Am. J. Heal. Pharm. 2015, 72, 1555–1565. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Wrzesniewski, C.E.; Hasson, N.K. Integrating patient-centric indications into the prescribing process: Experience at a tertiary academic medical center. Am. J. Heal. Pharm. 2020, 77, S26–S33. [Google Scholar] [CrossRef] [PubMed]
- Govender, R.; Abrahmsén-Alami, S.; Larsson, A.; Folestad, S. Therapy for the individual: Towards patient integration into the manufacturing and provision of pharmaceuticals. Eur. J. Pharm. Biopharm. 2020, 149, 58–76. [Google Scholar] [CrossRef] [PubMed]
- Alshetaili, A.S.; Almutairy, B.K.; Tiwari, R.V.; Morott, J.T.; AlShehri, S.M.; Feng, X.; Alsulays, B.B.; Park, J.-B.; Zhang, F.; Repka, M.A. Preparation and Evaluation of Hot-Melt Extruded Patient-Centric Ketoprofen Mini-Tablets. Curr. Drug Deliv. 2016, 13, 730–741. [Google Scholar] [CrossRef]
- Freerks, L.; Sommerfeldt, J.; Löper, P.C.; Klein, S. Safe, swallowable and palatable paediatric mini-tablet formulations for a WHO model list of essential medicines for children compound—A promising starting point for future PUMA applications. Eur. J. Pharm. Biopharm. 2020, 156, 11–19. [Google Scholar] [CrossRef]
- Aleksovski, A.; Dreu, R.; Gašperlin, M.; Planinšek, O. Mini-tablets: A contemporary system for oral drug delivery in targeted patient groups. Expert Opin. Drug Deliv. 2015, 12, 65–84. [Google Scholar] [CrossRef]
- Chen, T.; Li, J.; Chen, T.; Sun, C.C.; Zheng, Y. Tablets of multi-unit pellet system for controlled drug delivery. J. Control. Release 2017, 262, 222–231. [Google Scholar] [CrossRef]
- Ito, I.; Ito, A.; Unezaki, S. Preparation and evaluation of gelling granules to improve oral administration. Drug Discov. Ther. 2015, 9, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Marconati, M.; Lopez, F.; Tuleu, C.; Orlu, M.; Ramaioli, M. In vitro and sensory tests to design easy-to-swallow multi-particulate formulations. Eur. J. Pharm. Sci. 2019, 132, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Mohylyuk, V.; Patel, K.; Scott, N.; Richardson, C.; Murnane, D.; Liu, F. Wurster Fluidised Bed Coating of Microparticles: Towards Scalable Production of Oral Sustained-Release Liquid Medicines for Patients with Swallowing Difficulties. AAPS PharmSciTech 2020, 21, 3. [Google Scholar] [CrossRef] [PubMed]
- Al-Hashimi, N.; Begg, N.; Alany, R.G.; Hassanin, H.; Elshaer, A. Oral Modified Release Multiple-Unit Particulate Systems: Compressed Pellets, Microparticles and Nanoparticles. Pharmaceutics 2018, 10, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofmanová, J.K.; Bennett, J.; Coupe, A.; Bartlett, J.A.; Monahan, A.; Batchelor, H. A Novel Oral Syringe for Dosing and Administration of Multiparticulate Formulations: Acceptability Study in Preschool and School Children. Pharmaceutics 2020, 12, 806. [Google Scholar] [CrossRef]
- Shariff, Z.; Kirby, D.; Missaghi, S.; Rajabi-Siahboomi, A.; Maidment, I.D. Patient-Centric Medicine Design: Key Characteristics of Oral Solid Dosage Forms that Improve Adherence and Acceptance in Older People. Pharmaceutics 2020, 12, 905. [Google Scholar] [CrossRef]
- Robbins, D.A.; Curro, F.A.; Fox, C.H. Defining Patient-Centricity: Opportunities, Challenges, and Implications for Clinical Care and Research. Ther. Innov. Regul. Sci. 2013, 47, 349–355. [Google Scholar] [CrossRef]
