Development of a UV-Stabilized Topical Formulation of Nifedipine for the Treatment of Raynaud Phenomenon and Chilblains

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Chemicals
2.2. Preparation of Topical Nifedipine
2.3. Light Exposure
2.4. Extraction of Nifedipine from the Cream
2.5. Spectrophotometric Assay
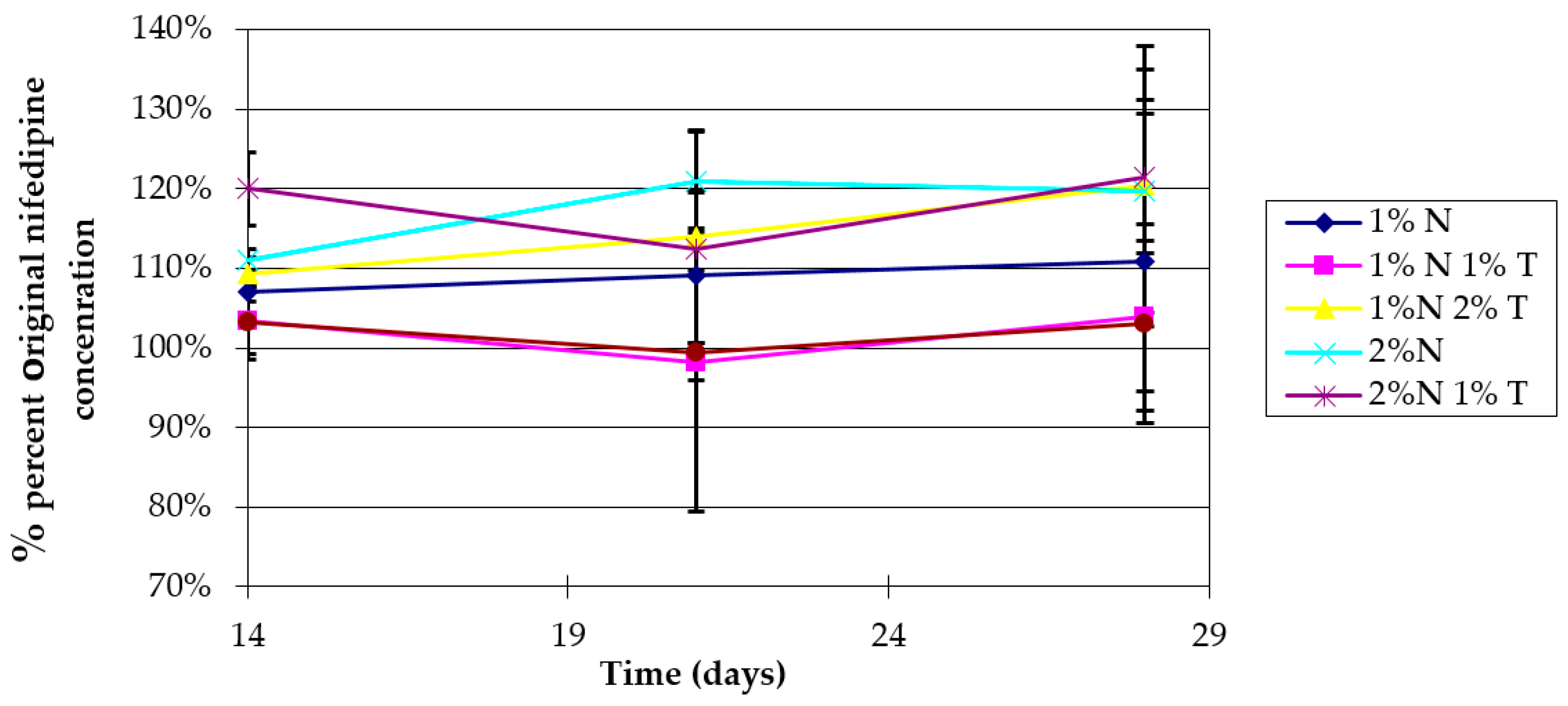
2.6. Stability Studies
2.7. HPLC Assay
2.8. Emulsion Phase Stability Analysis
2.9. High-Performance Liquid Chromatography–Photodiode Array (HPLC-PDA) For Ketoprofen Sparing
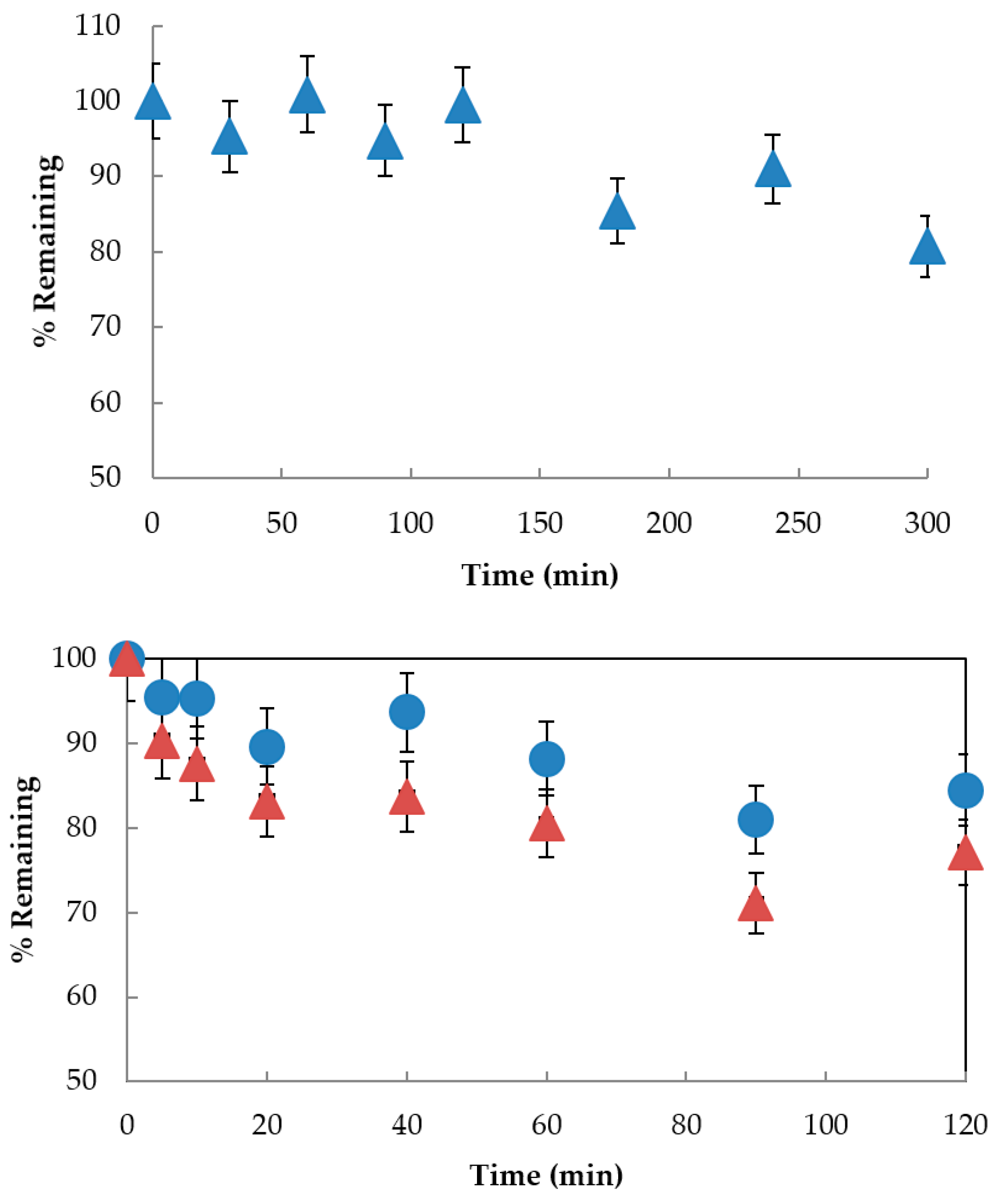
2.10. Time Course for UV Irradiation of Rutin and Ketoprofen
2.11. Ketoprofen Sparing
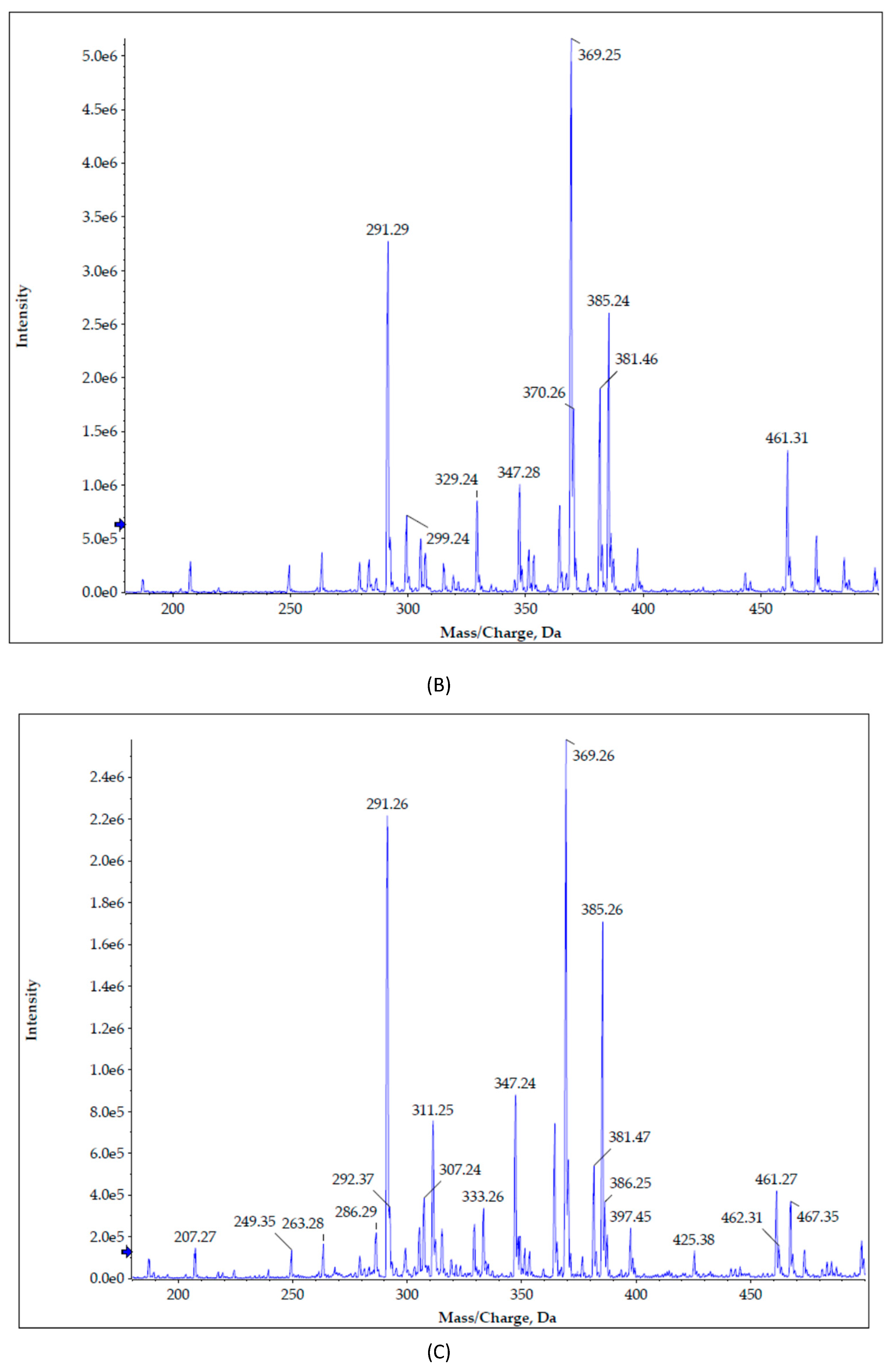
2.12. Mass Spectrometry Analysis of Nifedipine and its Photo-degradants
2.13. Statistical Analysis
3. Results and Discussion
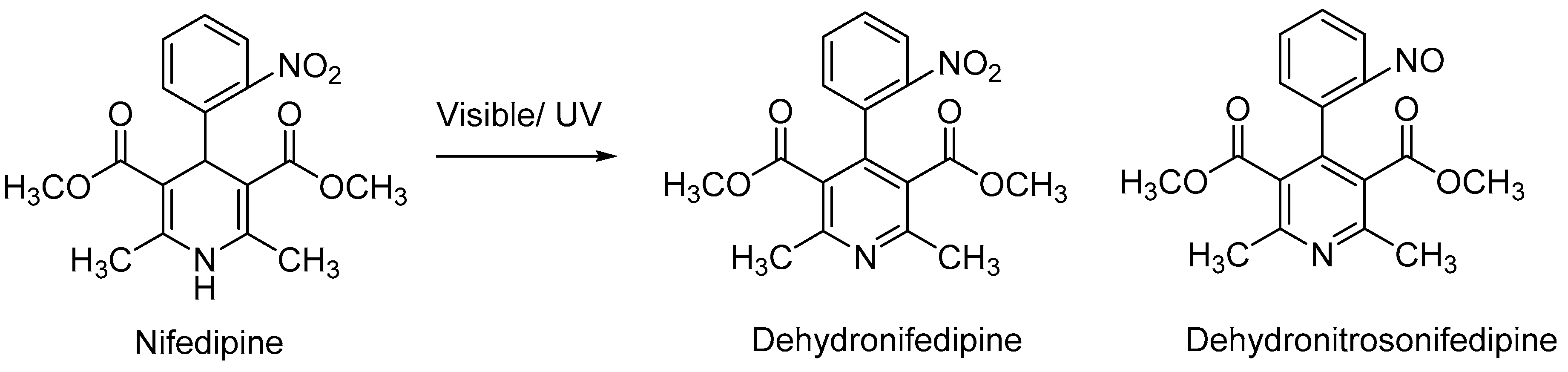
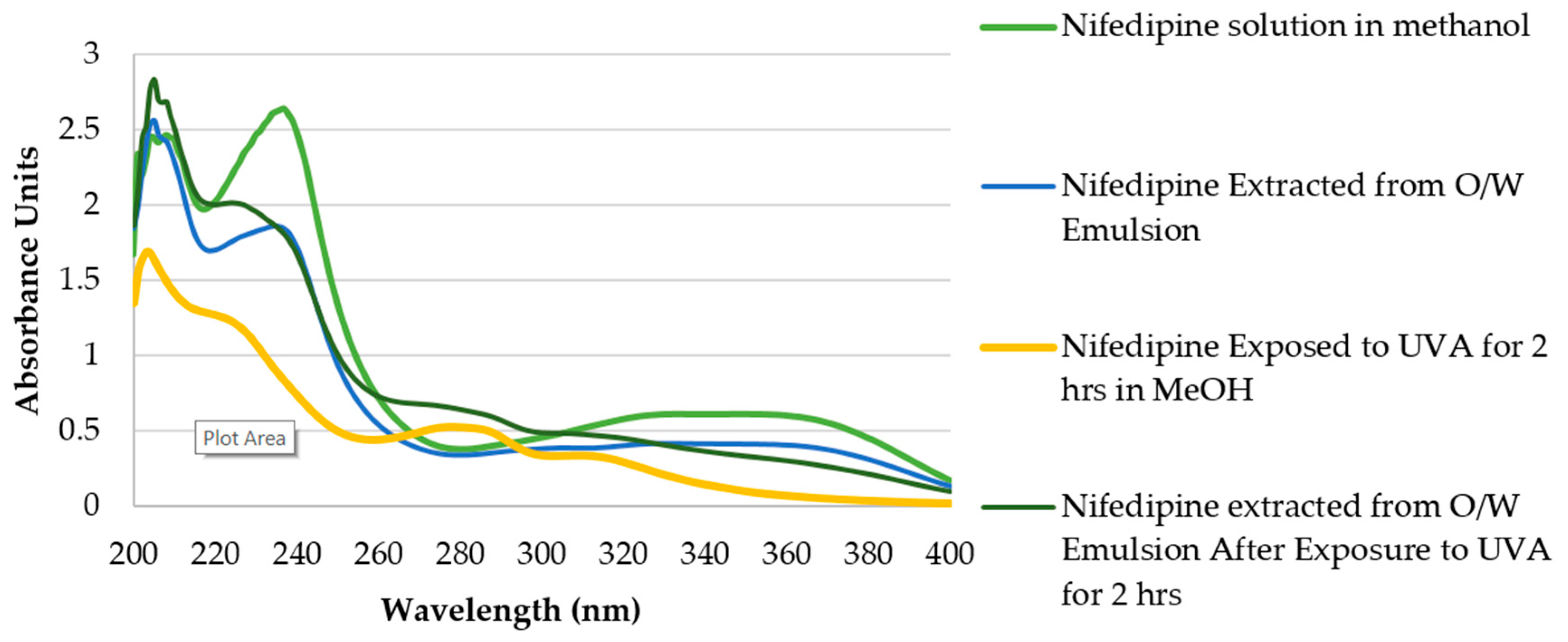
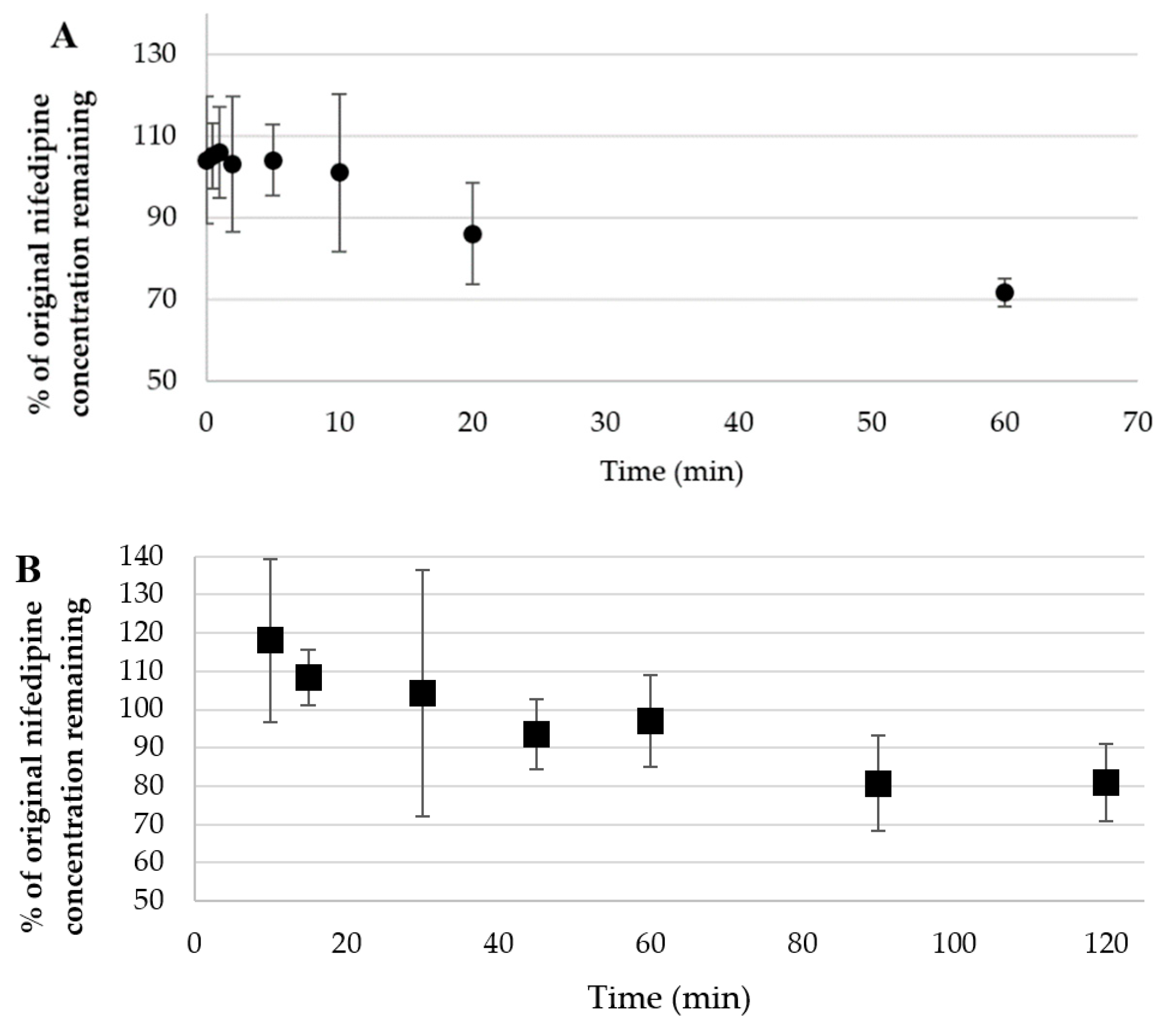
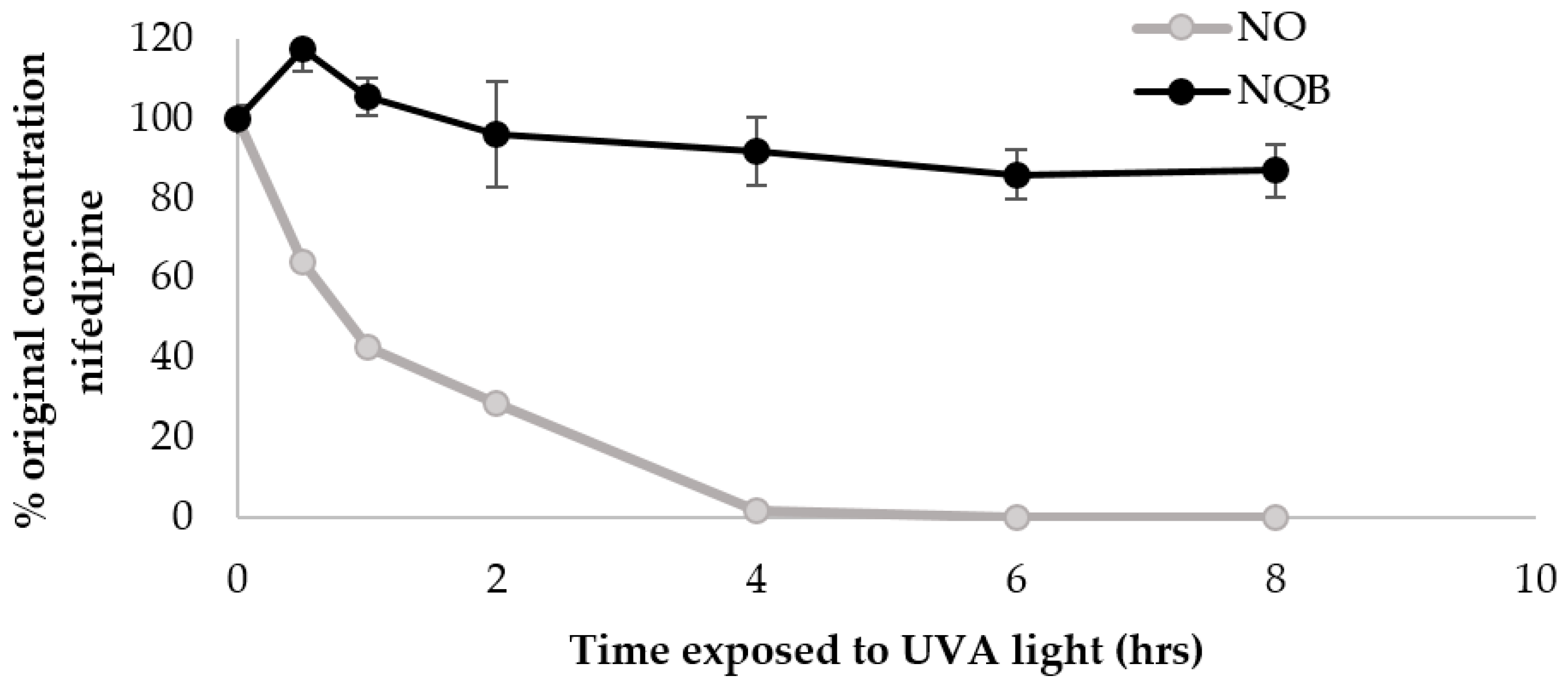
3.1. UVA and Visible Decomposition of Nifedipine
Nifedipine in Methanol
3.2. Characterization of Emulsion
3.3. Characterization of Topical Nifedipine Cream
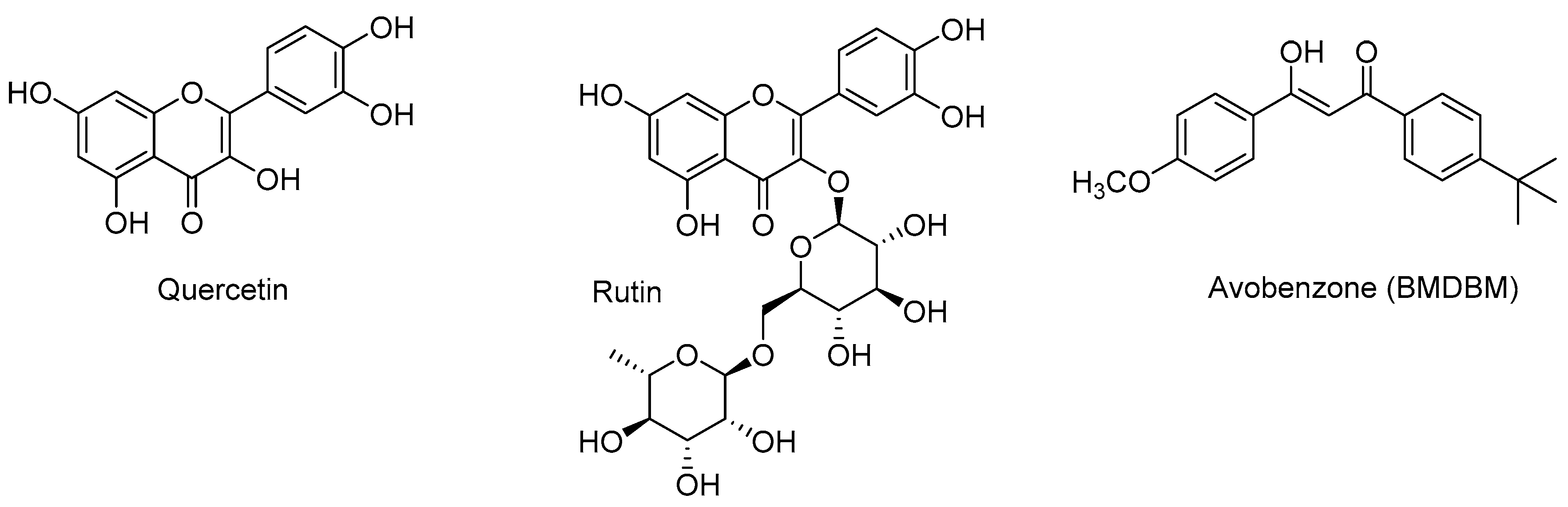
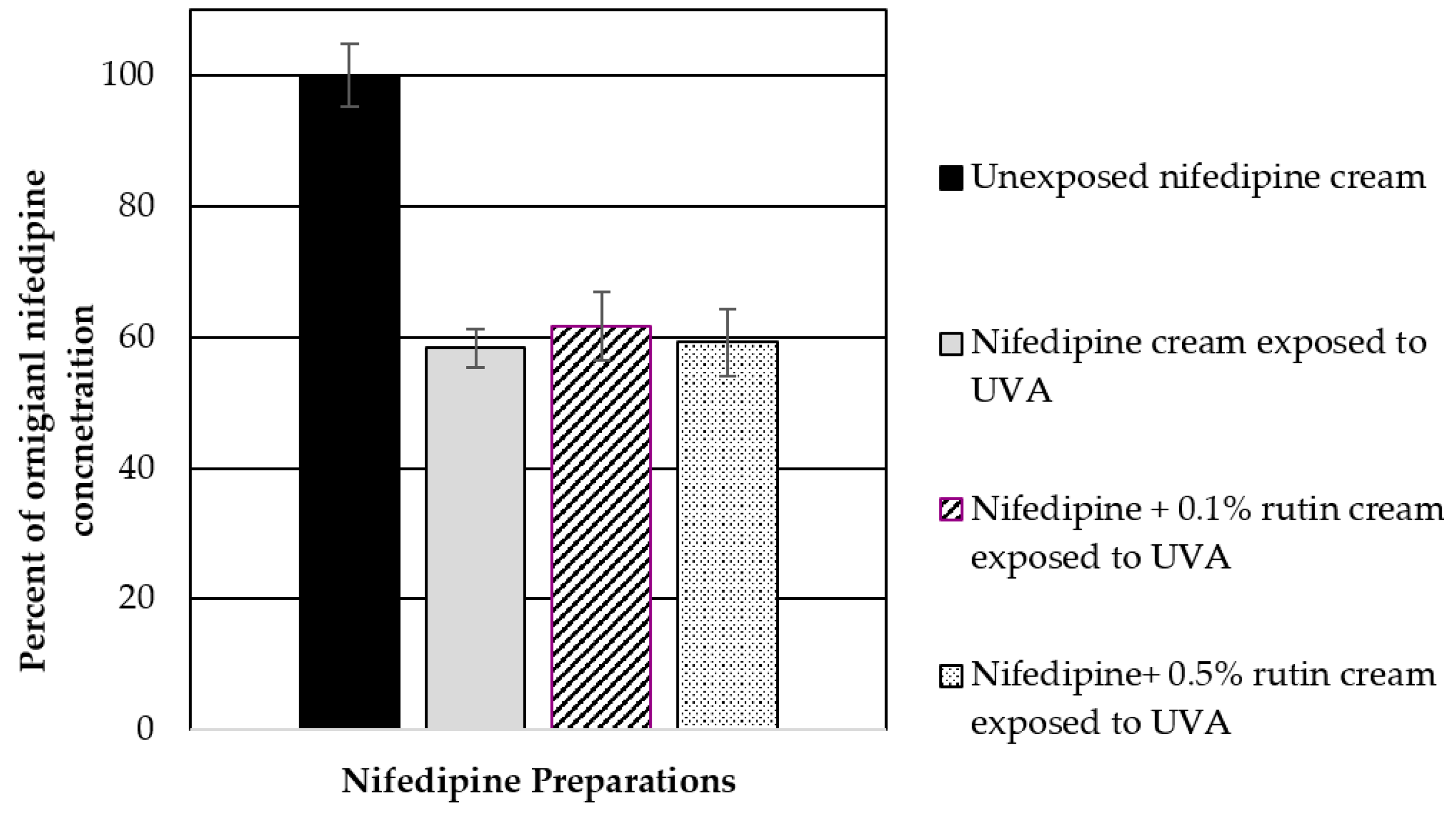
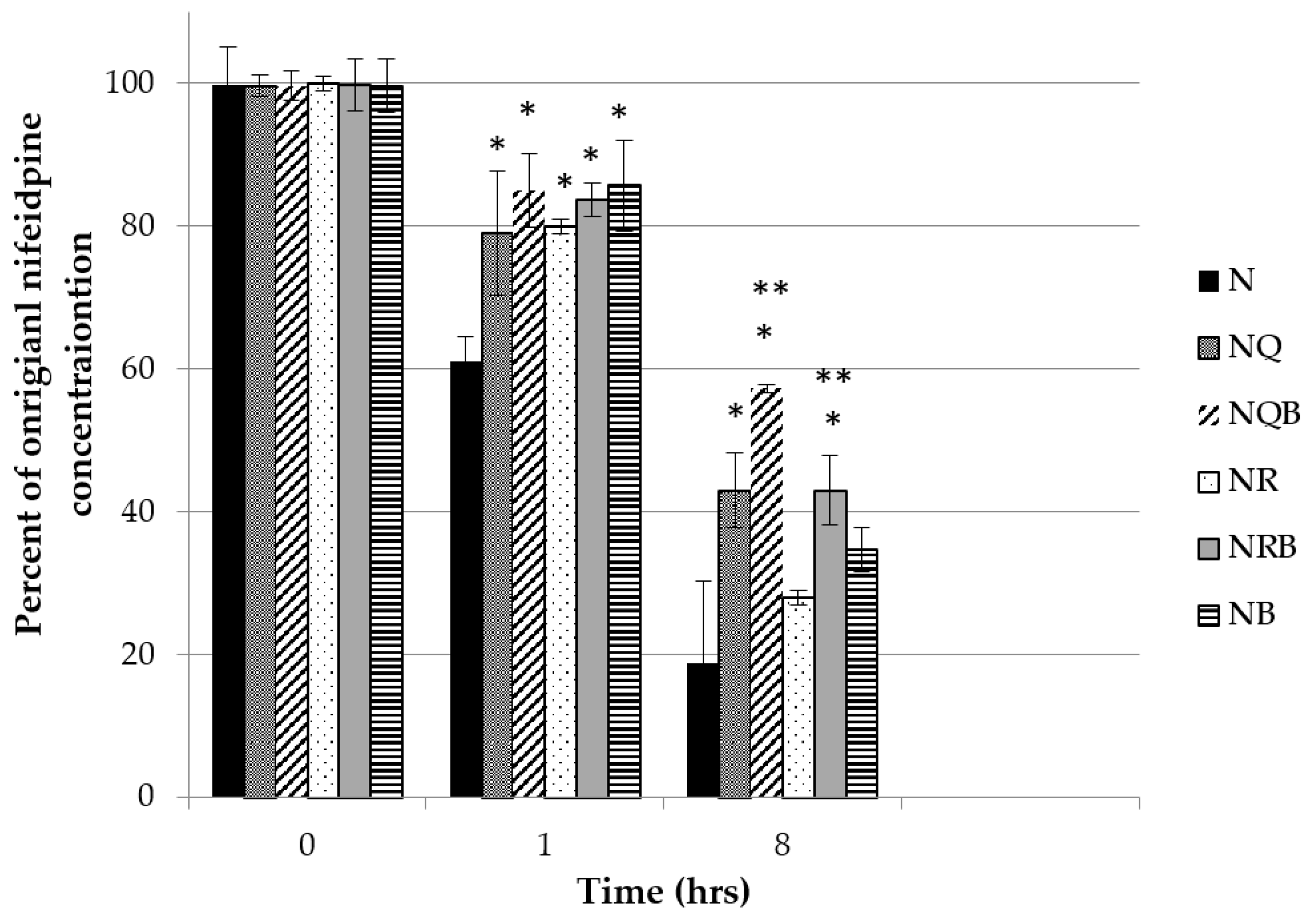
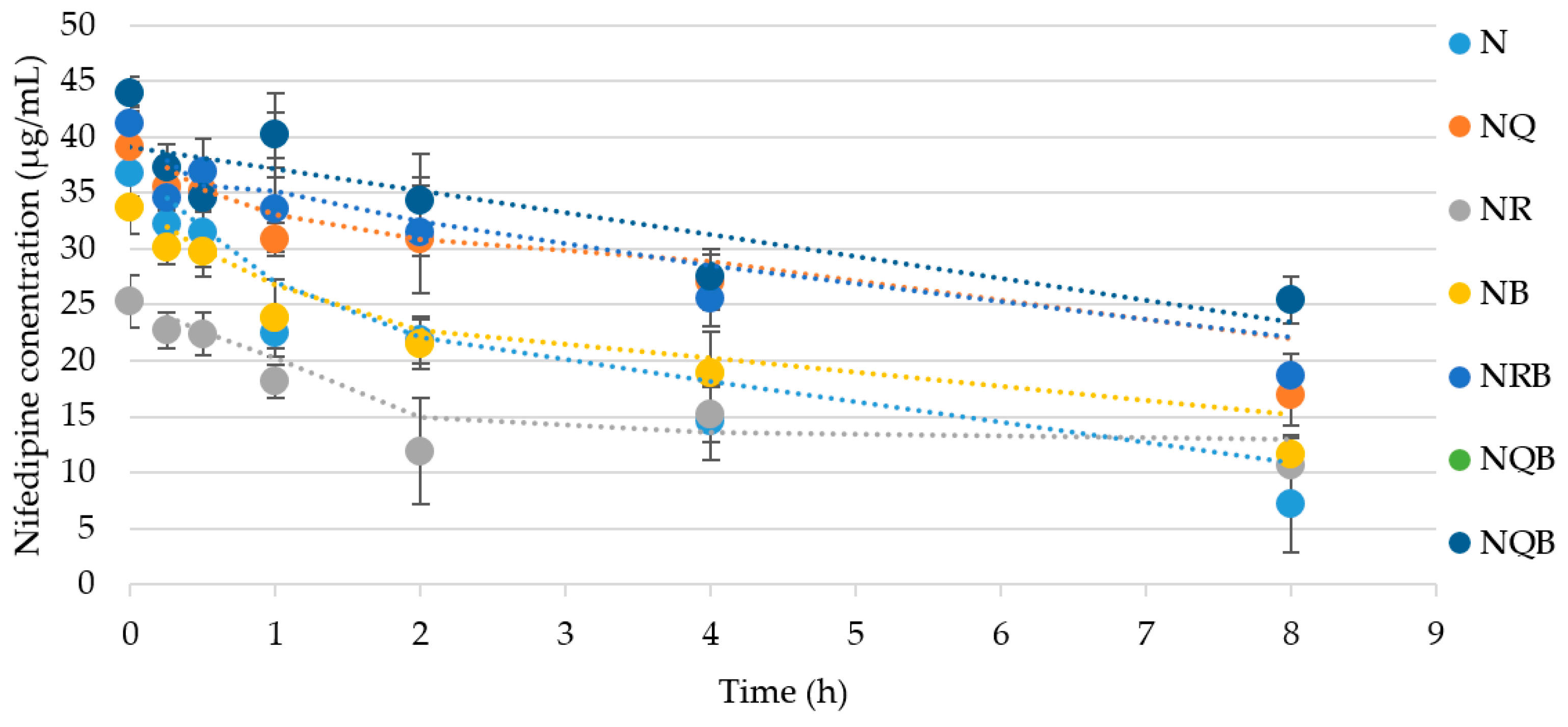
3.3.1. Influence of Butyl methoxydibenzoylmethane (BMDBM), Quercetin, and Rutin on Nifedipine UV Stability
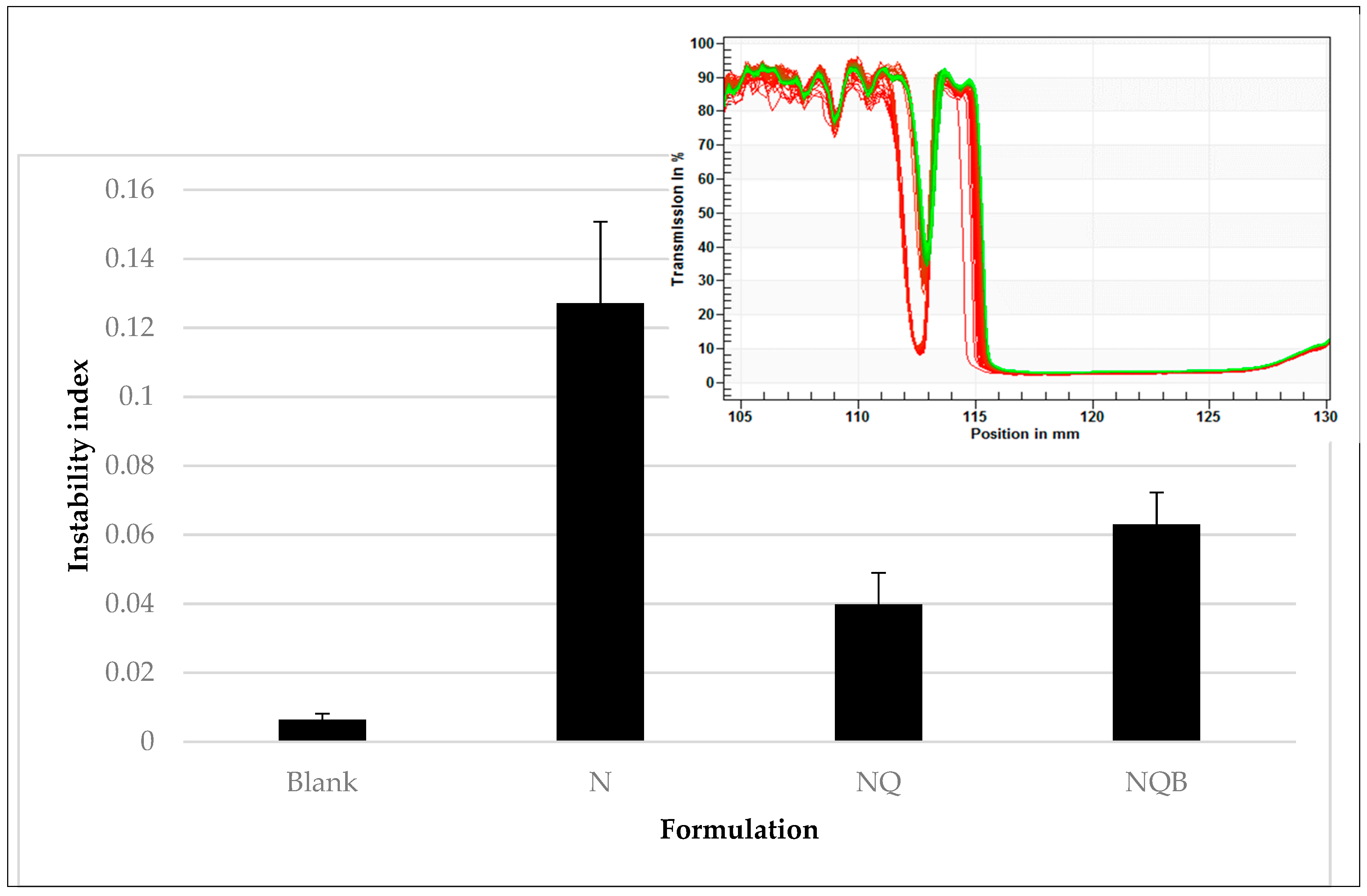
3.3.2. Effect of Photostabilizers on Emulsion Properties
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Garner, R.; Kumari, R.; Lanyon, P.; Doherty, M.; Zhang, W. Prevalence, risk factors and associations of primary Raynaud’s phenomenon: Systematic review and meta-analysis of observational studies. BMJ Open 2015, 5, e006389. [Google Scholar] [CrossRef] [PubMed]
- Wigley, F.M.; Flavahan, N.A. Raynaud’s Phenomenon. N. Engl. J. Med. 2016, 375, 556–565. [Google Scholar] [CrossRef] [PubMed]
