
Hantavirus Infection in Children—A Pilot Study of Single Regional Center
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Epidemiological Study
2.2. Serological Diagnostic
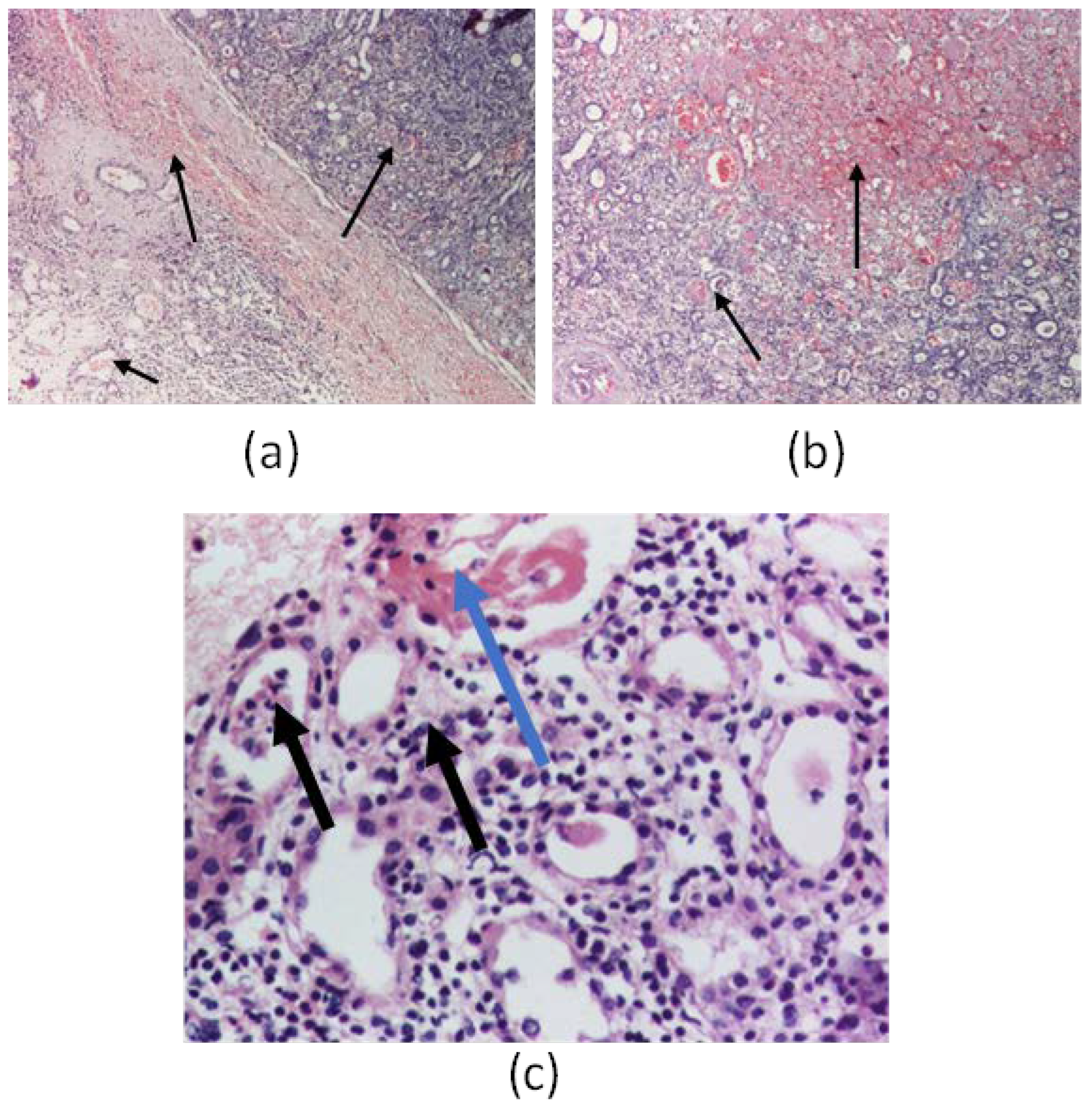
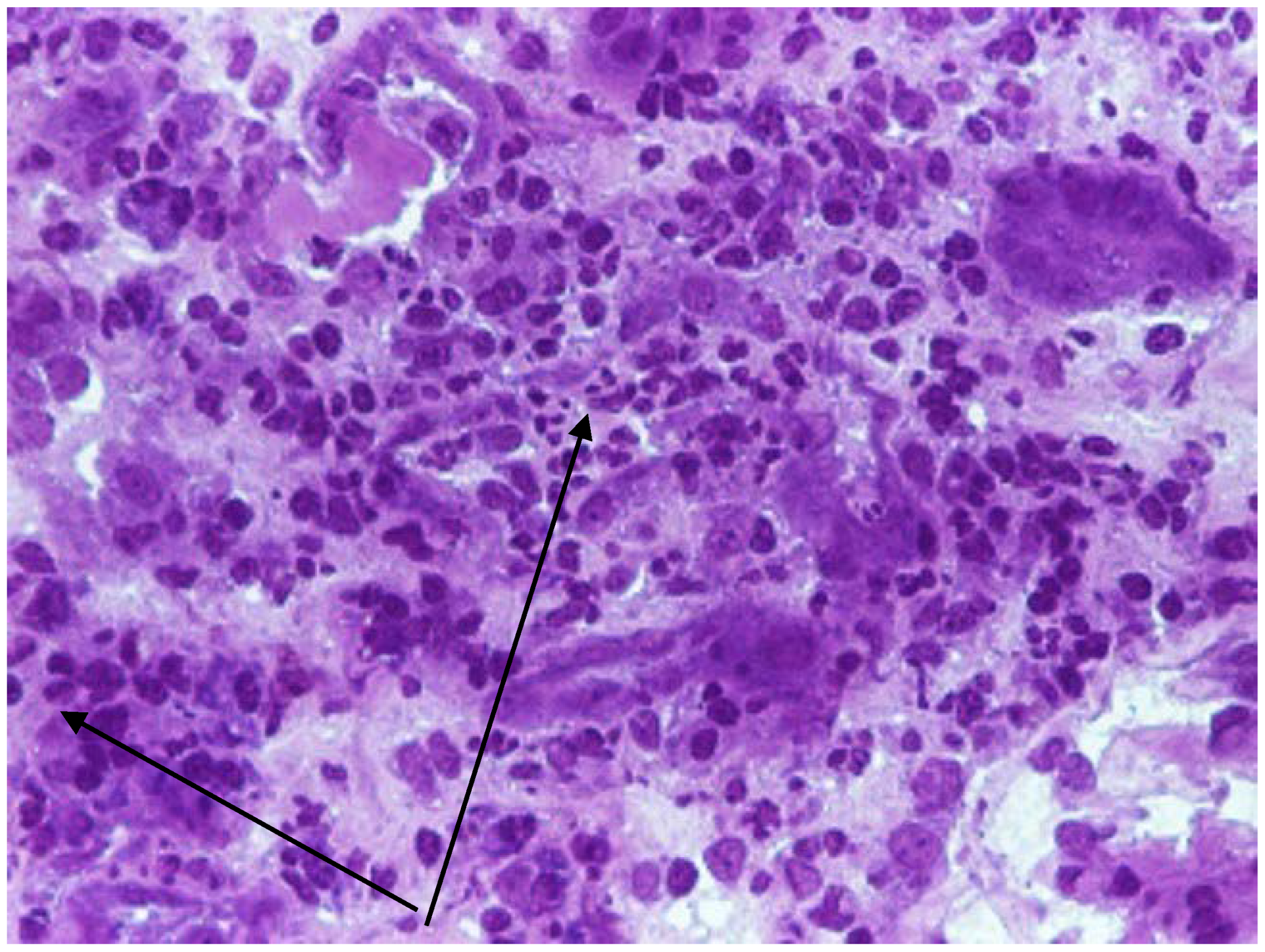
2.3. Kidney Biopsy
3. Results
4. Discussion
4.1. Epidemiology of Hantavirus Infection
4.2. Pathological Features of the Disease
4.3. Clinicals Features of the Disease
4.4. Biological Features in the Disease
4.5. Clinical-Evolutive Aspects in Children Hantavirosis
4.6. Differential Diagnosis
4.7. Evolutive and Therapeutic Features in the Disease
4.8. Prevention of the Disease
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teng, A.-Y.; Che, T.-L.; Zhang, A.-R.; Zhang, Y.-Y.; Xu, Q.; Wang, T.; Sun, Y.-Q.; Jiang, B.-G.; Lv, C.-L.; Chen, J.-J.; et al. Mapping the viruses belonging to the order Bunyavirales in China. Infect. Dis. Poverty 2022, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- Plyusnin, A.; Beaty, B.J.; Elliott, R.M.; Goldbach, R.; Kormelink, R.; Lundkvist, Å.; Schmaljohn, C.S.; Teshet, R.B. Family Bunyaviridae. In Virus Taxonomy; King, A.M.Q., Adams, M.J., Carstens, E.B., Lefkowitz, E.J., Eds.; Ninth Report of the International Committee on Taxonomy of Viruses; Elsevier/Academic Press: London, UK, 2011; pp. 725–741. [Google Scholar]
