
Multifactorial White Matter Damage in the Acute Phase and Pre-Existing Conditions May Drive Cognitive Dysfunction after SARS-CoV-2 Infection: Neuropathology-Based Evidence
 , , , , , , , , , , ,
, , , , , , , , , , ,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Global Findings
3.2. Specific Alterations
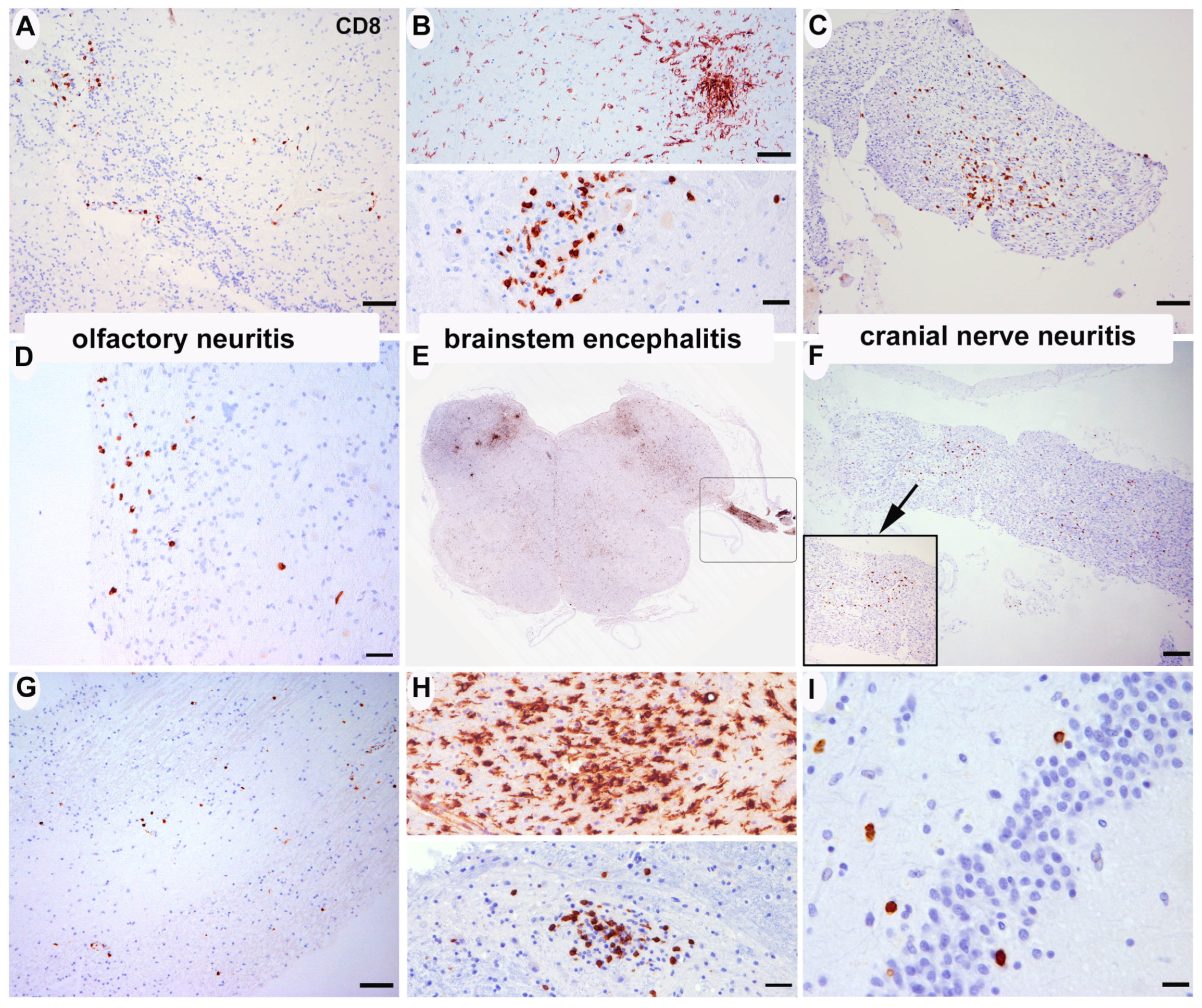
3.2.1. Inflammatory Changes (Figure 1)


{kind=link}
{kind=link}
{kind=link}
| Olfactory Bulb | Hippocampus | Cortical Areas Global | Basal Ganglia Global | Medulla Oblongata | Cerebellum Global | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CD8 | HLA-DR | CD20 | CD8 | HLA-DR | CD20 | CD8 | HLA-DR | CD20 | CD8 | HLA-DR | CD20 | CD8 | HLA-DR | CD20 | CD8 | HLA-DR | CD20 | |
| SARS-CoV-2 | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma |
| Case 1 | na | na | na | +/0 | +++/+++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | na | na | na | na | na | na |
| Case 2 | +/+ | ++/++ | 0/0 | ++/i | +++/++ | 0/0 | ++/0 | +++/+++ | i/0 | +/0 | ++/++ | 0/0 | ++/+ | +++/+++ | i/0 | ++/i | +++/++ | 0/0 |
| Case 3 | +/++ | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/+ | 0/0 | ++/++ | ++/++ | 0/0 | ++/+ | ++/++ | 0/0 |
| Case 4 | i/0 | +++/+++ | i/0 | +/+ | +++/++ | i/0 | +/0 | +++/+++ | i/0 | +/0 | +++/+++ | i/0 | +/++ | +++/+++ | 0/0 | +/0 | +++/+++ | 0/0 |
| Case 5 | +/++ | +++/+++ | 0/0 | +/0 | +++/++ | 0/0 | +/0 | +++/++ | 0/0 | +/0 | +++/++ | 0/0 | +/++ | +++/+++ | +/0 | +/0 | +++/++ | 0/0 |
| Case 6 | +/+ | ++/++ | 0/0 | +/0 | +++/++ | 0/0 | +/0 | +++/++ | 0/0 | +/0 | ++/++ | 0/0 | ++/++ | +++/++ | 0/0 | +/0 | +++/++ | 0/0 |
| Case 7 | +/+ | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | +/+ | 0/0 | ++/++ | +++/++ | i/0 | +/0 | ++/++ | 0/0 |
| Case 8 | i/i | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 |
| Case 9 | i/0 | ++/++ | 0/0 | i/0 | +++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | +++/+++ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 10 | na | na | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 |
| Case 11 | +/0 | ++/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | ++/+ | i/0 | +/0 | +/+ | 0/0 | +/0 | ++/+ | 0/0 | +/0 | ++/+ | 0/0 |
| Case 12 | +/+ | ++/++ | 0/0 | +/0 | +++/++ | 0/0 | +/0 | +++/+++ | i/0 | +/0 | ++/++ | 0/0 | +/+ | ++/++ | 0/0 | +/0 | +++/+++ | 0/0 |
| Case 13 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 |
| Case 14 | i/0 | ++/++ | 0/0 | +/0 | ++/++ * | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | +++/+++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 15 | i/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 16 | i/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/+ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/+++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 17 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 18 | i/0 | ++/++ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | i/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 19 | +/0 | ++/++ | i/0 | +/0 | +++/++ | i/0 | +/0 | +/+ | 0/0 | +/0 | ++/++ | 0/0 | ++/+ | +++/+++ | 0/0 | +/0 | +++/++ | 0/0 |
| Case 20 | +/0 | +/+ | i/0 | +/0 | ++/+ | 0/0 | +/0 | +/+ | i/0 | +/0 | +/+ | i/0 | +/0 | ++/++ | 0/0 | +/0 | ++/+ | 0/0 |
| Case 21 | +/+ | ++/++ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | ++/++ | ++/++ | 0/0 | +/0 | +/+ | 0/0 |
| Case 22 | +/++ | ++/++ | 0/0 | +/0 | ++/+ | +/0 | +/0 | +/+ | 0/0 | +/0 | ++/++ | +/+ | +/i | ++/+ | i/0 | ++/0 | ++/+ | i/0 |
| Case 23 | i/0 | ++/++ | 0/0 | +/0 | ++/+ | +/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 24 | i/0 | ++/++ | 0/0 | +/0 | ++/+ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 25 | +/0 | ++/++ | 0/0 | +/0 | +++/++ | 0/0 | +/0 | +++/+++ | 0/0 | +/0 | +++/+++ | 0/0 | +/0 | +++/+++ | 0/0 | +/0 | +++/+++ | 0/0 |
| Case 26 | i/0 | +/+ | 0/0 | i/0 | ++/+ | 0/0 | i/0 | +/+ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | i/0 | +/0 | ++/++ | 0/0 |
| Case 27 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | +/+ | 0/0 | i/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 28 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/+ | 0/0 | +/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 29 | i/0 | ++/++ | 0/0 | +/0 | ++/+ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 30 | +/i | ++/++ | 0/0 | i/0 | +++/+++ | 0/0 | i/0 | +++/+++ | 0/0 | i/0 | +++/+++ | 0/0 | +/+ | +++/+++ | 0/0 | +/+ | +++/+++ | 0/0 |
