
Genomic Surveillance of SARS-CoV-2 in Healthcare Workers: A Critical Sentinel Group for Monitoring the SARS-CoV-2 Variant Shift

 , , , , , , , , , add
Show full author list
, , , , , , , , , add
Show full author list
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Studied Regions and Sampling
2.2. SARS-CoV-2 Genome Sequencing
2.3. Genome Sampling
2.4. SARS-CoV-2 Variant Analysis
2.5. Maximum Likelihood (ML) Phylogenetic Analysis of HCW
3. Results
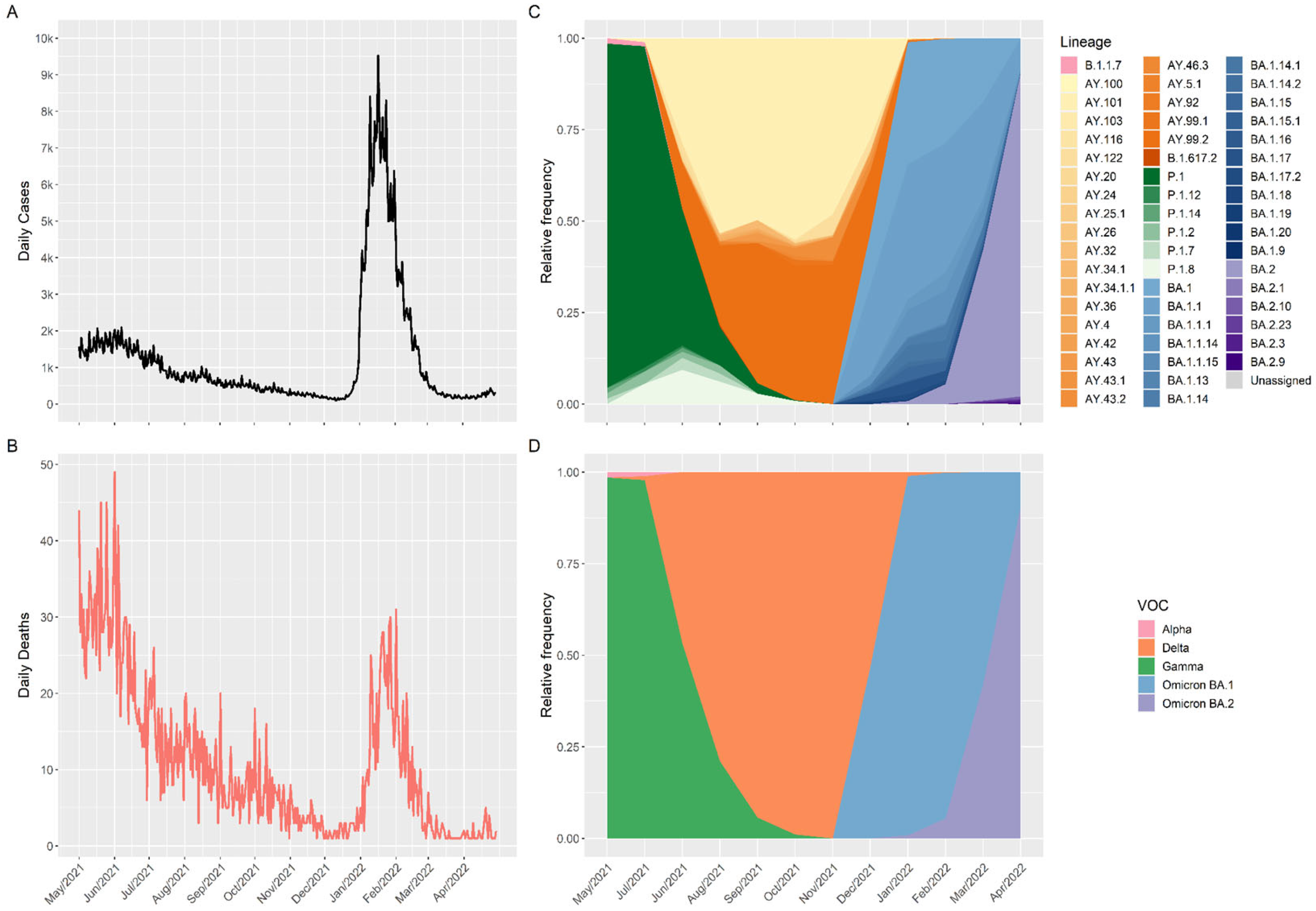
3.1. Profile of SARS-CoV-2 Variants in Santa Catarina (Brazil) during the Second Year of the COVID-19 Pandemic Period (May 2021 to April 2022)
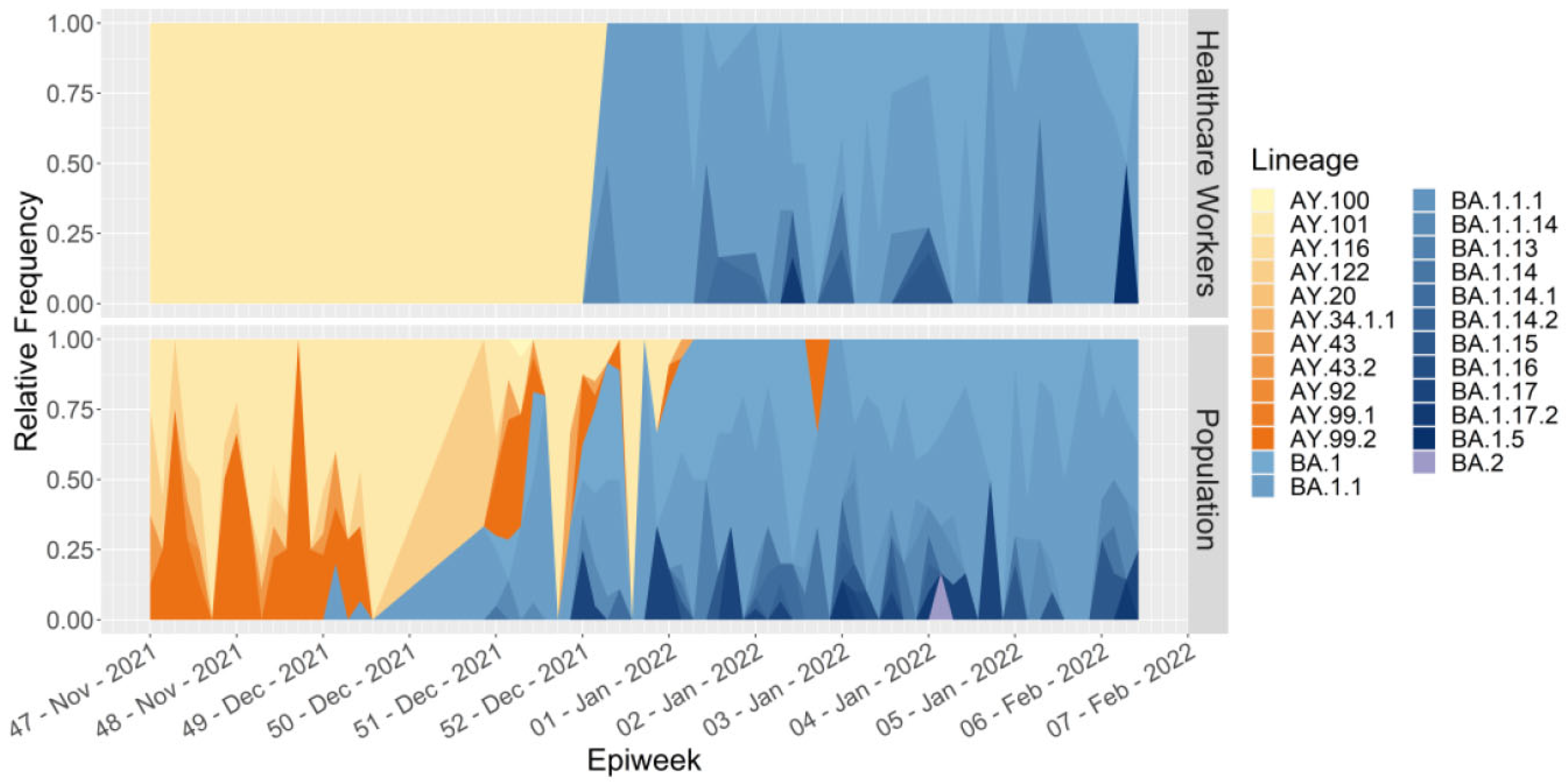
