
Laboratory Evaluation and Field Testing of Dengue NS1 and IgM/IgG Rapid Diagnostic Tests in an Epidemic Context in Senegal

 , , , ,
, , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Laboratory Tests
2.2.1. qRT-PCR for the Detection of Dengue Virus
2.2.2. Platelia Dengue Bio-Rad NS1 ELISA Test
2.2.3. IgM Antibody Capture (MAC)-ELISA
2.2.4. Indirect IgG ELISA
2.2.5. Plaque Reduction Neutralisation Test
- (a)
- PRNT testing for ZIKV, WNV, and YFV
- (b)
- PRNT testing for DENV
Samples Description
- Samples used for Dengue NS1 RDT lab evaluation
- Samples used for Dengue IgM/IgG RDT lab evaluation
- ✓
- IgM RDT Evaluation Panel
- ✓ IgG RDT Evaluation Panel
- Samples used for field evaluation
2.2.6. Dengue Rapid Diagnostic Tests Used for Evaluation
- Specimen collection, transportation, and processing
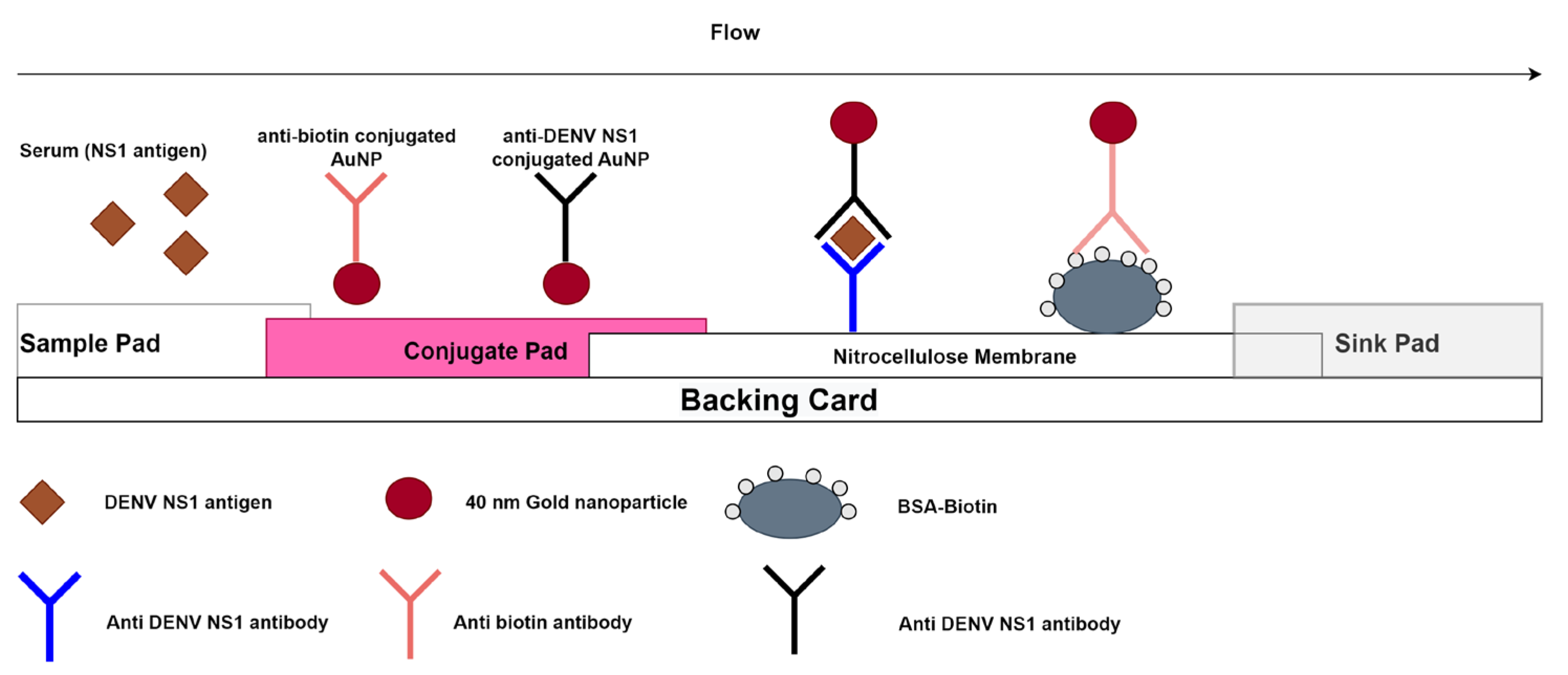
- Dengue NS1 Rapid Diagnostic Test
- ✓
- A red control line and NS1 test line indicate a positive result for DENV-NS1 antigen;
- ✓
- A red control line alone indicates a negative result for DENV-NS1 antigen;
- ✓
- Any result without a red control line is invalid.
