Size Distribution of Colistin Delivery by Different Type Nebulizers and Concentrations During Mechanical Ventilation


 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
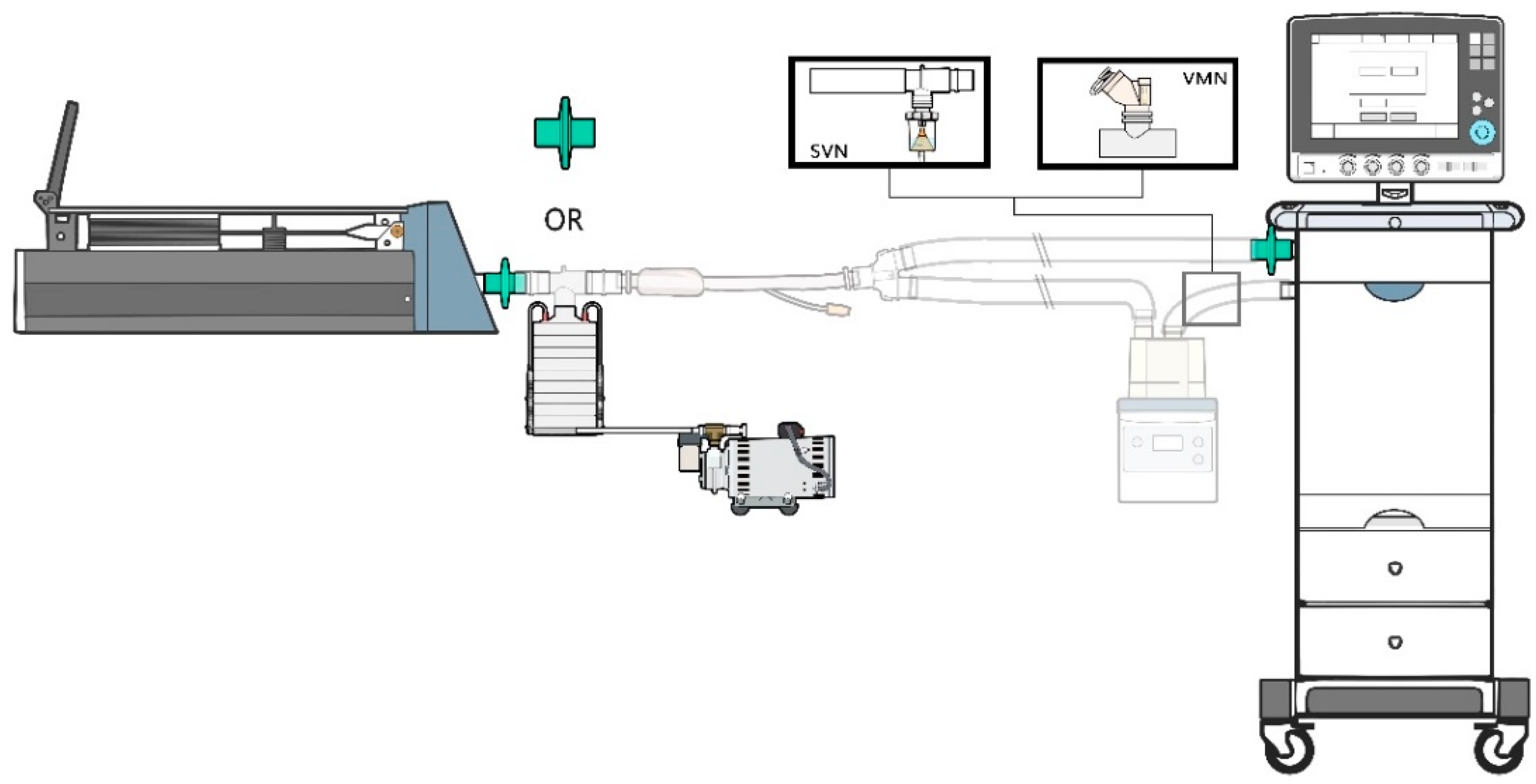
2.1. Lung Model
2.2. Study Design
2.3. Drug Delivery and Particle Size Distribution Measurement
2.3.1. Delivered Drug Dose
2.3.2. Nebulization Time
2.3.3. Drug Delivery Efficiency
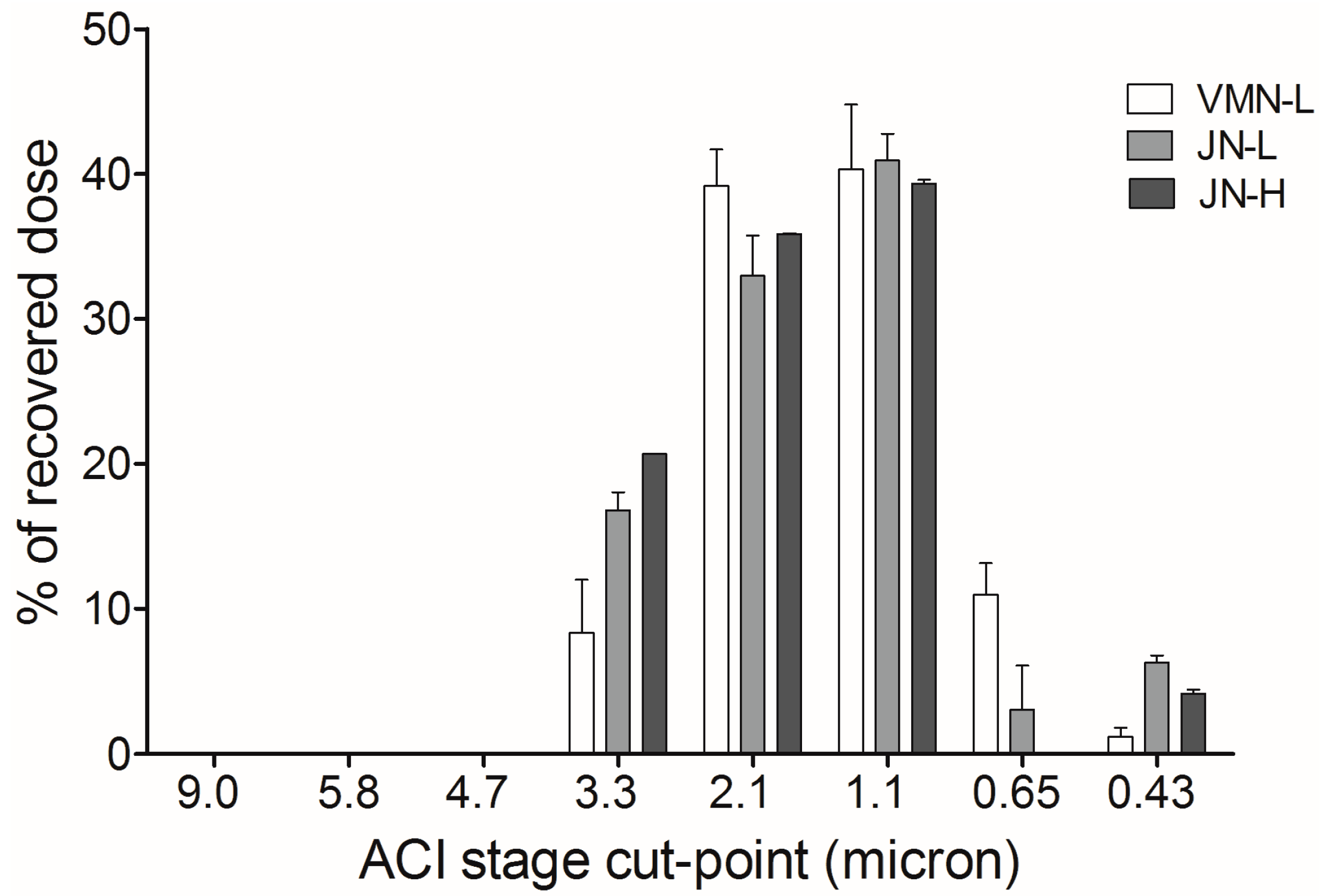
2.3.4. Particle Size Distribution
2.4. Drug Analysis
2.5. Statistical Analysis
3. Results
3.1. Viscosity of Colistin Solutions
3.2. Nebulizer Performance
3.3. Particle Size Distribution
4. Discussion
4.1. Delivered Drug Dose
4.2. Particle Size Distribution
4.3. Clinical Implication
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wenzler, E.; Fraidenburg, D.R.; Scardina, T.; Danziger, L.H. Inhaled Antibiotics for Gram-Negative Respiratory Infections. Clin. Microbiol. Rev. 2016, 29, 581–632. [Google Scholar] [CrossRef] [Green Version]
- Boisson, M.; Jacobs, M.; Gregoire, N.; Gobin, P.; Marchand, S.; Couet, W.; Mimoz, O. Comparison of intrapulmonary and systemic pharmacokinetics of colistin methanesulfonate (CMS) and colistin after aerosol delivery and intravenous administration of CMS in critically ill patients. Antimicro. Agents Chemother. 2014, 58, 7331–7339. [Google Scholar] [CrossRef]
- Vardakas, K.Z.; Voulgaris, G.L.; Samonis, G.; Falagas, M.E. Inhaled colistin monotherapy for respiratory tract infections in adults without cystic fibrosis: A systematic review and meta-analysis. Int. J. Antimicrob. Agents 2018, 51, 1–9. [Google Scholar] [CrossRef]
- Rodvold, K.A.; Yoo, L.; George, J.M. Penetration of anti-infective agents into pulmonary epithelial lining fluid: Focus on antifungal, antitubercular and miscellaneous anti-infective agents. Clin. Pharmacokinet. 2011, 50, 689–704. [Google Scholar] [CrossRef]
