
COVID-19 and Respiratory Virus Co-Infections: A Systematic Review of the Literature
 ,
, {kind=link}
Abstract
:1. Introduction
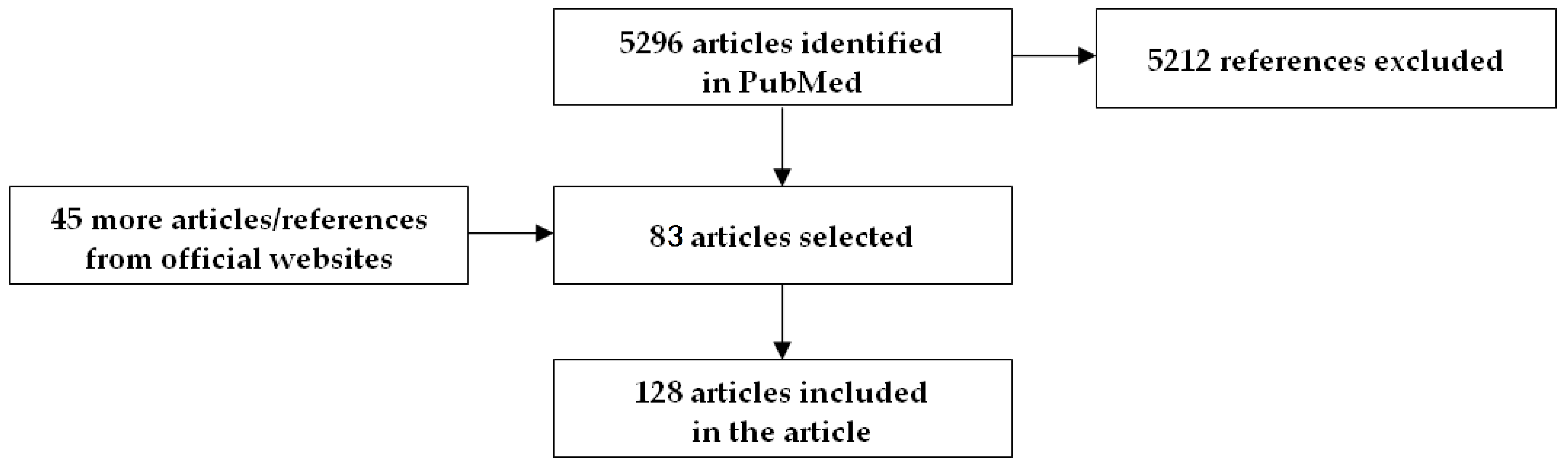
2. Methods
3. SARS-CoV-2 and Influenza Co-Infections
4. SARS-CoV-2 and Respiratory Virus Co-Infections Other Than Influenza
5. Animal Models of SARS-CoV-2 and Influenza Co-Infection
6. Implications for Upcoming Seasons
7. Limitations
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Faust, J.S.; Chen, A.J.; NguemeniTiako, M.J.; Du, C.; Li, S.X.; Krumholz, H.M.; Barnett, M.L. Leading Causes of Death Among Adults Aged 25 to 44 Years by Race and Ethnicity in Texas During the COVID-19 Pandemic, March to December 2020. JAMA Intern. Med. 2022, 182, 87–90. [Google Scholar] [CrossRef]
- Pifarre, I.A.H.; Acosta, E.; Lopez-Casasnovas, G.; Lo, A.; Nicodemo, C.; Riffe, T.; Myrskyla, M. Years of life lost to COVID-19 in 81 countries. Sci. Rep. 2021, 11, 3504. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.N.; Houhamdi, L.; Hoang, V.T.; Stoupan, D.; Fournier, P.E.; Raoult, D.; Colson, P.; Gautret, P. High rate of reinfection with the SARS-CoV-2 Omicron variant. J. Infect. 2022, 85, 174–211. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, L.B.; Foster, C.; Rawlinson, W.; Tedla, N.; Bull, R.A. Evolution of the SARS-CoV-2 omicron variants BA.1 to BA.5: Implications for immune escape and transmission. Rev. Med. Virol. 2022, 32, e2381. [Google Scholar] [CrossRef] [PubMed]
- Psaridi, L.; Maltezou, H.C.; Simonidou, S.; Lialliou, I.; Athanasopoulou, D.; Haila, Z.; Kyrimi, A.; Giannopoulou, I.; Giannousa, S.; Pseimada, M.; et al. Neutralizing antibody responses in healthcare personnel after three doses of mRNA BNT162b2 vaccine and association with baseline characteristics and past SARS-CoV-2 infection. Vaccine 2022, 40, 5752–5756. [Google Scholar] [CrossRef]
- Jayasundara, K.; Soobiahm, C.; Thommes, E.; Tricco, A.C.; Chit, A. Natural Attack Rates of Influenza in Unvaccinated Children and Adults: A Meta-Regression Analysis. BMC Infect. Dis. 2014, 14, 670. [Google Scholar] [CrossRef] [Green Version]
- Shi, T.; Denouel, A.; Tietjen, A.K.; Campbell, I.; Moran, E.; Li, X.; Campbell, H.; Demont, C.; Nyawanda, B.O.; Chu, H.Y.; et al. Global Disease Burden Estimates of Respiratory Syncytial Virus-Associated Acute Respiratory Infection in Older Adults in 2015: A Systematic Review and Meta-Analysis. J. Infect. Dis. 2020, 222 (Suppl. 7), S577–S583. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Wang, X.; Blau, D.M.; Caballero, M.T.; Feikin, D.R.; Gill, C.J.; Madhi, S.A.; Omer, S.B.; Simoes, E.A.F.; Campbell, H.; et al. Global, regional, and national disease burden estimates of acute lower respiratory infections due to respiratory syncytial virus in children younger than 5 years in 2019: A systematic analysis. Lancet 2022, 399, 2047–2064. [Google Scholar] [CrossRef]
- Kondo, Y.; Miyazaki, S.; Yamashita, R.; Ikeda, T. Coinfection with SARS-CoV-2 and influenza A virus. BMJ Case Rep. 2020, 13, 395–403. [Google Scholar] [CrossRef]
- Khodamoradi, Z.; Moghadami, M.; Lotfi, M. Co-infection of Coronavirus Disease 2019 and Influenza A: A Report from Iran. Arch. Iran. Med. 2020, 23, 239–243. [Google Scholar] [CrossRef] [Green Version]
- Hashemi, S.A.; Safamanesh, S.; Ghasemzadeh-Moghaddam, H.; Ghafouri, M.; Azimian, A. High prevalence of SARS-CoV-2 and influenza A virus (H1N1) coinfection in dead patients in Northeastern Iran. J. Med. Virol. 2021, 93, 1008–1012. [Google Scholar] [CrossRef] [PubMed]
- Huang, B.R.; Lin, Y.L.; Wan, C.K.; Wu, J.T.; Hsu, C.Y.; Chiu, M.H.; Huang, C.H. Co-infection of influenza B virus and SARS-CoV-2: A case report from Taiwan. J. Microbiol. Immunol. Infect. 2021, 54, 336–338. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Kaur, P.; Reid, R.J.; Shamoon, F.; Bikkina, M. COVID-19 and Influenza Co-Infection: Report of Three Cases. Cureus 2020, 12, e9852. [Google Scholar] [CrossRef] [PubMed]