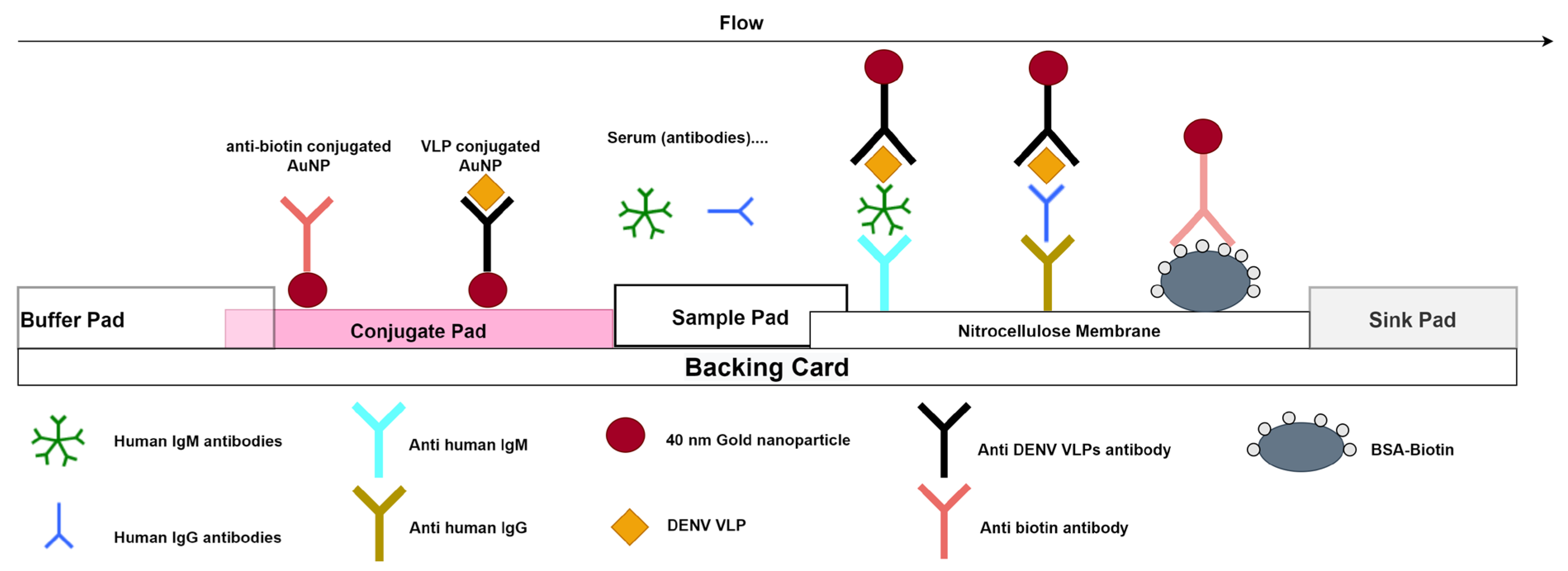
- Dengue IgM/IgG Rapid diagnostic test
- ✓
- A red control line and IgM test line indicate a positive result for anti-dengue IgM;
- ✓
- A red control line and IgG test line indicate a positive result for anti-dengue IgG;
- ✓
- A red control line and both test lines (IgM and IgG) indicated a positive result for both anti-dengue IgM and anti-dengue IgG;
- ✓
- A red control line alone indicates a negative result;
- ✓
- Any result without a red control line indicates an invalid test.
