
Leave No-One Behind: A Retrospective Study of Hepatitis C Testing and Linkage to Care for Hospital Inpatients
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting and Population
2.2. Study Design
- Had a separation with hepatitis C coding;
- Had hepatitis C virus (HCV) antibody testing (among those with hepatitis C coding) linked to admission, see below;
- Had HCV RNA testing (among those who were HCV antibody positive);
- Had evidence of treatment (among those who were HCV RNA positive and among those who had hepatitis C coding).
- The estimated number of people living with hepatitis C in the hospital catchment area.
- An estimate of the number of missed opportunities in primary outcomes 2–4.
2.3. Data Analysis
3. Results
3.1. Patient Summary
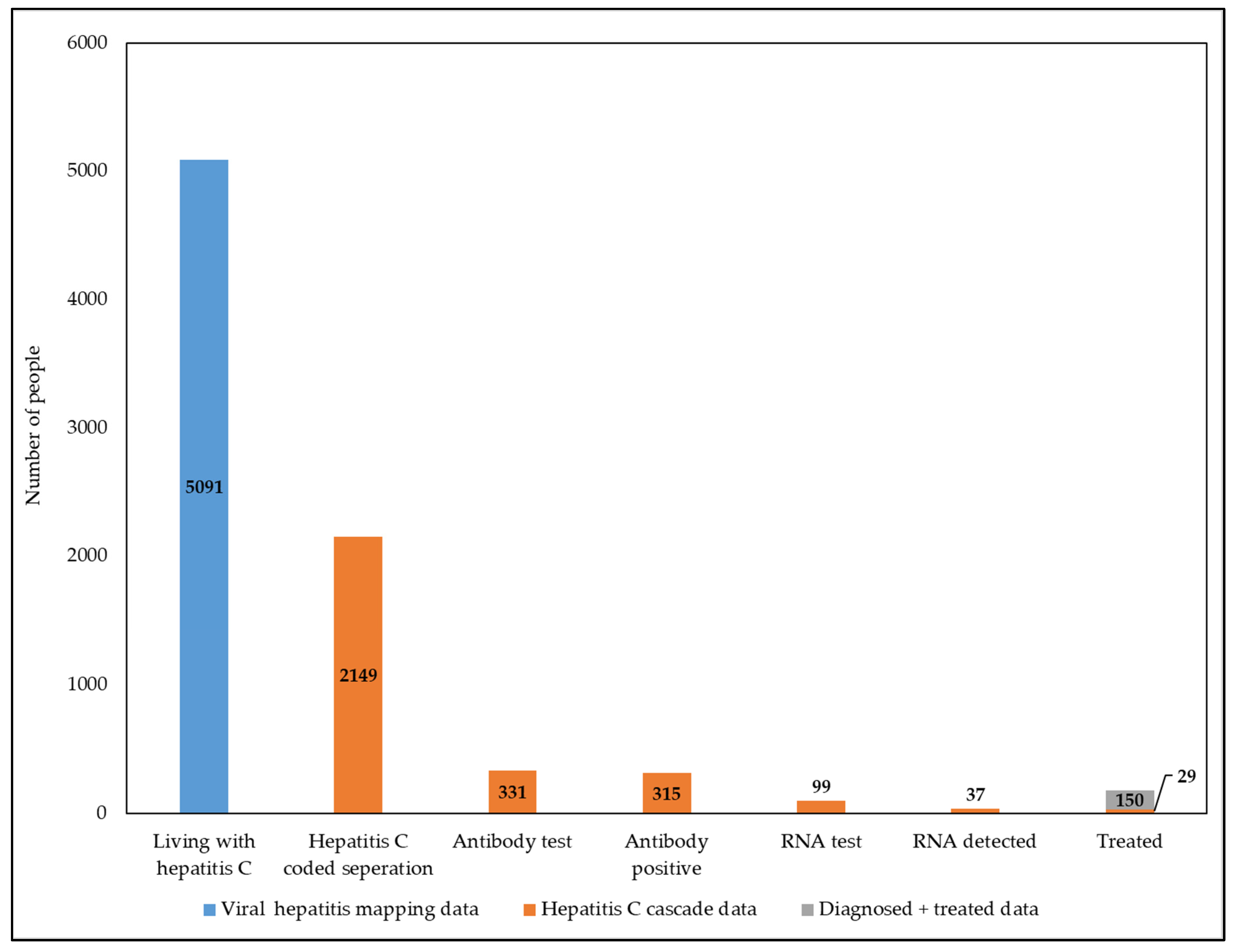
3.2. Hepatitis C Care Cascade
3.3. Identifying Missed Opportunities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Hepatitis Report 2017; World Hepatitis Organization: Geneva, Switzerland, 2017. Available online: https://www.who.int/publications/i/item/9789241565455 (accessed on 21 March 2023).