- Sang, C.J., 3rd; Heindl, B.; Von Mering, G.; Brott, B.; Kopf, R.S.; Benson, P.V.; Rajapreyar, I. Stress-Induced Cardiomyopathy Precipitated by COVID-19 and Influenza A Coinfection. JACC Case Rep. 2020, 2, 1356–1358. [Google Scholar] [CrossRef]
- Swets, M.C.; Russell, C.D.; Harrison, E.M.; Docherty, A.B.; Lone, N.; Girvan, M.; Hardwick, H.E.; Investigators, I.C.; Visser, L.G.; Openshaw, P.J.M.; et al. SARS-CoV-2 co-infection with influenza viruses, respiratory syncytial virus, or adenoviruses. Lancet 2022, 399, 1463–1464. [Google Scholar] [CrossRef]
- Rubin, R. Influenza’s Unprecedented Low Profile During COVID-19 Pandemic Leaves Experts Wondering What This Flu Season Has in Store. JAMA 2021, 326, 899–900. [Google Scholar] [CrossRef]
- Uyeki, T.M.; Wentworth, D.E.; Jernigan, D.B. Influenza Activity in the US During the 2020-2021 Season. JAMA 2021, 325, 2247–2248. [Google Scholar] [CrossRef]
- Uhteg, K.; Amadi, A.; Forman, M.; Mostafa, H.H. Circulation of Non-SARS-CoV-2 Respiratory Pathogens and Coinfection with SARS-CoV-2 Amid the COVID-19 Pandemic. Open Forum. Infect. Dis. 2022, 9, ofab618. [Google Scholar] [CrossRef]
- Zeng, Z.; Guan, W.; Liu, Y.; Lin, Z.; Liang, W.; Liang, J.; Chen, B.; Wu, T.; Wang, Y.; Yang, C.; et al. Different Circulation Pattern of Multiple Respiratory Viruses in Southern China During the COVID-19 Pandemic. Front. Microbiol. 2021, 12, 801946. [Google Scholar] [CrossRef]
- Tang, X.; Dai, G.; Jiang, X.; Wang, T.; Sun, H.; Chen, Z.; Huang, L.; Wang, M.; Zhu, C.; Yan, Y.; et al. Clinical Characteristics of Pediatric Respiratory Tract Infection and Respiratory Pathogen Isolation During the Coronavirus Disease 2019 Pandemic. Front. Pediatr. 2021, 9, 759213. [Google Scholar] [CrossRef]
- Yakovlev, A.S.; Belyaletdinova, I.K.; Mazankova, L.N.; Samitova, E.R.; Osmanov, I.M.; Gavelya, N.V.; Volok, V.P.; Kolpakova, E.S.; Shishova, A.A.; Dracheva, N.A.; et al. SARS-CoV-2 infection in children in Moscow in 2020: Clinical features and impact on circulation of other respiratory viruses: SARS-CoV-2 infection in children in Moscow in 2020. Int. J. Infect. Dis. 2022, 116, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Kanji, J.N.; Zelyas, N.; Pabbaraju, K.; Granger, D.; Wong, A.; Murphy, S.A.; Buss, E.; MacDonald, C.; Berenger, B.M.; Diggle, M.A.; et al. Respiratory virus coinfections with severe acute respiratory coronavirus virus 2 (SARS-CoV-2) continue to be rare one year into the coronavirus disease 2019 (COVID-19) pandemic in Alberta, Canada (June 2020-May 2021). Infect. Control Hosp. Epidemiol. 2021, 1–4, Online ahead of print. [Google Scholar] [CrossRef]
- De Francesco, M.A.; Pollara, C.; Gargiulo, F.; Giacomelli, M.; Caruso, A. Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 9525. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, G.; La Vecchia, A.; Umbrello, G.; Di Pietro, G.; Bono, P.; Scalia Catenacci, S.; Pinzani, R.; Tagliabue, C.; Bosis, S.; Agostoni, C.; et al. Disappearance of Seasonal Respiratory Viruses in Children Under Two Years Old During COVID-19 Pandemic: A Monocentric Retrospective Study in Milan, Italy. Front. Pediatr. 2021, 9, 721005. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Xu, M.; Cao, L.; Su, L.; Lu, L.; Dong, N.; Jia, R.; Zhu, X.; Xu, J. Impact of COVID-19 pandemic on the prevalence of respiratory viruses in children with lower respiratory tract infections in China. Virol. J. 2021, 18, 159. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Wang, D. Epidemiological changes of common respiratory viruses in children during the COVID-19 pandemic. J. Med. Virol 2022, 94, 1990–1997. [Google Scholar] [CrossRef]