- Dille, M.J.; Hattrem, M.N.; Draget, K.I. Soft, chewable gelatin-based pharmaceutical oral formulations: A technical approach. Pharm. Dev. Technol. 2017, 23, 504–511. [Google Scholar] [CrossRef]
- Uddin, M.N.; Allon, A.; Roni, M.A.; Kouzi, S. Overview and Future Potential of Fast Dissolving Buccal Films as Drug Delivery System for Vaccines. J. Pharm. Pharm. Sci. 2019, 22, 388–406. [Google Scholar] [CrossRef]
- Kumar, T.P.; Gowda, D.V. Patent Perspective on Orodispersible Films. Recent Patents Drug Deliv. Formul. 2020, 14, 88–97. [Google Scholar] [CrossRef]
- Speer, I.; Lenhart, V.; Preis, M.; Breitkreutz, J. Prolonged release from orodispersible films by incorporation of diclofenac-loaded micropellets. Int. J. Pharm. 2019, 554, 149–160. [Google Scholar] [CrossRef]
- Smart, J.D.; Dunkley, S.; Tsibouklis, J.; Young, S.W. An in vitro model for the evaluation of the adhesion of solid oral dosage forms to the oesophagus. Int. J. Pharm. 2013, 447, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Drumond, N.; Stegemann, S. Polymer adhesion predictions for oral dosage forms to enhance drug administration safety. Part 1: In vitro approach using particle interaction methods. Colloids Surf. B Biointerfaces 2018, 165, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Drumond, N.; Stegemann, S. Polymer adhesion predictions for oral dosage forms to enhance drug administration safety. Part 2: In vitro approach using mechanical force methods. Colloids Surf. B Biointerfaces 2018, 166, 17–23. [Google Scholar] [CrossRef]
- Drumond, N.; Stegemann, S. Polymer adhesion predictions for oral dosage forms to enhance drug administration safety. Part 3: Review of in vitro and in vivo methods used to predict esophageal adhesion and transit time. Colloids Surf. B Biointerfaces 2018, 165, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Hofmanová, J.; Rajabi-Siahboomi, A.; Haque, S.; Mason, J.; Teckoe, J.; To, D.; Batchelor, H. Developing methodology to evaluate the oral sensory features of pharmaceutical tablet coatings. Int. J. Pharm. 2019, 562, 212–217. [Google Scholar] [CrossRef]
- Smart, J.D.; Dunkley, S.; Tsibouklis, J.; Young, S.W. An evaluation of the adhesion of solid oral dosage form coatings to the oesophagus. Int. J. Pharm. 2015, 496, 299–303. [Google Scholar] [CrossRef] [Green Version]
- Drumond, N.; Stegemann, S. An evaluation of the gliding performance of solid oral dosage form film coatings using an artificial mucous layer. Colloids Surf. B Biointerfaces 2019, 177, 235–241. [Google Scholar] [CrossRef]
- Khan, K.; Kunz, R.; Kleijnen, J.; Antes, G. Five steps to conducting a systematic review. J. R. Soc. Med. 2003, 96, 118–121. [Google Scholar] [CrossRef]
- Okabe, H.; Suzuki, E.; Sugiura, Y.; Yanagimoto, K.; Takanashi, Y.; Hoshi, M.; Nogami, E.; Nakahara, K.; Sekiguchi, T.; Baba, M.; et al. Development of an easily swallowed film formulation. Int. J. Pharm. 2008, 355, 62–66. [Google Scholar] [CrossRef]
- Ito, I.; Ito, A.; Unezaki, S. Investigation of Oral Preparation That Is Expected to Improve Medication Administration: Preparation and Evaluation of Oral Gelling Tablet Using Sodium Alginate. Yakugaku Zasshi 2017, 137, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Clark, W.N. Improvement in Soluble Coatings for Pills. US209654A, 5 November 1878. [Google Scholar]
- Secora, M.; Alvin, B.R. Pharmaceutical Tablets Coated with Wax-Free Amonia Solubilized Water Soluble Shellac. US3390049A, 25 June 1968. [Google Scholar]