| Case 31 | i/0 | +/++ | 0/0 | i/0 | ++/+ | 0/0 | i/0 | +/+ | 0/0 | i/0 | +/+ | 0/0 | i/0 | ++/++ | 0/0 | i/0 | ++/+ | 0/0 |
| Case 32 | +/+ | ++/++ | 0/0 | ++/++ | +++/+++ | 0/0 | ++/+ | ++/++ | 0/0 | ++/+ | +++/+++ | 0/0 | +/+ | +++/+++ | 0/0 | +/0 | ++/++ | 0/0 |
| H1N1 | ||||||||||||||||||
| Case 1 | na | na | na | +/0 | ++/+ | 0/0 | i/0 | ++/+ | 0/0 | +/0 | +/+ | 0/0 | +/0 | +/++ | 0/0 | i/0 | +/+ | 0/0 |
| Case 2 | na | na | na | +/0 | +/++ | 0/0 | i/0 | +/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 3 | na | na | na | +/0 | +/+ | 0/0 | i/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 | +/i | +/++ | 0/0 | i/0 | +/+ | 0/0 |
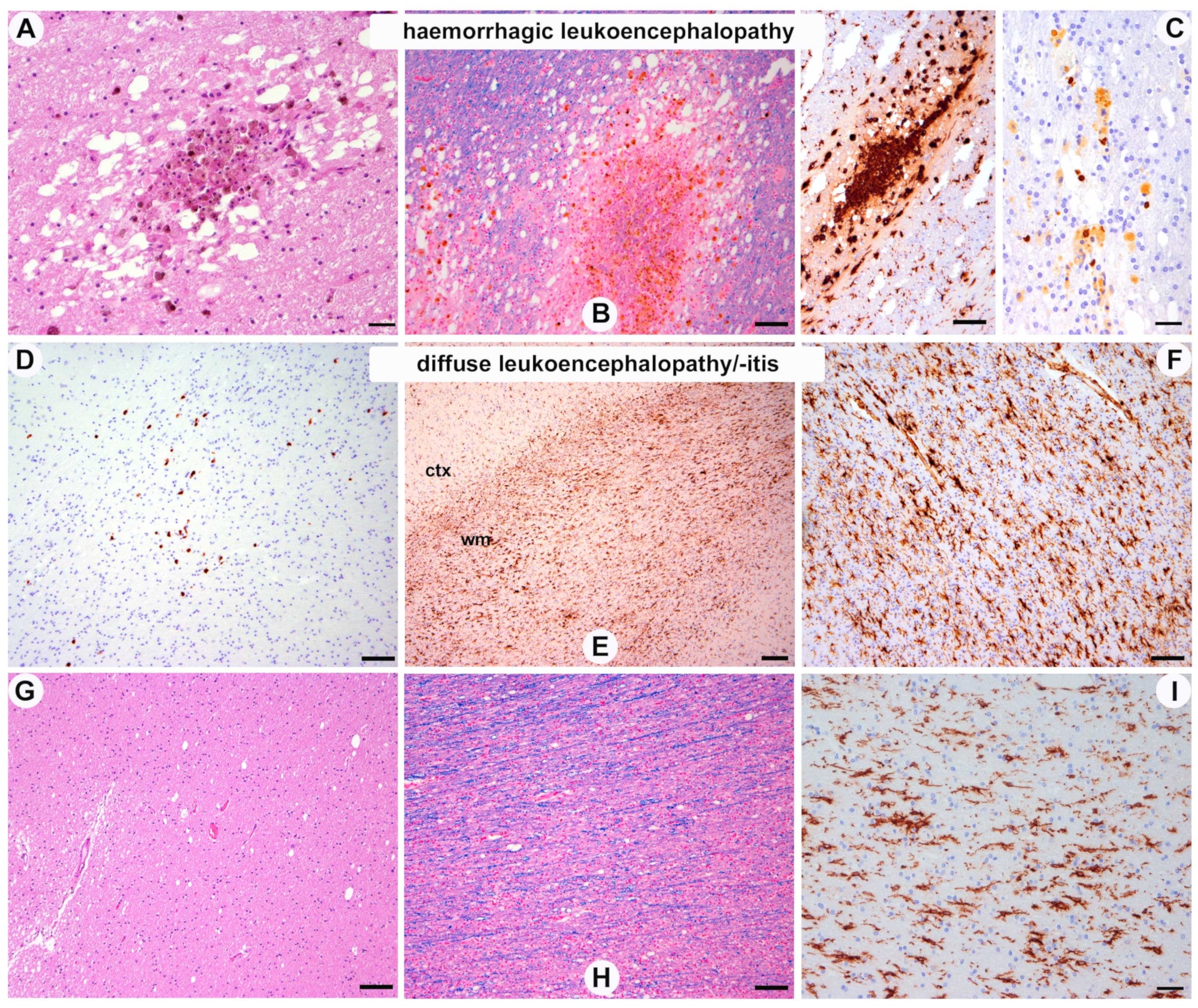
3.2.2. White Matter Pathology (Figure 2)

| White Matter Supratentorial | White Matter Cerebellum | |||||
|---|---|---|---|---|---|---|
| CD8 | HLA-DR | CD20 | CD8 | HLA-DR | CD20 | |
| Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | Perivascular/Parenchyma | |
| Case 1 | +/0 | ++/+++ | 0/0 | na | na | na |
| Case 2 | +/++ | ++/+++ | 0/0 | ++/i | +++/++ | 0/0 |
| Case 3 | +/0 | ++/+++ | 0/0 | ++/+ | ++/++ | 0/0 |
| Case 4 | +/0 | ++/+++ | i/0 | +/0 | +++/+++ | 0/0 |
| Case 5 | +/0 | +++/++ | 0/0 | +/0 | +++/++ | 0/0 |
| Case 6 | i/0 | ++/+++ | 0/0 | +/0 | +++/++ | 0/0 |
| Case 7 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 8 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 |
| Case 9 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 10 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 |
| Case 11 | +/0 | +/+ | 0/0 | +/0 | ++/+ | 0/0 |
| Case 12 | +/0 | ++/+++ | 0/0 | +/0 | +++/+++ | 0/0 |
| Case 13 | +/0 | +/+ | 0/0 | +/0 | +/+ | 0/0 |
| Case 14 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 15 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 16 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 17 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 18 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 19 | +/0 | ++/++ | 0/0 | +/0 | +++/++ | 0/0 |
| Case 20 | +/0 | ++/+ | i/0 | +/0 | ++/+ | 0/0 |
| Case 21 | +/0 | ++/++ | 0/0 | +/0 | +/+ | 0/0 |
| Case 22 | +/0 | ++/+ | 0/0 | ++/0 | ++/+ | i/0 |
| Case 23 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 24 | +/0 | ++/++ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 25 | +/0 | +++/++ | 0/0 | +/0 | +++/+++ | 0/0 |
| Case 26 | +/0 | ++/+ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 27 | +/0 | ++/+ | 0/0 | +/0 | ++/++ | 0/0 |
| Case 28 | +/0 | ++/+ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 29 | i/0 | ++/++ | 0/0 | i/0 | ++/++ | 0/0 |
| Case 30 | i/0 | +++/+++ | 0/0 | +/+ | +++/+++ | 0/0 |
| Case 31 | i/0 | +/+ | 0/0 | i/0 | ++/+ | 0/0 |
| Case 32 | +/0 | +++/+++ | 0/0 | +/0 | ++/++ | 0/0 |
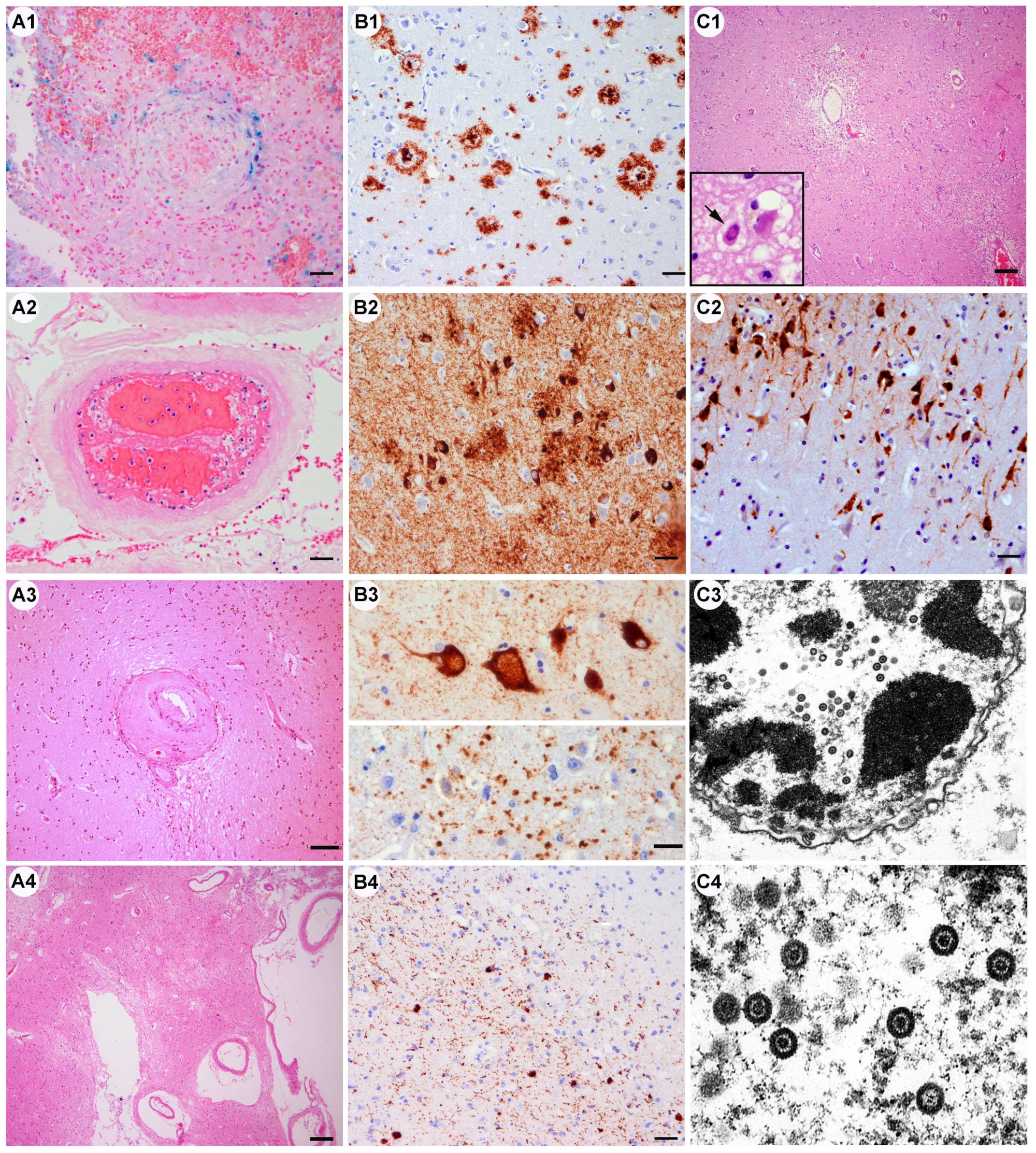
3.2.3. Vascular Pathology (Figure 3A, Table 4 and Table 5)
3.2.4. Pre-Existing Neurodegenerative Pathology (Figure 3B, Table 4)

3.2.5. Other
| Pathology (n = 32) | n° of Cases (%) |
|---|---|
| Vascular | |
| Small vessel disease, pre-exisiting | 11 (34%) |
| Large territorial infarct | 7 (22%) |
| Vascular thrombosis | 4 (12.5%) |
| Vasculitis/endotheliitis | 0 |
| Diffuse hypoxic–ischemic damage | 13 (40%) |
| Acute hemorrhage | 1 (3%) |
| Inflammation | |
| Olfactory neuritis | 8 (25%) |
| Brainstem encephalitis micronodular | 10 (31%) |
| Cranial nerve neuritis | 2 (6%) |
| Encephalitis | 0 |
| Myelitis | 0 |
| Meningitis/ependymitis/plexitis | 0 |
| Peripheral neuritis | 0 |
| Myositis | 0 |
| Vasculitis/endotheliitis | 0 |
| White matter pathology | |
| Hemorrhagic leukoencephalopathy | 1 (3%) |
| Diffuse leukoencephalopathy/microglial activation | 32 (100%) |
| ADEM | 0 |
| Neurodegenerative changes preexisting | |
| ADNC | 10 (32%) |
| PART | 5 (16%) |
| ARTAG | 2 (6%) |
| Lewy bodies | 3 (9%) |
| TDP-43 proteinopathy | 2 (6%) |
| Argyrophilic grain disease | 6 (18%) |
| Other | |
| Fulminant Herpes simplex encephalitis | 1 (3%) |
| Acute traumatic brain injury | 1 (3%) |
| Case | Age | Sex | Inflammation | Vascular Pathology/Other | Neurodeg Pathology |
|---|---|---|---|---|---|
| Case 1 | 88 | F | - | SVD, lacunar infarct | ADNC A2B3C2, LATE |
| Case 2 | 79 | M | Olfactory neuritis, micronodular brainstem encephalitis, cranial nerve neuritis | Patchy acute hypoxic–ischemic neuronal damage | PART II, ARTAG |