3. Results
3.1. Central Laboratory Evaluation Results
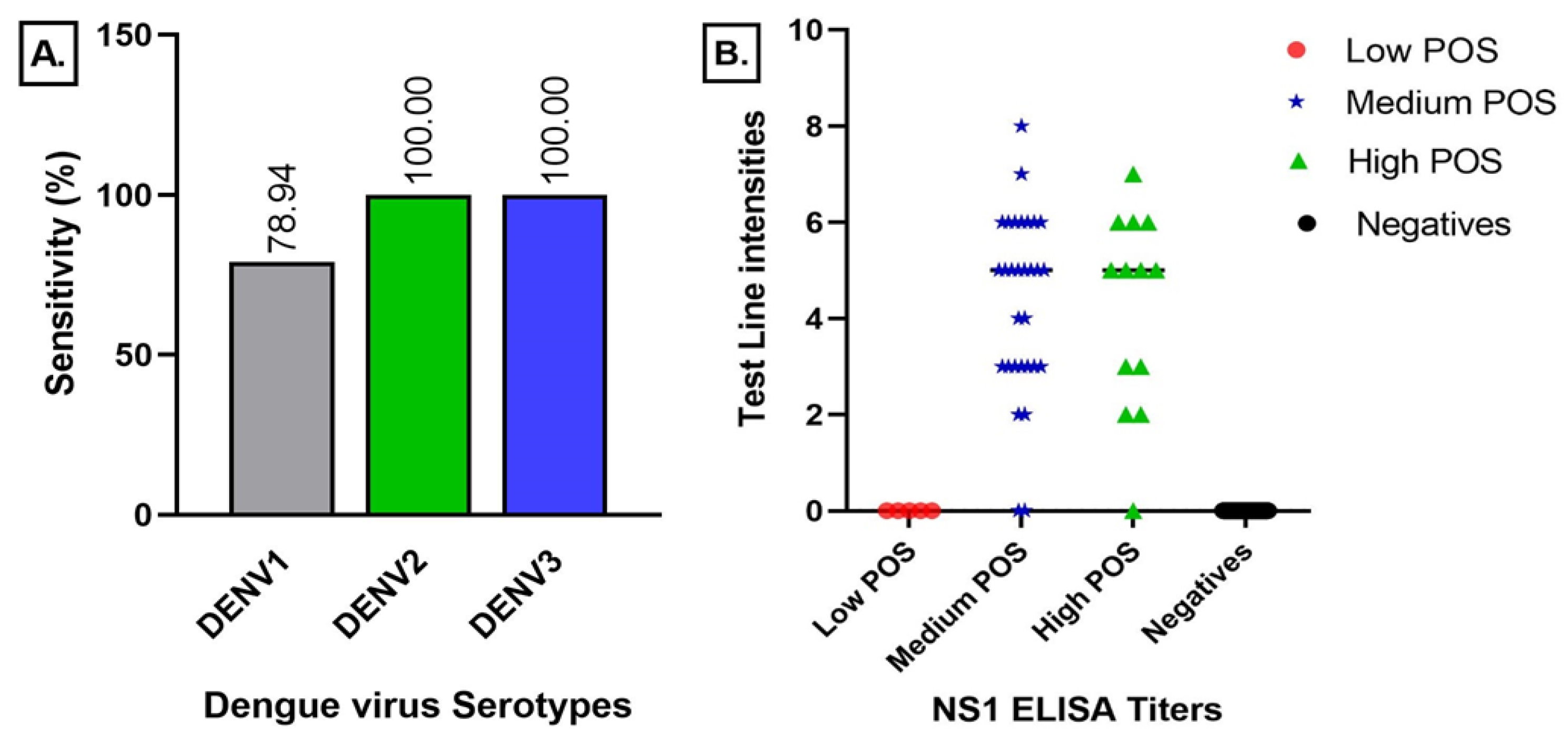
3.1.1. Dengue NS1 Lateral Flow Test Results
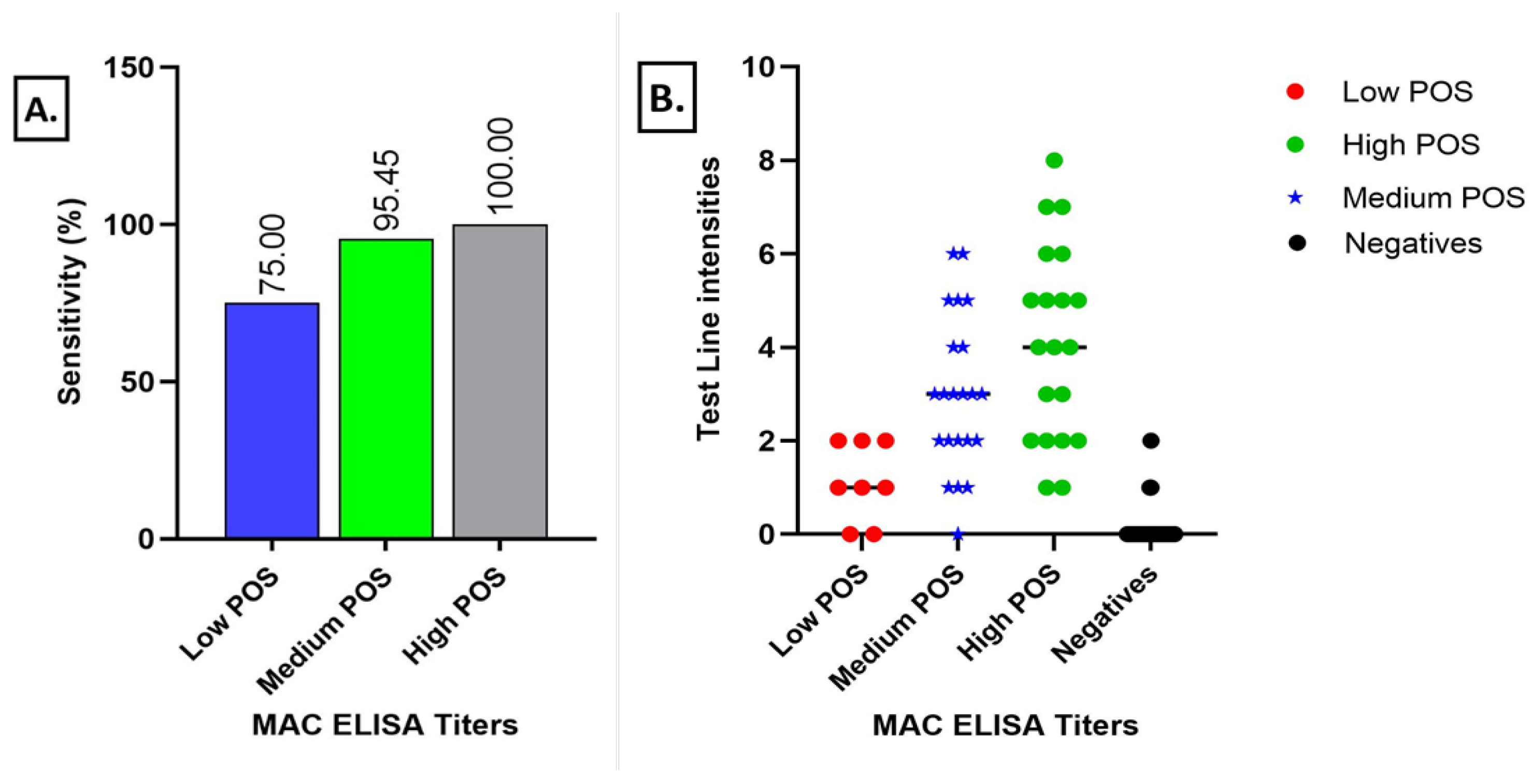
3.1.2. Dengue IgM Lateral Flow Test Results
3.1.3. Dengue IgG Lateral Flow Test Results
3.2. Field Evaluation Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hasan, S.; Jamdar, S.; Alalowi, M.; Al Ageel Al Beaiji, S. Dengue Virus: A Global Human Threat: Review of Literature. J. Int. Soc. Prevent. Communit. Dent. 2016, 6, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira-de-Lima, V.H.; Lima-Camara, T.N. Natural Vertical Transmission of Dengue Virus in Aedes Aegypti and Aedes Albopictus: A Systematic Review. Parasites Vectors 2018, 11, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishiura, H.; Halstead, S.B. Natural History of Dengue Virus (DENV)–1 and DENV-4 Infections: Reanalysis of Classic Studies. J. Infect. Dis. 2007, 195, 1007–1013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pull, L.; Brichler, S.; Bouchaud, O.; Siriez, J. Differential Diagnosis of Dengue Fever: Beware of Measles!: Table 1. J. Travel Med. 2012, 19, 268–271. [Google Scholar] [CrossRef]
- Simmons, C.P.; Farrar, J.J.; Nguyen, v.V.C.; Wills, B. Dengue. N. Engl. J. Med. 2012, 366, 1423–1432. [Google Scholar] [CrossRef]
- Kathiriya, D.J.; Patel, J.; Barad, D.; Shah, N.; Javia, B.; Tajpara, M.; Ghodasara, s.N. Epidemiological Surveillance of Dengue Fever: An Overview. Int. J. Vet. Sci. Amin. Hasb. 2020, 5, 1–10. [Google Scholar]
- Guo, C.; Zhou, Z.; Wen, Z.; Liu, Y.; Zeng, C.; Xiao, D.; Ou, M.; Han, Y.; Huang, S.; Liu, D.; et al. Global Epidemiology of Dengue Outbreaks in 1990–2015: A Systematic Review and Meta-Analysis. Front. Cell. Infect. Microbiol. 2017, 7, 317. [Google Scholar] [CrossRef] [Green Version]
- Yung, C.-F.; Lee, K.-S.; Thein, T.-L.; Tan, L.-K.; Gan, V.C.; Wong, J.G.X.; Lye, D.C.; Ng, L.-C.; Leo, Y.-S. Dengue Serotype-Specific Differences in Clinical Manifestation, Laboratory Parameters and Risk of Severe Disease in Adults, Singapore. Am. J. Trop. Med. Hyg. 2015, 92, 999–1005. [Google Scholar] [CrossRef]
- Khetarpal, N.; Khanna, I. Dengue Fever: Causes, Complications, and Vaccine Strategies. J. Immunol. Res. 2016, 2016, 6803098. [Google Scholar] [CrossRef] [Green Version]