- Bergersen, T.K.; Walloe, L. Acral coldness—Severely reduced blood flow to fingers and toes. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2018; Volume 157, pp. 677–685. [Google Scholar] [CrossRef]
- Joseph, L.; Kim, E.S.H. Non-Atherosclerotic Vascular Disease in Women. Curr. Treat. Options Cardiovasc. Med. 2017, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Plissonneau Duquene, P.; Pistorius, M.A.; Pottier, P.; Aymard, B.; Planchon, B. Cold climate could be an etiologic factor involved in Raynaud’s phenomenon physiopathology. Epidemiological investigation from 954 consultations in general practic. Int. Angiol. J. Int. Union Angiol. 2015, 34, 467–474. [Google Scholar]
- Rirash, F.; Tingey, P.C.; Harding, S.E.; Maxwell, L.J.; Tanjong Ghogomu, E.; Wells, G.A.; Tugwell, P.; Pope, J. Calcium channel blockers for primary and secondary Raynaud’s phenomenon. Cochrane Database Syst. Rev. 2017, 12, Cd000467. [Google Scholar] [CrossRef]
- Rustin, M.H.; Newton, J.A.; Smith, N.P.; Dowd, P.M. The treatment of chilblains with nifedipine: The results of a pilot study, a double-blind placebo-controlled randomized study and a long-term open trial. Br. J. Dermatol. 1989, 120, 267–275. [Google Scholar] [CrossRef]
- Belch, J.; Carlizza, A.; Carpentier, P.H.; Constans, J.; Khan, F.; Wautrecht, J.C.; Visona, A.; Heiss, C.; Brodeman, M.; Pecsvarady, Z.; et al. ESVM guidelines—The diagnosis and management of Raynaud’s phenomenon. Vasa 2017, 46, 413–423. [Google Scholar] [CrossRef]
- Schaller, D.; Gunduz, M.G.; Zhang, F.X.; Zamponi, G.W.; Wolber, G. Binding mechanism investigations guiding the synthesis of novel condensed 1,4-dihydropyridine derivatives with L-/T-type calcium channel blocking activity. Eur. J. Med. Chem. 2018, 155, 1–12. [Google Scholar] [CrossRef]
- Scholz, H. Pharmacological aspects of calcium channel blockers. Cardiovasc. Drugs Ther. 1997, 10 (Suppl. 3), 869–872. [Google Scholar] [CrossRef]