- Fujita, D.M.; Dos Santos Soares, G.; Sartori, G.P.; Henrique da Silva Nali, L. COVID-19 and Influenza coinfection: The rise of Omicron and H3N2 in Brazil—2022. Travel. Med. Infect. Dis. 2022, 46, 102262. [Google Scholar] [CrossRef]
- Australian Government. Department of Health and Aged Care. National 2022 Influenza Season Summary. Available online: https://www.health.gov.au/sites/default/files/2022-12/aisr-2022-national-influenza-season-summary.pdf (accessed on 19 March 2023).
- Centers for Disease Control and Prevention. Weekly US Influenza Surveillance Report. Available online: https://www.cdc.gov/flu/weekly/index.htm (accessed on 19 March 2023).
- Lee, S.S.; Viboud, C.; Petersen, E. Understanding the rebound of influenza in the post COVID-19 pandemic period holds important clues for epidemiology and control. Int. J. Infect. Dis. 2022, 122, 1002–1004. [Google Scholar] [CrossRef]
- Lofgren, E.T.; Naumova, E.N.; Gorski, J.; Naumov, Y.; Fefferman, N.H. How Drivers of Seasonality in Respiratory Infections May Impact Vaccine Strategy: A Case Study in How Coronavirus Disease 2019 (COVID-19) May Help Us Solve One of Influenza’s Biggest Challenges. Clin. Infect. Dis. 2022, 75 (Suppl. 1), S121–S129. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Poland, G. Influenza immunization and COVID-19. Vaccine 2020, 38, 6078–6079. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Intensified Circulation of Respiratory Syncytial Virus (RSV) and Associated Hospital Burden in the EU/EEA. Rapid Risk Assessment, 12 December 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/RRA-20221128-473.pdf (accessed on 19 March 2023).
- Yue, H.; Zhang, M.; Xing, L.; Wang, K.; Rao, X.; Liu, H.; Tian, J.; Zhou, P.; Deng, Y.; Shang, J. The epidemiology and clinical characteristics of co-infection of SARS-CoV-2 and influenza viruses in patients during COVID-19 outbreak. J. Med. Virol. 2020, 92, 2870–2873. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Lai, X.; Chen, Z.; Tu, S.; Qin, K. Clinical characteristics of critically ill patients co-infected with SARS-CoV-2 and the influenza virus in Wuhan, China. Int. J. Infect. Dis. 2020, 96, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Ma, J.; Wang, H.; Wang, X.; Hu, Z.; Li, H.; Zhang, H.; Liu, X. Co-infection of influenza A virus and SARS-CoV-2: A retrospective cohort study. J. Med. Virol. 2021, 93, 2947–2954. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Wang, H.; Su, Z.; Li, W.; Yang, D.; Deng, F.; Chen, J. Co-infection of SARS-CoV-2 and Influenza virus in Early Stage of the COVID-19 Epidemic in Wuhan, China. J. Infect. 2020, 81, e128–e129. [Google Scholar] [CrossRef] [PubMed]
- Miatech, J.L.; Tarte, N.N.; Katragadda, S.; Polman, J.; Robichaux, S.B. A case series of coinfection with SARS-CoV-2 and influenza virus in Louisiana. Respir. Med. Case Rep. 2020, 31, 101214. [Google Scholar] [CrossRef]
- Konala, V.M.; Adapa, S.; Naramala, S.; Chenna, A.; Lamichhane, S.; Garlapati, P.R.; Balla, M.; Gayam, V. A Case Series of Patients Coinfected With Influenza and COVID-19. J. Investig. Med. High. Impact. Case Rep. 2020, 8, 2324709620934674. [Google Scholar] [CrossRef]
- Ding, Q.; Lu, P.; Fan, Y.; Xia, Y.; Liu, M. The clinical characteristics of pneumonia patients coinfected with 2019 novel coronavirus and influenza virus in Wuhan, China. J. Med. Virol. 2020, 92, 1549–1555. [Google Scholar] [CrossRef]
- Wu, X.; Cai, Y.; Huang, X.; Yu, X.; Zhao, L.; Wang, F.; Li, Q.; Gu, S.; Xu, T.; Li, Y.; et al. Co-infection with SARS-CoV-2 and Influenza A Virus in Patient with Pneumonia, China. Emerg. Infect. Dis. 2020, 26, 1324–1326. [Google Scholar] [CrossRef]
