Transfersomes: A Promising Nanoencapsulation Technique for Transdermal Drug Delivery




Abstract
:1. Introduction
2. Transfersomes
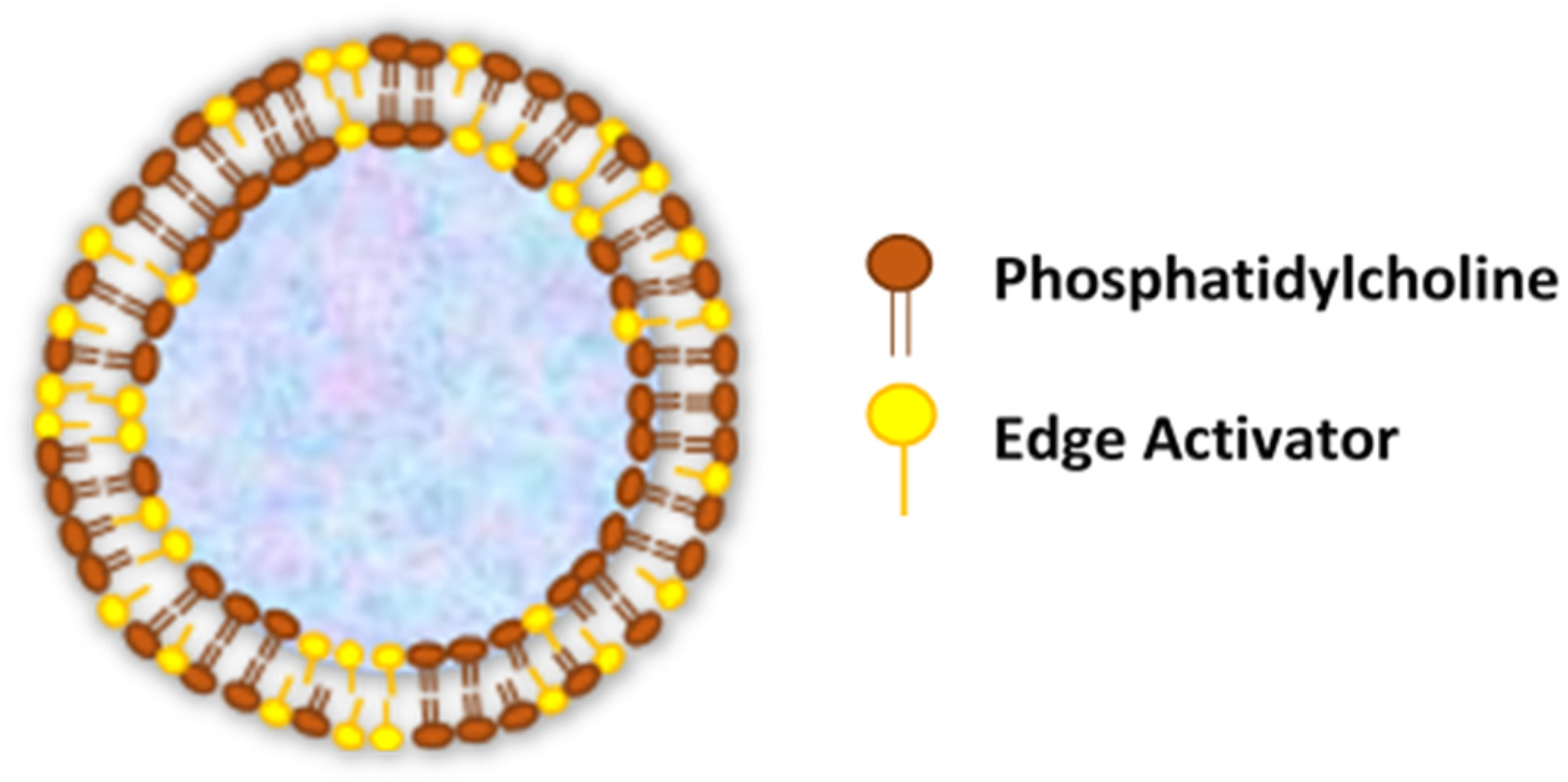
- Transfersomes carriers are composed of hydrophilic and hydrophobic moieties, which result in becoming a unique drug carrier system that can deliver therapeutic agents with wide range of solubility.
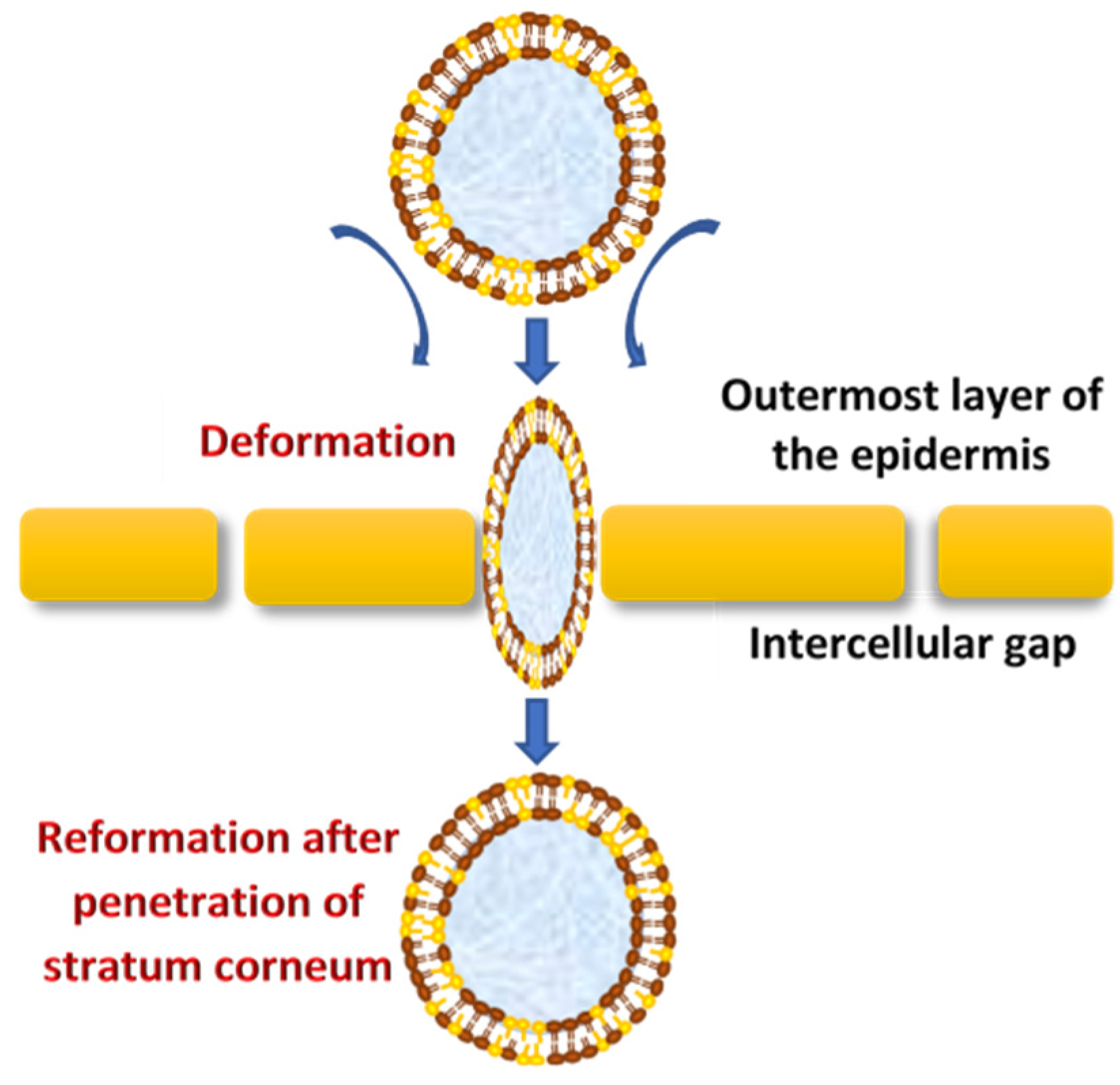
- Transfersomes are able to squeeze themselves through constrictions of the skin barrier that are very narrow, such as 5 to 10 times less than the vesicle diameter, owing to their ultra-deformability and elastic properties.