| Case 3 | 80 | F | Olfactory neuritis, micronodular brainstem encephalitis | - | ADNC A3B3C2 + CAA |
| Case 4 | 62 | F | micronodular brainstem encephalitis | Hemorrhagic leukoencephalopathy | iLBD 3, PART II |
| Case 5 | 69 | M | Olfactory neuritis, micronodular brainstem encephalitis, cranial nerve neuritis | Incidental cavernoma frontal | ADNC A3B2C2 + CAA |
| Case 6 | 79 | M | Olfactory neuritis, micronodular brainstem encephalitis | Laminar occipital cortical necrosis older bilat (Morel) | AgD II |
| Case 7 | 58 | M | Olfactory neuritis | SVD | - |
| Case 8 | 71 | F | - | Patchy acute hypoxic–ischemic neuronal damage, SVD | AgD I |
| Case 9 | 58 | M | - | Severe diffuse posthypoxic–postischemic pan encephalopathy with dural sinus thrombosis and meningeal vessel thrombosis; brainstem hemorrhage (Duret) | ADNC A1B0C0 |
| Case 10 | 80 | M | - | Old infarct cerebellum, SVD | LBD 4, ADNC A2B1C2 |
| Case 11 | 80 | F | - | Old lacunar infarct pons, SVD, patchy acute hypoxic–ischemic neuronal damage | iLBD 1, PART III |
| Case 12 | 66 | M | Olfactory neuritis, micronodular brainstem encephalitis | Acute cortical laminar necrosis occipital and parietal | - |
| Case 13 | 54 | M | - | Subacute infarct cerebellum | - |
| Case 14 | 97 | F | - | SVD | ADNC A3B3C3 + CAA |
| Case 15 | 71 | F | - | SVD, patchy acute hypoxic–ischemic neuronal damage | PART II |
| Case 16 | 57 | F | Micronodular brainstem encephalitis | Patchy acute hypoxic–ischemic neuronal damage | PART II |
| Case 17 | 81 | M | - | Patchy acute hypoxic–ischemic neuronal damage | ADNC A3B1C1 |
| Case 18 | 73 | M | - | - | ADNC A1B1C1, AgD I |
| Case 19 | 64 | M | Micronodular brainstem encephalitis | Small thrombus meningeal vessels frontal | ARTAG |
| Case 20 | 66 | M | Micronodular brainstem encephalitis | Acute partly hemorrhagic cortical infarcts cingulum and parietal ctx | - |
| Case 21 | 38 | M | Olfactory neuritis, micronodular brainstem encephalitis | Diffuse acute hypoxic–ischemic neuronal damage, CO intoxication | - |
| Case 22 | 34 | M | Olfactory neuritis | Patchy acute hypoxic–ischemic neuronal damage | - |
| Case 23 | 72 | M | - | Old SDH and SAB, patchy acute hypoxic–ischemic neuronal damage | - |
| Case 24 | 52 | F | - | Perivascular fibrosis (systemic sclerosis known) | - |
| Case 25 | 64 | M | Mild hypothalamus | Multiple bilateral old cortical laminar necrosis and cerebellar necrosis; sinus vein thrombosis | AgD III |
| Case 26 | 86 | M | - | Hemorrhagic infarcts frontal and frontobasal, vascular thrombosis | AgD I, LATE, ADNC A2B1C1 |
| Case 27 | 62 | F | - | Severe venous congestion and SAB occipital | ADNC A2B0C1 + CAA |
| Case 28 | 82 | F | - | SVD, acute traumatic SDH + SAB + acute hypoxic damage + diffuse axonal injury | AgD II, ADNC A3B2C2 |
| Case 29 | 67 | F | - | Old thalamic lacunar infarct, SVD, metabolic gliosis | ADNC A1B0C0 |
| Case 30 | 49 | M | - | Multiple subacute infarcts cingulum, amygdala, occipitomental, pons, medulla dorsolateral, cerebellum; Wernicke-like changes (alcohol abuse) | - |
| Case 31 | 21 | M | - | Patchy acute hypoxic–ischemic neuronal damage | - |
| Case 32 | 57 | F | HSV-related encephalitis | Red neurons in encephalitis regions |
3.2.6. H1N1-Infected Cases (Table 2)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ritchie, K.; Chan, D.; Watermeyer, T. The cognitive consequences of the COVID-19 epidemic: Collateral damage? Brain Commun. 2020, 2, fcaa069. [Google Scholar] [CrossRef] [PubMed]
- Yachou, Y.; El Idrissi, A.; Belapasov, V.; Ait Benali, S. Neuroinvasion, neurotropic, and neuroinflammatory events of SARS-CoV-2: Understanding the neurological manifestations in COVID-19 patients. Neurol. Sci. 2020, 41, 2657–2669. [Google Scholar] [CrossRef]
- Travi, G.; Rossotti, R.; Merli, M.; D’Amico, F.; Chiappetta, S.; Giussani, G.; Panariello, A.; Corradin, M.; Vecchi, M.; Raimondi, A.; et al. Neurological manifestations in patients hospitalized with COVID-19: A retrospective analysis from a large cohort in Northern Italy. Eur. J. Neurosci. 2021, 53, 2912–2922. [Google Scholar] [CrossRef]
- Al-Sarraj, S.; Troakes, C.; Hanley, B.; Osborn, M.; Richardson, M.P.; Hotopf, M.; Bullmore, E.; Everall, I.P. Invited Review: The spectrum of neuropathology in COVID-19. Neuropathol. Appl. Neurobiol. 2021, 47, 3–16. [Google Scholar] [CrossRef]