- Normile, D. Tropical Medicine. Surprising New Dengue Virus Throws a Spanner in Disease Control Efforts. Science 2013, 342, 415. [Google Scholar] [CrossRef]
- Vaughn, D.W.; Green, S.; Kalayanarooj, S.; Innis, B.L.; Nimmannitya, S.; Suntayakorn, S.; Endy, T.P.; Raengsakulrach, B.; Rothman, A.L.; Ennis, F.A.; et al. Dengue Viremia Titer, Antibody Response Pattern, and Virus Serotype Correlate with Disease Severity. J. Infect. Dis. 2000, 181, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Halstead, S.B. Dengue Antibody-Dependent Enhancement: Knowns and Unknowns. Microbiol. Spectr. 2014, 2, 6. [Google Scholar] [CrossRef] [Green Version]
- Guzman, M.G.; Alvarez, M.; Halstead, S.B. Secondary Infection as a Risk Factor for Dengue Hemorrhagic Fever/Dengue Shock Syndrome: An Historical Perspective and Role of Antibody-Dependent Enhancement of Infection. Arch. Virol. 2013, 158, 1445–1459. [Google Scholar] [CrossRef]
- Robin, Y.; Cornet, M.; Heme, G.; Le Gonidec, G. Isolement du virus de la dengue au Sénégal. Ann. De L’institut Pasteur/Virol. 1980, 131, 149–154. [Google Scholar] [CrossRef]
- Saluzzo, J.F.; Cornet, M.; Castagnet, P. Isolation of Dengue 2 and Dengue 4 Viruses from Patients in Senegal. Trans. R. Soc. Trop. Med. Hyg. 1986, 80, 5. [Google Scholar] [CrossRef]
- Traore-Lamizana, M.; Zeller, H.; Monlun, E.; Mondo, M.; Hervy, J.; Adam, F.; Digoutte, J. Dengue 2 Outbreak in Southeastern Senegal during 1990: Virus Isolations from Mosquitoes (Diptera: Culicidae). J. Med. Entomol. 1994, 31, 623–627. [Google Scholar] [CrossRef]
- Faye, O.; Ba, Y.; Faye, O.; Talla, C.; Diallo, D.; Chen, R.; Mondo, M.; Ba, R.; Macondo, E.; Siby, T.; et al. Urban Epidemic of Dengue Virus Serotype 3 Infection, Senegal, 2009. Emerg. Infect. Dis. 2014, 20, 456–459. [Google Scholar] [CrossRef]
- Dieng, I.; dos Passos Cunha, M.; Diagne, M.M.; Sembène, P.M.; de Andrade Zanotto, P.M.; Faye, O.; Faye, O.; Sall, A.A. Origin and Spread of the Dengue Virus Type 1, Genotype V in Senegal, 2015–2019. Viruses 2021, 13, 57. [Google Scholar] [CrossRef]
- Diagne, C.T.; Barry, M.A.; Ba, Y.; Faye, O.; Sall, A.A. Dengue Epidemic in Touba, Senegal: Implications for the Grand Magal Pilgrimage for Travellers. J. Travel Med. 2019, 26, tay123. [Google Scholar] [CrossRef]