- High vesicle deformability facilitates the transport of drugs across the skin without any measurable loss in intact vesicles and can be used for both topical, as well as systemic, treatments.
- Transfersomes carriers are very versatile and efficient in accommodating a variety of agents nearly independent of their size, structure, molecular weight or polarity.
- They are made up of natural phospholipids and EAs, therefore promisingly biocompatible and biodegradable.
- Transfersomes can be used for the delivery of various active compounds, including proteins and peptides, insulin, corticosteroids, interferons, anesthetics, NSAIDs, anticancer drugs and herbal drugs.
- Transfersomes are an obvious choice for achieving a sustained drug release, as well as a predictable and extended duration of activity.
- They are capable of increasing the transdermal flux and improving the site specificity of bioactive agents.
- Avoiding the first-pass metabolism, which is a major drawback in oral drug administration, and result in optimized bioavailability of the drug.
- Minimize the undesirable side effects of the drug, as well as protect the drug from metabolic degradation; moreover, the utility of short half-life drugs.
- In most of the cases, a relatively high entrapment efficiency (EE) of nearly 90% of the lipophilic drug can be achieved by transfersomes. For transfersome formulations of diclofenac diethylamine (DDEA) and curcumin (CRM), the maximum entrapment efficiency achieved was over 90% for both DDEA and CRM transfersomes. Nevertheless, the entrapment efficiency can variate due to various reasons, as, when the lipid concentration was more, a high entrapment efficiency could be observed. The EE decreases when the surfactant concentration increases above certain concentrations due to the formation of mixed micelles. According to the literature, in case of a low EE, the lipophilic drug encapsulation could be enhanced by incorporating a surfactant with a low HLB (hydrophilic-lipophilic balance) value. It has been identified as a fact that transfersomes show a distinctive property of the very high encapsulation of lipophilic drugs.
- They have the advantage of being made from pharmaceutically acceptable ingredients using standard methods but need to be designed and optimized on a case-by-case basis.
- Due to a short and simple production procedure, it is easy to scale-up.
- Transfersomes are considered as chemically unstable due to their tendency to oxidative degradation. The oxidation of transfersomes can be significantly decreased when the aqueous media is degassed and purged with inert gases, such as nitrogen and argon [59]. Storage at a low temperature and protection from light will also reduce the chance of oxidation [60]. Post-preparation processing, such as freeze-drying and spray-drying, can improve the storage stability of transfersomes [61].
- Another obstacle of utilizing transfersomes as a drug delivery system is the difficulty to achieve the purity of natural phospholipids. Therefore, synthetic phospholipids could be used as alternatives [62].
- The expensiveness of transfersomal formulations is associated with the raw materials used in lipid excipients, as well as the expensive equipment needed to increase manufacturing. Hence, the widely used lipid component is phosphatidylcholine, because it is relatively low in cost [6].
3. Mechanism of Action
4. Composition of Transfersomes
- secondly, 10–25% surfactants/edge activators; the most commonly used edge activators in transfersome preparations are surfactants as sodium cholates; sodium deoxycholate; Tweens and Spans (Tween 20, Tween 60, Tween 80, Span 60, Span 65 and Span 80) and dipotassium glycyrrhizinate, which are biocompatible bilayer-softening compounds that increase the vesicles’ bilayer flexibility and improve the permeability [3,8,52,68,69].
5. Preparation Methods
5.1. Thin Film Hydration Technique/Rotary Evaporation-Sonication Method
5.2. Vortexing-Sonication Method
5.3. Modified Handshaking Process
5.4. Suspension Homogenization Method
5.5. Centrifugation Process
5.6. Reverse-Phase Evaporation Method
5.7. High-Pressure Homogenization Technique
5.8. Ethanol Injection Method
6. Factors Affecting Properties of Transfersomes
6.1. Effect of Phospholipids: Edge Activator Ratio
6.2. Effect of Various Solvents
6.3. Effect of Various Edge Activators (Surfactants)
6.4. Effect of the Hydration Medium
7. Characterization of the Transfersomes
7.1. Vesicle Size, Zeta Potential and Morphology
7.2. Number of Vesicles Per Cubic mm
7.3. Entrapment Efficiency (%EE)
7.4. Degree of Deformability
7.5. In Vitro Drug Release
7.6. In Vitro Skin Permeation Studies
7.7. Stability of Transfersomes
8. Applications of Transfersomes as the Transdermal Delivery System
8.1. Delivery of Antioxidants
8.2. Delivery of Anticancer Drugs
8.3. Delivery of Corticosteroids
8.4. Delivery of Anti-Inflammatory Drugs
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Chaurasiya, P.; Ganju, E.; Upmanyu, N.; Ray, S.K.; Jain, P. Transfersomes: A novel technique for transdermal drug delivery. J. Drug Deliv. Ther. 2019, 9, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Modi, C.; Bharadia, P. Transfersomes: New dominants for transdermal drug delivery. Am. J. PharmTech. Res. 2012, 2, 71–91. [Google Scholar]
- Jain, A.K.; Kumar, F. Transfersomes: Ultradeformable vesicles for transdermal drug delivery. Asian J. Biomater. Res. 2017, 3, 1–13. [Google Scholar]
- Elsayed, M.A.; Abdallah, O.Y.; Naggar, V.F.; Khalafallah, N.M. Lipid vesicles for skin delivery of drugs: Reviewing three decades of research. Int. J. Pharm. 2007, 332, 1–16. [Google Scholar] [CrossRef]
- Touitou, E.; Junginger, H.E.; Weiner, N.D.; Nagai, T.; Mezei, M. Liposomes as carriers for topical and transdermal delivery. J. Pharm. Sci. 1994, 83, 1189–1203. [Google Scholar] [CrossRef]
- Yadav, D.; Sandeep, K.; Pandey, D.; Dutta, R.K. Liposomes for drug delivery. J. Biotechnol. Biomater. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Cevc, G. Transfersomes, liposomes and other lipid suspensions on the skin: Permeation enhancement, vesicle penetration, and transdermal drug delivery. Crit. Rev. Ther. Drug Carr. Syst. 1996, 13, 257–388. [Google Scholar] [CrossRef]
- Rajan, R.; Jose, S.; Mukund, V.P.B.; Vasudevan, D.T. Transferosomes—A vesicular transdermal delivery system for enhanced drug permeation. J. Adv. Pharm. Technol. Res. 2011, 2, 138–143. [Google Scholar] [CrossRef]
- Lymberopoulos, A.; Demopoulou, C.; Kyriazi, M.; Katsarou, M.; Demertzis, N.; Hatziandoniou, S.; Maswadeh, H.; Papaioanou, G.; Demetzos, C.; Maibach, H.; et al. Liposome percutaneous penetration in vivo. Toxicol. Res. Appl. 2017, 1, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Khan, M.A.; Burgess, D.J. Predicting hydrophilic drug encapsulation inside unilamellar liposomes. Int. J. Pharm. 2012, 423, 410–418. [Google Scholar] [CrossRef]
- Szoka, F.; Papahadjopoulos, D. Procedure for preparation of liposomes with large internal aqueous space and high capture by reverse-phase evaporation. Proc. Natl. Acad. Sci. USA 1978, 75, 4194–4198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crommelin, D.J.A.; Fransen, G.J.; Salemink, P.J.M. Stability of liposomes on storage. Target. Drugs Synth. Syst. 1986, 277–287. [Google Scholar] [CrossRef]