- Maiese, A.; Manetti, A.C.; Bosetti, C.; Del Duca, F.; La Russa, R.; Frati, P.; Di Paolo, M.; Turillazzi, E.; Fineschi, V. SARS-CoV-2 and the brain: A review of the current knowledge on neuropathology in COVID-19. Brain Pathol. 2021, 31, e13013. [Google Scholar] [CrossRef]
- Kantonen, J.; Mahzabin, S.; Mäyränpää, M.I.; Tynninen, O.; Paetau, A.; Andersson, N.; Sajantila, A.; Vapalahti, O.; Carpén, O.; Kekäläinen, E.; et al. Neuropathologic features of four autopsied COVID-19 patients. Brain Pathol. 2020, 30, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F., Jr.; Sabeti, P. Neuropathological Features of COVID-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef]
- Mehta, S.; Bhandari, S.; Mehta, S. Brain autopsies in fatal COVID-19 and postulated pathophysiology: More puzzling than a Rubik’s cube. J. Clin. Pathol. 2021, 74, 612–613. [Google Scholar] [CrossRef]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Glatzel, M.; Hagel, C.; Matschke, J.; Sperhake, J.; Deigendesch, N.; Tzankov, A.; Frank, S. Neuropathology associated with SARS-CoV-2 infection. Lancet 2021, 397, 276. [Google Scholar] [CrossRef]
- Nasrallah, M.P.; Mourelatos, Z.; Lee, E.B. Neuropathology associated with SARS-CoV-2 infection. Lancet 2021, 397, 277. [Google Scholar] [CrossRef] [PubMed]
- Egervari, K.; Thomas, C.; Lobrinus, J.A.; Kuhlmann, T.; Brück, W.; Love, S.; Crary, J.F.; Stadelmann, C.; Paulus, W.; Merkler, D. Neuropathology associated with SARS-CoV-2 infection. Lancet 2021, 397, 276–277. [Google Scholar] [CrossRef] [PubMed]
- Reichard, R.R.; Kashani, K.B.; Boire, N.A.; Constantopoulos, E.; Guo, Y.; Lucchinetti, C.F. Neuropathology of COVID-19: A spectrum of vascular and acute disseminated encephalomyelitis (ADEM)-like pathology. Acta Neuropathol. 2020, 140, 1–6. [Google Scholar] [CrossRef]
- Kirschenbaum, D.; Imbach, L.L.; Rushing, E.J.; Frauenknecht, K.B.M.; Gascho, D.; Ineichen, B.V.; Keller, E.; Kohler, S.; Lichtblau, M.; Reimann, R.R.; et al. Intracerebral endotheliitis and microbleeds are neuropathological features of COVID-19. Neuropathol. Appl. Neurobiol. 2021, 47, 454–459. [Google Scholar] [CrossRef]
- Lou, J.J.; Movassaghi, M.; Gordy, D.; Olson, M.G.; Zhang, T.; Khurana, M.S.; Chen, Z.; Perez-Rosendahl, M.; Thammachantha, S.; Singer, E.J.; et al. Neuropathology of COVID-19 (neuro-COVID): Clinicopathological update. Free Neuropathol. 2021, 2, 2. [Google Scholar] [PubMed]
- Thakur, K.T.; Miller, E.H.; Glendinning, M.D.; Al-Dalahmah, O.; Banu, M.A.; Boehme, A.K.; Boubour, A.L.; Bruce, S.S.; Chong, A.M.; Claassen, J.; et al. COVID-19 neuropathology at Columbia University Irving Medical Center/New York Presbyterian Hospital. Brain 2021, 144, awab148. [Google Scholar] [CrossRef]
- Deigendesch, N.; Sironi, L.; Kutza, M.; Wischnewski, S.; Fuchs, V.; Hench, J.; Frank, A.; Nienhold, R.; Mertz, K.D.; Cathomas, G.; et al. Correlates of critical illness-related encephalopathy predominate postmortem COVID-19 neuropathology. Acta Neuropathol. 2020, 140, 583–586. [Google Scholar] [CrossRef]
- Fisicaro, F.; Di Napoli, M.; Liberto, A.; Fanella, M.; Di Stasio, F.; Pennisi, M.; Bella, R.; Lanza, G.; Mansueto, G. Neurological Sequelae in Patients with COVID-19: A Histopathological Perspective. Int. J. Environ. Res. Public Health 2021, 18, 1415. [Google Scholar] [CrossRef]
- Manca, R.; De Marco, M.; Ince, P.G.; Venneri, A. Heterogeneity in Regional Damage Detected by Neuroimaging and Neuropathological Studies in Older Adults With COVID-19: A Cognitive-Neuroscience Systematic Review to Inform the Long-Term Impact of the Virus on Neurocognitive Trajectories. Front. Aging Neurosci. 2021, 13, 646908. [Google Scholar] [CrossRef]
- Hosp, J.A.; Dressing, A.; Blazhenets, G.; Bormann, T.; Rau, A.; Schwabenland, M.; Thurow, J.; Wagner, D.; Waller, C.; Niesen, W.D.; et al. Cognitive impairment and altered cerebral glucose metabolism in the subacute stage of COVID-19. Brain 2021, 144, 1263–1276. [Google Scholar] [CrossRef]
- Altuna, M.; Sanchez-Saudinos, M.B.; Lleo, A. Cognitive symptoms after COVID-19. Neurol. Perspect. 2021, 1 (Suppl. S1), s16–s24. [Google Scholar] [CrossRef]