- Ehrmann, S.; Chastre, J.; Diot, P.; Lu, Q. Nebulized antibiotics in mechanically ventilated patients: A challenge for translational research from technology to clinical care. Ann. Intensive Care 2017, 7, 78. [Google Scholar] [CrossRef]
- Sole-Lleonart, C.; Rouby, J.J.; Blot, S.; Poulakou, G.; Chastre, J.; Palmer, L.B.; Bassetti, M.; Luyt, C.E.; Pereira, J.M.; Riera, J.; et al. Nebulization of Antiinfective Agents in Invasively Mechanically Ventilated Adults: A Systematic Review and Meta-analysis. Anesthesiology 2017, 126, 890–908. [Google Scholar] [CrossRef]
- Kofteridis, D.P.; Alexopoulou, C.; Valachis, A.; Maraki, S.; Dimopoulou, D.; Georgopoulos, D.; Samonis, G. Aerosolized plus intravenous colistin versus intravenous colistin alone for the treatment of ventilator-associated pneumonia: A matched case-control study. Clin. Infect. Dis. 2010, 51, 1238–1244. [Google Scholar] [CrossRef]
- Spapen, H.; Jacobs, R.; Van Gorp, V.; Troubleyn, J.; Honore, P.M. Renal and neurological side effects of colistin in critically ill patients. Ann. Intensive Care 2011, 1, 14. [Google Scholar] [CrossRef]
- Lee, Y.J.; Wi, Y.M.; Kwon, Y.J.; Kim, S.R.; Chang, S.H.; Cho, S. Association between colistin dose and development of nephrotoxicity. Crit. Care Med. 2015, 43, 1187–1193. [Google Scholar] [CrossRef]
- Haworth, C.S.; Foweraker, J.E.; Wilkinson, P.; Kenyon, R.F.; Bilton, D. Inhaled colistin in patients with bronchiectasis and chronic Pseudomonas aeruginosa infection. Am. J. Respir. Crit. Care Med. 2014, 189, 975–982. [Google Scholar] [CrossRef]
- Guerin, C.; Fassier, T.; Bayle, F.; Lemasson, S.; Richard, J.C. Inhaled bronchodilator administration during mechanical ventilation: How to optimize it, and for which clinical benefit? J. Aerosol. Med. Pulm. Drug Deliv. 2008, 21, 85–96. [Google Scholar] [CrossRef]