- Ge, X.; Wei, M.; He, S.; Yuan, W. Advances of non-ionic surfactant vesicles (niosomes) and their application in drug delivery. Pharmaceutics 2019, 11, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marianecci, C.; Di Marzio, L.; Rinaldi, F.; Celia, C.; Paolino, D.; Alhaique, F.; Esposito, S.; Carafa, M. Niosomes from 80s to present: The state of the art. Adv. Colloid Interface Sci. 2014, 205, 187–206. [Google Scholar] [CrossRef]
- Mujoriya, R.Z.; Dhamande, K.; Bodla, R.B. Niosomal drug delivery system—A review. Int. J. App. Pharm. 2011, 3, 7–10. [Google Scholar]
- Ezzat, H.M.; Elnaggar, Y.S.R.; Abdallah, O.Y. Improved oral bioavailability of the anticancer drug catechin using chitosomes: Design, in-vitro appraisal and in-vivo studies. Int. J. Pharm. 2019, 565, 488–498. [Google Scholar] [CrossRef]
- Manca, M.L.; Manconi, M.; Valenti, D.; Lai, F.; Loy, G.; Matricardi, P.; Fadda, A.M. Liposomes coated with chitosan–xanthan gum (chitosomes) as potential carriers for pulmonary delivery of rifampicin. J. Pharm. Sci. 2012, 101, 566–575. [Google Scholar] [CrossRef]
- Mertins, O.; Dimova, R. Binding of Chitosan to Phospholipid Vesicles Studied with Isothermal Titration Calorimetry. Langmuir 2011, 27, 5506–5515. [Google Scholar] [CrossRef]
- Jain, S.; Jain, V.; Mahajan, S.C. Lipid Based Vesicular Drug Delivery Systems. Adv. Pharm. 2014, 2014, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mann, J.F.; Scales, H.E.; Shakir, E.; Alexander, J.; Carter, K.C.; Mullen, A.B.; Ferro, V.A. Oral delivery of tetanus toxoid using vesicles containing bile salts (bilosomes) induces significant systemic and mucosal immunity. Methods 2006, 38, 90–95. [Google Scholar] [CrossRef]
- Yang, L.; Tucker, I.G.; Østergaard, J. Effects of bile salts on propranolol distribution into liposomes studied by capillary electrophoresis. J. Pharm. Biomed. Anal. 2011, 56, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.; Pandey, V.; Rai, G. Transfersomes as versatile and flexible nano-vesicular carriers in skin cancer therapy: The state of the art. Nano Rev. Exp. 2017, 8, 1325708. [Google Scholar] [CrossRef] [PubMed]
- Cevc, G.; Schatzlein, A.G.; Richardsen, H. Ultradeformable lipid vesicles can penetrate the skin and other semi-permeable barriers unfragmented. Evidence from double label CLSM experiments and direct size measurements. Biochim. et Biophys. Acta (BBA)-Biomembr. 2002, 1564, 21–30. [Google Scholar] [CrossRef] [Green Version]
- Cevc, G. Lipid vesicles and other colloids as drug carriers on the skin. Adv. Drug Deliv. Rev. 2004, 56, 675–711. [Google Scholar] [CrossRef]
- Rother, M.; Lavins, B.J.; Kneer, W.; Lehnhardt, K.; Seidel, E.J.; Mazgareanu, S. Efficacy and safety of epicutaneous ketoprofen in Transfersome (IDEA-033) versus oral celecoxib and placebo in osteoarthritis of the knee: Multicentre randomised controlled trial. Ann. Rheum. Dis. 2007, 66, 1178–1183. [Google Scholar] [CrossRef]
- Kumar, A.; Pathak, K.; Bali, V. Ultra-adaptable nanovesicular systems: A carrier for systemic delivery of therapeutic agents. Drug Discov. Today 2012, 17, 1233–1241. [Google Scholar] [CrossRef]
- Fesq, H.; Lehmann, J.; Kontny, A.; Erdmann, I.; Theiling, K.; Rother, M.; Ring, J.; Cevc, G.; Abeck, D. Improved risk-benefit ratio for topical triamcinolone acetonide in Transfersome in comparison with equipotent cream and ointment: A randomized controlled trial. Brit. J. Dermatol. 2003, 149, 611–619. [Google Scholar] [CrossRef]
- Cevc, G. Transfersomes: Innovative transdermal drug carriers. In Modified-Release Drug Delivery Technology, 1st ed.; Rathbone, M.J., Hadgraft, J., Roberts, M.S., Eds.; Marcel Dekker, Inc.: New York, NY, USA, 2002; Volume 126, pp. 533–546. ISBN 0-8247-0869-5. [Google Scholar]
- Touitou, E. Composition of Applying Active Substance to or Through the Skin. U.S. Patent 5540934A, 30 July 1996. [Google Scholar]
- Touitou, E.; Dayan, N.; Bergelson, L.; Godin, B.; Eliaz, M. Ethosomes novel vesicular carriers for enhanced delivery: Characterization and skin penetration properties. J. Control. Release 2000, 65, 403–418. [Google Scholar] [CrossRef]
- Shah, S.M.; Ashtikar, M.; Jain, A.S.; Makhija, D.T.; Nikam, Y.; Gude, R.P.; Steiniger, F.; Jagtap, A.A.; Nagarsenker, M.S.; Fahr, A. LeciPlex, invasomes, and liposomes: A skin penetration study. Int. J. Pharm. 2015, 490, 391–403. [Google Scholar] [CrossRef]
- Qadri, G.R.; Ahad, A.; Aqil, M.; Imam, S.S.; Ali, A. Invasomes of isradipine for enhanced transdermal delivery against hypertension: Formulation, characterization, and in vivo pharmacodynamic study. Artif. Cells Nanomed. Biotechnol. 2016, 45, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Walve, J.R.; Bakliwal, S.R.; Rane, B.R.; Pawar, S.P. Transfersomes: A surrogated carrier for transdermal drug delivery system. Int. J. Appl. Biol. Pharm. Technol. 2011, 2, 204–213. [Google Scholar]
- Sivannarayana, P.; Rani, A.P.; Saikishore, V.; VenuBabu, C.; SriRekha, V. Transfersomes: Ultra deformable vesicular carrier systems in transdermal drug delivery system. Res. J. Pharm. Dos. Forms Technol. 2012, 4, 243–255. [Google Scholar]
- Sachan, R.; Parashar, T.; Soniya, S.V.; Singh, G.; Tyagi, S.; Patel, C.; Gupta, A. Drug carrier transfersomes: A novel tool for transdermal drug delivery system. Int. J. Res. Dev. Pharm. Life Sci. 2013, 2, 309–316. [Google Scholar]
- Li, J.; Wang, X.; Zhang, T.; Wang, C.; Huang, Z.; Luo, X.; Deng, Y. A review on phospholipids and their main applications in drug delivery systems. Asian J. Pharm. Sci. 2015, 10, 81–98. [Google Scholar] [CrossRef]
- Bhasin, B.; Londhe, V.Y. An overview of transfersomal drug delivery. Int. J. Pharm. Sci. Res. 2018, 9, 2175–2184. [Google Scholar] [CrossRef]
- Lei, W.; Yu, C.; Lin, H.; Zhou, X. Development of tacrolimus-loaded transfersomes for deeper skin penetration enhancement and therapeutic effect improvement in vivo. Asian J. Pharm. Sci. 2013, 8, 336–345. [Google Scholar] [CrossRef] [Green Version]
- Pandey, A. Role of surfactants as penetration enhancer in transdermal drug delivery system. J. Mol. Pharm. Org. Process. Res. 2014, 2, 1–10. [Google Scholar] [CrossRef]
- Duangjit, S.; Opanasopit, P.; Rojanarata, T.; Ngawhirunpat, T. Characterization and in vitro skin permeation of meloxicam-loaded Liposomes versus Transfersomes. J. Drug Deliv. 2010, 2011, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, N.; Goindi, S. Preparation and evaluation of antifungal efficacy of griseofulvin loaded deformable membrane vesicles in optimized guinea pig model of Microsporum canis—Dermatophytosis. Int. J. Pharm. 2012, 437, 277–287. [Google Scholar] [CrossRef]
- Chen, J.; Lu, W.-L.; Gu, W.; Lu, S.-S.; Chen, Z.-P.; Cai, B.-C. Skin permeation behavior of elastic liposomes: Role of formulation ingredients. Expert Opin. Drug Deliv. 2013, 10, 845–856. [Google Scholar] [CrossRef]
- Duangjit, S.; Opanasopit, P.; Rojanarata, T.; Ngawhirunpat, T. Effect of edge activator on characteristic and in vitro skin permeation of meloxicam loaded in elastic liposomes. Adv. Mater. Res. 2011, 194, 537–540. [Google Scholar] [CrossRef]
- Jacob, L.; Anoop, K.R. A review on surfactants as edge activators in ultradeformable vesicles for enhanced skin delivery. Int. J. Pharma Bio Sci. 2013, 4, 337–344. [Google Scholar]
- Kim, B.; Cho, H.-E.; Moon, S.H.; Ahn, H.-J.; Bae, S.; Cho, H.-D.; An, S. Transdermal delivery systems in cosmetics. Biomed. Dermatol. 2020, 4, 1–12. [Google Scholar] [CrossRef]