- Gjorup, T.; Kelbaek, H.; Hartling, O.J.; Nielsen, S.L. Controlled double-blind trial of the clinical effect of nifedipine in the treatment of idiopathic Raynaud’s phenomenon. Am. Heart J. 1986, 111, 742–745. [Google Scholar] [CrossRef]
- Golfam, F.; Golfam, P.; Khalaj, A.; Sayed Mortaz, S.S. The effect of topical nifedipine in treatment of chronic anal fissure. Acta Med. Iran. 2010, 48, 295–299. [Google Scholar] [PubMed]
- Agrawal, V.; Kaushal, G.; Gupta, R. Randomized controlled pilot trial of nifedipine as oral therapy vs. topical application in the treatment of fissure-in-ano. Am. J. Surg. 2013, 206, 748–751. [Google Scholar] [CrossRef] [PubMed]
- Ashkani-Esfahani, S.; Hosseinabadi, O.K.; Moezzi, P.; Moafpourian, Y.; Kardeh, S.; Rafiee, S.; Fatheazam, R.; Noorafshan, A.; Nadimi, E.; Mehrvarz, S.; et al. Verapamil, a Calcium-Channel Blocker, Improves the Wound Healing Process in Rats with Excisional Full-Thickness Skin Wounds Based on Stereological Parameters. Adv. Skin Wound Care 2016, 29, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.M.; Goa, K.L. Iloprost. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic potential in peripheral vascular disease, myocardial ischaemia and extracorporeal circulation procedures. Drugs 1992, 43, 889–924. [Google Scholar] [CrossRef] [PubMed]
- Hotkar, M.S.; Avachat, A.M.; Bhosale, S.S.; Oswal, Y.M. Preliminary investigation of topical nitroglycerin formulations containing natural wound healing agent in diabetes-induced foot ulcer. Int. Wound J. 2015, 12, 210–217. [Google Scholar] [CrossRef] [PubMed]
- O’Meara, S.; Cullum, N.; Majid, M.; Sheldon, T. Systematic Reviews of Wound Care Management: (3) Antimicrobial Agents for Chronic Wounds; (4) Diabetic Foot Ulceration. Health Technol. Assess. 2000, 4, 1–237. [Google Scholar] [CrossRef]
- McClusky, S.V.; Brunn, G.J. Nifedipine in Compounded Oral and Topical Preparations. Int. J. Pharm. Compd. 2013, 15, 166–169. [Google Scholar]