- Laenen, L.; Vergote, V.; Calisher, C.H.; Klempa, B.; Klingström, J.; Kuhn, J.H.; Maes, P. Hantaviridae: Current Classification and Future Perspectives. Viruses 2019, 11, 788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abudurexiti, A.; Adkins, S.; Alioto, D.; Alkhovsky, S.V.; Avšič-Županc, T.; Ballinger, M.J.; Bente, D.A.; Beer, M.; Bergeron, É.; Blair, C.D.; et al. Taxonomy of the order Bunyavirales: Update 2019. Arch. Virol. 2019, 164, 1949–1965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, H.; Hu, S.; Cazelles, B.; Chowell, G.; Gao, L.; Laine, M.; Li, Y.; Yang, H.; Li, Y.; Yang, Q.; et al. Urbanization prolongs hantavirus epidemics in cities. Proc. Natl. Acad. Sci. USA 2018, 115, 4707–4712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, H.; Yu, P.; Bjørnstad, O.N.; Cazelles, B.; Yang, J.; Tan, H.; Huang, S.; Cui, Y.; Dong, L.; Ma, C.; et al. Anthropogenically driven environmental changes shift the ecological dynamics of hemorrhagic fever with renal syndrome. PLoS Pathog. 2017, 13, e1006198. [Google Scholar] [CrossRef] [Green Version]
- Bloom, D.E.; Cadarette, D. Infectious Disease Threats in the Twenty-First Century: Strengthening the Global Response. Front. Immunol. 2019, 10, 549. [Google Scholar] [CrossRef] [Green Version]