- Rello, J.; Rouby, J.J.; Sole-Lleonart, C.; Chastre, J.; Blot, S.; Luyt, C.E.; Riera, J.; Vos, M.C.; Monsel, A.; Dhanani, J.; et al. Key considerations on nebulization of antimicrobial agents to mechanically ventilated patients. Clin. Microbiol. Infect. 2017, 23, 640–646. [Google Scholar] [CrossRef] [Green Version]
- Boe, J.; Dennis, J.H.; Driscoll, B.R.; Bauer, T.T.; Carone, M.; Dautzenberg, B.; Diot, P.; Heslop, K.; Lannefors, L. European Respiratory Society Task Force on the use of nebulizers. European Respiratory Society Guidelines on the use of nebulizers. Eur. Respir. J. 2001, 18, 228. [Google Scholar]
- Mc Callion, O.N.M.; Patel, M.J. Viscosity effects on nebulisation of aqueous solutions. Int. J. Pharm. 1996, 130, 245–249. [Google Scholar] [CrossRef]
- Finlay, W.H.; Lange, C.F.; King, M.; Speert, D.P. Lung delivery of aerosolized dextran. Am. J. Respir. Crit. Care Med. 2000, 161, 91–97. [Google Scholar] [CrossRef]
- Lu, Q.; Luo, R.; Bodin, L.; Yang, J.; Zahr, N.; Aubry, A.; Golmard, J.L.; Rouby, J.J. Efficacy of high-dose nebulized colistin in ventilator-associated pneumonia caused by multidrug-resistant Pseudomonas aeruginosa and Acinetobacter baumannii. Anesthesiology 2012, 117, 1335–13347. [Google Scholar] [CrossRef]
- Kim, Y.K.; Lee, J.H.; Lee, H.K.; Chung, B.C.; Yu, S.J.; Lee, H.Y.; Park, J.H.; Kim, S.; Kim, H.K.; Kiem, S.; et al. Efficacy of nebulized colistin-based therapy without concurrent intravenous colistin for ventilator-associated pneumonia caused by carbapenem-resistant Acinetobacter baumannii. J. Thorac. Dis. 2017, 9, 555–567. [Google Scholar] [CrossRef] [Green Version]
- Athanassa, Z.E.; Markantonis, S.L.; Fousteri, M.Z.; Myrianthefs, P.M.; Boutzouka, E.G.; Tsakris, A.; Baltopoulos, G.J. Pharmacokinetics of inhaled colistimethate sodium (CMS) in mechanically ventilated critically ill patients. Intensive Care Med. 2012, 38, 1779–1786. [Google Scholar] [CrossRef]
- Hess, D.; Fisher, D.; Williams, P.; Pooler, S.; Kacmarek, R.M. Medication nebulizer performance. Effects of diluent volume, nebulizer flow, and nebulizer brand. Chest 1996, 110, 498–505. [Google Scholar] [CrossRef]