- Hixon, A.M.; Thaker, A.A.; Pelak, V.S. Persistent visual dysfunction following posterior reversible encephalopathy syndrome due to COVID-19: Case series and literature review. Eur. J. Neurol. 2021, 28, 3289–3302. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.M.; Gilbert, A.R.; Bieniek, K.F.; Richardson, T.E. COVID-19 Patients with CNS Complications and Neuropathologic Features of Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalopathy. J. Neuropathol. Exp. Neurol. 2021, 80, 628–631. [Google Scholar] [CrossRef]
- Rogers, J.P.; Chesney, E.; Oliver, D.; Pollak, T.A.; McGuire, P.; Fusar-Poli, P.; Zandi, M.S.; Lewis, G.; David, A.S. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: A systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 611–627. [Google Scholar] [CrossRef]
- Heming, M.; Li, X.; Räuber, S.; Mausberg, A.K.; Börsch, A.L.; Hartlehnert, M.; Singhal, A.; Lu, I.N.; Fleischer, M.; Szepanowski, F.; et al. Neurological manifestations of COVID-19 feature T cell exhaustion and dedifferentiated monocytes in cerebrospinal fluid. Immunity 2021, 54, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Song, E.; Bartley, C.M.; Chow, R.D.; Ngo, T.T.; Jiang, R.; Zamecnik, C.R.; Dandekar, R.; Loudermilk, R.P.; Dai, Y.; Liu, F.; et al. Divergent and self-reactive immune responses in the CNS of COVID-19 patients with neuro-logical symptoms. Cell Rep. Med. 2021, 2, 100288. [Google Scholar] [CrossRef]
- Etter, M.M.; Martins, T.A.; Kulsvehagen, L.; Pössnecker, E.; Duchemin, W.; Hogan, S.; Sanabria-Diaz, G.; Müller, J.; Chiappini, A.; Rychen, J.; et al. Severe Neuro-COVID is associated with peripheral immune signatures, autoimmunity and neurodegeneration: A prospective cross-sectional study. Nat. Commun. 2022, 13, 6777. [Google Scholar] [CrossRef]
- Bonetto, V.; Pasetto, L.; Lisi, I.; Carbonara, M.; Zangari, R.; Ferrari, E.; Punzi, V.; Luotti, S.; Bottino, N.; Biagianti, B.; et al. Markers of blood-brain barrier disruption increase early and persistently in COVID-19 patients with neurological manifestations. Front. Immunol. 2022, 13, 1070379. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Gomes, M.; Kruglov, A.; Durek, P.; Heinrich, F.; Tizian, C.; Heinz, G.A.; Pascual-Reguant, A.; Du, W.; Mothes, R.; Fan, C.; et al. SARS-CoV-2 in severe COVID-19 induces a TGF-β-dominated chronic immune response that does not target itself. Nat. Commun. 2021, 12, 1961. [Google Scholar] [CrossRef]
- Bernard-Valnet, R.; Perriot, S.; Canales, M.; Pizzarotti, B.; Caranzano, L.; Castro-Jiménez, M.; Epiney, J.-B.; Vijiala, S.; Salvioni-Chiabotti, P.; Anichini, A.; et al. Encephalopathies associ-ated with severe COVID-19 present neurovascular unit alterations without evidence for strong neuroinflammation. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, e1029. [Google Scholar] [CrossRef]
- Fernández-Castañeda, A.; Lu, P.; Geraghty, A.C.; Song, E.; Lee, M.H.; Wood, J.; Yalçın, B.; Taylor, K.R.; Dutton, S.; Acosta-Alvarez, L.; et al. Mild respiratory SARS-CoV-2 infection can cause multi-lineage cellular dysregulation and myelin loss in the brain. Cell 2022, 185, 2452–2468. [Google Scholar] [CrossRef] [PubMed]
- Daroische, R.; Hemminghyth, M.S.; Eilertsen, T.H.; Breitve, M.H.; Chwiszczuk, L.J. Cognitive Impairment after COVID-19-A Review on Objective Test Data. Front. Neurol. 2021, 12, 699582. [Google Scholar] [CrossRef] [PubMed]
- Buyanova, I.S.; Arsalidou, M. Cerebral White Matter Myelination and Relations to Age, Gender, and Cognition: A Selective Review. Front. Hum. Neurosci. 2021, 15, 662031. [Google Scholar] [CrossRef]
- MacLean, M.A.; Kamintsky, L.; Leck, E.D.; Friedman, A. The potential role of microvascular pathology in the neurological manifestations of coronavirus infection. Fluids Barriers CNS 2020, 17, 55. [Google Scholar] [CrossRef]
- Gutierrez Amezcua, J.M.; Jain, R.; Kleinman, G.; Muh, C.R.; Guzzetta, M.; Folkerth, R.; Snuderl, M.; Placantonakis, D.G.; Galetta, S.L.; Hochman, S.; et al. COVID-19-Induced Neurovascular Injury: A Case Series with Emphasis on Pathophysiological Mechanisms. SN Compr. Clin. Med. 2020, 2, 2109–2125. [Google Scholar] [CrossRef]
- Jaunmuktane, Z.; Mahadeva, U.; Green, A.; Sekhawat, V.; Barrett, N.A.; Childs, L.; Shankar-Hari, M.; Thom, M.; Jäger, H.R.; Brandner, S. Microvascular injury and hypoxic damage: Emerging neuropathological signatures in COVID-19. Acta Neuropathol. 2020, 140, 397–400. [Google Scholar] [CrossRef]