- Xiang, X.; Wang, Z.H.; Ye, L.L.; He, X.L.; Wei, X.S.; Ma, Y.L.; Li, H.; Chen, L.; Wang, X.R.; Zhou, Q. Co-infection of SARS-COV-2 and Influenza A Virus: A Case Series and Fast Review. Curr. Med. Sci. 2021, 41, 51–57. [Google Scholar] [CrossRef]
- Cuadrado-Payan, E.; Montagud-Marrahi, E.; Torres-Elorza, M.; Bodro, M.; Blasco, M.; Poch, E.; Soriano, A.; Pineiro, G.J. SARS-CoV-2 and influenza virus co-infection. Lancet 2020, 395, e84. [Google Scholar] [CrossRef]
- Konala, V.M.; Adapa, S.; Gayam, V.; Naramala, S.; Daggubati, S.R.; Kammari, C.B.; Chenna, A. Co-infection with Influenza A and COVID-19. Eur. J. Case Rep. Intern. Med. 2020, 7, 001656. [Google Scholar] [CrossRef]
- Hashemi, S.A.; Safamanesh, S.; Ghafouri, M.; Taghavi, M.R.; Mohajer Zadeh Heydari, M.S.; Namdar Ahmadabad, H.; Ghasemzadeh-Moghaddam, H.; Azimian, A. Co-infection with COVID-19 and influenza A virus in two died patients with acute respiratory syndrome, Bojnurd, Iran. J. Med. Virol. 2020, 92, 2319–2321. [Google Scholar] [CrossRef] [PubMed]
- Munivenkatappa, A.; Yadav, P.D.; Swetha, K.; Jayaswamy, M.; Nyayanit, D.A.; Sahay, R.R.; Basavaraj, T.J. SARS-CoV-2 & influenza A virus co-infection in an elderly patient with pneumonia. Indian J. Med. Res. 2021, 153, 190–195. [Google Scholar] [PubMed]
- Coutinho, A.; Riaz, A.; Makan, A.; Crawford, E.; Dev, D.; Srinivasan, K.; Ahmad, N.; Moudgil, H. Lessons of the month: Co-infection with SARS-CoV-2 and influenza B virus in a patient with community-acquired pneumonia. Clin. Med. 2020, 20, e262–e263. [Google Scholar] [CrossRef]
- Azekawa, S.; Namkoong, H.; Mitamura, K.; Kawaoka, Y.; Saito, F. Co-infection with SARS-CoV-2 and influenza A virus. IDCases 2020, 20, e00775. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Zhang, Z.; Guo, Y.; Shi, J.; Pei, G.; Yao, Y.; Liao, W.; Zeng, R. Lopinavir/ritonavir is associated with pneumonia resolution in COVID-19 patients with influenza coinfection: A retrospective matched-pair cohort study. J. Med. Virol. 2021, 93, 472–480. [Google Scholar] [CrossRef]
- D’Abramo, A.; Lepore, L.; Palazzolo, C.; Barreca, F.; Liuzzi, G.; Lalle, E.; Nicastri, E. Acute respiratory distress syndrome due to SARS-CoV-2 and Influenza A co-infection in an Italian patient: Mini-review of the literature. Int. J. Infect. Dis. 2020, 97, 236–239. [Google Scholar] [CrossRef]
- Lozano-Parras, M.A.; Amann-Arevalo, M.; Ciller-Martinez, M.; Culebras-Lopez, E. COVID-19 and influenza A coinfection: A matter of principle. Enferm. Infecc. Microbiol. Clin. 2021, 39, 214–215. [Google Scholar] [CrossRef]
- Jing, R.; Vunnam, R.R.; Schnaubelt, E.; Vokoun, C.; Cushman-Vokoun, A.; Goldner, D.; Vunnam, S.R. Co-infection of COVID-19 and influenza A in a hemodialysis patient: A case report. BMC Infect. Dis. 2021, 21, 68. [Google Scholar] [CrossRef]
- Lew, S.; Manes, P.; Smith, B. Coinfection with SARS-CoV-2 and Influenza A Virus in a 32-Year-Old Man. Am. J. Case Rep. 2020, 21, e926092. [Google Scholar] [CrossRef]
- Alosaimi, B.; Naeem, A.; Hamed, M.E.; Alkadi, H.S.; Alanazi, T.; Al Rehily, S.S.; Almutairi, A.Z.; Zafar, A. Influenza co-infection associated with severity and mortality in COVID-19 patients. Virol. J. 2021, 18, 127. [Google Scholar] [CrossRef] [PubMed]
- Fontana, C.; Favaro, M.; Minelli, S.; Bossa, M.C.; Altieri, A. Co-infections observed in SARS-CoV-2 positive patients using a rapid diagnostic test. Sci. Rep. 2021, 11, 16355. [Google Scholar] [CrossRef] [PubMed]
- Maddali, R.; Cervellione, K.L.; Lew, L.Q. Apnea in a Two-Week-Old Infant Infected with SARS-CoV-2 and Influenza B. Case Rep. Pediatr. 2022, 2022, 2969561. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, N.; Potdar, V.; Vijay, N.; Mukhopadhyay, L.; Borkakoty, B.; Manjusree, S.; Choudhary, M.L.; Chowdhury, D.; Verma, R.; Bhardwaj, S.D.; et al. SARS-CoV-2 and Influenza Virus Co-Infection Cases Identified through ILI/SARI Sentinel Surveillance: A Pan-India Report. Viruses 2022, 14, 627. [Google Scholar] [CrossRef] [PubMed]