- World Health Organization. Accelerating Access to Hepatitis C Diagnostics and Treatment: Overcoming Barriers in Low- and Middle-Income Countries; Global Progress Report 2020; World Health Organization: Geneva, Switzerland, 2021. Available online: https://www.who.int/publications/i/item/9789240019003 (accessed on 21 March 2023).
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016. Available online: https://apps.who.int/iris/handle/10665/246177 (accessed on 2 February 2023).
- de Graaff, B.; Yee, K.C.; Clarke, P.; Palmer, A. Uptake of and Expenditure on Direct-Acting Antiviral Agents for Hepatitis C Treatment in Australia. Appl. Health Econ. Health Policy 2018, 16, 495–502. [Google Scholar] [CrossRef] [PubMed]
- MacLachlan, J.H.; Stewart, S.; Cowie, B.C. Viral Hepatitis Mapping Project: National Report 2020; Australasian Society for HIV, Viral Hepatitis, and Sexual Health Medicine (ASHM): Darlinghurst, NSW, Australia, 2020; Available online: https://www.ashm.org.au/programs/Viral-Hepatitis-Mapping-Project/ (accessed on 17 February 2023).
- Scott, N.; Hainsworth, S.W.; Sacks-Davis, R.; Pedrana, A.; Doyle, J.; Wade, A.; Hellard, M. Heterogeneity in hepatitis C treatment prescribing and uptake in Australia: A geospatial analysis of a year of unrestricted treatment access. J. Virus Erad. 2018, 4, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Valerio, H.; Alavi, M.; Law, M.; McManus, H.; Tillakeratne, S.; Bajis, S.; Martinello, M.; Matthews, G.V.; Amin, J.; Janjua, N.Z.; et al. Opportunities to enhance linkage to hepatitis C care among hospitalized people with recent drug dependence in New South Wales, Australia: A population-based linkage study. Clin. Infect. Dis. 2021, 73, 2037–2044. [Google Scholar] [CrossRef] [PubMed]
- Wade, A.J.; McCormack, A.; Roder, C.; McDonald, K.; Davies, M.; Scott, N.; Wardrop, M.; Athan, E.; Hellard, M.E. Aiming for elimination: Outcomes of a consultation pathway supporting regional general practitioners to prescribe direct-acting antiviral therapy for hepatitis C. J. Viral Hepat. 2018, 25, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Roder, C.; Nguyen, P.; Harvey, C.; Wardrop, M.; Finlay, J.; Ogunleye, L.; Hill, H.; Athan, E.; Wade, A.J. Psychiatrists can treat hepatitis C. J. Viral Hepat. 2021, 28, 1763–1764. [Google Scholar] [CrossRef] [PubMed]