- Ioele, G.; Gunduz, M.G. A New Generation of Dihydropyridine Calcium Channel Blockers: Photostabilization of Liquid Formulations Using Nonionic Surfactants. Pharmaceutics 2019, 11, 28. [Google Scholar] [CrossRef]
- Hayase, N.; Itagaki, Y.; Ogawa, S.; Akutsu, S.; Inagaki, S.; Abiko, Y. Newly discovered photodegradation products of nifedipine in hospital prescriptions. J. Pharm. Sci. 1994, 83, 532–538. [Google Scholar] [CrossRef]
- Aman, W.; Thoma, K. Particular features of photolabile substances in tablets. Die Pharm. 2003, 58, 645–650. [Google Scholar]
- Görner, H. Nitro group photoreduction of 4-(2-nitrophenyl)- and 4-(3-nitrophenyl)-1,4-dihydropyridines. Chem. Phys. 2010, 373, 153–158. [Google Scholar] [CrossRef]
- Grooff, D.; Francis, F.; De Villiers, M.M.; Ferg, E. Photostability of crystalline versus amorphous nifedipine and nimodipine. J. Pharm. Sci. 2013, 102, 1883–1894. [Google Scholar] [CrossRef] [PubMed]
- Maafi, W.; Maafi, M. Modelling nifedipine photodegradation, photostability and actinometric properties. Int. J. Pharm. 2013, 456, 153–164. [Google Scholar] [CrossRef] [PubMed]
- De Luca, M.; Ioele, G.; Spatari, C.; Ragno, G. Photostabilization studies of antihypertensive 1, 4-dihydropyridines using polymeric containers. Int. J. Pharm. 2016, 505, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Majeed, I.A.; Murray, W.J.; Newton, D.W.; Othman, S.; Al-turk, W.A. Spectrophotometric study of the photodecomposition kinetics of nifedipine. J. Pharm. Pharmacol. 1987, 39, 1044–1046. [Google Scholar] [CrossRef] [PubMed]
- Baertschi, S.W.; Clapham, D.; Foti, C.; Kleinman, M.H.; Kristensen, S.; Reed, R.A.; Templeton, A.C.; Tønnesen, H.H. Implications of In-Use Photostability: Proposed Guidance for Photostability Testing and Labeling to Support the Administration of Photosensitive Pharmaceutical Products, Part 2: Topical Drug Product. J. Pharm. Sci. 2015, 104, 2688–2701. [Google Scholar] [CrossRef] [PubMed]
- Tonnesen, H.H. Photostability of Drugs and Drug Formulations; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar]