- Alhoufie, S.T.; Alsharif, N.H.; Alfarouk, K.O.; Ibrahim, N.A.; Kheyami, A.M.; Aljifri, A.A. COVID-19 with underdiagnosed influenza B and parainfluenza-2 co-infections in Saudi Arabia: Two case reports. J. Infect. Public Health 2021, 14, 1567–1570. [Google Scholar] [CrossRef]
- Ishiguro, T.; Kobayashi, Y.; Shimizu, Y.; Uemura, Y.; Isono, T.; Takano, K.; Nishida, T.; Kobayashi, Y.; Hosoda, C.; Takaku, Y.; et al. Frequency and Significance of Coinfection in Patients with COVID-19 at Hospital Admission. Intern. Med. 2021, 60, 3709–3719. [Google Scholar] [CrossRef]
- Rizzo, K.R.; Hoover, C.; Jain, S.; Sun, M.; Myers, J.F.; Bregman, B.; Dominguez, D.M.; Jacobsen, A.; Jenkins, G.J.; Hennessy-Burt, T.; et al. Influenza and SARS-CoV-2 Co-infections in California, USA, September 2020-April 2021. Emerg. Infect. Dis. 2021, 27, 2923–2926. [Google Scholar] [CrossRef]
- Heshmat-Ghahdarijani, K.; Vaseghi, G.; Nasirian, M.; Javanmard, S.H. Co-infection between the severe acute respiratory syndrome coronavirus 2 and the influenza Type B in Isfahan, Iran. J. Res. Med. Sci. 2021, 26, 51. [Google Scholar]
- Ali, R.; Patel, A.; Chan, K.H.; Veeraballi, S.; Slim, J. A Case Series of SARS-CoV-2 and Influenza Co-infection. Cureus 2021, 13, e17597. [Google Scholar] [CrossRef]
- Zheng, J.; Chen, F.; Wu, K.; Wang, J.; Li, F.; Huang, S.; Lu, J.; Huang, J.; Liu, H.; Zhou, R.; et al. Clinical and virological impact of single and dual infections with influenza A (H1N1) and SARS-CoV-2 in adult inpatients. PLoS Negl. Trop. Dis. 2021, 15, e0009997. [Google Scholar] [CrossRef]
- Akhtar, Z.; Islam, M.A.; Aleem, M.A.; Mah, E.M.S.; Ahmmed, M.K.; Ghosh, P.K.; Rahman, M.; Rahman, M.Z.; Sumiya, M.K.; Rahman, M.M.; et al. SARS-CoV-2 and influenza virus coinfection among patients with severe acute respiratory infection during the first wave of COVID-19 pandemic in Bangladesh: A hospital-based descriptive study. BMJ Open 2021, 11, e053768. [Google Scholar] [CrossRef] [PubMed]
- Venkatram, S.; Alapati, A.; Dileep, A.; Diaz-Fuentes, G. Change in patterns of hospitalization for influenza during COVID-19 surges. Influenza. Other. Respir. Viruses 2022, 16, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Sreenath, K.; Batra, P.; Vinayaraj, E.V.; Bhatia, R.; SaiKiran, K.; Singh, V.; Singh, S.; Verma, N.; Singh, U.B.; Mohan, A.; et al. Coinfections with Other Respiratory Pathogens among Patients with COVID-19. Microbiol. Spectr. 2021, 9, e0016321. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.; Lee, N.; Park, Y.; Kim, J.; Jeon, K.; Park, M.J.; Song, W. Prevalence and Clinical Impact of Coinfection in Patients with Coronavirus Disease 2019 in Korea. Viruses 2022, 14, 446. [Google Scholar] [CrossRef]
- Castillo, E.M.; Coyne, C.J.; Brennan, J.J.; Tomaszewski, C.A. Rates of coinfection with other respiratory pathogens in patients positive for coronavirus disease 2019 (COVID-19). J. Am. Coll. Emerg. Physicians Open 2020, 1, 592–596. [Google Scholar] [CrossRef]
- Chotpitayasunondh, T.; Fischer, T.K.; Heraud, J.M.; Hurt, A.C.; Monto, A.S.; Osterhaus, A.; Shu, Y.; Tam, J.S. Influenza and COVID-19: What does co-existence mean? Influenza Other Respir. Viruses 2021, 15, 407–412. [Google Scholar] [CrossRef]
- Lai, C.C.; Wang, C.Y.; Hsueh, P.R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti-SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef]