- Kumar, G.P.; Rajeshwarrao, P. Nonionic surfactant vesicular systems for effective drug delivery—An overview. Acta Pharm. Sin. B 2011, 1, 208–219. [Google Scholar] [CrossRef] [Green Version]
- Mathur, M. Approaches for improving the pharmacological and pharmacokinetics properties of herbal drugs. Int. Res. J. Pharm. Appl. Sci. 2013, 3, 40–50. [Google Scholar]
- Pawar, A.Y.; Jadhav, K.R.; Chaudhari, L.H. Transfersome: A novel technique which improves transdermal permeability. Asian J. Pharm. 2016, 10, 425–436. [Google Scholar] [CrossRef]
- Ghai, I.; Chaudhary, H.; Ghai, S.; Kohli, K.; Kr, V. A review of transdermal drug delivery using nano-vesicular carriers: Transfersomes. Recent Pat. Nanomed. 2012, 2, 164–171. [Google Scholar] [CrossRef]
- Vinod, K.R.; Kumar, M.S.; Anbazhagan, S.; Sandhya, S.; Saikumar, P.; Rohit, R.T.; Banji, D. Critical issues related to transfersomes-novel vesicular system. Acta Sci. Pol. Technol. Aliment. 2012, 11, 67–82. [Google Scholar]
- Benson, H.A. Transfersomes for transdermal drug delivery. Expert Opin. Drug Deliv. 2006, 3, 727–737. [Google Scholar] [CrossRef]
- Jiang, T.; Wang, T.; Li, T.; Ma, Y.; Shen, S.; He, B.; Mo, R. Enhanced transdermal drug delivery by transfersome-embedded oligopeptide hydrogel for topical chemotherapy of melanoma. ACS Nano 2018, 12, 9693–9701. [Google Scholar] [CrossRef]
- Chauhan, P.; Tyagi, B.K. Herbal novel drug delivery systems and transfersomes. J. Drug Deliv. Ther. 2018, 8, 162–168. [Google Scholar] [CrossRef]
- Cevc, G. Transdermal drug delivery of insulin with ultradeformable carriers. Clin. Pharmacokinet. 2003, 42, 461–474. [Google Scholar] [CrossRef] [PubMed]
- Garg, V.; Singh, H.; Bimbrawh, S.; Singh, S.K.; Gulati, M.; Vaidya, Y.; Kaur, P. Ethosomes and transfersomes: Principles, perspectives and practices. Curr. Drug Deliv. 2016, 14, 613–633. [Google Scholar] [CrossRef]
- Moawad, F.A.; Ali, A.A.; Salem, H.F. Nanotransfersomes-loaded thermosensitive in situ gel as a rectal delivery system of tizanidine HCl: Preparation, in vitro and in vivo performance. Drug Deliv. 2017, 24, 252–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bnyan, R.; Khan, I.; Ehtezazi, T.; Saleem, I.; Gordon, S.; Neill, F.O.; Roberts, M. Surfactant effects on lipid-based vesicles properties. J. Pharm. Sci. 2018, 107, 1237–1246. [Google Scholar] [CrossRef]
- Kumar, A. Transferosome: A recent approach for transdermal drug delivery. J. Drug Deliv. Ther. 2018, 8, 100–104. [Google Scholar] [CrossRef] [Green Version]
- MirAfzali, Z.; Thompson, C.S.; Tallua, K. Chapter 13—Application of liposomes in the food industry. In Microencapsulation in the Food Industry: A Practical Implementation Guide; Academic Press: Cambridge, MA, USA, 2014; pp. 139–150. [Google Scholar]
- Grit, M.; Crommelin, D.J. Chemical stability of liposomes: Implications for their physical stability. Chem. Phys. Lipids 1993, 64, 3–18. [Google Scholar] [CrossRef]
- Iskandarsyah; Rahmi, A.D.; Pangesti, D.M. Comparison of the characteristics of transfersomes and protransfersomes containing azelaic acid. J. Young-Pharm. 2018, 10, S11–S15. [Google Scholar] [CrossRef] [Green Version]
- Van Hoogevest, P.; Wendel, A. The use of natural and synthetic phospholipids as pharmaceutical excipients. Eur. J. Lipid Sci. Technol. 2014, 116, 1088–1107. [Google Scholar] [CrossRef] [Green Version]
- Jadupati, M.; Kumar, N.A. Transferosome: An opportunistic carrier for transdermal drug delivery system. Int. Res. J. Pharm. 2012, 3, 35–38. [Google Scholar]
- Cevc, G.; Blume, G.; Schätzlein, A.; Gebauer, D.; Paul, A. The skin: A pathway for systemic treatment with patches and lipid-based agent carriers. Adv. Drug Deliv. Rev. 1996, 18, 349–378. [Google Scholar] [CrossRef]
- Mandal, U.K.; Mahmood, S.; Taher, M. Experimental design and optimization of raloxifene hydrochloride loaded nanotransfersomes for transdermal application. Int. J. Nanomed. 2014, 9, 4331–4346. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cipolla, D.; Wu, H.; Gonda, I.; Eastman, S.; Redelmeier, T.; Chan, H.-K. Modifying the release properties of liposomes toward personalized medicine. J. Pharm. Sci. 2014, 103, 1851–1862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dudhipala, N.; Mohammed, R.P.; Youssef, A.A.A.; Banala, N. Effect of lipid and edge activator concentration on development of Aceclofenac loaded transfersomes gel for transdermal application: In vitro and ex vivo skin permeation. Drug Dev. Ind. Pharm. 2020, 46, 1–28. [Google Scholar] [CrossRef]
- Kotla, N.G.; Chandrasekar, B.; Rooney, P.; Sivaraman, G.; Larrañaga, A.; Krishna, K.V.; Pandit, A.; Rochev, Y. Biomimetic lipid-based nanosystems for enhanced dermal delivery of drugs and bioactive agents. ACS Biomater. Sci. Eng. 2017, 3, 1262–1272. [Google Scholar] [CrossRef]
- Ascenso, A.; Batista, C.; Cardoso, P.; Mendes, T.; Praça, F.G.; Bentley, M.V.L.B.; Raposo, S.; Simões, S. Development, characterization, and skin delivery studies of related ultradeformable vesicles: Transfersomes, ethosomes, and transethosomes. Int. J. Nanomed. 2015, 10, 5837–5851. [Google Scholar] [CrossRef] [Green Version]
- Sarangi, M.; Padhi, S. Novel herbal drug delivery system: An overview. Arch. Med. Heal. Sci. 2018, 6, 171. [Google Scholar] [CrossRef]
- Podili, C.; Firoz, S. A review on transferosomes for transdermal drug delivery. J. Glob. Trends Pharm. Sci. 2014, 5, 2118–2127. [Google Scholar]
- Anggraini, W.; Sagita, E.; Iskandarsyah, I. Effect of hydrophilicity surfactants toward characterization and in vitro transfersomes penetration in gels using franz diffusion test. Int. J. Appl. Pharm. 2017, 9, 112–115. [Google Scholar] [CrossRef]
- Cevc, G.; Schatzlein, A.G.; Blume, G. Transdermal drug carriers: Basic properties, optimization and transfer efficiency in the case of epicutaneously applied peptides. J. Control. Release 1995, 36, 3–16. [Google Scholar] [CrossRef]
- Cevc, G.; Gebauer, D.; Stieber, J.; Schätzlein, A.; Blume, G. Ultraflexible vesicles, transfersomes, have an extremely low pore penetration resistance and transport therapeutic amounts of insulin across the intact mammalian skin. Biochim. et Biophys. Acta (BBA)-Biomembr. 1998, 1368, 201–215. [Google Scholar] [CrossRef] [Green Version]
- Kadu, S.D.P. Transfersomes—A boon for transdermal delivery. Indo Am. J. Pharm. Sci. 2017, 4, 2908–2919. [Google Scholar] [CrossRef]
- El Zaafarany, G.M.; Awad, G.A.S.; Holayel, S.M.; Mortada, N. Role of edge activators and surface charge in developing ultradeformable vesicles with enhanced skin delivery. Int. J. Pharm. 2010, 397, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Sharma, V.; Yusuf, M.; Pathak, K. Nanovesicles for transdermal delivery of felodipine: Development, characterization, and pharmacokinetics. Int. J. Pharm. Investig. 2014, 4, 119–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.; Li, D.; Jin, Y.; Zhang, W.; Teng, L.; Bunt, C.; Wen, J. Deformable liposomes by reverse-phase evaporation method for an enhanced skin delivery of (+)-catechin. Drug Dev. Ind. Pharm. 2013, 40, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.-S.; Li, Y.-S.; Kuo, Y.-C.; Tsai, S.-J.J.; Lin, C.-C. Preparation and evaluation of novel transfersomes combined with the natural antioxidant resveratrol. Molecules 2019, 24, 600. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Ou, R.; Guan, S.; Ye, X.; Hu, B.; Zhang, Y.; Lu, S.; Zhou, Y.; Yuan, Z.; Zhang, J.; et al. A novel drug delivery gel of terbinafine hydrochloride with high penetration for external use. Drug Deliv. 2014, 22, 1–8. [Google Scholar] [CrossRef]
