A Prospective Randomized Study: The Usefulness and Efficacy of Negative Pressure Wound Therapy with Lipidocolloid Polyester Mesh Compared to Traditional Negative Pressure Wound Therapy for Treatment of Pressure Ulcers



Abstract
:1. Introduction
2. Materials and Methods
2.1. Size of the Wound
2.2. Granulation Tissue Grade
2.3. Photo Analysis
2.4. Bacterial Culture
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Bacterial Cculture
3.3. Granulation Tissue Grade
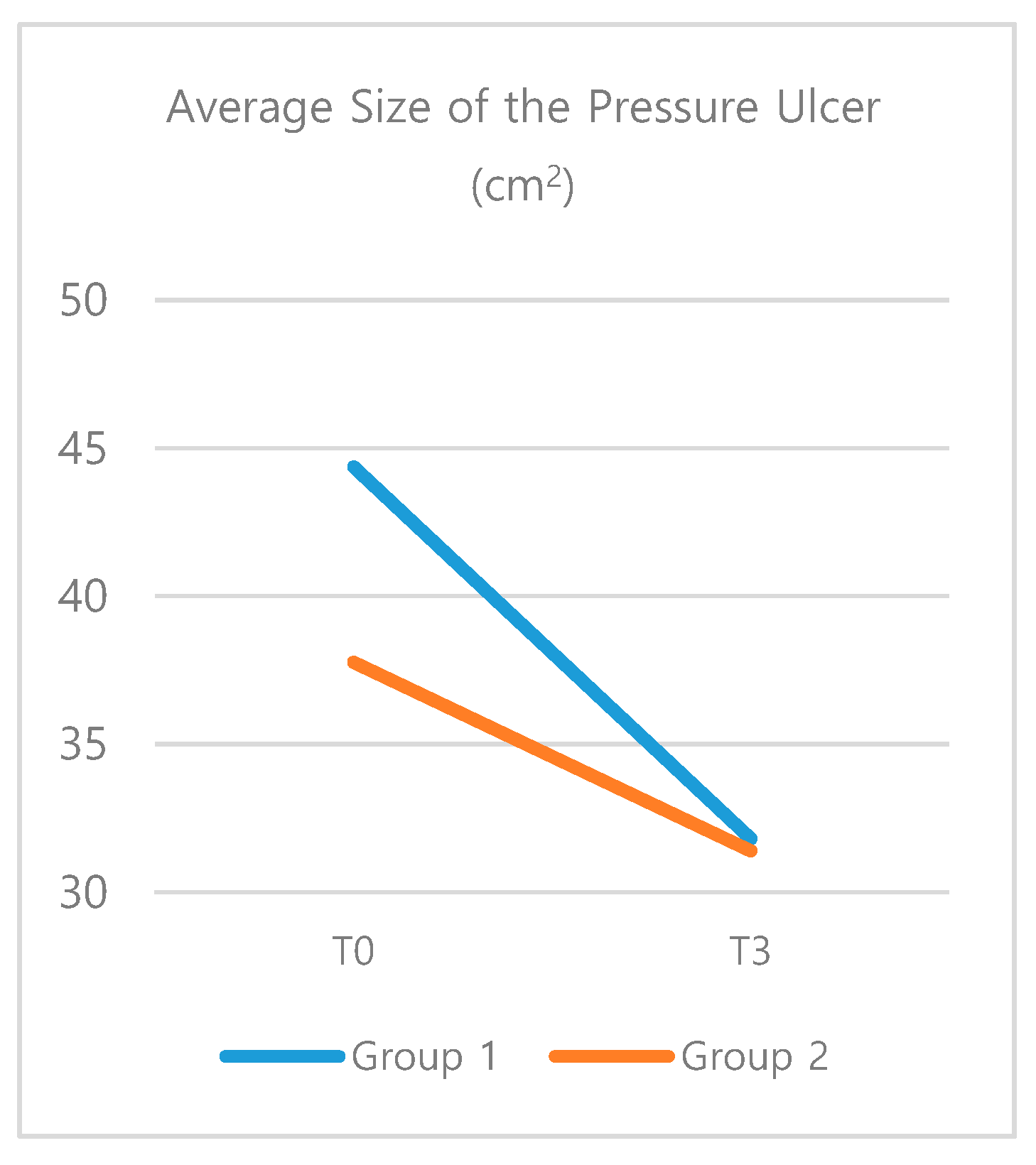
3.4. Size of the Pressure Ulcer
3.5. Photo Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bluestein, D.; Javaheri, A. Pressure ulcers: Prevention, evaluation, and management. Am. Fam. Phys. 2008, 78, 1186–1194. [Google Scholar]
- Fronek, K.; Zweifach, B.W. Microvascular pressure distribution in skeletal muscle and the effect of vasodilation. Am. J. Physiol. Content 1975, 228, 791–796. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, W.; Strecker, W.; Bombelli, M.; Kinzl, L. Vacuum sealing as treatment of soft tissue damage in open fractures. Der Unf. 1993, 96, 488–492. [Google Scholar]
- Gebala-Prajsnar, K.; Stanek, A.; Pasek, J.; Prajsnar, G.; Berszakiewicz, A.; Sierón, A.; Cholewka, A. Selected physical medicine interventions in the treatment of diabetic foot syndrome. Acta Angiol. 2016, 21, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Schimp, V.L.; Worley, C.; Brunello, S.; Levenback, C.C.; Wolf, J.K.; Sun, C.C.; Bodurka, D.C.; Ramirez, P.T. Vacuum-assisted closure in the treatment of gynecologic oncology wound failures. Gynecol. Oncol. 2004, 92, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Birke-Sorensen, H.; Malmsjo, M.; Rome, P.; Hudson, D.; Krug, E.; Berg, L.; Bruhin, A.; Caravaggi, C.; Chariker, M.; Depoorter, M.; et al. Evidence-based recommendations for negative pressure wound therapy: Treatment variables (pressure levels, wound filler and contact layer)—Steps towards an international consensus. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, S1–S16. [Google Scholar] [CrossRef] [PubMed]
- Krasner, D.L. Managing wound pain in patients with vacuum-assisted closure devices. Ostomy Wound Manag. 2002, 48, 38. [Google Scholar]
- Lindstedt, S.; Hansson, J.; Hlebowicz, J. Comparative study of the microvascular blood flow in the intestinal wall during conventional negative pressure wound therapy and negative pressure wound therapy using paraffin gauze over the intestines in laparostomy. Int. Wound J. 2011, 9, 150–155. [Google Scholar] [CrossRef] [PubMed]
- Téot, L.; Lambert, L.; Ourabah, Z.; Bey, E.; Steenman, C.; Wierzbiecka, E.; Malikov, S.; Charles, J.; Vives, F.; Bohbot, S. Use of topical negative pressure with a lipidocolloid dressing: Results of a clinical evaluation. J. Wound Care 2006, 15, 355–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braakenburg, A.; Obdeijn, M.C.; Feitz, R.; Van Rooij, I.A.L.M.; Van Griethuysen, A.J.; Klinkenbijl, J.H.G. The clinical efficacy and cost effectiveness of the vacuum-assisted closure technique in the management of acute and chronic wounds: A randomized controlled trial. Plast. Reconstr. Surg. 2006, 118, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Ciliberti, M.; De Lara, F.; Serra, G.; Tafuro, F.; Iazzetta, F.M.; Filosa, A.; Scognamiglio, R.; Ciliberti, G.; Veneri, M.R. The effect of a bacteria- and fungi-binding mesh dressing on the bacterial load of pressure ulcers treated with negative pressure wound therapy: A pilot study. Wounds 2016, 28, 408–420. [Google Scholar] [PubMed]