- Viral Hemorrhagic Fevers (VHFs): Bunyavirales. Available online: https://www.cdc.gov/vhf/virus-families/bunyaviridae.html (accessed on 23 March 2023).
- Rabiee, M.H.; Mahmoudi, A.; Siahsarvie, R.; Kryštufek, B.; Mostafavi, E. Rodent-borne diseases and their public health importance in Iran. PLOS Neglected Trop. Dis. 2018, 12, e0006256. [Google Scholar] [CrossRef] [Green Version]
- Mir, M.A. Hantaviruses. Clin. Lab. Med. 2010, 30, 67–91. [Google Scholar] [CrossRef]
- Cherry, J.D.; Harrison, G.J.; Kaplan, S.L.; Hotez, P.J.; Steinbach, W.J. “Hantaviruses.” Essay. In Feigin and Cherry’s Textbook of Pediatric Infectious Diseases, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 1854–1865. [Google Scholar]
- Zhang, R.; Mao, Z.; Yang, J.; Liu, S.; Liu, Y.; Qin, S.; Tian, H.; Guo, S.; Ren, J.; Shi, X.; et al. The changing epidemiology of hemorrhagic fever with renal syndrome in Southeastern China during 1963–2020: A retrospective analysis of surveillance data. PLoS Neglected Trop. Dis. 2021, 15, e0009673. [Google Scholar] [CrossRef]
- WHO. Hemorrhagic Fever with Renal Syndrome; WHO: Geneva, Switzerland, 2021; Available online: https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccine-standardization/hfrs (accessed on 23 March 2023).