- Balata, G.F.; Faisal, M.M.; Elghamry, H.A.; Sabry, S.A. Preparation and characterization of ivabradine HCl transfersomes for enhanced transdermal delivery. J. Drug Deliv. Sci. Technol. 2020, 60, 101921. [Google Scholar] [CrossRef]
- Vasanth, S.; Dubey, A.; Ravi, G.S.; Lewis, S.A.; Ghate, V.M.; El-Zahaby, S.A.; Hebbar, S. Development and investigation of vitamin c-enriched adapalene-loaded transfersome gel: A collegial approach for the treatment of acne vulgaris. AAPS Pharm. Sci. Tech. 2020, 21, 61. [Google Scholar] [CrossRef]
- Qushawy, M.; Nasr, A.; Abd-Alhaseeb, M.; Swidan, S. Design, optimization and characterization of a transfersomal gel using miconazole nitrate for the treatment of candida skin infections. Pharmaceutics 2018, 10, 26. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.C.; Barry, B.W. Penetration enhancers. Adv. Drug Deliv. Rev. 2004, 56, 603–618. [Google Scholar] [CrossRef] [PubMed]
- Shamma, R.N.; Elsayed, I. Transfersomal lyophilized gel of buspirone HCl: Formulation, evaluation and statistical optimization. J. Liposome Res. 2013, 23, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.K.; Jain, P.; Umamaheshwari, R.B.; Jain, N.K. Transfersomes—A novel vesicular carrier for enhanced transdermal delivery: Development, characterization, and performance evaluation. Drug Dev. Ind. Pharm. 2003, 29, 1013–1026. [Google Scholar] [CrossRef] [PubMed]
- N’Da, D.D. Prodrug strategies for enhancing the percutaneous absorption of drugs. Molecules 2014, 19, 20780–20807. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.; Vardhan, H.; Kotla, N.G.; Maddiboyina, B.; Sharma, D.; Webster, T.J. The role of surfactants in the formulation of elastic liposomal gels containing a synthetic opioid analgesic. Int. J. Nanomed. 2016, 11, 1475–1482. [Google Scholar]
- Al Shuwaili, A.H.; Rasool, B.K.A.; Abdulrasool, A.A. Optimization of elastic transfersomes formulations for transdermal delivery of pentoxifylline. Eur. J. Pharm. Biopharm. 2016, 102, 101–114. [Google Scholar] [CrossRef]
- Ahad, A.; Al-Saleh, A.A.; Al-Mohizea, A.M.; Al-Jenoobi, F.I.; Raish, M.; Yassin, A.E.B.; Alam, M.A. Formulation and characterization of novel soft nanovesicles for enhanced transdermal delivery of eprosartan mesylate. Saudi Pharm. J. 2017, 25, 1040–1046. [Google Scholar] [CrossRef]
- Bnyan, R.; Khan, I.; Ehtezazi, T.; Saleem, I.; Gordon, S.; O’Neill, F.; Roberts, M. Formulation and optimisation of novel transfersomes for sustained release of local anaesthetic. J. Pharm. Pharmacol. 2019, 71, 1508–1519. [Google Scholar] [CrossRef]
- Kumar, M.S. Preeti Development of celecoxibtransfersomal gel for the treatment of rheumatoid arthritis. Indian J. Pharm. Boil. Res. 2014, 2, 7–13. [Google Scholar] [CrossRef]
- Singh, S.; Verma, D.; Mirza, M.A.; Das, A.K.; Dudeja, M.; Anwer, M.K.; Sultana, Y.; Talegaonkar, S.; Iqbal, Z.; Mukharjee, A. Development and optimization of ketoconazole loaded nano-transfersomal gel for vaginal delivery using Box-Behnken design: In vitro, ex vivo characterization and antimicrobial evaluation. J. Drug Deliv. Sci. Technol. 2017, 39, 95–103. [Google Scholar] [CrossRef]
- Omar, M.M.; Hasan, O.A.; El Sisi, A.M. Preparation and optimization of lidocaine transferosomal gel containing permeation enhancers: A promising approach for enhancement of skin permeation. Int. J. Nanomed. 2019, 14, 1551–1562. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Murawsky, M.; LaCount, T.; Hao, J.; Kasting, G.B.; Newman, B.; Ghosh, P.; Raney, S.G.; Li, S.K. Characterization of temperature profiles in skin and transdermal delivery system when exposed to temperature gradients in vivo and in vitro. Pharm. Res. 2017, 34, 1491–1504. [Google Scholar] [CrossRef] [PubMed]
- El Sayyad, M.K.; Zaky, A.A.; Samy, A.M. Fabrication and Characterization of Sildenafil Citrate Loaded Transfersomes as a Carrier for Transdermal Drug Delivery. Pharm. Pharmacol. Int. J. 2017, 5, 1–10. [Google Scholar] [CrossRef]
- Ruela, A.L.M.; Perissinato, A.G.; Lino, M.E.D.S.; Mudrik, P.S.; Pereira, G.R. Evaluation of skin absorption of drugs from topical and transdermal formulations. Braz. J. Pharm. Sci. 2016, 52, 527–544. [Google Scholar] [CrossRef] [Green Version]
- El Maghraby, G.M.; Barry, B.W.; Williams, A.C. Liposomes and skin: From drug delivery to model membranes. Eur. J. Pharm. Sci. 2008, 34, 203–222. [Google Scholar] [CrossRef] [PubMed]
- Haq, A.; Goodyear, B.; Ameen, D.; Joshi, V.; Michniak-Kohn, B.B. Strat-M® synthetic membrane: Permeability comparison to human cadaver skin. Int. J. Pharm. 2018, 547, 432–437. [Google Scholar] [CrossRef]
- Avadhani, K.S.; Manikkath, J.; Tiwari, M.; Chandrasekhar, M.; Godavarthi, A.; Vidya, S.M.; Hariharapura, R.C.; Kalthur, G.; Udupa, N.; Mutalik, S. Skin delivery of epigallocatechin-3-gallate (EGCG) and hyaluronic acid loaded nano-transfersomes for antioxidant and anti-aging effects in UV radiation induced skin damage. Drug Deliv. 2017, 24, 61–74. [Google Scholar] [CrossRef] [Green Version]
- Cevc, G.; Blume, G. Biological activity and characteristics of triamcinolone-acetonide formulated with the self-regulating drug carriers, Transfersomes®. Biochim. et Biophys. Acta (BBA) Biomembr. 2003, 1614, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Cevc, G.; Blume, G. Hydrocortisone and dexamethasone in very deformable drug carriers have increased biological potency, prolonged effect, and reduced therapeutic dosage. Biochim. et Biophys. Acta (BBA) Biomembr. 2004, 1663, 61–73. [Google Scholar] [CrossRef]
- Shabana, S.; Sailaja, A.K. Formulation and evaluation of diclofenac sodium transferosomes using different surfactants by thin film hydration method. Der Pharm. Lett. 2015, 7, 43–53. [Google Scholar]
- Ghanbarzadeh, S.; Arami, S. Enhanced transdermal delivery of diclofenac sodium via conventional liposomes, ethosomes, and transfersomes. Biomed. Res. Int. 2013, 2013, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Cevc, G.; Blume, G.; Schätzlein, A. Transfersomes-mediated transepidermal delivery improves the regio-specificity and biological activity of corticosteroids in vivo. J. Control. Release 1997, 45, 211–226. [Google Scholar] [CrossRef]
- Cevc, G.; Blume, G. New, highly efficient formulation of diclofenac for the topical, transdermal administration in ultradeformable drug carriers, transfersomes. Biochim. et Biophys. Acta (BBA) Biomembr. 2001, 1514, 191–205. [Google Scholar] [CrossRef] [Green Version]
- Sailaja, K.; Supraja, R. Formulation of mefenamic acid loaded transfersomal gel by thin film hydration technique and hand shaking method. Nanomed. J. 2017, 4, 126–134. [Google Scholar]
- Sardana, V.; Burzynski, J.; Zalzal, P. Safety and efficacy of topical ketoprofen in transfersome gel in knee osteoarthritis: A systematic review. Musculoskelet. Care 2016, 15, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Rother, M.; Seidel, E.J.; Clarkson, P.M.; Mazgareanu, S.; Vierl, U.; Rother, I. Efficacy of epicutaneous diractin (ketoprofen in transfersome gel) for the treatment of pain related to eccentric muscle contractions. Drug Des. Devel. Ther. 2009, 3, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Irfan, M.; Verma, S.R.; Ram, A. Preparation and characterization of ibuprofen loaded transferosome as a novel carrier for transdermal drug delivery system. Asian J. Pharm. Clin. Res. 2012, 5, 162–165. [Google Scholar]