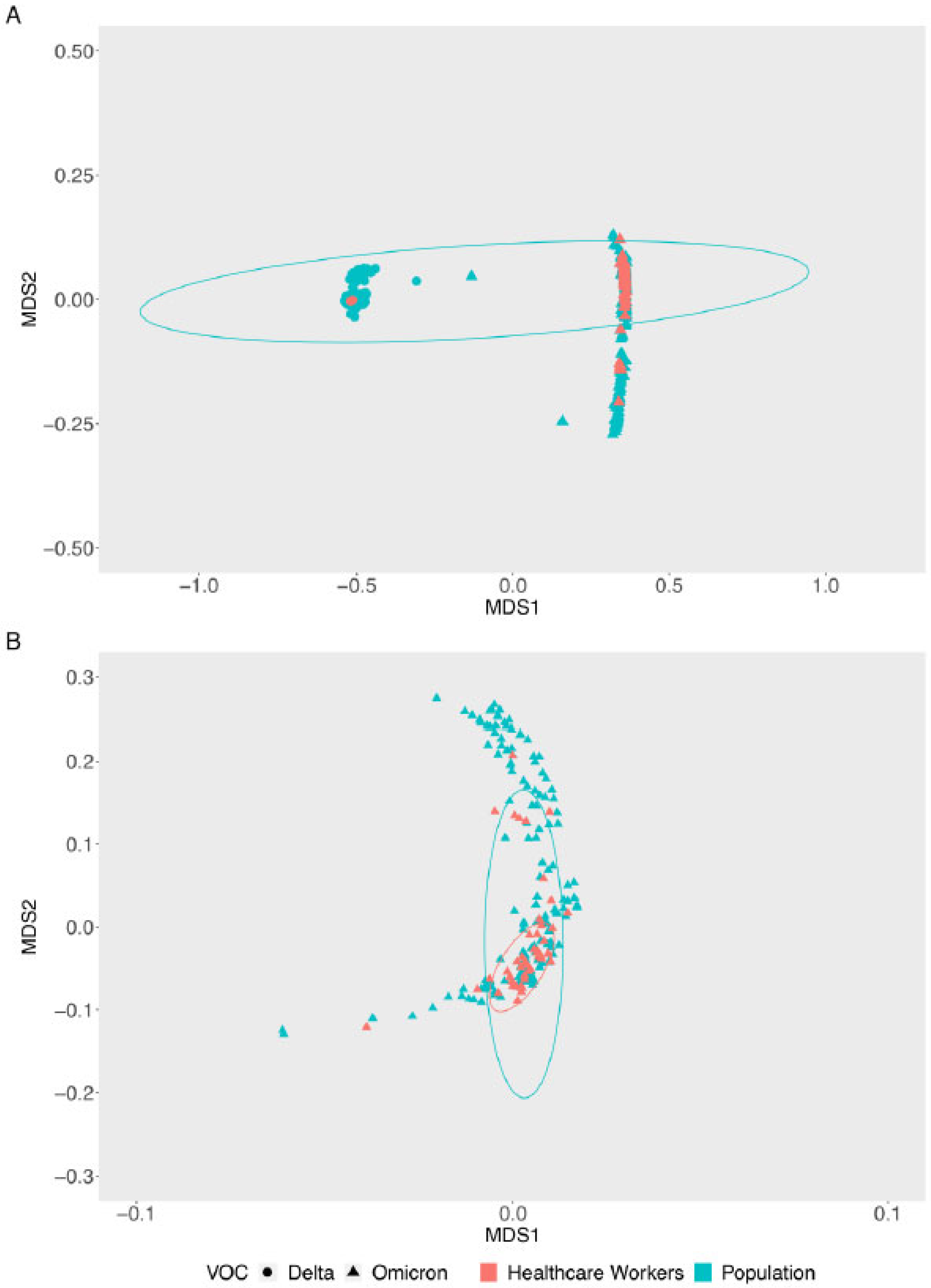
3.2. Variant Shift (Delta to Omicron) in HCW and General Population in Santa Catarina (Brazil)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO—World Health Organization. WHO Coronavirus (COVID-19). 2023. Available online: https://www.who.int (accessed on 27 January 2023).