- Bernard, F.; Barrault, C.; Juchaux, F.; Laurensou, C.; Apert, L. Stimulation of the proliferation of human dermal fibroblasts in vitro by a lipidocolloid dressing. J. Wound Care 2005, 14, 215–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Black, J.; Baharestani, M.M.; Cuddigan, J.; Dorner, B.; Edsberg, L.; Langemo, D.; Posthauer, M.E.; Ratliff, C.; Taler, G.; National Pressure Ulcer Advisory Panel. National Pressure Ulcer Advisory Panel’s updated pressure ulcer staging system. Adv. Skin Wound Care 2007, 20, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Argenta, L.; Morykwas, M. Vacuum-assisted closure: A new method for wound control and treatment: Clinical experience. Ann Plast Surg 1997, 38, 563–576. [Google Scholar] [CrossRef] [PubMed]
- Morykwas, M.J.; Argenta, L.C.; Shelton-Brown, E.I. Vacuum-assisted closure: A new method for wound control and treatment: Animal studies and basic foundation. Ann. Plast. Surg. 1997, 38, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Shiroky, J.; Lillie, E.; Muaddi, H.; Sevigny, M.; Choi, W.J.; Karanicolas, P. The impact of negative pressure wound therapy for closed surgical incisions on surgical site infection: A systematic review and meta-analysis. Surgery 2020, 167, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Benrashid, E.; Youngwirth, L.M.; Guest, K.; Cox, M.W.; Shortell, C.K.; Dillavou, E.D. Negative pressure wound therapy reduces surgical site infections. J. Vasc. Surg. 2020, 71, 896–904. [Google Scholar] [CrossRef] [PubMed]
- Costa, M.L.; Achten, J.; Knight, R.; Bruce, J.; Dutton, S.J.; Madan, J.; Dritsaki, M.; Parsons, N.; Fernandez, M.; Grant, R.; et al. Effect of incisional negative pressure wound therapy vs standard wound dressing on deep surgical site infection after surgery for lower limb fractures associated with major trauma: The whist randomized clinical trial. JAMA 2020, 323, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.J.; Attinger, C.E.; Steinberg, J.S.; Evans, K.K.; Powers, K.A.; Hung, R.W.; Smith, J.R.; Rocha, Z.M.; Lavery, L.A. The impact of negative-pressure wound therapy with instillation compared with standard negative-pressure wound therapy. Plast. Reconstr. Surg. 2014, 133, 709–716. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Screening Period (1~14 days before Treatment) |
|
| Treatment period (the day of Starting Treatment) |
|
| Follow Period (~3 Weeks after the Treatment) |
|
| Characteristics | Categories | Exp. (n = 19) | Cont. (n = 19) | t or x2 | p |
|---|---|---|---|---|---|
| M ± SD/n (%) | M ± SD/n (%) | ||||
| Gender | Male | 10 (52.6) | 12 (63.2) | 0.43 | 0.511 |
| Female | 9 (47.4) | 7 (36.8) | |||