- Li, J.; Milne, R.W.; Nation, R.L.; Turnidge, J.D.; Coulthard, K. Stability of colistin and colistin methanesulfonate in aqueous media and plasma as determined by high-performance liquid chromatography. Antimicrob. Agents Chemother. 2003, 47, 1364–1370. [Google Scholar] [CrossRef]
- Wallace, S.J.; Li, J.; Rayner, C.R.; Coulthard, K.; Nation, R.L. Stability of colistin methanesulfonate in pharmaceutical products and solutions for administration to patients. Antimicrob. Agents Chemother. 2008, 52, 3047–3051. [Google Scholar] [CrossRef]
- Ari, A.; Atalay, O.T.; Harwood, R.; Sheard, M.M.; Aljamhan, E.A.; Fink, J.B. Influence of nebulizer type, position, and bias flow on aerosol drug delivery in simulated pediatric and adult lung models during mechanical ventilation. Respir. Care 2010, 55, 845–851. [Google Scholar]
- Ge, H.Q.; Wang, J.M.; Lin, H.L.; Fink, J.B.; Luo, R.; Xu, P.; Ying, K. Effect of Nebulizer Location and Spontaneous Breathing on Aerosol Delivery During Airway Pressure Release Ventilation in Bench Testing. J. Aaerosol. Med. Pulm. Drug Deliv. 2019, 32, 34–39. [Google Scholar] [CrossRef]
- Wan, G.H.; Lin, H.L.; Fink, J.B.; Chen, Y.H.; Wang, W.J.; Chiu, Y.C.; Kao, Y.Y.; Liu, C. In vitro evaluation of aerosol delivery by different nebulization modes in pediatric and adult mechanical ventilators. Respir. Care 2014, 59, 1494–1500. [Google Scholar] [CrossRef]
- Zhang, G.; David, A.; Wiedmann, T.S. Performance of the vibrating membrane aerosol generation device: Aeroneb Micropump Nebulizer. J. Aerosol. Med. Pulm. Drug Deliv. 2007, 20, 408–416. [Google Scholar] [CrossRef]
- Ghazanfari, T.; Elhissi, A.M.; Ding, Z.; Taylor, K.M. The influence of fluid physicochemical properties on vibrating-mesh nebulization. Int. J. Pharm. 2007, 339, 103–111. [Google Scholar] [CrossRef]