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara SL, R.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Health-Care Workers: A Living Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Cannizzaro, E.; Verso, M.G.; Tramuto, F.; Maida, C.M.; Lacca, G.; Alba, D.; Cimino, L.; Conforto, A.; Cirrincione, L.; et al. SARS-CoV-2 Infection in Healthcare Workers and General Population During “First Wave” of COVID-19 Pandemic: A Cross-Sectional Study Conducted in Sicily, Italy. Front. Public Health 2021, 9, 644008. [Google Scholar] [CrossRef] [PubMed]
- De Maria, L.; Sponselli, S.; Caputi, A.; Pipoli, A.; Giannelli, G.; Delvecchio, G.; Zagaria, S.; Cavone, D.; Stefanizzi, P.; Bianchi, F.P.; et al. Comparison of Three Different Waves in Healthcare Workers during the COVID-19 Pandemic: A Retrospective Observational Study in an Italian University Hospital. J. Clin. Med. 2022, 11, 3074. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.F.; Giavina-Bianchi, P.; Buss, L.; Mesquita Peres, C.H.; Rafael, M.M.; Dos Santos LG, N.; Bedin, A.A.; Francisco MC, P.B.; Satakie, F.M.; Jesus Menezes, M.A.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Seroprevalence and Risk Factors among Oligo/Asymptomatic Healthcare Workers: Estimating the Impact of Community Transmission. Clin. Infect. Dis. 2021, 73, E1214–E1218. [Google Scholar] [CrossRef] [PubMed]
- Korth, J.; Wilde, B.; Dolff, S.; Anastasiou, O.E.; Krawczyk, A.; Jahn, M.; Cordes, S.; Ross, B.; Esser, S.; Lindemann, M.; et al. SARS-CoV-2-specific antibody detection in healthcare workers in Germany with direct contact to COVID-19 patients. J. Clin. Virol. 2020, 128, 104437. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Cheng, S.-Z.; Xu, K.-W.; Yang, Y.; Zhu, Q.-T.; Zhang, H.; Yang, D.-Y.; Cheng, S.; Xiao, H.; Wang, J.-W.; et al. Use of personal protective equipment against coronavirus disease 2019 by healthcare workers in Wuhan, China: Cross sectional study. BMJ 2020, 369, 6–11. [Google Scholar] [CrossRef]
- Khanna, R.; Htun, H.L.; Li, A.L.; Kyaw, W.M.; Ang, H.; Ang, B.; Chow, A. Staff and patient surveillance in hospitals: Good sentinels for the emergence of new SARS-CoV-2 variants. J. Infect. 2022, 85, 436–480. [Google Scholar] [CrossRef]
- WHO—World Health Organization. Integrated Sentinel Surveillance of Influenza and SARS-CoV-2 and the Development of the Global Influenza Surveillance and Response System Plus: Virtual Meeting, 12–14 October 2021; WHO: Geneva, Switzerland, 2022; Available online: https://apps.who.int/iris/handle/10665/356310 (accessed on 15 December 2022).
- Bromberg, M.; Keinan-Boker, L.; Gur-Arie, L.; Sefty, H.; Mandelboim, M.; Dichtiar, R.; Kaufman, Z.; Glatman-Freedman, A. Monitoring SARS-CoV-2 Activity with Sentinel Surveillance: Lessons Learned from the First Wave in Israel. Isr. Med. Assoc. J. 2022, 24, 215–218. [Google Scholar] [PubMed]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Omicron sub-lineage BA.2 may have “substantial growth advantage”, UKHSA reports. BMJ 2022, 376, o263. [Google Scholar] [CrossRef] [PubMed]
- GISAID. Global Initiative on Sharing Avian Influenza Data. 2022. Available online: https://www.gisaid.org (accessed on 15 December 2022).