- Harney, B.L.; Whitton, B.; Paige, E.; Brereton, R.; Weiss, R.; Membrey, D.; Wade, A.J.; Iser, D.; Kemp, W.; Roberts, S.K.; et al. A multi-site, nurse-coordinated hepatitis C model of care in primary care and community services in Melbourne, Australia. Liver Int. 2022, 42, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Harney, B.L.; Brereton, R.; Whitton, B.; Pietrzak, D.; Paige, E.; Roberts, S.K.; Birks, S.; Saraf, S.; Hellard, M.E.; Doyle, J.S. Hepatitis C treatment in a co-located mental health and alcohol and drug service using a nurse-led model of care. J. Viral Hepat. 2021, 28, 771–778. [Google Scholar] [CrossRef] [PubMed]
- Doyle, J.S.; Scott, N.; Sacks-Davis, R.; Pedrana, A.; Thompson, A.J.; Hellard, M.E.; Eliminate Hepatitis C Partnership. Treatment access is only the first step to hepatitis C elimination: Experience of universal anti-viral treatment access in Australia. Aliment. Pharmacol. Ther. 2019, 49, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Burnet Institute; Kirby Institute. Australia’s Progress towards Hepatitis C Elimination: Annual Report 2022; Burnet Institute: Melbourne, Australia, 2022. [Google Scholar]
- Scott, N.; Doyle, J.S.; Wilson, D.P.; Wade, A.; Howell, J.; Pedrana, A.; Thompson, A.; Hellard, M.E. Reaching hepatitis C virus elimination targets requires health system interventions to enhance the care cascade. Int. J. Drug Policy 2017, 47, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Rosato, V.; Kondili, L.A.; Nevola, R.; Perillo, P.; Mastrocinque, D.; Aghemo, A.; Claar, E. Elimination of Hepatitis C in Southern Italy: A Model of HCV Screening and Linkage to Care among Hospitalized Patients at Different Hospital Divisions. Viruses 2022, 14, 1096. [Google Scholar] [CrossRef] [PubMed]
- Le, E.; Chee, G.; Kwan, M.; Cheung, R. Treating the Hardest to Treat: Reframing the Hospital Admission as an Opportunity to Initiate Hepatitis C Treatment. Dig. Dis. Sci. 2021, 67, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Girardin, F.; Painter, C.; Hearmon, N.; Eddowes, L.; Kaiser, S.; Negro, F.; Vernaz, N. Hepatitis C prevalences in the psychiatric setting: Cost-effectiveness of scaling-up screening and direct-acting antiviral therapy. JHEP Rep. 2021, 3, 100279. [Google Scholar] [CrossRef] [PubMed]
- Alfred Health Annual Report 2019–2020. Available online: https://www.alfredhealth.org.au/about/corporate-publications?category=66|88 (accessed on 15 February 2023).
- WHO. ICD–10/2019 Revision. Available online: https://icd.who.int/browse10/2019/en (accessed on 17 January 2022).