- John, P.M.; Belanger, R.J.; Paikoff, M. Easily-Swallowed, Powder-Free and Gastric-Disintegrable Aspirin Tablet Thinly-Coated with Hydroxypropyl Methylcellulose and Aqueous Spray-Coating Preparation Thereof. US4302440A, 24 November 1981. [Google Scholar]
- Sato, M. Method of Making Solid Material Easily Swallowable. JPS61161215A, 21 July 1986. [Google Scholar]
- Tencza, T.M.; Patell, M. Thin Film Coated Tablets. CA1217140A, 27 January 1987. [Google Scholar]
- Becker, D. Gelatin Coated Tablets and Method For Producing Same. US5114720A, 19 May 1992. [Google Scholar]
- Imanishi, S. Medicine Coated with Gelatinizing Agent, Lubricating Agent And Lubricant. JPH09104621A, 22 April 1997. [Google Scholar]
- Gruber, P. Easy to Swallow Oral Medicament Composition. WO9806385A1, 19 February 1998. [Google Scholar]
- Nitsuto, S.; Sogawa, K.; Shirai, H.; Yamamura, S. Easily Administrable Solid Preparation. JP2002275054A, 25 September 2002. [Google Scholar]
- Flanagan, T.; Colegrove, G.; Nivaggioli, T. Gellan Gum Tablet Coating. US6395298B1, 28 May 2002. [Google Scholar]
- Flanagan, T.; Colegrove, G.; Nivaggioli, T. Gellan Gum Tablet Film Coating. US6635282B1, 21 October 2003. [Google Scholar]
- Tsukioka, T.; Nishimura, M.; Matsuura, K.; Sugiyama, T.; Katagiri, Y. Internal Medicine. JP2007070344A, 22 March 2007. [Google Scholar]
- Robertson, J.R. Solid Medicament Dosage form Consumption Aid. US20070259038A1, 8 November 2007. [Google Scholar]
- Kawasumi, S.; Saito, T. Easily-Swallowable Film-Coated Pharmaceutical Preparations Containing Antacids. JP2007015950A, 25 January 2007. [Google Scholar]
- Lincoln, E. Lubricious Coatings for Pharmaceutical Applications. US2007243246A1, 18 October 2007. [Google Scholar]
- Kata, A.; Suzuki, E.; Sugiura, Y. Film for Assisting Deglution, Hollow Film-Spliced Material for Assisting Deglution, and Method for Continuously Producing the Same. JP2009120497A, 4 June 2009. [Google Scholar]
- Kata, A.; Suzuki, E.; Sugiura, Y. Oral Administration Preparation. JP2010120877A, 3 June 2010. [Google Scholar]
- Fujioka, H.; Tsukuda, Y.; Shimaguchi, S.; Shiga, Y. Easily Swallowable Tablet. JP2011195569A, 6 October 2011. [Google Scholar]
- Chen, H.L. Oral Tablet. TW201121586A, 1 July 2011. [Google Scholar]
- Waldman, J. Tablet Sleeve for Improved Performance. WO2012024360A2, 23 February 2012. [Google Scholar]
- Yang, Y.; Shen, Z.; Guo, C.; Zhao, H. Novel Medicinal Outer Wrapper Facilitating Swallow. CN102652738A, 5 September 2012. [Google Scholar]
- Sugiura, Y.; Takano, Y. Adhesion Preventing Composition, Solid Preparation and Method for Producing Same. CN102361652A, 22 February 2012. [Google Scholar]
- Li, J.; Luo, J.; Zhang, C.; Liu, Y.; Liu, P. Pill Coating with Ultralow Friction Coefficient and Preparation Method Thereof. CN102430124A, 2 May 2012. [Google Scholar]
- Mizuhara, G.; Tomioka, S.; Miyata, T. Water-Swellable Laminated Film and Swallowable Substance-Coated Body. JP2014227391A, 8 December 2014. [Google Scholar]
- Takano, Y. Swallowable Film-Coated Body for Oral Drug Delivery. JP2014189547A, 6 October 2014. [Google Scholar]
- Yinjian, B. Coating Composition and Related Use Thereof. CN108543072A, 18 September 2018. [Google Scholar]
- Yinjian, B. Composition Used for Swallowing and Relevant Applications of Composition. CN108578704A, 28 September 2018. [Google Scholar]
- Jeffrey, R.G.; Jason, T.; Daniel, T. Easy to Swallow Coatings and Substrates Coated Therewith. US2018036413A1, 8 February 2018. [Google Scholar]