- Hedberg, P.; Johansson, N.; Ternhag, A.; Abdel-Halim, L.; Hedlund, J.; Naucler, P. Bacterial co-infections in community-acquired pneumonia caused by SARS-CoV-2, influenza virus and respiratory syncytial virus. BMC Infect. Dis. 2022, 22, 108. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Papadima, K.; Gkolfinopoulou, K.; Ferentinos, G.; Mouratidou, E.; Andreopoulou, A.; Pavli, A.; Magaziotou, I.; Georgakopoulou, T.; Mellou, K.; et al. Coronavirus disease 2019 pandemic in Greece, February 26–May 3, 2020: The first wave. Travel. Med. Infect. Dis. 2021, 41, 102051. [Google Scholar] [CrossRef]
- Guan, Z.; Chen, C.; Li, Y.; Yan, D.; Zhang, X.; Jiang, D.; Yang, S.; Li, L. Impact of Coinfection With SARS-CoV-2 and Influenza on Disease Severity: A Systematic Review and Meta-Analysis. Front. Public Health 2021, 9, 773130. [Google Scholar] [CrossRef]
- Wanga, V.; Gerdes, M.E.; Shi, D.S.; Choudhary, R.; Dulski, T.M.; Hsu, S.; Idubor, O.I.; Webber, B.J.; Wendel, A.M.; Agathis, N.T.; et al. Characteristics and Clinical Outcomes of Children and Adolescents Aged <18 Years Hospitalized with COVID-19—Six Hospitals, United States, July-August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1766–1772. [Google Scholar] [PubMed]
- Chekuri, S.; Szymczak, W.A.; Goldstein, D.Y.; Nori, P.; Marrero Rolon, R.; Spund, B.; Singh-Tan, S.; Mohrmann, L.; Assa, A.; Southern, W.N.; et al. SARS-CoV-2 coinfection with additional respiratory virus does not predict severe disease: A retrospective cohort study. J. Antimicrob. Chemother. 2021, 76 (Suppl. 3), iii12–iii19. [Google Scholar] [CrossRef] [PubMed]
- Soto, A.; Quinones-Laveriano, D.M.; Valdivia, F.; Juscamayta-Lopez, E.; Azanero-Haro, J.; Chambi, L.; Horna, H.; Patino, G.; Guzman, E.; De la Cruz-Vargas, J.A. Detection of Viral and Bacterial Respiratory Pathogens Identified by Molecular Methods in COVID-19 Hospitalized Patients and Its Impact on Mortality and Unfavorable Outcomes. Infect. Drug. Resist. 2021, 14, 2795–2807. [Google Scholar] [CrossRef] [PubMed]
- Cooksey, G.L.S.; Morales, C.; Linde, L.; Schildhauer, S.; Guevara, H.; Chan, E.; Gibb, K.; Wong, J.; Lin, W.; Bonin, B.J.; et al. Severe Acute Respiratory Syndrome Coronavirus 2 and Respiratory Virus Sentinel Surveillance, California, USA, May 10, 2020-June 12, 2021. Emerg. Infect. Dis. 2022, 28, 9–19. [Google Scholar] [CrossRef]
- Perez-Lazo, G.; Silva-Caso, W.; Del Valle-Mendoza, J.; Morales-Moreno, A.; Ballena-Lopez, J.; Soto-Febres, F.; Martins-Luna, J.; Carrillo-Ng, H.; Del Valle, L.J.; Kym, S.; et al. Identification of Coinfections by Viral and Bacterial Pathogens in COVID-19 Hospitalized Patients in Peru: Molecular Diagnosis and Clinical Characteristics. Antibiotics 2021, 10, 1358. [Google Scholar] [CrossRef]
- Karaaslan, A.; Cetin, C.; Akin, Y.; Demir Tekol, S.; Sobu, E.; Demirhan, R. Coinfection in SARS-CoV-2 Infected Children Patients. J. Infect. Dev. Ctries 2021, 15, 761–765. [Google Scholar] [CrossRef]
- Ma, L.; Wang, W.; Le Grange, J.M.; Wang, X.; Du, S.; Li, C.; Wei, J.; Zhang, J.N. Coinfection of SARS-CoV-2 and Other Respiratory Pathogens. Infect. Drug. Resist. 2020, 13, 3045–3053. [Google Scholar] [CrossRef]
- Zhu, X.; Ge, Y.; Wu, T.; Zhao, K.; Chen, Y.; Wu, B.; Zhu, F.; Zhu, B.; Cui, L. Co-infection with respiratory pathogens among COVID-2019 cases. Virus. Res. 2020, 285, 198005. [Google Scholar] [CrossRef]
- Boschi, C.; Hoang, V.T.; Giraud-Gatineau, A.; Ninove, L.; Lagier, J.C.; La Scola, B.; Gautret, P.; Raoult, D.; Colson, P. Coinfections with SARS-CoV-2 and other respiratory viruses in Southeastern France: A matter of sampling time. J. Med. Virol. 2021, 93, 1878–1881. [Google Scholar] [CrossRef]
- Allou, N.; Larsen, K.; Dubernet, A.; Traversier, N.; Masse, L.; Foch, E.; Bruneau, L.; Maillot, A.; Andre, M.; Lagrange-Xelot, M.; et al. Co-infection in patients with hypoxemic pneumonia due to COVID-19 in Reunion Island. Medicine 2021, 100, e24524. [Google Scholar] [CrossRef]