- Gaye, A.; Ndiaye, T.; Sy, M.; Deme, A.B.; Thiaw, A.B.; Sene, A.; Ndiaye, C.; Diedhiou, Y.; Mbaye, A.M.; Ndiaye, I.; et al. Genomic Investigation of a Dengue Virus Outbreak in Thiès, Senegal, in 2018. Sci. Rep. 2021, 11, 10321. [Google Scholar] [CrossRef]
- Burke, D.S.; Kliks, S. Antibody-Dependent Enhancement in Dengue Virus Infections. J. Infect. Dis. 2006, 193, 601–603. [Google Scholar] [CrossRef]
- Wiwanitkit, V. Dengue Fever: Diagnosis and Treatment. Expert Rev. Anti-Infect. Ther. 2010, 8, 841–845. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for South-East Asia. Comprehensive Guideline for Prevention and Control of Dengue and Dengue Haemorrhagic Fever. Revised and Expanded Edition; WHO Regional Office for South-East Asia: New Delhi, India, 2011; ISBN 978-92-9022-387-0. [Google Scholar]
- Durbin, A.P.; Whitehead, S.S. Dengue Vaccine Candidates in Development. Curr. Top. Microbiol. Immunol. 2010, 338, 129–143. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Tissera, H.; AbuBakar, S.; Kittayapong, P.; Logan, J.; Neumayr, A.; Rocklöv, J.; Byass, P.; Louis, V.R.; Tozan, Y.; et al. Novel Tools for the Surveillance and Control of Dengue: Findings by the DengueTools Research Consortium. Glob. Health Action 2018, 11, 1549930. [Google Scholar] [CrossRef] [Green Version]
- Peeling, R.W.; Artsob, H.; Pelegrino, J.L.; Buchy, P.; Cardosa, M.J.; Devi, S.; Enria, D.A.; Farrar, J.; Gubler, D.J.; Guzman, M.G.; et al. Evaluation of Diagnostic Tests: Dengue. Nat. Rev. Microbiol. 2010, 8, S30–S38. [Google Scholar] [CrossRef]
- Magnitude of Antibody Cross-Reactivity in Medically Important Mosquito-Borne Flaviviruses: A Systematic Review. Available online: https://www.tandfonline.com/doi/epdf/10.2147/IDR.S336351?needAccess=true&role=button (accessed on 26 December 2021).
- Hunsperger, E.A.; Yoksan, S.; Buchy, P.; Nguyen, V.C.; Sekaran, S.D.; Enria, D.A.; Pelegrino, J.L.; Vázquez, S.; Artsob, H.; Drebot, M.; et al. Evaluation of Commercially Available Anti–Dengue Virus Immunoglobulin M Tests. Emerg. Infect. Dis. 2009, 15, 436–439. [Google Scholar] [CrossRef]
- Muller, D.A.; Depelsenaire, A.C.I.; Young, P.R. Clinical and Laboratory Diagnosis of Dengue Virus Infection. J. Infect. Dis. 2017, 215, S89–S95. [Google Scholar] [CrossRef]
- Yamada, K.-I.; Takasaki, T.; Nawa, M.; Kurane, I. Virus Isolation as One of the Diagnostic Methods for Dengue Virus Infection. J. Clin. Virol. 2002, 24, 203–209. [Google Scholar] [CrossRef]