- Clavé, P.; Arreola, V.; Romea, M.; Medina, L.; Palomera, E.; Serra-Prat, M. Accuracy of the volume-viscosity swallow test for clinical screening of oropharyngeal dysphagia and aspiration. Clin. Nutr. 2008, 27, 806–815. [Google Scholar] [CrossRef] [PubMed]
- Suput, D.; Lazić, V.L.; Pezo, L.L.; Popovic, S.; Hromiš, N.; Bulut, S. The effects of glycerol and guar-xanthan mixture on mechanical and barrier properties of starch based edible films—chemometric analysis. Chem. Ind. 2016, 70, 739–744. [Google Scholar] [CrossRef]
- Schwartz, R.H. Enhancing children’s satisfaction with antibiotic therapy: A taste study of several antibiotic suspensions. Curr. Ther. Res. 2000, 61, 570–581. [Google Scholar] [CrossRef]
- Rahman, M.S. Handbook of Food Preservation, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Otoni, C.G.; Avena-Bustillos, R.J.; Azeredo, H.M.C.; Lorevice, M.V.; Moura, M.R.; Mattoso, L.H.; McHugh, T.H. Recent Advances on Edible Films Based on Fruits and Vegetables-A Review. Compr. Rev. Food Sci. Food Saf. 2017, 16, 1151–1169. [Google Scholar] [CrossRef] [Green Version]
- Sohi, H.; Sultana, Y.; Khar, R.K. Taste Masking Technologies in Oral Pharmaceuticals: Recent Developments and Approaches. Drug Dev. Ind. Pharm. 2004, 30, 429–448. [Google Scholar] [CrossRef] [Green Version]
- Satokawa, Y.; Shikata, T. Hydration Structure and Dynamic Behavior of Poly(vinyl alcohol)s in Aqueous Solution. Macromolecules 2008, 41, 2908–2913. [Google Scholar] [CrossRef]
- Al-Harthi, M.A.; Bin-Dahman, O.A.; De, S.K.; Jose, J. Poly(acrylic acid)-Glycerol Blends. US9346938B1, 24 May 2016. [Google Scholar]
- Stephen, A.; Phillips, G. (Eds.) Food Polysaccharides and Their Applications; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Yang, M.; Xie, S.; Li, Q.; Wang, Y.; Chang, X.; Shan, L.; Sun, L.; Huang, X.; Gao, C. Effects of polyvinylpyrrolidone both as a binder and pore-former on the release of sparingly water-soluble topiramate from ethylcellulose coated pellets. Int. J. Pharm. 2014, 465, 187–196. [Google Scholar] [CrossRef]
- Sahoo, R.; Dhanapal, K.; Reddy, G.; Arumugam, B.; Sravani, K. Study on The Functional Properties Of Gelatin Extracted From The Skin Of The Fish Pacu (Piaractus Brachypomus). Int. J. Innov. Sci. Eng. Technol. 2015, 2, 218–232. [Google Scholar]
- Zaikov, G. Chemistry of Polysaccharides; CRC Press: London, UK, 2005. [Google Scholar]
- Sánchez, V.; Bartholomai, G.; Pilosof, A. Rheological properties of food gums as related to their water binding capacity and to soy protein interaction. LWT 1995, 28, 380–385. [Google Scholar] [CrossRef]
- Dos Santos, M.A.; Grenha, A. Polysaccharide Nanoparticles for Protein and Peptide Delivery. In Advances in Protein Chemistry and Structural Biology; Academic Press: Cambridge, MA, USA, 2015; pp. 223–261. [Google Scholar] [CrossRef]
- Tracton, A. Coatings Materials and Surface Coatings; CRC Press: Boca Raton, FL, USA, 2006. [Google Scholar]
- Medina-Torres, L.; Calderas, F.; Sanchez-Olivares, G.; Nuñez-Ramirez, D.-M. Rheology of Sodium Polyacrylate as an Emulsifier Employed in Cosmetic Emulsions. Ind. Eng. Chem. Res. 2014, 53, 18346–18351. [Google Scholar] [CrossRef]