- Cosa, G. Photodegradation and photosensitization in pharmaceutical products: Assessing drug phototoxicity. Pure Appl. Chem. 2004, 76, 263. [Google Scholar] [CrossRef]
- Kockler, J.; Robertson, S.; Oelgemoller, M.; Davies, M.; Bowden, B.; Brittain, H.G.; Glass, B.D. Butyl methoxy dibenzoylmethane. In Profiles of Drug Substances, Excipients and Related Methodology; Harry, G.B., Ed.; Academic Press: New York, NY, USA, 2013; Volume 38, pp. 87–111. [Google Scholar] [CrossRef]
- Gange, R.W.; Soparkar, A.; Matzinger, E.; Dromgoole, S.H.; Sefton, J.; DeGryse, R. Efficacy of a sunscreen containing butyl methoxydibenzoylmethane against ultraviolet. A radiation in photosensitized subjects. J. Am. Acad. Dermatol 1986, 15, 494–499. [Google Scholar] [CrossRef]
- Lhiaubet-Vallet, V.; Marin, M.; Jimenez, O.; Gorchs, O.; Trullas, C.; Miranda, M.A. Filter-filter interactions. Photostabilization, triplet quenching and reactivity with singlet oxygen. Photochem. Photobiol. Sci. 2010, 9, 552–558. [Google Scholar] [CrossRef]
- Solovchenko, A.; Schmitz-Eiberger, M. Significance of skin flavonoids for UV-B-protection in apple fruits. J. Exp. Bot. 2003, 54, 1977–1984. [Google Scholar] [CrossRef]
- Wilson, K.E.; Wilson, M.I.; Greenberg, B.M. Identification of the Flavonoid Glycosides that Accumulate in Brassica napus L. cv. Topas Specifically in Response to Ultraviolet B Radiation. Photochem. Photobiol. 1998, 67, 547–553. [Google Scholar] [CrossRef]
- Fahlman, B.M.; Krol, E.S. Inhibition of UVA and UVB Radiation-Induced Lipid Oxidation by Quercetin. J. Agric. Food Chem. 2009, 57, 5301–5305. [Google Scholar] [CrossRef] [PubMed]
- Maini, S.; Fahlman, B.M.; Krol, E.S. Flavonols Protect Against UV Radiation-Induced Thymine Dimer Formation in an Artificial Skin Mimic. J. Pharm. Pharm. Sci. 2015, 18, 600–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, C.A.; Peres, D.D.; Graziola, F.; Chacra, N.A.; Araújo, G.L.; Flórido, A.C.; Mota, J.; Rosado, C.; Velasco, M.V.; Rodrigues, L.M.; et al. Cutaneous biocompatible rutin-loaded gelatin-based nanoparticles increase the SPF of the association of UVA and UVB filters. Eur. J. Pharm. Sci. 2016, 81, 1–9. [Google Scholar] [CrossRef]