- Garcia-Beltran, W.F.; St Denis, K.J.; Hoelzemer, A.; Lam, E.C.; Nitido, A.D.; Sheehan, M.L.; Berrios, C.; Ofoman, O.; Chang, C.C.; Hauser, B.M.; et al. mRNA-based COVID-19 vaccine boosters induce neutralizing immunity against SARS-CoV-2 Omicron variant. Cell 2022, 185, 457–466.e4. [Google Scholar] [CrossRef] [PubMed]
- Padilha, D.A.; Benetti Filho, V.; Moreira, R.S.; Soratto, T.A.T.; Maia, G.A.; Christoff, A.P.; Barazzetti, F.H.; Schörner, M.A.; Ferrari, F.L.; Martins, C.L.; et al. Emergence of Two Distinct SARS-CoV-2 Gamma Variants and the Rapid Spread of P.1-like-II SARS-CoV-2 during the Second Wave of COVID-19 in Santa Catarina, Southern Brazil. Viruses 2022, 14, 695. [Google Scholar] [CrossRef] [PubMed]
- Bhoyar, R.C.; Jain, A.; Sehgal, P.; Divakar, M.K.; Sharma, D.; Imran, M.; Jolly, B.; Ranjan, G.; Rophina, M.; Sharma, S.; et al. High throughput detection and genetic epidemiology of SARS-CoV-2 using COVIDSeq next-generation sequencing. PLoS ONE 2021, 16, e0247115. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Available online: https://ggplot2.tidyverse.org (accessed on 15 December 2022).
- Katoh, K.; Standley, D.M. MAFFT multiple sequence alignment software version 7: Improvements in performance and usability. Mol. Biol. Evol. 2013, 30, 772–780. [Google Scholar] [CrossRef]
- Minh, B.Q.; Schmidt, H.A.; Chernomor, O.; Schrempf, D.; Woodhams, M.D.; von Haeseler, A.; Lanfear, R. IQ-TREE 2: New Models and Efficient Methods for Phylogenetic Inference in the Genomic Era. Mol. Biol. Evol. 2020, 37, 1530–1534. [Google Scholar] [CrossRef] [PubMed]
- Kalyaanamoorthy, S.; Minh, B.Q.; Wong TK, F.; von Haeseler, A.; Jermiin, L.S. Model Finder: Fast model selection for accurate phylogenetic estimates. Nat. Methods 2017, 14, 587–589. [Google Scholar] [CrossRef] [PubMed]
- Hoang, D.T.; Chernomor, O.; von Haeseler, A.; Minh, B.Q.; Vinh, L.S. UFBoot2: Improving the ultrafast bootstrap approximation. Mol. Biol. Evol. 2018, 35, 518–522. [Google Scholar] [CrossRef]
- Letunic, I.; Bork, P. Interactive Tree of Life (iTOL) v5: An online tool for phylogenetic tree display and annotation. Nucleic Acids Res. 2021, 49, W293–W296. [Google Scholar] [CrossRef]
- United Nations Department of Economic and Social Affairs. World Population Prospects; UN: New York, NY, USA, 2016. [Google Scholar] [CrossRef]
- Scheler, C.A.; Discacciati, M.G.; Vale, D.B.; Lajos, G.J.; Surita, F.G.; Teixeira, J.C. Maternal Deaths from COVID-19 in Brazil: Increase during the Second Wave of the Pandemic. Rev. Bras. Ginecol. Obs. RBGO Gynecol. Obstetr. 2022, 44, 567–572. [Google Scholar] [CrossRef]
- Orellana, J.D.Y.; Marrero, L.; Horta, B.L. COVID-19 mortality in Brazil in different age groups: Differentials between extreme rates in 2021 and 2022. Rep. Public Health 2022, 38, e00041922. [Google Scholar] [CrossRef] [PubMed]
- de Souza, F.S.H.; Hojo-Souza, N.S.; da Silva, C.M.; Guidoni, D.L. Second wave of COVID-19 in Brazil: Younger at higher risk. Eur. J. Epidemiol. 2021, 36, 441–443. [Google Scholar] [CrossRef]