- Tang, M.L.; Li, Y.Q.; Chen, X.; Lin, H.; Jiang, Z.C.; Gu, D.L.; Chen, X.; Tang, C.X.; Xie, Z.Q. Co-Infection with Common Respiratory Pathogens and SARS-CoV-2 in Patients with COVID-19 Pneumonia and Laboratory Biochemistry Findings: A Retrospective Cross-Sectional Study of 78 Patients from a Single Center in China. Med. Sci. Monit. 2021, 27, e929783. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, H.; Wang, F.; Lu, X.; Du, H.; Xu, J.; Han, F.; Zhang, L.; Zhang, M. Co-infections of SARS-CoV-2 with multiple common respiratory pathogens in infected children: A retrospective study. Medicine 2021, 100, e24315. [Google Scholar] [CrossRef] [PubMed]
- Nowak, M.D.; Sordillo, E.M.; Gitman, M.R.; PanizMondolfi, A.E. Coinfection in SARS-CoV-2 infected patients: Where are influenza virus and rhinovirus/enterovirus? J. Med. Virol. 2020, 92, 1699–1700. [Google Scholar] [CrossRef]
- Schirmer, P.; Lucero-Obusan, C.; Sharma, A.; Sohoni, P.; Oda, G.; Holodniy, M. Respiratory co-infections with COVID-19 in the Veterans Health Administration, 2020. Diagn. Microbiol. Infect. Dis. 2021, 100, 115312. [Google Scholar] [CrossRef] [PubMed]
- Weissberg, D.; Boni, J.; Rampini, S.K.; Kufner, V.; Zaheri, M.; Schreiber, P.W.; Abela, I.A.; Huber, M.; Sax, H.; Wolfensberger, A. Does respiratory co-infection facilitate dispersal of SARS-CoV-2? investigation of a super-spreading event in an open-space office. Antimicrob. Resist. Infect. Control 2020, 9, 191. [Google Scholar] [CrossRef] [PubMed]
- Si, Y.; Zhao, Z.; Chen, R.; Zhong, H.; Liu, T.; Wang, M.; Song, X.; Li, W.; Ying, B. Epidemiological surveillance of common respiratory viruses in patients with suspected COVID-19 in Southwest China. BMC Infect. Dis. 2020, 20, 688. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, S.A.; Safamanesh, S.; Ghasemzadeh-Moghaddam, H.; Ghafouri, M.; Mohajerzadeh-Heydari, M.S.; Namdar-Ahmadabad, H.; Azimian, A. Report of death in children with SARS-CoV-2 and human metapneumovirus (hMPV) coinfection: Is hMPV the trigger? J. Med. Virol. 2021, 93, 579–581. [Google Scholar] [CrossRef] [PubMed]
- Leuzinger, K.; Roloff, T.; Gosert, R.; Sogaard, K.; Naegele, K.; Rentsch, K.; Bingisser, R.; Nickel, C.H.; Pargger, H.; Bassetti, S.; et al. Epidemiology of Severe Acute Respiratory Syndrome Coronavirus 2 Emergence Amidst Community-Acquired Respiratory Viruses. J. Infect. Dis. 2020, 222, 1270–1279. [Google Scholar] [CrossRef]
- Motta, J.C.; Gomez, C.C. Adenovirus and novel coronavirus (SARS-Cov2) coinfection: A case report. IDCases 2020, 22, e00936. [Google Scholar] [CrossRef]
- Sanchez-Nadales, A.; Treminio-Quezada, M.; Abad, H.; Navarro-Motta, J.; Contreras-Chavez, P.; Kachru, A.; Chu, C. Critical Care Management for Novel 2019 SARS-CoV-2 and HCoV-NL63 Coinfection in a Young Immunocompromised Patient: A Chicago Experience. Case Rep. Crit. Care 2020, 2020, 8877641. [Google Scholar] [CrossRef]
- Nascimento, J.; Castro, R.R.T.; Nascimento, J.; Knoploch, B.B.; Duque, P.; Neves, M.A.O. Coinfection of SARS-CoV-2 and Measles morbillivirus in a front-line health worker in Rio de Janeiro, Brasil. Rev. Assoc. Med. Bras. 2020, 66, 1027–1029. [Google Scholar] [CrossRef] [PubMed]
- Touzard-Romo, F.; Tape, C.; Lonks, J.R. Co-infection with SARS-CoV-2 and Human Metapneumovirus. Rhode Isl. Med. J. 2020, 103, 75–76. [Google Scholar]
- Sohal, S.; Rodriguez-Nava, G.; Khabbaz, R.; Chaudry, S.; Musurakis, C.; Chitrakar, S.; Chundi, V.V.; Friedman, H.J. SARS-CoV2 and Co-Infections: A Review of Two Cases. Case Rep. Infect. Dis. 2020, 2020, 8882348. [Google Scholar] [CrossRef] [PubMed]