- Darusman, F.; Raisya, R.; Priani, S.E. Development, characterization, and performance evaluation of transfersome gel of ibuprofen as a transdermal drug delivery system using nanovesicular carrier. Drug Invent. Today 2019, 10, 3750–3755. [Google Scholar]
- Patel, R.; Singh, S.K.; Singh, S.; Sheth, N.; Gendle, R. Development and characterization of curcumin loaded transfersome for transdermal delivery. J. Pharm. Sci. Res. 2009, 1, 71–80. [Google Scholar]
- Agrawal, R.; Sandhu, S.K.; Sharma, I.; Kaur, I.P. Development and evaluation of curcumin-loaded elastic vesicles as an effective topical anti-inflammatory formulation. AAPS PharmSciTech 2014, 16, 364–374. [Google Scholar] [CrossRef]
- Kaur, C.D.; Saraf, S. Topical vesicular formulations of Curcuma longa extract on recuperating the ultraviolet radiation–damaged skin. J. Cosmet. Dermatol. 2011, 10, 260–265. [Google Scholar] [CrossRef]
- Saraf, S.; Jeswani, G.; Kaur, C.D.; Saraf, S.K. Development of novel herbal cosmetic cream with curcuma longa extract loaded transfersomes for antiwrinkle effect. Afr. J. Pharm. Pharmaco. 2011, 5, 1054–1062. [Google Scholar]
- Sarwa, K.K.; Mazumder, B.; Rudrapal, M.; Verma, V.K. Potential of capsaicin-loaded transfersomes in arthritic rats. Drug Deliv. 2014, 22, 638–646. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Hou, S.-X.; Chen, T.; Sun, Y.-Y.; Yang, B.-X.; Yuan, Z.-Y. Preparation of transfersomes of vincristine sulfate and study on its prcutaneous penetration. China J. Chin. Mater. Med. 2005, 30, 900–903. [Google Scholar]
- Lu, Y.; Hou, S.X.; Zhang, L.K.; Li, Y.; He, J.Y.; Guo, D.D. Transdermal and lymph targeting transfersomes of vincristine. Yao Xue Xue Bao Acta Pharm. Sin. 2007, 42, 1097–1101. [Google Scholar]
- Bhatia, A.; Usha, K.; Wadhwa, S.; Raza, K.; Katare, O.P. Novel phospholipid-based topical formulations of tamoxifen: Evaluation for antipsoriatic activity using mouse-tail model. Pharm. Dev. Technol. 2013, 19, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Kong, M.; Hou, L.; Wang, J.; Feng, C.; Liu, Y.; Cheng, X.J.; Chen, X. Enhanced transdermal lymphatic drug delivery of hyaluronic acid modified transfersomes for tumor metastasis therapy. Chem. Commun. 2015, 51, 1453–1456. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Pandit, J.; Sultana, Y.; Sultana, S.; Ali, A.; Aqil, M.; Chauhan, M. Novel carbopol-based transfersomal gel of 5-fluorouracil for skin cancer treatment: In vitro characterization and in vivo study. Drug Deliv. 2014, 22, 1–8. [Google Scholar] [CrossRef]
- Jain, S.; Jain, N. PUB040 formulation and evaluation of embelin loaded transfersome for effective treatment of skin cancer. J. Thorac. Oncol. 2017, 12, S2378. [Google Scholar] [CrossRef]
- Amin, S.; Sarfenejad, A.; Ahmad, J.; Kohli, K.; Mir, S.R. Nanovesicular transfersomes for enhanced systemic delivery of telmisartan. Adv. Sci. Eng. Med. 2013, 5, 299–308. [Google Scholar] [CrossRef]
- Gupta, A.; Aggarwal, G.; Singla, S.; Arora, R. Transfersomes: A novel vesicular carrier for enhanced transdermal delivery of sertraline: Development, characterization, and performance evaluation. Sci. Pharm. 2012, 80, 1061–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, P.N.; Mishra, V.; Singh, P.; Rawat, A.; Dubey, P.; Mahor, S.; Vyas, S.P. Tetanus toxoid-loaded transfersomes for topical immunization. J. Pharm. Pharmacol. 2005, 57, 295–301. [Google Scholar] [CrossRef]
- Paul, A.; Cevc, G.; Bachhawat, B.K. Transdermal immunisation with an integral membrane component, gap junction protein, by means of ultradeformable drug carriers, transfersomes. Vaccine 1998, 16, 188–195. [Google Scholar] [CrossRef]
- Laxmi, M.V.; Zafaruddin, M.; Kuchana, V. Design and characterization of transferosomal gel of repaglinide. Int. Res. J. Pharm. 2015, 6, 38–42. [Google Scholar] [CrossRef]
- Hussain, G.; Kohli, K.; Umar, A.; Amin, S. Nanovesicular delivery of repaglinide through skin. Sci. Adv. Mater. 2013, 5, 810–821. [Google Scholar] [CrossRef]
- Sarita, K.C.; Sunil, K. Design, development and evaluation of itraconazole loaded transfersomal gel. Int. J. Farm. 2016, 2, 198–209. [Google Scholar]
- Mahmood, S.; Chatterjee, B.; Mandal, U.K. Nano transfersomes vesicles of raloxifene hcl with sorbitan 80: Formulation and characterization. Bioequivalence Bioavailab. Int. J. 2018, 2, 1–7. [Google Scholar] [CrossRef]
- Badr-Eldin, S.M.; Ahmed, O.A. Optimized nano-transfersomal films for enhanced sildenafil citrate transdermal delivery: Ex vivo and in vivo evaluation. Drug Des. Dev. Ther. 2016, 10, 1323–1333. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, T.A. Preparation of transfersomes encapsulating sildenafil aimed for transdermal drug delivery: Plackett–Burman design and characterization. J. Liposome Res. 2014, 25, 1–10. [Google Scholar] [CrossRef]
- Hofer, C.; Göbel, R.; Deering, P.; Lehmer, A.; Breul, J. Formulation of interleukin-2 and interferon-alpha containing ultradeformable carriers for potential transdermal application. Anticancer. Res. 1999, 19, 1505–1507. [Google Scholar]
- Singh, H.P.; Tiwary, A.K.; Jain, S. Preparation and in vitro, in vivo characterization of elastic liposomes encapsulating cyclodextrin-colchicine complexes for topical delivery of colchicine. Yakugaku Zasshi 2010, 130, 397–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Hou, S.X.; Chen, T.; Lu, Y. Preparation and characterization of transfersomes of three drugs in vitro. China J. Chin. Mater. Med. 2006, 31, 728–731. [Google Scholar]
- Abd, E.; Grice, J.E.; Roberts, J.A. A comparison of the penetration and permeation of caffeine into and through human epidermis after application in various vesicle formulations. Ski. Pharmacol. Physiol. 2015, 29, 24–30. [Google Scholar] [CrossRef]
- Ramezani, V.; Honarvar, M.; Seyedabadi, M.; Karimollah, A.; Ranjbar, A.M.; Hashemi, M. Formulation and optimization of transfersome containing minoxidil and caffeine. J. Drug Deliv. Sci. Technol. 2018, 44, 129–135. [Google Scholar] [CrossRef]
- Parkash, V.; Maan, S.; Chaudhary, V.; Jogpal, V.; Mittal, G.; Jain, V. Implementation of design of experiments in development and optimization of transfersomal carrier system of tacrolimus for the dermal management of psoriasis in albino wistar rat. J. Bioequiv. Availab. 2018, 10, 98–105. [Google Scholar] [CrossRef]
- Maghraby, G.M.M.E.; Williams, A.C.; Barry, B.W. Skin hydration and possible shunt route penetration in controlled estradiol delivery from ultradeformable and standard liposomes. J. Pharm. Pharmacol. 2001, 53, 1311–1322. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameter | Method/Equipment |
|---|---|
| Vesicle size, size distribution Zeta potential | Dynamic light scattering (DLS) method by Malvern Zetasizer Electrophoretic mobility technique by Malvern Zetasizer |
| Vesicle morphology | DLS method, Photon correlation spectroscopy, Transmission electron microscopy |
| Number of vesicles for cubic mm | Hemocytometer and optical microscope |
| Entrapment efficiency | Directly or indirectly using high-performance liquid chromatography (HPLC) or spectrophotometric method |
| Drug content | Modified HPLC method using an ultraviolet detector, auto sample, column oven, pump and computerized analysis program depending upon the analytical method of the active pharmaceutical agent |
| Degree of deformability | Microporous filter with DLS, Transmission electron microscopy |