- Birkun, A. Exogenous pulmonary surfactant as a vehicle for antimicrobials: Assessment of surfactant-antibacterial interactions in vitro. Scientifica 2014, 2014, 930318. [Google Scholar] [CrossRef]
- Ratjen, F.; Rietschel, E.; Kasel, D.; Schwiertz, R.; Starke, K.; Beier, H.; van Koningsbruggen, S.; Grasemann, H. Pharmacokinetics of inhaled colistin in patients with cystic fibrosis. J. Antimicrob. Chemother. 2006, 57, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.L.; Ho, S.L.; Coates, A.L. Nebulizer choice for inhaled colistin treatment in cystic fibrosis. Chest 2001, 119, 250–255. [Google Scholar] [CrossRef]
- Miller, D.D.; Amin, M.M.; Palmer, L.B.; Shah, A.R.; Smaldone, G.C. Aerosol delivery and modern mechanical ventilation: In vitro/in vivo evaluation. Am. J. Respir. Crit. Care Med. 2003, 168, 1205–1209. [Google Scholar] [CrossRef]
- Yang, S.H.; Yang, T.M.; Lin, H.L.; Tsai, Y.H.; Fang, T.P.; Wan, G.H. Size distribution of salbutamol/ipratropium aerosols produced by different nebulizers in the absence and presence of heat and humidification. Pulm. Pharmacol. Ther. 2018, 48, 22–27. [Google Scholar] [CrossRef]
- Haddrell, A.E.; Davies, J.F.; Miles, R.E.; Reid, J.P.; Dailey, L.A.; Murnane, D. Dynamics of aerosol size during inhalation: Hygroscopic growth of commercial nebulizer formulations. Int. J. Pharm. 2014, 463, 50–61. [Google Scholar] [CrossRef] [Green Version]
- Lee, A.K.; Ling, T.Y.; Chan, C.K. Understanding hygroscopic growth and phase transformation of aerosols using single particle Raman spectroscopy in an electrodynamic balance. Faraday Discuss 2008, 137, 245–263. [Google Scholar] [CrossRef]
- Steckel, H.; Eskandar, F. Factors affecting aerosol performance during nebulization with jet and ultrasonic nebulizers. Eur. J. Pharm. Sci. 2003, 19, 443–455. [Google Scholar] [CrossRef]