- Chaiprasongsuk, A.; Onkoksoong, T.; Pluemsamran, T.; Limsaengurai, S.; Panich, U. Photoprotection by dietary phenolics against melanogenesis induced by UVA through Nrf2-dependent antioxidant responses. Redox Biol. 2016, 8, 79–90. [Google Scholar] [CrossRef]
- Choquenet, B.; Couteau, C.; Paparis, E.; Coiffard, L.J. Quercetin and rutin as potential sunscreen agents: Determination of efficacy by an in vitro method. J. Nat. Prod. 2008, 71, 1117–1118. [Google Scholar] [CrossRef]
- Scalia, S.; Mezzena, M. Photostabilization Effect of Quercetin on the UV Filter Combination, Butyl Methoxydibenzoylmethane–Octyl Methoxycinnamate. Photochem. Photobiol. 2010, 86, 273–278. [Google Scholar] [CrossRef]
- Barak, N.; Rice, H.; Kamsler, A. Variability of compounded topical 0.2% nifedipine formulations. J. Pharm. Pract. Res. 2019, 49, 130–134. [Google Scholar] [CrossRef]
- Huong, S.P.; Rocher, E.; Fourneron, J.-D.; Charles, L.; Monnier, V.; Bun, H.; Andrieu, V. Photoreactivity of the sunscreen butylmethoxydibenzoylmethane (DBM) under various experimental conditions. J. Photochem. Photobiol. A Chem. 2008, 196, 106–112. [Google Scholar] [CrossRef]
- Vallejo, J.J.; Mesa, M.; Gallardo, C. Evaluation of the Avobenzone Photostability in Solvents Used in Cosmetic Formulations. Vitae 2011, 18, 63–71. [Google Scholar]
- Afonso, S.; Horita, K.; Sousa e Silva, J.P.; Almeida, I.F.; Amaral, M.H.; Lobao, P.A.; Costa, P.C.; Miranda, M.S.; Esteves da Silva, J.C.; Sousa Lobo, J.M. Photodegradation of avobenzone: Stabilization effect of antioxidants. J. Photochem. Photobiol. B Biol. 2014, 140, 36–40. [Google Scholar] [CrossRef]