| Age (years) | 60.95 ± 12.40 | 60.63 ± 21.38 | 0.56 | 0.956 | |
| Period of prevalence (months) | 9.26 ± 12.17 | 5.68 ± 3.19 | 1.19 | 0.248 | |
| Location of pressure sore | Coccyx | 12 (63.2) | 14 (73.7) | 3.82 | 0.431 |
| Ischium | 2 (10.5) | 4 (21.1) | |||
| Trochanter | 3 (15.8) | 1 (5.3) | |||
| others | 2 (10.6) | 0 (0) | |||
| Stage of pressure sore | Stage 3 | 1 (5.3) | 0 (0) | 1.03 | 0.311 |
| Stage 4 | 18 (94.7) | 19 (100) | |||
| Risk factors | Age over 65 | 11 (57.9) | 10 (52.6) | 0.11 | 0.744 |
| BMI (kg/m2) | 19.55 (4.2) | 20.38 (4.6) | 0.58 | 0.570 | |
| Spinal cord injury | 7 (36.8) | 5 (26.3) | 0.49 | 0.485 | |
| Brain damage | 8 (42.1) | 10 (52.6) | 0.42 | 0.516 | |
| Acute phase disease | 16 (84.2) | 15 (78.9) | 0.18 | 0.656 | |
| DM | 7 (36.8) | 4 (21.1) | 1.15 | 0.283 | |
| ICU admission | 5 (26.3) | 5 (26.3) | 0.00 | 1.000 | |
| Bacterial Count | Group 1 (n = 19) | Group 2 (n = 19) | Group1 (p) | Group2 (p) |
|---|---|---|---|---|
| N (%) | N (%) | |||
| Improved | 11 (57.9) | 8 (42.1) | 1.76 | 0.415 |
| No interval change | 2 (10.5) | 5 (26.3) | ||
| Aggravation | 6 (31.6) | 6 (31.6) |
| Variable | Group | T0 | T3 | Source | F | p |
|---|---|---|---|---|---|---|
| M (SD) | M (SD) | |||||
| Size | Exp. (N = 19) | 44.37 (± 7.79) | 31.81 (± 5.43) | G | 0.15 | 0.704 |
| Md = 12.56, p = 0.001 | T | 14.13 | 0.001 | |||
| Cont. (N = 19) | 37.77 (± 7.79) | 31.40 (± 5.43) | G × T | 1.51 | 0.227 | |
| Md = 6.37, p = 0.082 | ||||||
| Granulation tissue grade | Exp. (N = 19) | 1.29 (± 0.12) | 3.58 (± 0.15) | G | 0.51 | 0.478 |
| Md = –2.29, p ≤ 0.001 | T | 567.21 | < 001 | |||
| Cont. (N = 19) | 1.15 (± 0.116) | 3.49 (± 0.153) | G × T | 0.07 | 0.778 | |
| Md = –2.34, p ≤ 0.001 | ||||||
| Photo analysis | Exp. (N = 19) | 3.26 (± 0.15) | 4.63 (± 0.22) | G | 0.05 | 0.820 |
| Md = –1.37, p ≤ 0.001 | T | 114.95 | < 001 | |||
| Cont. (N = 19) | 3.16 (± 0.15) | 4.63 (± 0.22) | G × T | 0.16 | 0.694 | |
| Md = –1.47, p ≤ 0.001 | ||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, W.; Lee, N.; Han, E.J.; Roh, T.S.; Lee, W.J. A Prospective Randomized Study: The Usefulness and Efficacy of Negative Pressure Wound Therapy with Lipidocolloid Polyester Mesh Compared to Traditional Negative Pressure Wound Therapy for Treatment of Pressure Ulcers. Pharmaceutics 2020, 12, 813. https://doi.org/10.3390/pharmaceutics12090813
Baek W, Lee N, Han EJ, Roh TS, Lee WJ. A Prospective Randomized Study: The Usefulness and Efficacy of Negative Pressure Wound Therapy with Lipidocolloid Polyester Mesh Compared to Traditional Negative Pressure Wound Therapy for Treatment of Pressure Ulcers. Pharmaceutics. 2020; 12(9):813. https://doi.org/10.3390/pharmaceutics12090813
Chicago/Turabian StyleBaek, Wooyeol, Nara Lee, Eun Jin Han, Tai Suk Roh, and Won Jai Lee. 2020. "A Prospective Randomized Study: The Usefulness and Efficacy of Negative Pressure Wound Therapy with Lipidocolloid Polyester Mesh Compared to Traditional Negative Pressure Wound Therapy for Treatment of Pressure Ulcers" Pharmaceutics 12, no. 9: 813. https://doi.org/10.3390/pharmaceutics12090813