- Drumond, N.; Van Riet-Nales, D.A.; Karapinar-Çarkit, F.; Stegemann, S. Patients’ appropriateness, acceptability, usability and preferences for pharmaceutical preparations: Results from a literature review on clinical evidence. Int. J. Pharm. 2017, 521, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Vallet, T.; Belissa, E.; Laribe-Caget, S.; Chevallier, A.; Chedhomme, F.-X.; Leglise, P.; Piccoli, M.; Michelon, H.; Bloch, V.; Meaume, S.; et al. A Decision Support Tool Facilitating Medicine Design for Optimal Acceptability in The Older Population. Pharm. Res. 2018, 35, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shariff, Z.; Dahmash, D.T.; Kirby, D.J.; Missaghi, S.; Rajabi-Siahboomi, A.; Maidment, I.D. Does the Formulation of Oral Solid Dosage Forms Affect Acceptance and Adherence in Older Patients? A Mixed Methods Systematic Review. J. Am. Med Dir. Assoc. 2020, 21, 1015–1023.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belissa, E.; Vallet, T.; Laribe-Caget, S.; Chevallier, A.; Chedhomme, F.-X.; Abdallah, F.; Bachalat, N.; Belbachir, S.-A.; Boulaich, I.; Bloch, V.; et al. Acceptability of oral liquid pharmaceutical products in older adults: Palatability and swallowability issues. BMC Geriatr. 2019, 19, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Atkin, P.A.; Finnegan, T.P.; Ogle, S.J.; Shenfield, G.M. Functional Ability of Patients to manage Medication Packaging: A Survey of Geriatric Inpatients. Age Ageing 1994, 23, 113–116. [Google Scholar] [CrossRef]
- Dietlein, T.; Jordan, J.F.; Lüke, C.; Schild, A.; Dinslage, S.; Krieglstein, G.K. Self-application of single-use eyedrop containers in an elderly population: Comparisons with standard eyedrop bottle and with younger patients. Acta Ophthalmol. 2008, 86, 856–859. [Google Scholar] [CrossRef]
- Braun-Münker, M.; Ecker, F. Ease of opening of blistered solid dosage forms in a senior citizens target group. Int. J. Pharm. 2016, 512, 412–415. [Google Scholar] [CrossRef]
- Notenboom, K.; Beers, E.; Riet-Nales, D.A.; Egberts, T.C.G.; Leufkens, H.G.M.; Jansen, P.A.F.; Bouvy, M.L. Practical Problems with Medication Use that Older People Experience: A Qualitative Study. J. Am. Geriatr. Soc. 2014, 62, 2339–2344. [Google Scholar] [CrossRef] [Green Version]
- Stegemann, S.; Van Riet-Nales, D.A.; De Boer, A. Demographics in the 2020s—Longevity as a challenge for pharmaceutical drug development, prescribing, dispensing, patient care and quality of life. Br. J. Clin. Pharmacol. 2020, 86, 1899–1903. [Google Scholar] [CrossRef]
- Drumond, N.; Stegemann, S. An Investigation into the Relationship between Xanthan Gum Film Coating Materials and Predicted Oro-Esophageal Gliding Performance for Solid Oral Dosage Forms. Pharmaceutics 2020, 12, 1241. [Google Scholar] [CrossRef]
- Wahlich, J.; Orlu, M.; Mair, A.; Stegemann, S.; Van Riet-Nales, D.A. Age-Related Medicine. Pharmaceutics 2019, 11, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stegemann, S. Preventing aging and age-related diseases—A new era for drug repurposing. Am. Pharm. Rev. 2019, 22, 44–46. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Predisposition | Condition |
|---|---|
| Neurologic disorders and stroke | Cerebral infarction |
| Brain-stem infarction | |
| Intracranial hemorrhage | |
| Parkinson’s disease | |
| Multiple sclerosis | |
| Amyotrophic lateral sclerosis | |
| Poliomyelitis | |
| Myasthenia gravis | |
| Dementia | |
| Structural lesions | Thyromegaly |
| Cervical hyperostosis | |
| Congenital web | |
| Zenker’s diverticulum | |
| Ingestion of caustic material | |
| Neoplasm | |
| Psychiatric disorder | Psychogenic dysphagia |