- Kumaria, R.; Chakravarti, A. Molecular Detection and Serotypic Characterization of Dengue Viruses by Single-Tube Multiplex Reverse Transcriptase-Polymerase Chain Reaction. Diagn. Microbiol. Infect. Dis. 2005, 52, 311–316. [Google Scholar] [CrossRef]
- Kumarasamy, V.; Wahab, A.H.A.; Chua, S.K.; Hassan, Z.; Chem, Y.K.; Mohamad, M.; Chua, K.B. Evaluation of a Commercial Dengue NS1 Antigen-Capture ELISA for Laboratory Diagnosis of Acute Dengue Virus Infection. J. Virol. Methods 2007, 140, 75–79. [Google Scholar] [CrossRef]
- Scaramozzino, N.; Crance, J.-M.; Jouan, A.; DeBriel, D.A.; Stoll, F.; Garin, D. Comparison of Flavivirus Universal Primer Pairs and Development of a Rapid, Highly Sensitive Heminested Reverse Transcription-PCR Assay for Detection of Flaviviruses Targeted to a Conserved Region of the NS5 Gene Sequences. J. Clin. Microbiol. 2001, 39, 1922–1927. [Google Scholar] [CrossRef] [Green Version]
- Martin, D.A.; Muth, D.A.; Brown, T.; Johnson, A.J.; Karabatsos, N.; Roehrig, J.T. Standardization of Immunoglobulin M Capture Enzyme-Linked Immunosorbent Assays for Routine Diagnosis of Arboviral Infections. J. Clin. Microbiol. 2000, 38, 1823–1826. [Google Scholar] [CrossRef] [Green Version]
- Emmerich, P.; Mika, A.; von Possel, R.; Rackow, A.; Liu, Y.; Schmitz, H.; Günther, S.; Sherifi, K.; Halili, B.; Jakupi, X.; et al. Sensitive and Specific Detection of Crimean-Congo Hemorrhagic Fever Virus (CCHFV)—Specific IgM and IgG Antibodies in Human Sera Using Recombinant CCHFV Nucleoprotein as Antigen in μ-Capture and IgG Immune Complex (IC) ELISA Tests. PLoS Negl. Trop. Dis. 2018, 12, e0006366. [Google Scholar] [CrossRef] [Green Version]
- Jelinek, T.; Wastlhuber, J.; Pröll, S.; Schattenkirchner, M.; Löscher, T. Influence of Rheumatoid Factor on the Specificity of a Rapid Immunochromatographic Test for Diagnosing Dengue Infection. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 555–556. [Google Scholar] [CrossRef]
- Laureti, M.; Narayanan, D.; Rodriguez-Andres, J.; Fazakerley, J.K.; Kedzierski, L. Flavivirus Receptors: Diversity, Identity, and Cell Entry. Front. Immunol. 2018, 9, 2180. [Google Scholar] [CrossRef] [Green Version]