- Tariq, M.; Kim, D.-M. Hemorrhagic Fever with Renal Syndrome: Literature Review, Epidemiology, Clinical Picture and Pathogenesis. Infect. Chemother. 2022, 54, 1–19. [Google Scholar] [CrossRef]
- Armstrong, L.R.; Bryan, R.T.; Sarisky, J.; Khan, A.S.; Rowe, T.; Ettestad, P.J.; Cheek, J.E.; Peters, C.J.; Rollin, P.; Martin, M.L.; et al. Mild Hantaviral Disease Caused by Sin Nombre Virus in a Four-Year-Old Child. Pediatr. Infect. Dis. J. 1995, 14, 1108–1109. [Google Scholar] [CrossRef] [PubMed]
- Terças-Trettel, A.C.P.; Melo, A.V.G.; Bonilha, S.M.F.; Moraes, J.M.; Oliveira, R.C.; Guterres, A.; Fernandes, J.; Atanaka, M.; Espinosa, M.M.; Sampaio, L.; et al. Hantavirus pulmonary syndrome in children: Case report and case series from an endemic area of Brazil. Rev. Inst. Med. Trop. Sao Paulo 2019, 61, e65. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Hantavirus infection. In ECDC; Annual Epidemiological Report for 2018; Hantavirus, AER for 2018 (europa.eu); ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Kim, W.-K.; Kim, J.-A.; Song, D.H.; Lee, D.; Kim, Y.C.; Lee, S.-Y.; Lee, S.-H.; No, J.S.; Kim, J.H.; Kho, J.H.; et al. Phylogeographic analysis of hemorrhagic fever with renal syndrome patients using multiplex PCR-based next generation sequencing. Sci. Rep. 2016, 6, 26017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noh, J.Y.; Jung, J.; Song, J.W. Hemorrhagic fever with renal syndrome. Infect. Chemother. 2019, 51, 405–413. [Google Scholar] [CrossRef]
- Zeier, M.; Handermann, M.; Bahr, U.; Rensch, B.; Kehm, R.; Muranyi, W.; Darai, G. New Ecological Aspects of Hantavirus Infection: A Change of a Paradigm and a Challenge of Prevention—A Review. Virus Genes 2005, 30, 157–180. [Google Scholar] [CrossRef]
- Muñoz-Zanzi, C.; Saavedra, F.; Otth, C.; Domancich, L.; Hott, M.; Padula, P. Serological Evidence of Hantavirus Infection in Apparently Healthy People from Rural and Slum Communities in Southern Chile. Viruses 2015, 7, 2006–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Valdebenito, C.; Calvo, M.; Vial, C.; Mansilla, R.; Marco, C.; Palma, R.E.; Vial, P.A.; Valdivieso, F.; Mertz, G.; Ferrés, M. Person-to-Person Household and Nosocomial Transmission of Andes Hantavirus, Southern Chile, 2011. Emerg. Infect. Dis. 2014, 20, 1629–1636. [Google Scholar] [CrossRef]
- Pettersson, L.; Klingström, J.; Hardestam, J.; Lundkvist, A.; Ahlm, C.; Evander, M. Hantavirus RNA in Saliva from Patients with Hemorrhagic Fever with Renal Syndrome. Emerg. Infect. Dis. 2008, 14, 406–411. [Google Scholar] [CrossRef]
- Cabinian, A.; Sinsimer, D.; Tang, M.; Zumba, O.; Mehta, H.; Toma, A.; Sant’Angelo, D.; Laouar, Y.; Laouar, A. Transfer of Maternal Immune Cells by Breastfeeding: Maternal Cytotoxic T Lymphocytes Present in Breast Milk Localize in the Peyer’s Patches of the Nursed Infant. PLoS ONE 2016, 11, e0156762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrés, M.; Martínez-Valdebenito, C.; Angulo, J.; Henríquez, C.; Vera-Otárola, J.; Vergara, M.J.; Pérez, J.; Fernández, J.; Sotomayor, V.; Valdés, M.F.; et al. Mother-to-Child Transmission of Andes Virus through Breast Milk, Chile1. Emerg. Infect. Dis. 2020, 26, 1885–1888. [Google Scholar] [CrossRef]
- Hantavirus Infection—Annual Epidemiological Report for 2019. European Centre for Disease Prevention and Control, 22 April 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/hantavirus-infection-annual-epidemiological-report-2019 (accessed on 23 March 2023).