- Wade, A.J.; Doyle, J.S.; Gane, E.; Stedman, C.; Draper, B.; Iser, D.; Roberts, S.K.; Kemp, W.; Petrie, D.; Scott, N.; et al. Outcomes of treatment for hepatitis C in primary care, compared to hospital-based care: A randomized, controlled trial in people who inject drugs. Clin. Infect. Dis. 2019, 70, 1900–1906. [Google Scholar] [CrossRef] [PubMed]
- Hutton, J.; Doyle, J.S.; Zordan, R.; Weiland, T.; Cocco, A.; Howell, J.; Iser, S.; Snell, J.; Fry, S.; New, K.; et al. Point-of-care Hepatitis C virus testing and linkage to treatment in an Australian inner-city emergency department. Int. J. Drug Policy 2019, 72, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Chiong, F.; Post, J. Opportunistic assessment and treatment of people with hepatitis C virus infection admitted to hospital for other reasons: A prospective cohort study. Int. J. Drug Policy 2019, 65, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Roder, C.; Chand, S.; Streat, S.; Beynon, S.; Huning, E.; Dabkowski, P.; Athan, E.; Wade, A.J. Pregnancy—A key moment for engaging women with hepatitis B in care. Aust. New Zealand J. Public Health 2021, 45, 299–300. [Google Scholar] [CrossRef] [PubMed]
- Podubinski, T.; Townsin, L.; Thompson, S.C.; Tynan, A.; Argus, G. Experience of healthcare access in Australia during the first year of the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10687. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Term | Definition |
|---|---|
| Episode | Inpatient admission or attendance to emergency department (ED) |
| Separation coding | The diagnosis coding according to the International Classification of Diseases, Tenth revision (ICD-10) [19] as per the medical information included in the patients discharge/ED summary |
| Hepatitis C exposure | A positive HCV antibody test or hepatitis C separation coding |
| Diagnosis of hepatitis C | A positive HCV RNA test |
| Evidence of treatment | A prescription for DAAs dispensed at the Alfred Hospital pharmacy |
| Episode specialty | Admission ward |
| Hepatitis specialty units | Infectious disease and gastroenterology |
| Mental health | All psychiatric wards |
| Surgical | All general and specialist surgical units. |
| Emergency | Emergency department and trauma unit |
| General medicine | All general medicine wards |
| Other medical specialty | All non-surgical specialty wards |
| Hepatitis C ICD-10 codes [19] | Acute hepatitis C (B171) Chronic viral hepatitis C (B182) Chronic viral hepatitis Unspecified (B189) Unspecified viral hepatitis without hepatic coma (B199) |
| Hospital catchment area [18] | The combination of the following statistical area 3 (SA3) regions:
|
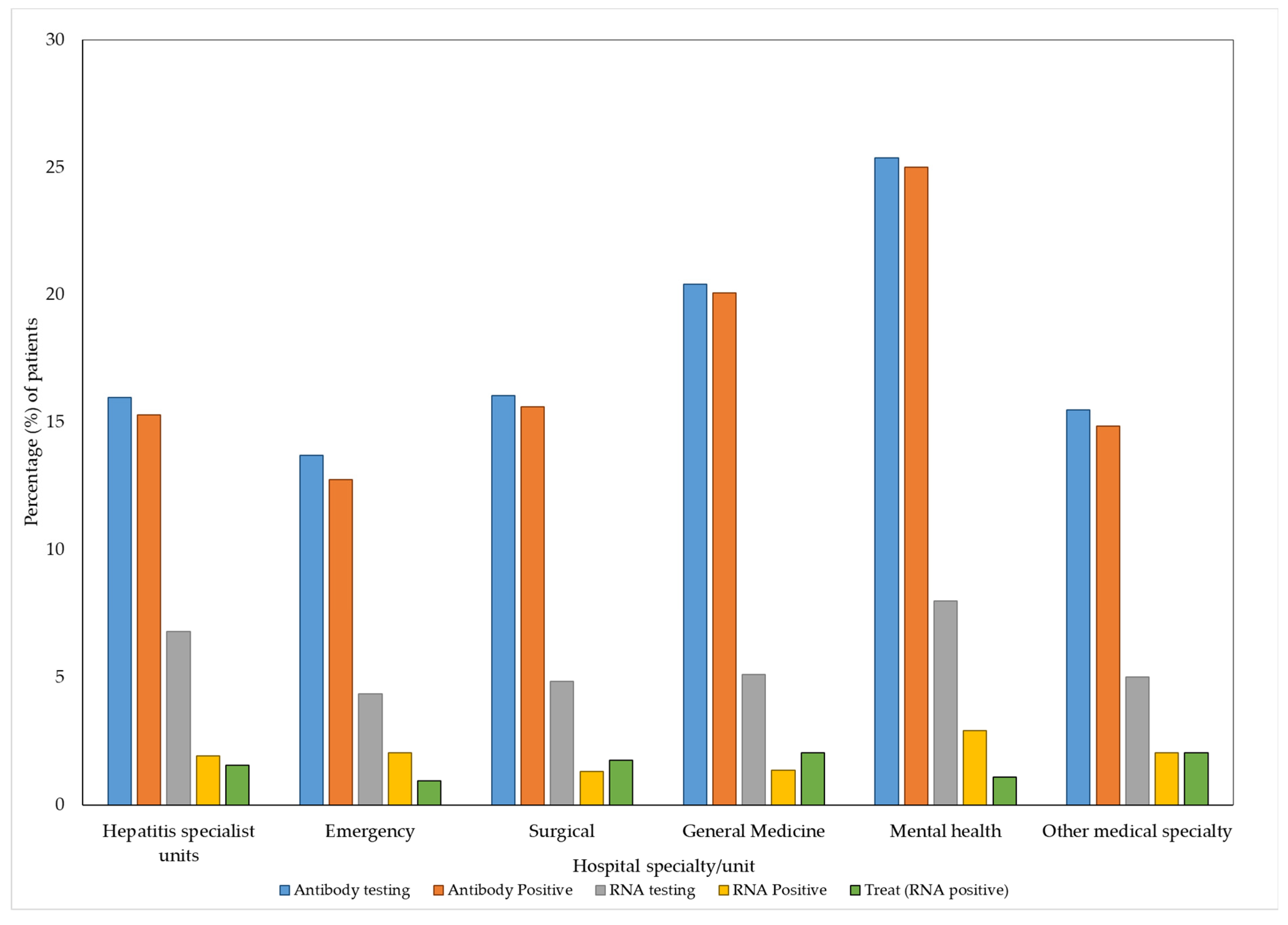