- Chappuis, F.; Alirol, E.; d’Acremont, V.; Bottieau, E.; Yansouni, C.P. Rapid Diagnostic Tests for Non-Malarial Febrile Illness in the Tropics. Clin. Microbiol. Infect. 2013, 19, 422–431. [Google Scholar] [CrossRef] [Green Version]
- Babaliche, P.; Doshi, D. Catching Dengue Early: Clinical Features and Laboratory Markers of Dengue Virus Infection. J. Assoc. Physicians India 2015, 63, 38–41. [Google Scholar]
- Shu, P.-Y.; Huang, J.-H. Current Advances in Dengue Diagnosis. Clin. Vaccine Immunol. 2004, 11, 642–650. [Google Scholar] [CrossRef] [Green Version]
- Larremore, D.B.; Wilder, B.; Lester, E.; Shehata, S.; Burke, J.M.; Hay, J.A.; Tambe, M.; Mina, M.J.; Parker, R. Test Sensitivity Is Secondary to Frequency and Turnaround Time for COVID-19 Screening. Sci. Adv. 2021, 7, eabd5393. [Google Scholar] [CrossRef]
- Jang, W.S.; Kwak, S.Y.; May, W.L.; Yang, D.J.; Nam, J.; Lim, C.S. Comparative Evaluation of Three Dengue Duo Rapid Test Kits to Detect NS1, IgM, and IgG Associated with Acute Dengue in Children in Myanmar. PLoS ONE 2019, 14, e0213451. [Google Scholar] [CrossRef]
- Blacksell, S.D.; Jarman, R.G.; Bailey, M.S.; Tanganuchitcharnchai, A.; Jenjaroen, K.; Gibbons, R.V.; Paris, D.H.; Premaratna, R.; de Silva, H.J.; Lalloo, D.G.; et al. Evaluation of Six Commercial Point-of-Care Tests for Diagnosis of Acute Dengue Infections: The Need for Combining NS1 Antigen and IgM/IgG Antibody Detection To Achieve Acceptable Levels of Accuracy. Clin. Vaccine Immunol. 2011, 18, 2095–2101. [Google Scholar] [CrossRef] [Green Version]
- Chatchen, S.; Sabchareon, A.; Sirivichayakul, C. Serodiagnosis of Asymptomatic Dengue Infection. Asian Pac. J. Trop. Med. 2017, 10, 11–14. [Google Scholar] [CrossRef]
- Vilibic-Cavlek, T.; Kristofic, B.; Savic, V.; Kolaric, B.; Barbic, L.; Tabain, I.; Peric, L.; Sabadi, D.; Miklausic, B.; Potocnik-Hunjadi, T.; et al. Diagnostic Significance of Immunoglobulin G Avidity in Symptomatic and Asymptomatic West Nile Virus Infection. Rev. Soc. Bras. Med. Trop. 2018, 51, 591–595. [Google Scholar] [CrossRef]
- Makino, Y.; Tadano, M.; Saito, M.; Maneekarn, N.; Sittisombut, N.; Sirisanthana, V.; Poneprasert, B.; Fukunaga, T. Studies on Serological Cross-Reaction in Sequential Flavivirus Infections. Microbiol. Immunol. 1994, 38, 951–955. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dengue NS1 Sensitivity Panel | Dengue NS1 Specificity Panel | ||
|---|---|---|---|