- Keller, E.; Brandi, G.; Winklhofer, S.; Imbach, L.L.; Kirschenbaum, D.; Frontzek, K.; Steiger, P.; Dietler, S.; Haeberlin, M.; Willms, J.; et al. Large and Small Cerebral Vessel Involvement in Severe COVID-19: Detailed Clinical Workup of a Case Series. Stroke 2020, 51, 3719–3722. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, R.; Ferrante, L.E. Long-term recovery after critical illness in older adults. Curr. Opin. Crit. Care 2022, 28, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Cadar, D.; Jellinger, K.A.; Riederer, P.; Strobel, S.; Monoranu, C.M.; Tappe, D. No Metagenomic Evidence of Causative Viral Pathogens in Postencephalitic Parkinsonism Following Encephalitis Lethargica. Microorganisms 2021, 9, 1716. [Google Scholar] [CrossRef] [PubMed]
- Bulfamante, G.; Bocci, T.; Falleni, M.; Campiglio, L.; Coppola, S.; Tosi, D.; Chiumello, D.; Priori, A. Brainstem neuropathology in two cases of COVID-19: SARS-CoV-2 trafficking between brain and lung. J. Neurol. 2021, 268, 4486–4491. [Google Scholar] [CrossRef] [PubMed]
- Bulfamante, G.; Chiumello, D.; Canevini, M.P.; Priori, A.; Mazzanti, M.; Centanni, S.; Felisati, G. First ultrastructural autoptic findings of SARS -CoV-2 in olfactory pathways and brainstem. Minerva Anestesiol. 2020, 86, 678–679. [Google Scholar] [CrossRef] [PubMed]
- Montini, F.; Martinelli, V.; Sangalli, F.; Callea, M.; Anzalone, N.; Filippi, M. Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS) after SARS-CoV-2 pneumonia. Neurol. Sci. 2021, 42, 4373–4375. [Google Scholar] [CrossRef] [PubMed]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef]
- Aschman, T.; Mothes, R.; Heppner, F.L.; Radbruch, H. What SARS-CoV-2 does to our brains. Immunity 2022, 55, 1159–1172. [Google Scholar] [CrossRef]
- Li, Y.C.; Zhang, Y.; Tan, B.H. What can cerebrospinal fluid testing and brain autopsies tell us about viral neuroinvasion of SARS-CoV-2. J. Med. Virol. 2021, 93, 4247–4257. [Google Scholar] [CrossRef] [PubMed]
- Serrano, G.E.; Walker, J.E.; Tremblay, C.; Piras, I.S.; Huentelman, M.J.; Belden, C.M.; Goldfarb, D.; Shprecher, D.; Atri, A.; Adler, C.H.; et al. SARS-CoV-2 Brain Regional Detection, Histopathology, Gene Expression, and Immunomodulatory Changes in Decedents with COVID-19. J. Neuropathol. Exp. Neurol. 2022, 81, 666–695. [Google Scholar] [CrossRef]
- Poloni, T.E.; Medici, V.; Moretti, M.; Visonà, S.D.; Cirrincione, A.; Carlos, A.F.; Davin, A.; Gagliardi, S.; Pansarasa, O.; Cereda, C.; et al. COVID-19-related neuropathology and microglial activation in elderly with and without dementia. Brain Pathol. 2021, 31, e12997. [Google Scholar] [CrossRef]
- Pröbstel, A.K.; Schirmer, L. SARS-CoV-2-specific neuropathology: Fact or fiction? Trends Neurosci. 2021, 44, 933–935. [Google Scholar] [CrossRef]
- Schmidbauer, M.; Budka, H.; Ambros, P. Herpes simplex virus (HSV) DNA in microglial nodular brainstem encephalitis. J. Neuropathol. Exp. Neurol. 1989, 48, 645–652. [Google Scholar] [CrossRef]
- Cosentino, G.; Todisco, M.; Hota, N.; Della Porta, G.; Morbini, P.; Tassorelli, C.; Pisani, A. Neuropathological findings from COVID-19 patients with neurological symptoms argue against a direct brain invasion of SARS-CoV-2: A critical systematic review. Eur. J. Neurol. 2021, 28, 3856–3865. [Google Scholar] [CrossRef]
- Remmelink, M.; De Mendonça, R.; D’Haene, N.; De Clercq, S.; Verocq, C.; Lebrun, L.; Lavis, P.; Racu, M.L.; Trépant, A.L.; Maris, C.; et al. Unspecific post-mortem findings despite multiorgan viral spread in COVID-19 patients. Crit. Care 2020, 24, 495. [Google Scholar] [CrossRef] [PubMed]
- Budka, H. Flaviviruses 1. General Introduction and Tick Borne Encephalitis. In Infections of the Central Nervous System: Neuropathology and Genetics; Chrétien, F., Wong, K.T., Sharer, L.R., Keohane, C., Gray, F., Eds.; International Society of Neuropathology (ISN) Book Series Pathology and Genetics; Wiley: Hoboken, NJ, USA, 2020; Chapter 14; pp. 131–146. [Google Scholar]
- Kreye, J.; Reincke, S.M.; Prüss, H. Do cross-reactive antibodies cause neuropathology in COVID-19? Nat. Rev. Immunol. 2020, 20, 645–646. [Google Scholar] [CrossRef] [PubMed]
- Budka, H. HIV-Related Dementia: Pathology and Possible Pathogenesis. In The Neuropathology of HIV Infection; Scaravilli, F., Ed.; Springer: London, UK, 1993; pp. 171–185. [Google Scholar]