- Gaspar, L.R.; Campos, P.M. Photostability and efficacy studies of topical formulations containing UV-filters combination and vitamins A, C and E. Int. J. Pharm. 2007, 343, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Shrewsbury, R.P. Applied Pharmaceutics in Contemporary Compounding; Morton Publishing Company: Englewood, CO, USA, 2015. [Google Scholar]
- U.S. Food and Drug Administration. Part 352 Sunscreen drug products for over-the-counter human use. In CFR—Code of Federal Regulations Title 21; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2018; Volume 5. [Google Scholar]
- European Medicines Agency. ICH Topic Q1B Stability testing: Photostability testing of new drug substances and products. In ICH Harmonised Tripartite Guideline; European Medicines Agency: London, UK, 1996. [Google Scholar]
- Fasani, E.; Dondi, D.; Ricci, A.; Albini, A. Photochemistry of 4-(2-Nitrophenyl)-1,4-Dihydropyridines. Evidence for Electron Transfer and Formation of an Intermediate. Photochem. Photobiol. 2006, 82, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Baranda, A.B.; Alonso, R.M.; Jiménez, R.M.; Weinmann, W. Instability of calcium channel antagonists during sample preparation for LC–MS–MS analysis of serum samples. Forensic Sci. Int. 2006, 156, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, D.W., Jr.; Gad, S.C.; Julien, M. A review of the nonclinical safety of Transcutol(R), a highly purified form of diethylene glycol monoethyl ether (DEGEE) used as a pharmaceutical excipient. Food Chem. Toxicol. 2014, 72, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Osborne, D.W. Diethylene glycol monoethyl ether: An emerging solvent in topical dermatology products. J. Cosmet. Dermatol. 2011, 10, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Streel, B.; Zimmer, C.; Sibenaler, R.; Ceccato, A. Simultaneous determination of nifedipine and dehydronifedipine in human plasma by liquid chromatography–tandem mass spectrometry. J. Chrom. B Biomed. Sci. App. 1998, 720, 119–128. [Google Scholar] [CrossRef]
- Fahlman, B.M.; Krol, E.S. UVA and UVB radiation-induced oxidation products of quercetin. J. Photochem. Photobiol. B Biol. 2009, 97, 123–131. [Google Scholar] [CrossRef]