- Najlah, M.; Vali, A.; Taylor, M.; Arafat, B.T.; Ahmed, W.; Phoenix, D.A.; Taylor, K.M.; Elhissi, A. A study of the effects of sodium halides on the performance of air-jet and vibrating-mesh nebulizers. Int. J. Pharm. 2013, 456, 520–527. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
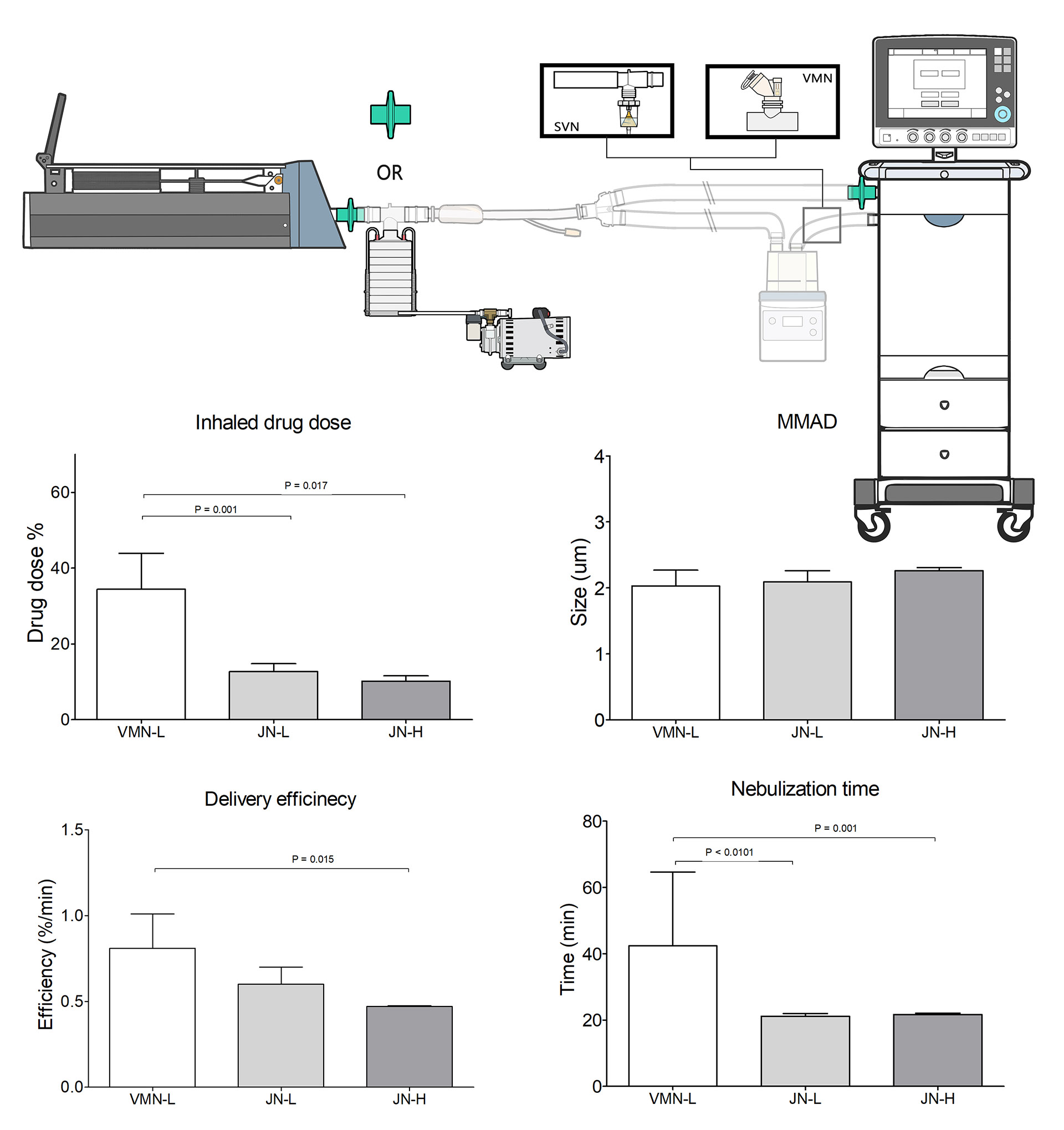
| Variables | VMN-L | JN-L | JN-H | P-Value |
|---|---|---|---|---|
| Inhaled mass (mg) | 53.80 ± 14.79 | 19.82 ± 3.34 * | 31.72 ± 4.48 * | <0.001 |
| Inhaled mass (%) | 34.44 ± 9.47 | 12.69 ± 2.14 † | 10.15 ± 1.43 † | <0.001 |
| Nebulization time (min) | 42.35 ± 2.30 | 21.12 ± 0.86 ‡ | 21.65 ± 0.42 ‡ | <0.001 |
| Delivery efficiency (mg/min) | 1.27 ± 0.32 | 0.94 ± 0.17 | 1.46 ± 0.20 § | 0.023 |
| Delivery efficiency (%/min) | 0.81 ± 0.20 | 0.60 ± 0.1 | 0.47 ± 0.06 ‖ | 0.014 |
| Variables | VMN-L | JN-L | JN-H | P-Value |
|---|---|---|---|---|
| MMAD (µm) | 2.03 ± 0.24 | 2.09 ± 0.17 | 2.26 ± 0.05 | 0.434 |
| GSD | 1.58 ± 0.14 | 1.59 ± 0.10 | 1.58 ± 0.01 | 0.994 |
| Fine particle % (1.1 to 4.7 µm) | 87.83 ± 3.08 | 90.69 ± 4.55 | 95.83 ± 0.36 | 0.128 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.-Y.; Ko, H.-K.; Fink, J.B.; Wan, G.-H.; Huang, C.-C.; Chen, Y.-C.; Lin, H.-L. Size Distribution of Colistin Delivery by Different Type Nebulizers and Concentrations During Mechanical Ventilation. Pharmaceutics 2019, 11, 459. https://doi.org/10.3390/pharmaceutics11090459
Liu C-Y, Ko H-K, Fink JB, Wan G-H, Huang C-C, Chen Y-C, Lin H-L. Size Distribution of Colistin Delivery by Different Type Nebulizers and Concentrations During Mechanical Ventilation. Pharmaceutics. 2019; 11(9):459. https://doi.org/10.3390/pharmaceutics11090459
Chicago/Turabian StyleLiu, Ching-Yi, Hsin-Kuo Ko, James B. Fink, Gwo-Hwa Wan, Chung-Chi Huang, Yu-Chun Chen, and Hui-Ling Lin. 2019. "Size Distribution of Colistin Delivery by Different Type Nebulizers and Concentrations During Mechanical Ventilation" Pharmaceutics 11, no. 9: 459. https://doi.org/10.3390/pharmaceutics11090459