| Age | Sex | Clinical Diagnosis | Cause of Death | Disease Duration | Days in ICU | Neurological Symptoms | Vascular Risk Factors | Additional co-Morbidities | Treatments | SARS-CoV-2 PCR Positivity | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 88 | Female | na | na | na | na | na | na | na | na | na * |
| Case 2 | 78 | Male | COVID-19 pneumonia | Cardiovascular failure | 56 | 48 | Did not regain consciousness after stop of narcotics | Diabetes, hypertension, obesity, atrial fibrillation | Dilatative cardiomyopathy, arteriosclerosis | Remdesivir | blood, perianal, trachea, larynx |
| Case 3 | 79 | Female | COVID-19 pneumonia | Pulmonary thrombosis, pulmonary bleeding, Sepsis | 18 | 11 | None | Hypertension, obesity | - | Kaletra, cortisone, 3 doses reconvalescent plasma, remdesivir | Larynx |
| Case 4 | 62 | Female | COVID-19 pneumonia | Respiratory failure | na | 63 | Critical illness polyneuropathy/myopathy, reduced vigilance, EEG diffuse slowing | Atrial fibrillation, arterial hypertension | Suspicion of latent tuberculosis | Cortisone; positive EBV PCR- Ganciclovir | na * |
| Case 5 | 68 | Male | COVID-19 pneumonia | Multi-organ failure | 31 | 27 | Agitation, confusion, aggression, psychosis | Diabetes, hypertension, obesity | Pulmonary emphysema, steatosis hepatis, arteriosclerosis | Kaletra, remdesivir, cortisone, Roactemra, 3 doses reconvalescent plasma | larynx, trachea |
| Case 6 | 78 | Male | COVID-19 pneumonia | Multi-organ failure | 28 | 25 | Did not regain consciousness after stop of narcotics, anisocoria, meningismus, tetraparesis | Arterial hypertension, atrial fibrillation | Pulmonary emphysema, arteriosclerosis, chronic kidney injury, prostate hyperplasia, hyperuricemia | Reconvalescent plasma, Roactemra, dialysis | trachea, larynx |
| Case 7 | 57 | Male | COVID-19 pneumonia | Respiratory failure | 5 | 0 | None | Arterial hypertension, obesity | Steatosis hepatis | None | naso-pharynx |
| Case 8 | 71 | Female | COVID-19 pneumonia | Multi-organ failure secondary to respiratory failure due to pneumonia | 10 | 4 | na | Arteriosclerosis | Myotonic dystrophy type 2, steatosis hepatis, asthma | Cortisone, remdesivir | naso-pharynx |
| Case 9 | 58 | Male | COVID-19 pneumonia | Sinus thrombosis | 26 | 7 | Seizures, coma | Chronic kidney failure, arteriosclerosis | Pulmonary emphysema | None | trachea, naso-pharynx |
| Case 10 | 80 | Male | COVID-19 pneumonia | Respiratory failure | 7 | 0 | Anxiety disorder, somnolence due to psychopharmaceuticals | Arterial hypertension, arteriosclerosis, acute on chronic kidney disease | Humerus fracture left arm | Ceftriaxone, hydroxychloroquine, zinc | na * |
| Case 11 | 80 | Female | COVID-19 pneumonia | Cardiorespiratory failure | 3 | 3 | None | Cardiac insufficiency (NYHA IV), diabetes, arterial hypertension, arteriosclerosis | - | None due to rapid cardiac deterioration | na * |
| Case 12 | 66 | Male | COVID-19 pneumonia | Multi-organ failure, hypoxic encephalopathy | 42 | 35 | Impaired consciousness of unknown origin, potentially due to hypoxic encephalopathy | Arterial hypertension, hypercholesterinemia | Status post transient ischemic attack 2014 | Cortisone, remdesivir; EBV, HSV and Aspergillus infection | na * |
| Case 13 | 54 | Male | COVID-19 pneumonia, mucormycosis with pulmonary infarction | Respiratory failure | 24 | 18 | None | Obesity, arterial hypertension, hypertrophic left ventricle | Myelodysplastic syndrome, secondary acute myeloid leukemia with chemotherapy and complete hematologic remission, bone marrow hypoplasia, signs of dysplastic hematopoiesis in the peripheral blood | Tocilizumab | na * |
| Case 14 | 96 | Female | Rib fractures, hemothorax, and COVID-19 pneumonia | Respiratory failure | na | na | na | Arterial hypertension, hypertensive cardiomyopathy, pulmonary hypertension | - | None | naso-pharynx |
| Case 15 | 71 | Male | COVID-19 pneumonia | Multi-organ failure secondary to respiratory failure due to pneumonia with interstitial fibrosis | 24 | 15 | Ageusia, agitation | Arterial hypertension | Arteriosclerosis, steatosis hepatis, cholecystolithiasis | Cortisone, remdesivir | trachea, naso-pharynx, bronchial |
| Case 16 | 56 | Female | COVID-19 pneumonia | Hemorrhagic shock after ECMO implantation | 15 | 12 | None | Diabetes, obesity | Status post thyroid carcinoma | Cortisone, remdesivir | naso-pharynx, trachea |
| Case 17 | 81 | Male | Unclear, postoperative multi-organ failure | Multi-organ failure | na | 1 | None | Intermittent atrial fibrillation | IPMN of the pancreas | None | na * |