- Nakajima, A.; Tahara, M.; Yoshimura, Y.; Nakazawa, H. Study of Compounds Suppressing Free Radical Generation from UV-Exposed Ketoprofen. Chem. Pharm. Bull. 2007, 55, 1431–1438. [Google Scholar] [CrossRef] [Green Version]
- Smith, G.J.; Thomsen, S.J.; Markham, K.R.; Andary, C.; Cardon, D. The photostabilities of naturally occurring 5-hydroxyflavones, flavonols, their glycosides and their aluminium complexes. J. Photochem. Photobiol. A Chem. 2000, 136, 87–91. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FORMU-LATIONS | Phase 1 0–2 h k1 (%/h) | Phase 2 2–8 h k2 (%/h) |
|---|---|---|
| N | 14.3 ± 0.8 | 2.18 ± 0.7 |
| NQ | 8.21 ± 2.6* # | 2.32 ± 0.49 |
| NR | 8.59 ± 2.87 | 3.5 ± 0.52 |
| NB | 7.86 ± 5.1 | 4.6 ± 0.46 * |
| NRB | 5.26 ± 1.6 * | 2.1 ± 0.26 |
| NQB | 3.7 ± 2.14 * # | 1.4 ± 0.72* |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wasan, E.K.; Zhao, J.; Poteet, J.; Mohammed, M.A.; Syeda, J.; Orlowski, T.; Soulsbury, K.; Cawthray, J.; Bunyamin, A.; Zhang, C.; et al. Development of a UV-Stabilized Topical Formulation of Nifedipine for the Treatment of Raynaud Phenomenon and Chilblains. Pharmaceutics 2019, 11, 594. https://doi.org/10.3390/pharmaceutics11110594
Wasan EK, Zhao J, Poteet J, Mohammed MA, Syeda J, Orlowski T, Soulsbury K, Cawthray J, Bunyamin A, Zhang C, et al. Development of a UV-Stabilized Topical Formulation of Nifedipine for the Treatment of Raynaud Phenomenon and Chilblains. Pharmaceutics. 2019; 11(11):594. https://doi.org/10.3390/pharmaceutics11110594
Chicago/Turabian StyleWasan, Ellen K., Jinying Zhao, Joshua Poteet, Munawar A. Mohammed, Jaweria Syeda, Tatiana Orlowski, Kevin Soulsbury, Jacqueline Cawthray, Amanda Bunyamin, Chi Zhang, and et al. 2019. "Development of a UV-Stabilized Topical Formulation of Nifedipine for the Treatment of Raynaud Phenomenon and Chilblains" Pharmaceutics 11, no. 11: 594. https://doi.org/10.3390/pharmaceutics11110594