| Serotype | n= | Related flaviviruses | n= |
| DENV1 natural infection | 38 | YFV spiked samples | 25 |
| DENV2 natural infection | 7 | ZIKV spiked samples | 20 |
| DENV3 natural infection | 3 | WNV spiked samples | 19 |
| TOTAL | 48 | Other Febrile illnesses | |
| CHIKV spiked samples | 20 | ||
| P. falciparum positive samples | 34 | ||
| Healthy donor samples | |||
| NEG all * | 10 | ||
| TOTAL | 128 * | ||
| Dengue IgM Sensitivity Panel | Dengue IgM Specificity Panel | ||
|---|---|---|---|
| DENV MAC ELISA Titre | n= | Related flaviviruses | n= |
| High POS | 20 | IgM YFV | 41 |
| Medium POS | 22 | IgM ZIKV | 20 |
| Low POS | 8 | Other Febrile illnesses | |
| TOTAL | 50 | Malaria positive | 20 |
| Interfering Conditions | |||
| Rheumatoid Factor+ | 6 | ||
| Healthy donor samples | |||
| NEG all * | 50 | ||
| TOTAL | 137 | ||
| Dengue IgG Sensitivity Panel | Dengue IgG Specificity Panel | ||
| Serum description | n= | Serum description | n= |
| Healthy donor samples IgG POS | 39 | Other Febrile illnesses | |
| Convalescent IgG POS | 50 | Malaria PCR positive | 6 |
| Interfering Conditions | |||
| TOTAL | 89 | Rheumatoid Factor+ | 6 |
| Healthy donor samples | |||
| NEG all * | 50 | ||
| Related flaviviruses | |||
| IgG YFV | 10 | ||
| IgG ZIKV | 10 | ||
| TOTAL | 82 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndiaye, O.; Woolston, K.; Gaye, A.; Loucoubar, C.; Cocozza, M.; Fall, C.; Dia, F.; Adams, E.R.; Samb, M.; Camara, D.; et al. Laboratory Evaluation and Field Testing of Dengue NS1 and IgM/IgG Rapid Diagnostic Tests in an Epidemic Context in Senegal. Viruses 2023, 15, 904. https://doi.org/10.3390/v15040904
Ndiaye O, Woolston K, Gaye A, Loucoubar C, Cocozza M, Fall C, Dia F, Adams ER, Samb M, Camara D, et al. Laboratory Evaluation and Field Testing of Dengue NS1 and IgM/IgG Rapid Diagnostic Tests in an Epidemic Context in Senegal. Viruses. 2023; 15(4):904. https://doi.org/10.3390/v15040904
Chicago/Turabian StyleNdiaye, Oumar, Kevin Woolston, Aboubacry Gaye, Cheikh Loucoubar, Michael Cocozza, Cheikh Fall, Fatou Dia, Emily R. Adams, Marième Samb, Diogop Camara, and et al. 2023. "Laboratory Evaluation and Field Testing of Dengue NS1 and IgM/IgG Rapid Diagnostic Tests in an Epidemic Context in Senegal" Viruses 15, no. 4: 904. https://doi.org/10.3390/v15040904