- Fidan, K.; Polat, M.; Isıyel, E.; Kalkan, G.; Tezer, H.; Söylemezoğlu, O. An Adolescent Boy with Acute Kidney Injury and Fever: Answers. Pediatr. Nephrol. 2012, 28, 2115–2116. [Google Scholar] [CrossRef]
- Maftei, I.-D.; Segall, L.; Panculescu-Gatej, R.; Ceianu, C.; Covic, A. Hantavirus Infection—Hemorrhagic Fever with Renal Syndrome: The First Case Series Reported in Romania and Review of the Literature. Int. Urol. Nephrol. 2011, 44, 1185–1191. [Google Scholar] [CrossRef]
- Županc, T.A.; Korva, M.; Markotić, A. HFRS and Hantaviruses in the Balkans/South-East Europe. Virus Res. 2014, 187, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metodologie de Supraveghere a Infectiei cu Hantavirusuri 2012. Available online: https://www.cnscbt.ro/index.php/metodologii/infectia-cu-hantavirus/476-metodologie-de-supraveghere-a-infectiei-cu-hantavirusuri-2012 (accessed on 23 March 2023).
- Koskela, S.; Mäkelä, S.; Strandin, T.; Vaheri, A.; Outinen, T.; Joutsi-Korhonen, L.; Pörsti, I.; Mustonen, J.; Laine, O. Coagulopathy in Acute Puumala Hantavirus Infection. Viruses 2021, 13, 1553. [Google Scholar] [CrossRef]
- Klingström, J.; Smed-Sörensen, A.; Maleki, K.T.; Solà-Riera, C.; Ahlm, C.; Björkström, N.K.; Ljunggren, H.G. Innate and adaptive immune re-sponses against human Puumala virus infection: Immunopathogenesis and suggestions for novel treatment strategies for severe hantavirus-associated syndromes. J. Intern. Med. 2019, 285, 510–523. [Google Scholar] [CrossRef] [Green Version]
- Jost, S.; Altfeld, M. Control of human viral infections by natural killer cells. Annu. Rev. Immunol. 2013, 31, 163–194. [Google Scholar] [CrossRef]
- Noor, R. General awareness on hantavirus infection: A brief review. Biomed. Biotechnol. Res. J. (BBRJ) 2020, 4, 274. [Google Scholar] [CrossRef]
- Khaiboullina, S.F.; Levis, S.; Morzunov, S.P.; Martynova, E.V.; Anokhin, V.A.; Gusev, O.A.; Jeor, S.C.S.; Lombardi, V.C.; Rizvanov, A.A. Serum Cytokine Profiles Differentiating Hemorrhagic Fever with Renal Syndrome and Hantavirus Pulmonary Syndrome. Front. Immunol. 2017, 8, 567. [Google Scholar] [CrossRef] [Green Version]
- Mustonen, J.; Outinen, T.; Laine, O.; Pörsti, I.; Vaheri, A.; Mäkelä, S. Kidney disease in Puumala hantavirus infection. Inf. Dis. 2017, 49, 321–332. [Google Scholar] [CrossRef]
- Caramello, P.; Canta, F.; Bonino, L.; Moiraghi, C.; Navone, F.; Lipani, F.; Balbiano, R.; Caputo, A.M.; Gai, V. Puumala Virus Pulmonary Syndrome in a Romanian Immigrant. J. Travel Med. 2006, 9, 326–329. [Google Scholar] [CrossRef]
- Echterdiek, F.; Kitterer, D.; Alscher, M.D.; Schwenger, V.; Ruckenbrod, B.; Bald, M.; Latus, J. Clinical course of hantavirus-induced nephropathia epidemica in children compared to adults in Germany—Analysis of 317 patients. Pediatr. Nephrol. 2019, 34, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Lupuşoru, G.; Lupuşoru, M.; Ailincăi, I.; Bernea, L.; Berechet, A.; Spătaru, R.; Ismail, G. Hanta Hemorrhagic Fever with Renal Syndrome: A Pathology in Whose Diagnosis Kidney Biopsy Plays a Major Role (Review). Exp. Ther. Med. 2021, 22, 984. [Google Scholar] [CrossRef]