- Araf, Y.; Akter, F.; Tang, Y.D.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron variant of SARS-CoV-2: Genomics, transmissibility, and responses to current COVID-19 vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Noureddine, F.Y.; Chakkour, M.; El Roz, A.; Reda, J.; Al Sahily, R.; Assi, A.; Joma, M.; Salami, H.; Hashem, S.J.; Harb, B.; et al. The Emergence of SARS-CoV-2 Variant(s) and Its Impact on the Prevalence of COVID-19 Cases in the Nabatieh Region, Lebanon. Med. Sci 2021, 9, 40. [Google Scholar] [CrossRef] [PubMed]
- Chakkour, M.; Salami, A.; Olleik, D.; Kamal, I.; Noureddine, F.Y.; Roz, A.E.; Ghssein, G. Risk Markers of COVID-19, a Study from South-Lebanon. COVID 2022, 2, 867–876. [Google Scholar] [CrossRef]
- Ribeiro Xavier, C.; Sachetto Oliveira, R.; da Fonseca Vieira, V.; Lobosco, M.; Weber Dos Santos, R. Characterisation of Omicron Variant during COVID-19 Pandemic and the Impact of Vaccination, Transmission Rate, Mortality, and Reinfection in South Africa, Germany, and Brazil. BioTech 2022, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Adamoski, D.; Baura, V.A.; Rodrigues, A.C.; Royer, C.A.; Aoki, M.N.; Tschá, M.K.; Bonatto, A.C.; Wassem, R.; Nogueira, M.B.; Raboni, S.M.; et al. SARS-CoV-2 Delta and Omicron Variants Surge in Curitiba, Southern Brazil, and Its Impact on Overall COVID-19 Lethality. Viruses 2022, 14, 809. [Google Scholar] [CrossRef]
- Lamarca, A.P.; Souza, U.J.B.d.; Moreira, F.R.R.; Almeida, L.G.P.d.; Menezes, M.T.d.; Souza, A.B.d.; Ferreira, A.C.d.S.; Gerber, A.L.; Lima, A.B.d.; Guimarães, A.P.d.C.; et al. The Omicron Lineages BA.1 and BA.2 (Betacoronavirus SARS-CoV-2) Have Repeatedly Entered Brazil through a Single Dispersal Hub. Viruses 2023, 15, 888. [Google Scholar] [CrossRef]
- Guijarro, C.; Galán, I.; Martínez-Ponce, D.; Pérez-Fernández, E.; Goyanes, M.J.; Castilla, V.; Velasco, M. SARS-CoV-2 new infections among healthcare workers after the first dose of the BNT162b2 mRNA COVID-19 vaccine. A hospital-wide cohort study. Clin. Microbiol. Infect. 2021, 27, e1–e1699. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padilha, D.A.; Souza, D.S.M.; Kawagoe, E.K.; Filho, V.B.; Amorim, A.N.; Barazzetti, F.H.; Schörner, M.A.; Fernandes, S.B.; Coelho, B.K.; Rovaris, D.B.; et al. Genomic Surveillance of SARS-CoV-2 in Healthcare Workers: A Critical Sentinel Group for Monitoring the SARS-CoV-2 Variant Shift. Viruses 2023, 15, 984. https://doi.org/10.3390/v15040984
Padilha DA, Souza DSM, Kawagoe EK, Filho VB, Amorim AN, Barazzetti FH, Schörner MA, Fernandes SB, Coelho BK, Rovaris DB, et al. Genomic Surveillance of SARS-CoV-2 in Healthcare Workers: A Critical Sentinel Group for Monitoring the SARS-CoV-2 Variant Shift. Viruses. 2023; 15(4):984. https://doi.org/10.3390/v15040984
Chicago/Turabian StylePadilha, Dayane Azevedo, Doris Sobral Marques Souza, Eric Kazuo Kawagoe, Vilmar Benetti Filho, Ariane Nicaretta Amorim, Fernando Hartmann Barazzetti, Marcos André Schörner, Sandra Bianchini Fernandes, Bruna Kellet Coelho, Darcita Buerger Rovaris, and et al. 2023. "Genomic Surveillance of SARS-CoV-2 in Healthcare Workers: A Critical Sentinel Group for Monitoring the SARS-CoV-2 Variant Shift" Viruses 15, no. 4: 984. https://doi.org/10.3390/v15040984