| Connective tissue diseases | Polymyositis |
| Muscular dystrophy | |
| Iatrogenic causes | Surgical resection |
| Radiation fibrosis | |
| Medications |
| Physiological Condition | Class of Drugs |
|---|---|
| Sedation, pharyngeal weakness, dystonia | Benzodiazepines |
| Neuroleptics | |
| Anticonvulsants | |
| Myopathy | Corticosteroids |
| Lipid-lowering drugs | |
| Xerostomia | Anticholinergics |
| Antihypertensives | |
| Antihistamines | |
| Antipsychotics | |
| Narcotics | |
| Anticonvulsants | |
| Antiparkinsonian agents | |
| Antineoplastics | |
| Antidepressants | |
| Anxiolytics | |
| Muscle relaxants | |
| Diuretics | |
| Inflammation (from tablet irritation) | Tetracycline |
| Doxycycline | |
| Iron preparations | |
| Quinidine | |
| Nonsteroidal anti-inflammatory drugs | |
| Potassium | |
| Impaired motility or gastroesophageal reflux | Anticholinergics |
| Calcium channel blockers | |
| Theophylline | |
| Esophagitis (related to immunosuppression) | Corticosteroids |
| Authors | Title | Year | Reference |
|---|---|---|---|
| Diamond et al. | Experience with a pill-swallowing enhancement aid | 2010 | [87] |
| Uloza et al. | A randomized cross-over study to evaluate the swallow-enhancing and taste-masking properties of a novel coating for oral tablets | 2010 | [88] |
| Sadamoto et al. | Innovative Tool for Taking Large Pills for the Elderly and Patients with Swallowing Difficulties | 2012 | [83] |
| Author(s) | Patent Number | Related Invention | Year | Reference |
|---|---|---|---|---|
| L.A. Lenk | US2007275053A1 | Anti-stick formula delivered by spray process to facilitate swallowing of solid object, such as pill, tablet, capsule or caplet | 2007 | [89] |
| Craig et al. | WO2009098520A2 | Composition and method for assisting swallowing | 2009 | [86] |
| Axelsson et al. | WOUS2018311108 | A new coating composition and use thereof | 2010 | [90] |
| Guomin et al. | CN103721264A | Gel for assisting swallow of oral solid medicinal preparation | 2014 | [84] |
| Morimoto et al. | WO2014064840A1 | Device for oral drug administration | 2014 | [85] |
| Nappi Bryan | US2018311108A1 | Pill coating apparatus and method | 2018 | [91] |
| Priority Order | Inclusion | Exclusion |
|---|---|---|
| 1 | Oral drug delivery | Other routes for drug delivery |
| 2 | Capsules and tablets | Powders, granules, sachets, multiparticulates, effervescent tablets |
| 3 | Tablets swallowed intact (e.g., non-dispersible, bulk tablets) | Dispersible tablets (e.g., dispersible, effervescent, orodispersible) |
| 4 | Interventions to facilitate swallowing of tablets and capsules | Dosage form manipulations |
| 5 | Coatings to enhance swallowing of tablets and capsules | Other functional coatings |
| Authors | Title | Year | Reference |
|---|---|---|---|
| Okabe et al. | Development of an easily swallowed film formulation | 2008 | [161] |
| Ito et al. | Investigation of Oral Preparation That Is Expected to Improve Medication Administration: Preparation and Evaluation of Oral Gelling Tablet Using Sodium Alginate | 2017 | [162] |
| Author(s) | Patent Number | Year | Related Invention | Reference |
|---|---|---|---|---|
| William N. Clark | US209654A | 1878 | Improvement in soluble coatings for pills | [163] |
| Secora et al. | US3390049A | 1968 | Pharmaceutical tablets coated with wax-free ammonia solubilized water soluble shellac | [164] |