| Surface charge and charge density | DLS method by Malvern Zetasizer, Thin-layer chromatography |
| In-vitro drug release | Franz diffusion cell with cellulose membrane, Extrusion method |
| In-vitro skin permeation studies | Franz diffusion cell |
| In-vivo skin permeation ability | Confocal scanning laser microscopy (CSLM), Fluorescence microscopy, histological study used to determine the bioadhesive potential and retention of transfersomes in the skin [93] |
| Stability studies | DLS method, Transmission electron microscopy |
| No. | Drug | Methods of Preparation and Formulation Details | Inference | Reference |
|---|---|---|---|---|
| 1. | Insulin | Thin-film hydration technique (10 Pa), ethanolic SPC, SC (8.7 wt % SPC, 1.3 wt % SC, 8.5 vol % ethanol), triethanolamine–HCl buffer (pH 6.5) Subjected to intermediate-pressure homogenization or ultrasonication | Therapeutically significant hypoglycemia was induced in both mice and humans, with a good efficacy. as well as reproducibility | [54,74] |
| 2. | Resveratrol | High-pressure homogenization technique (5 cycles, 1500 bar), PC, TW20, Plantacare® 1200 UP, TW80 | Antioxidant activity was not affected by coating, improved instability, bioavailability, solubility and safety | [79] |
| 3. | Epigallocatechin-3-gallate (EGCG) and hyaluronic acid | Modified thin-film hydration method followed by high-pressure homogenization technique, chloroform:methanol (4:1 v/v), SPC, SC, hydration by PBS (pH 6.8); after removing the film, the mixture was passed through a high-pressure homogenizer (1000–1200 bars, 10 cycles) | Promising free radical-scavenging effect with considerably high skin permeation and deposition of EGCG | [100] |
| 4. | Triamcinolone-acetonide | Thin-film hydration technique (10 Pa; 12 h), methanol/chloroform (1:1 v/v), SPC as an ethanolic solution (1:1 w/v), TW80 (9:11 w/w) relative to SPC, buffer (pH = 6.5), homogenized by sonication | Prolonged anti-inflammatory activity and 10-fold dose reduction to achieve the therapeutic level compared to the conventional formulation | [101] |
| 5. | Corticosteroids Glucocortico steroids Hydrocortisone and dexamethasone | Conventional film method (10 Pa, 12 h), methanol/chloroform (1:1 v/v), SPC, TW20 (1:1 molar ratio relatively to SPC), buffer (pH = 6.5), homogenized by gentle sonication | Improved biological potency, prolonged effect and reduced therapeutic dosage | [102,105] |
| 6. | Diclofenac sodium | Vortexing-sonication method and Rotary evaporation–sonication method (Despite the simple and less time-consuming nature of the vortexing method, rotary evaporation method was recommended), chloroform and methanol (2:1, v/v), EPC, SC, SDC, TW80, SP80, SP85, PBS (pH 7.4), sonicated in a bath sonicator | Maximum deformability was provided by vesicles consisted with tween 80 and more effective compared to bile salts and spans and significantly improved the in vitro skin delivery of the drug | [75] |
| Thin-film hydration method, chloroform and ethanol, soya lecithin, SP20, SP60, SP80, PBS (pH 7.4) | Formulation with span 60 exhibited good entrapment efficiency and stability | [101] | ||
| Rotary evaporation method, chloroform-methanol mixture (3:1), soya lecithin, CH, SP80 | Significantly higher amount of cumulative permeation, steady state flux, permeability coefficient, residual drug into skin and promising stability over three months [56] | [102] | ||
| Suspension homogenization (e.g., sonication), soy phosphatidylcholine, drug-to-lipid ratio between 1/4 and 1/9 | Has shown the potential to replace combined oral/topical diclofenac administration in humans | [106] | ||
| 7. | Celecoxib | modified handshaking method, chloroform:methanol (3:1 v/v), SPC, SDC, hydrated with PBS (pH 7.4), sonicated using bath sonicator | Proven to be therapeutically effective drug delivery system for treatment of rheumatoid arthritis | [92] |
| 8. | Meloxicam [80] | Sonication method, chloroform: methanol (2:1 v/v), bilayer formation by EPC and either CH, SC, sodium oleate or dicetylphosphate in a molar ratio of 10:2 | Significantly higher skin permeation | [40] |
| 9. | Mefenamic acid | Modified handshaking technique and thin-film hydration technique, SPC, SP60, chloroform:ethanol (2:1), PBS (pH 7.4), stirred in orbitary shaker | Thin-film hydration method produced better results with highest drug content, spreadability and sustained drug release profile for 12 h | [107] |
| 10. | Ketoprofen | Diractin® (Trademark) Ketoprofen in transfersomes (nondisclosure of preparation methods and formulation details) | Superiorly effective in relieving the pain of knee osteoarthritis over a 6-week treatment period compared to placebo and comparatively fewer adverse events | [25,108] |
| Proved to be efficacious in relieving pain from both eccentric muscle contractions and muscle over-exercise | [109] | |||
| 11. | Ibuprofen | Lipid film hydration by rotary evaporation method, SPC, SP80, tween TW80, ethanol, PBS | Promising prolonged delivery system with reasonably good stability characteristics | [110] |
| P90G, SP80 for F1, F2, F3 and F4 were 90:10, 85:15, 80:20 and 75:25 by direct mixing method | Result showed that F4 was the best transfersomes. With promising results for entrapment efficiency and increased in vitro skin permeation | [111] | ||
| 12 | Curcumin | Modified handshaking method, ethanol:chloroform (1:1), lecithin, TW80 and SP80, lecithin:surfactant ratio (95:05,85:15), solvents (ethanol, isopropyl alcohol), PBS (pH 7.4) | Exhibit potent anti-inflammatory properties with better permeation and bioavailability | [112,113] |
| 13 | Curcuma longa extract | Conventional rotary evaporation technique, chloroform:methanol (2:1), lecithin, TW80 and TW20, subjected to sonication | Promising photoprotective properties were observed with resulting improved skin properties (skin hydration and sebum content) with better skin penetration | [114,115] |
| 14 | Capsaicin | Conventional thin-film hydration method, P90G dissolved in ethanol, TW80, hydrated with distilled water, sonicated by bath sonicator | In vivo antiarthritic activity study exhibited superior inhibitory activity (in reducing arthritis and associated inflammations), enhanced permeability and better tolerance | [116] |
| Thin-layer method, PC and the surfactant (SP80, TW80 and mixture of SP80 and TW80) (ratio 85:15) dissolved in dichloromethane, PBS (pH 7.4) | The transfersomal formulation using Tween 80 resulted in the best characteristics (the highest entrapment efficiency, the smallest particle size, the best deformability index and the highest penetration) | [72] | ||
| 15 | Vincristine | Dry-film and ultrasonic dispersing methods, Lecithin to SDC 70/20 | Enhanced skin permeation and entrapment efficiency | [117] |
| Dry-film and ultrasonic dispersing methods | Exhibited good lymph targeting ability | [118] | ||
| 16 | Tamoxifen | Thin-film hydration technique, chloroform, P90G, SP80, hydrated using triple distilled water; suspension was vortexed | Immense potential in management of psoriasis | [119] |
| 17 | Doxorubicin loaded hyaluronic acid modified transfersomes | Lipid film method, chloroform:ethanol (1:1, v/v), lecithin, GMS, SDC, PBS (pH 7.4), size reduction with sonication | Enhanced absorption by lymphatics and improved uptake by tumor cells | [120] |