| Unit | Admissions (n = 4901) | Unique Patients (n = 2149 *) | Antibody Testing, n (% of Patients) | Antibody Positive, n (% of Antibody Testing) | RNA Testing, n (% of Antibody Positive) | RNA Positive, n (% of RNA Testing) | Treatment, n (% of Ab Positive) | Treatment, n (% of RNA Positive) | Treatment, n (% of Unique Patients) |
|---|---|---|---|---|---|---|---|---|---|
| Hepatitis Specialist | 1159 (23.6%) | 576 (26.8%) | 92 (16%) | 88 (95.7%) | 39 (44.3%) | 11 (28.2%) | 7 (8%) | 2 (18.2%) | 74 (12.9%) |
| Emergency | 1075 (22%) | 738 (34.3%) | 101 (13.7%) | 94 (93.1%) | 32 (34.1%) | 15 (46.9%) | 5 (5.3%) | 2 (13.3%) | 61 (8.3%) |
| Surgical | 592 (12.1%) | 455 (21.2%) | 73 (16%) | 71 (97.3%) | 22 (31%) | 6 (27.3%) | 7 (9.9%) | 1 (16.7%) | 41 (9%) |
| General Medicine | 469 (9.6%) | 294 (13.7%) | 60 (20.4%) | 59 (98.3%) | 15 (25.4%) | 4 (26.7%) | 6 (10.2%) | 0 | 32 (10.9%) |
| Mental Health | 477 (9.7%) | 276 (12.8%) | 70 (25.4%) | 69 (98.6%) | 22 (31.9%) | 8 (36.4%) | 3 (4.3%) | 0 | 39 (14.1%) |
| Other specialty medicine | 1129 (23%) | 640 (29.8%) | 100 (15.7%) | 95 (96%) | 32 (35.7%) | 13 (40.6%) | 11 (11.6%) | 2 (15.4%) | 68 (10.6%) |
| Specialty | RNA Testing | |||
|---|---|---|---|---|
| OR | 95% CI | aOR | 95% CI | |
| Hepatitis Specialist | 1.95 | 1.26–3.02 | 1.66 | 0.40–6.95 |
| Emergency | 0.94 | 0.59–1.48 | 1.19 | 0.28–5.10 |
| Surgical | 1.18 | 0.71–1.94 | 3.58 | 0.42–30.79 |
| General Medicine | 1.2 | 0.67–2.16 | 1.57 | 0.18–13.89 |
| Mental Health | 2.22 | 1.34–3.69 | 3.16 | 0.37–27.39 |
| Other medical specialties | 1.05 | 0.66–1.67 | 0.51 | 0.13–1.98 |
| Age | 1.02 | 0.96–1.07 | ||
| Sex (male) | 3.04 | 2.29–4.03 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roder, C.; Cosgrave, C.; Mackie, K.; Roberts, S.K.; Hellard, M.E.; Wade, A.J.; Doyle, J.S. Leave No-One Behind: A Retrospective Study of Hepatitis C Testing and Linkage to Care for Hospital Inpatients. Viruses 2023, 15, 913. https://doi.org/10.3390/v15040913
Roder C, Cosgrave C, Mackie K, Roberts SK, Hellard ME, Wade AJ, Doyle JS. Leave No-One Behind: A Retrospective Study of Hepatitis C Testing and Linkage to Care for Hospital Inpatients. Viruses. 2023; 15(4):913. https://doi.org/10.3390/v15040913
Chicago/Turabian StyleRoder, Christine, Carl Cosgrave, Kathryn Mackie, Stuart K. Roberts, Margaret E. Hellard, Amanda J. Wade, and Joseph S. Doyle. 2023. "Leave No-One Behind: A Retrospective Study of Hepatitis C Testing and Linkage to Care for Hospital Inpatients" Viruses 15, no. 4: 913. https://doi.org/10.3390/v15040913