| John et al. | US4302440A | 1981 | Easily-swallowed aspirin tablet thinly-coated with HPMC and aqueous spray-coating preparation | [165] |
| Motoaki Sato | JPS61161215A | 1986 | Method of making solid material easily swallowable | [166] |
| Tencza et al. | CA1217140A | 1987 | Thin film coated tablets | [167] |
| Becker et al. | US5114720A | 1992 | Gelatin coated tablets and method for producing same | [168] |
| S. Imanishi | JPH09104621A | 1997 | Medicine coated with gelatinizing agent, lubricating agent and lubricant | [169] |
| Peter Gruber | WO9806385A1 | 1998 | Easy to swallow oral medicament composition | [170] |
| Nitsuto et al. | JP2002275054A | 2002 | Easily administrable solid preparation | [171] |
| Flanagan et al. | US6395298B1 | 2002 | Gellan gum tablet coating | [172] |
| Flanagan et al. | US6635282B1 | 2003 | Gellan gum tablet film coating | [173] |
| Tsukioka et al. | JP2007070344A | 2007 | Internal medicine | [174] |
| Jerry Robertson | US20070259038A1 | 2007 | Solid medicament dosage form consumption aid | [175] |
| Kawasumi et al. | JP2007015950A | 2007 | Easily-swallowable film-coated preparations containing antacids | [176] |
| Eramo Lincoln | US2007243246A1 | 2007 | Lubricious coatings for pharmaceutical applications | [177] |
| Kata et al. | JP2009120497A | 2009 | Film for assisting deglutition and method for producing the same | [178] |
| Kata et al. | JP2010120877A | 2010 | Oral administration preparation | [179] |
| Fujioka et al. | JP2011195569A | 2011 | Easily swallowable tablet | [180] |
| Chen et al. | TW 201121586A | 2011 | Oral tablet | [181] |
| Joel Waldman | WO2012024360A2 | 2012 | Tablet sleeve for improved performance | [182] |
| Yang et al. | CN102652738A | 2012 | Novel medicinal outer wrapper facilitating swallowing | [183] |
| Sugiura et al. | CN102361652A | 2012 | Adhesion preventing composition, solid preparation and method for producing the same | [184] |
| Li et al. | CN102430124A | 2012 | Pill coating with ultralow friction coefficient and preparation method | [185] |
| Mizuhara et al. | JP2014227391A | 2014 | Water-swellable laminated film and swallowable substance-coated body | [186] |
| Takano et al. | JP2014189547A | 2014 | Swallowable film-coated cover for oral drug delivery | [187] |
| Bao Yinjian | CN108543072A | 2018 | Coating composition and related used thereof | [188] |
| Bao Yinjian | CN108578704A | 2018 | Composition used for swallowing and relevant applications of composition | [189] |
| Jeffrey et al. | US2018036413A1 | 2018 | Easy to swallow coatings and substrates coated therewith | [190] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drumond, N.; Stegemann, S. Better Medicines for Older Patients: Considerations between Patient Characteristics and Solid Oral Dosage Form Designs to Improve Swallowing Experience. Pharmaceutics 2021, 13, 32. https://doi.org/10.3390/pharmaceutics13010032
Drumond N, Stegemann S. Better Medicines for Older Patients: Considerations between Patient Characteristics and Solid Oral Dosage Form Designs to Improve Swallowing Experience. Pharmaceutics. 2021; 13(1):32. https://doi.org/10.3390/pharmaceutics13010032
Chicago/Turabian StyleDrumond, Nélio, and Sven Stegemann. 2021. "Better Medicines for Older Patients: Considerations between Patient Characteristics and Solid Oral Dosage Form Designs to Improve Swallowing Experience" Pharmaceutics 13, no. 1: 32. https://doi.org/10.3390/pharmaceutics13010032