- Huttunen, N.-P.; Mäkelä, S.; Pokka, T.; Mustonen, J.; Uhari, M. Systematic literature review of symptoms, signs and severity of serologically confirmed nephropathia epidemica in paediatric and adult patients. Scand. J. Infect. Dis. 2011, 43, 405–410. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Sun, J.; Chen, Y.; Fan, X.; Wang, X.; Zhang, X.; Zhang, K.; Han, Q.; Liu, Z. Clinical and laboratory features and factors predicting disease severity in pediatric patients with hemorrhagic fever with renal syndrome caused by Hantaan virus. J. Med Virol. 2022, 95, e28339. [Google Scholar] [CrossRef] [PubMed]
- Mäkelä, S.; Mustonen, J.; Ala-Houhala, I.; Hurme, M.; Koivisto, A.-M.; Vaheri, A.; Pasternack, A. Urinary excretion of interleukin-6 correlates with proteinuria in acute Puumala hantavirus-induced nephritis. Am. J. Kidney. Dis. 2004, 43, 809–816. [Google Scholar] [CrossRef]
- ietäväinen, J.; Mantula, P.; Outinen, T.; Huhtala, H.; Pörsti, I.H.; Niemelä, O.; Vaheri, A.; Mäkelä, S.; Mustonen, J. Glucosuria Predicts the Severity of Puumala Hantavirus Infection. Kidney Int. Rep. 2019, 4, 1296–1303. [Google Scholar] [CrossRef] [Green Version]
- Vaheri, A.; Henttonen, H.; Mustonen, J. Hantavirus Research in Finland: Highlights and Perspectives. Viruses 2021, 13, 1452. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Hantaviruses in Agricultural and Forestry Workers: Knowledge, Attitudes and Practices in Italian Physicians. Trop. Med. Infect. Dis. 2021, 6, 169. [Google Scholar] [CrossRef]
- de Oliveira, S.V.; Faccini-Martínez, Á.A. Hantavirus Infection and the Renal Syndrome. Trop. Nephrol. 2020, 2020, 175–192. [Google Scholar]
- Panculescu-Gatej, R.I.; Sirbu, A.; Dinu, S.; Waldstrom, M.; Heyman, P.; Murariu, D.; Petrescu, A.; Szmal, C.; Oprisan, G.; Lundkvist, Å.; et al. Dobrava Virus Carried by the Yellow-Necked Field Mouse Apodemus Flavicollis, Causing Hemorrhagic Fever with Renal Syndrome in Romania. Vector-Borne Zoonotic Dis. 2014, 14, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Dheerasekara, K.; Sumathipala, S.; Muthugala, R. Hantavirus Infections—Treatment and Prevention. Curr. Treat. Options Infect. Dis. 2020, 12, 410–421. [Google Scholar] [CrossRef] [PubMed]
- Malinin, O.; Platonov, A. Insufficient efficacy and safety of intravenous ribavirin in treatment of haemorrhagic fever with renal syndrome caused by Puumala virus. Infect. Dis. 2017, 49, 514–520. [Google Scholar] [CrossRef]
- Avsic-Zupanc, T.; Saksida, A.; Korva, M. Hantavirus infections. Clin. Microbiol. Infect. 2019, 21S, e6–e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saavedra, F.; Díaz, F.E.; Retamal-Díaz, A.; Covián, C.; González, P.A.; Kalergis, A.M. Immune response during hantavirus diseases: Implications for immunotherapies and vaccine design. Immunology 2021, 163, 262–277. [Google Scholar] [CrossRef]
- Koehler, F.C.; Di Cristanziano, V.; Späth, M.R.; Hoyer-Allo, J.; Wanken, M.; Müller, R.U.; Burst, V. The kidney in hantavirus infection—Epidemiology, virology, pathophysiology, clinical presentation, diagnosis and management. Clin. Kidney J. 2022, 15, 1231–1252. [Google Scholar] [CrossRef]
- WHO. Hantavirus Pulmonary Syndrome. Emergence Preparedness Response. Hantavirus Pulmonary Syndrome—Argentine Republic. 2019. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/23-January-2019-hantavirus-argentina-en (accessed on 23 March 2023).