| Case 18 | 73 | Male | COVID-19 pneumonia | Cardiogenic shock after ECMO implantation | 16 | 11 | None | Arterial hypertension, hypercholesterinemia | - | Cortisone, remdesivir | naso-pharynx, trachea |
| Case 19 | 63 | Female | COVID-19 pneumonia | Respiratory failure | 1 | 0 | None | Arterial hypertension, obesity, arteriosclerosis | Chronic venous insufficiency, steatosis hepatis | None | naso-pharynx |
| Case 20 | 65 | Male | COVID-19 pneumonia | Respiratory failure | 36 | 26 | Hemiparesis right side (onset 1 November 2021) | Obesity, sleep apnea syndrome, arterial hypertension, diabetes | Steatosis hepatis | Cortisone | naso-pharynx |
| Case 21 | 38 | Male | Not applicable (death at home) | Carbon monoxide poisoning | na | 0 | na | None | - | None | naso-pharynx post mortem |
| Case 22 | 33 | Male | Cardiac arrest | Cardiovascular failure | 7 | 0 | None | None | - | None | naso-pharynx |
| Case 23 | 71 | Male | COVID-19 pneumonia | Multi-organ failure | 71 | 57 | None/prolonged weaning | Diabetes, arterial hypertension, PAOD, hyperlipidemia | Status post TIA | Cortisone | naso-pharynx |
| Case 24 | 52 | Female | COVID-19 pneumonia | Cardiogenic shock due to myocarditis, death during new cannulation of ECMO | 12 | 5 | None | Obesity | Scleroderma | Cortisone | naso-pharynx |
| Case 25 | 64 | Male | Sepsis | Multi-organ failure | na | 34 | Coma, therapy-resistant status epilepticus | Arteriosclerosis, arterial hypertension, obesity, chronic kidney disease, hypercholesterinemia, nicotine abuse | Alcohol abuse, steatosis hepatis, chronic pancreatitis, pulmonary edema and congestion, hypothyroidism, hyperuricemia, pericarditis | None | naso-pharynx |
| Case 26 | 86 | Male | Cardiac arrest | Diffuse myocardial ischemia | na | 0 | Delirium | Arteriosclerosis, arterial hypertension | Prostate hyperplasia, status post meningioma resection left frontal lobe 9 days before death | Cortisone | naso-pharynx |
| Case 27 | 62 | Female | COVID-19 pneumonia | Respiratory failure | 14 | 4 | na | None | - | Cortisone | naso-pharynx |
| Case 28 | 82 | Female | Subdural hematoma | Subdural hematoma | 8 | 0 | Coma, anisocoria | Atrial fibrillation | Anxiety disorder | None | naso-pharynx |
| Case 29 | 67 | Female | Not applicable (death at home) | Cardiovascular failure | na | 0 | na | Arterial hypertension, atrial fibrillation | Chronic kidney failure | None | naso-pharynx post mortem |
| Case 30 | 49 | Male | Progressive stroke | Cardiovascular failure | 61 | 12 | Stroke with visual disturbance, gait disturbance, dysphagia, dysarthria, aphasia, agitation, reduced vigilance | Diabetes, arterial hypertension | Chronic kidney disease, schizoaffective disorder | Cortisone | naso-pharynx |
| Case 31 | 21 | Male | Myocardial infarction | Acute myocardial infarction | na | 0 | Epileptic seizure | Obesity | Purpura Schönlein–Henoch | None | naso-pharynx |
| Case 32 | 57 | Female | COVID-19 pneumonia | Cardiorespiratory failure | na | na | na | Arteriosclerosis | Invasive mammary carcinoma | na | na * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gelpi, E.; Klotz, S.; Beyerle, M.; Wischnewski, S.; Harter, V.; Kirschner, H.; Stolz, K.; Reisinger, C.; Lindeck-Pozza, E.; Zoufaly, A.; et al. Multifactorial White Matter Damage in the Acute Phase and Pre-Existing Conditions May Drive Cognitive Dysfunction after SARS-CoV-2 Infection: Neuropathology-Based Evidence. Viruses 2023, 15, 908. https://doi.org/10.3390/v15040908
Gelpi E, Klotz S, Beyerle M, Wischnewski S, Harter V, Kirschner H, Stolz K, Reisinger C, Lindeck-Pozza E, Zoufaly A, et al. Multifactorial White Matter Damage in the Acute Phase and Pre-Existing Conditions May Drive Cognitive Dysfunction after SARS-CoV-2 Infection: Neuropathology-Based Evidence. Viruses. 2023; 15(4):908. https://doi.org/10.3390/v15040908
Chicago/Turabian StyleGelpi, Ellen, Sigrid Klotz, Miriam Beyerle, Sven Wischnewski, Verena Harter, Harald Kirschner, Katharina Stolz, Christoph Reisinger, Elisabeth Lindeck-Pozza, Alexander Zoufaly, and et al. 2023. "Multifactorial White Matter Damage in the Acute Phase and Pre-Existing Conditions May Drive Cognitive Dysfunction after SARS-CoV-2 Infection: Neuropathology-Based Evidence" Viruses 15, no. 4: 908. https://doi.org/10.3390/v15040908