| 18 | 5-fluorouracil | Conventional rotary evaporation sonication method, chloroform and methanol (3:1 v/v), Lipoid S 100 (SPC), SP80, TW80 (95–80:5–20% w/w PC:surfactant), hydrated with 10% v/v ethanol in PBS (pH 6.5), subjected to sonication | Exhibited better skin penetration, as well as skin deposition, of the drug | [121] |
| 19 | Embelin | Thin-film hydration method, SP80 and TW80 | Can be potentially used for the treatment of skin cancer | [122] |
| 20 | Felodipine | Vortexing-sonication method, SPC, EPC, TW80, SP80, lipid:edge activator (95:5) | The composition variation and the preparation method exhibited significant effects on the vesicles’ characteristics. Transfersomes rapidly, as well as noninvasively, permeated across the skin and achieved rapid therapeutic plasma drug levels at a lower dose | [77] |
| 21 | Telmisartan | Conventional rotary evaporation sonication method, chloroform:methanol (1:1), SPC was melted, dissolved in ethanol and SC, PBS (pH 6.4), sonicated using probe sonicator | Enhanced transdermal permeation and revealed to have prolonged release of the drug | [123] |
| 22. | Eprosartan mesylate | Thin-film hydration technique, chloroform–methanol (2:1), P90G, SP80 and SDC, PBS (pH 7.4), sonication using a probe sonicator | Exhibited good entrapment of the drug and better transdermal flux | [90] |
| 23. | Buspirone hydrochloride | Thin-layer evaporation technique, chloroform/methanol (2:1 v/v), EPC and TW80 (molar ratio 5:1); oleic acid was incorporated in some formulations as a transdermal permeation enhancer, hydrated with distilled water or hydroalcoholic solution, subjected to sonication | Promising physical stability, improved permeation and accurate dosing of potent hydrophilic drug | [85] |
| 24. | Sertraline | Conventional rotary evaporation sonication method, ethanol, soya lecithin, SP80, hydrated with 7% v/v ethanol, subjected to sonication | Better antidepressant activity, with significantly higher advanced permeation characteristics | [124] |
| 25 | Tetanus-toxoid | Ethanolic solution of SPC was mixed with SDC (95:5; 90:10; 85:15; 80:20 and 75:25% w/w); PBS (pH 6.5) and the obtained suspension was pushed through a series of 0.45-, 0.22-, 0.10- and 0.05-µm polycarbonate membrane filters | Potential system of noninvasive topical immunization | [125,126] |
| 26. | Lidocaine | Thin-film hydration method, SPC, CH, SC, SP80, and brij 35 different molar ratios were dissolved in a mixture of methanol:chloroform:ethanol)at (2:2:1) a v/v/v ratio, isotonic phosphate buffer (pH 5.8), subjected to sonication | Enhanced skin permeation with increased local anesthetic efficacy | [91,94] |
| 27. | Repaglinide | Handshaking thin-film hydration method, methanol:chloroform (3:1), soy lecithin, SP80, SP60, SP40, TW80, PBS (pH 6.8), sonicated using bath sonicator | Improved topical delivery, site specificity and prolonged release of the antihyperglycemic agent | [127,128] |
| 28. | Itraconazole | Thin-film hydration method, SPC, TW80, SP80, chloroform: methanol (3:1), phosphate buffer (pH 6.8), sonicated using for 30 min | Promising results with targeted and prolonged release of the drug | [129] |
| 29. | Miconazole nitrate | Thin lipid film hydration technique, chloroform:methanol (2:1, v/v), soya lecithin, SP80, TW80, PBS (pH 7.4), sonicated using the sonicator digital sonifier | Showed a relatively higher antifungal activity than the standard commercial product | [83] |
| 30. | Ketoconazole | Conventional solvent evaporation method, P90 G, ethanolic solution of Lipoid S100, TW80 | Showed promising antimicrobial activity and excellent potential for the delivery of the drug | [93] |
| 31 | Raloxifene hydrochloride | Rotary evaporation method using chloroform:methanol (2:1), P90G:SP80 (85:15 w/w), hydrated with water, vesicle size reduction by sonication | Ex-vivo findings indicated a great potential for transdermal delivery | [130] |
| Conventional thin-layer rotary evaporation method, chloroform and methanol (2:1, v/v), P90G, SDC, PBS (pH 6.5), subjected to sonication | Proved a significantly superior amount of drug permeation and deposition in the skin and identified to be a superior alternative compared to oral delivery [32] | [65] | ||
| 32. | Tizanidine HCl | Conventional rotary evaporation method, chloroform, L-a-PC, CH, SP80, TW80, SDC, Brij 35, PBS, sonicated using a bath sonicator | Successively enhanced bioavailability and prolonged release of the drug; use for the treatment of spasticity | [56] |
| 33. | Sildenafil Citrate | Thin-film hydration and sonication method, chloroform and methanol (1:1), P90 G, sodium lauryl sulphate, SP80, TW80, cetrimide, PBS (pH 5.8), sonicated using probe sonicator | Treatment for erectile dysfunction. Improved transdermal permeation and bioavailability with reduced dose administration frequency | [102,131,132] |
| 34. | Interleukin-2 and Interferon-α | PC, SC, PBS | Agents were incorporated in the transfersomes for immunotherapy in sufficient concentrations and in their biological active form | [133] |
| 35. | Cyclodextrin-colchicine complex | Conventional rotary evaporation sonication method, chloroform:methanol (2:1), SPC, CH, SP80, SP60, hydrated with drug, drug-cyclodextrin complex or fluorescence marker solution in ethanol, subjected to sonication | Showed 6-fold increase in transdermal flux and better and sustained antigout activity in rats. Enhanced skin accumulation, prolonged drug release, and improved the site-specificity of colchicine | [134] |
| Colchicine | Increased skin penetration | [135] | ||
| 36. | Caffeine | Thin-film hydration method, chloroform, DLPC:DPGluc:CH (35:7:7), hydrated with caffeine solution (2% in water) | Showed significantly greater permeation across the stratum corneum and significant enhancement of hydrophilic drug caffeine penetration into hair follicles | [136] |
| 37. | Minoxidil and caffeine | Modified thin-film hydration method, SPC, TW20, TW80, lecithin was mixed with various amounts of edge activators and dissolved in chloroform | Increasing the ratio of polysorbate enhanced the entrapment efficiency of minoxidil and caffeine. Topical application of this formulation more effectively promoted the hair growth in rats compared to the commercial product | [137] |
| 38. | Tacrolimus | Thin lipid film hydration method, SPC, SDC, chloroform/methanol (2:1 v/v), hydration medium phosphate buffer, pH 7.2 | Better antipsoriatic activities compared to liposomes due to better skin permeations | [138] |
| 39. | Estradiol | Bath sonication and homogenization by manual extrusion, DPPC, SP80, TW80, SDC | Superior estradiol skin delivery compared to traditional liposomes | [139] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Opatha, S.A.T.; Titapiwatanakun, V.; Chutoprapat, R. Transfersomes: A Promising Nanoencapsulation Technique for Transdermal Drug Delivery. Pharmaceutics 2020, 12, 855. https://doi.org/10.3390/pharmaceutics12090855
Opatha SAT, Titapiwatanakun V, Chutoprapat R. Transfersomes: A Promising Nanoencapsulation Technique for Transdermal Drug Delivery. Pharmaceutics. 2020; 12(9):855. https://doi.org/10.3390/pharmaceutics12090855
Chicago/Turabian StyleOpatha, Shakthi Apsara Thejani, Varin Titapiwatanakun, and Romchat Chutoprapat. 2020. "Transfersomes: A Promising Nanoencapsulation Technique for Transdermal Drug Delivery" Pharmaceutics 12, no. 9: 855. https://doi.org/10.3390/pharmaceutics12090855