- Douglas, K.O.; Payne, K.; Sabino-Santos, G., Jr.; Agard, J. Influence of Climatic Factors on Human Hantavirus Infections in Latin America and the Caribbean: A Systematic Review. Pathogens 2022, 11, 15. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients | Age, Month and Year at Admission | Baseline Characteristics | n = 8 | Biological Findings | n = 8 |
|---|---|---|---|---|---|
| Patient 1 | 16 y.o. | Gender | CBC | ||
| November 2017 | Female | 0 | Mild anemia | 1 | |
| Patient 2 | 16 y.o. | Male | 8 | Leukocytosis | 2 |
| October 2021 | Residence | Thrombocytopenia | 6 | ||
| Patient 3 | 18 y.o. | Rural | 7 | Inflammatory markers | |
| October 2018 | Urban | 1 | CRP > 10 mg/dL | 8 | |
| Patient 4 | 16 y.o. | Symptoms | ESR > 15 mm/1 h | 5 | |
| May 2020 | Vomiting | 8 | Hepatic cytolysis | 6 | |
| Patient 5 | 16 y.o. | Abdominal pain | 6 | Urinalysis | |
| October 2019 | Fever | 5 | No proteinuria | 0 | |
| Patient 6 | 11 y.o. | Diarrhea | 3 | Proteinuria < 30 mg/dL | 2 |
| November 2017 | Oedema | 3 | Proteinuria 30–100 mg/dL | 2 | |
| Patient 7 | 16 y.o. | Oligo-anuria | 2 | Proteinuria > 300 mg/dL | 4 |
| January 2022 | Headache | 2 | No hematuria | 4 | |
| Patient 8 | 15 y.o. | Cough | 1 | Hematuria < 10 RBC/µL | 4 |
| October 2022 | Shiver | 1 | Hematuria > 10 RBC/µL | 0 |
| Patients | Urea (mg/dL) | Creatinine (mg/dL) | ||
|---|---|---|---|---|
| Onset | Highest Value | Onset | Highest Value | |
| Patient 1 | 154 | 172 | 3.4 | 6.4 |
| Patient 2 | 111 | 215 | 1.3 | 6.6 |
| Patient 3 | 79 | 110 | 2.6 | 5.7 |
| Patient 4 | 103 | 172 | 2.2 | 5.7 |
| Patient 5 | 76 | 296 | 2.3 | 8.5 |
| Patient 6 | 84 | 140 | 2.7 | 4.4 |
| Patient 7 | 107 | 125 | 2.8 | 3.7 |
| Patient 8 | 132 | 132 | 4 | 5.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mocanu, A.; Cajvan, A.-M.; Lazaruc, T.I.; Lupu, V.V.; Florescu, L.; Lupu, A.; Bogos, R.A.; Ioniuc, I.; Scurtu, G.; Dragan, F.; et al. Hantavirus Infection in Children—A Pilot Study of Single Regional Center. Viruses 2023, 15, 872. https://doi.org/10.3390/v15040872
Mocanu A, Cajvan A-M, Lazaruc TI, Lupu VV, Florescu L, Lupu A, Bogos RA, Ioniuc I, Scurtu G, Dragan F, et al. Hantavirus Infection in Children—A Pilot Study of Single Regional Center. Viruses. 2023; 15(4):872. https://doi.org/10.3390/v15040872
Chicago/Turabian StyleMocanu, Adriana, Ana-Maria Cajvan, Tudor Ilie Lazaruc, Vasile Valeriu Lupu, Laura Florescu, Ancuta Lupu, Roxana Alexandra Bogos, Ileana Ioniuc, Georgiana Scurtu, Felicia Dragan, and et al. 2023. "Hantavirus Infection in Children—A Pilot Study of Single Regional Center" Viruses 15, no. 4: 872. https://doi.org/10.3390/v15040872