- Danley, K.; Kent, P. 4-month-old boy coinfected with COVID-19 and adenovirus. BMJ Case Rep. 2020, 13, e236264. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Liu, P.; Xiong, G.; Yang, Z.; Wang, M.; Li, Y.; Yu, X.J. Coinfection of SARS-CoV-2 and multiple respiratory pathogens in children. Clin. Chem. Lab. Med. 2020, 58, 1160–1161. [Google Scholar] [CrossRef] [Green Version]
- Kakuya, F.; Okubo, H.; Fujiyasu, H.; Wakabayashi, I.; Syouji, M.; Kinebuchi, T. The First Pediatric Patients with Coronavirus Disease 2019 (COVID-19) in Japan: Risk of Co-Infection with Other Respiratory Viruses. Jpn. J. Infect. Dis. 2020, 73, 377–380. [Google Scholar] [CrossRef]
- Langerbeins, P.; Furstenau, M.; Gruell, H.; Klein, F.; Persigehl, T.; Rybniker, J.; Seeger-Nukpezah, T.; Kochanek, M.; Hallek, M.; Eichhorst, B.; et al. COVID-19 complicated by parainfluenza co-infection in a patient with chronic lymphocytic leukemia. Eur. J. Haematol. 2020, 105, 508–511. [Google Scholar] [CrossRef]
- Rodriguez, J.A.; Rubio-Gomez, H.; Roa, A.A.; Miller, N.; Eckardt, P.A. Co-Infection with SARS-COV-2 and Parainfluenza in a young adult patient with pneumonia: Case Report. IDCases 2020, 20, e00762. [Google Scholar] [CrossRef]
- Alharthy, A.; Faqihi, F.; Karakitsos, D. SARS-CoV-2 Complicated by Sinusitis and Co-Infection with Human Metapneumovirus. Rhode Isl. Med. J. 2020, 103, 23–24. [Google Scholar]
- Scott, S.J.; Pfotenhauer, B.; Weiner, J.J.; Hilleshiem, J.; Khubbar, M.; Bhattacharyya, S. Respiratory Pathogen Coinfections in SARS-CoV-2-Positive Patients in Southeastern Wisconsin: A Retrospective Analysis. Microbiol. Spectr. 2021, 9, e0083121. [Google Scholar] [CrossRef]
- Davis, B.; Rothrock, A.N.; Swetland, S.; Andris, H.; Davis, P.; Rothrock, S.G. Viral and atypical respiratory co-infections in COVID-19: A systematic review and meta-analysis. J. Am. Coll. Emerg. Physicians Open 2020, 1, 533–548. [Google Scholar] [CrossRef] [PubMed]
- Lansbury, L.; Lim, B.; Baskaran, V.; Lim, W.S. Co-infections in people with COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Bai, L.; Zhao, Y.; Dong, J.; Liang, S.; Guo, M.; Liu, X.; Wang, X.; Huang, Z.; Sun, X.; Zhang, Z.; et al. Coinfection with influenza A virus enhances SARS-CoV-2 infectivity. Cell Res. 2021, 31, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.J.; Lee, A.C.; Chan, J.F.; Liu, F.; Li, C.; Chen, Y.; Chu, H.; Lau, S.Y.; Wang, P.; Chan, C.C.; et al. Coinfection by Severe Acute Respiratory Syndrome Coronavirus 2 and Influenza A(H1N1)pdm09 Virus Enhances the Severity of Pneumonia in Golden Syrian Hamsters. Clin. Infect. Dis. 2021, 72, e978–e992. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Nguyen, T.Q.; Casel, M.A.B.; Rollon, R.; Kim, S.M.; Kim, Y.I.; Yu, K.M.; Jang, S.G.; Yang, J.; Poo, H.; et al. Coinfection with SARS-CoV-2 and Influenza A Virus Increases Disease Severity and Impairs Neutralizing Antibody and CD4(+) T Cell Responses. J. Virol. 2022, 96, e0187321. [Google Scholar] [CrossRef] [PubMed]
- Achdout, H.; Vitner, E.B.; Politi, B.; Melamed, S.; Yahalom-Ronen, Y.; Tamir, H.; Erez, N.; Avraham, R.; Weiss, S.; Cherry, L.; et al. Increased lethality in influenza and SARS-CoV-2 coinfection is prevented by influenza immunity but not SARS-CoV-2 immunity. Nat. Commun. 2021, 12, 5819. [Google Scholar] [CrossRef]
- Huang, Y.; Skarlupka, A.L.; Jang, H.; Blas-Machado, U.; Holladay, N.; Hogan, R.J.; Ross, T.M. SARS-CoV-2 and Influenza A Virus Coinfections in Ferrets. J. Virol. 2022, 96, e0179121. [Google Scholar] [CrossRef]
- Ryan, K.A.; Schewe, K.E.; Crowe, J.; Fotheringham, S.A.; Hall, Y.; Humphreys, R.; Marriott, A.C.; Paterson, J.; Rayner, E.; Salguero, F.J.; et al. Sequential Delivery of Live Attenuated Influenza Vaccine and Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) in the Ferret Model Can Reduce SARS-CoV-2 Shedding and Does Not Result in Enhanced Lung Pathology. J. Infect. Dis. 2022, 225, 404–412. [Google Scholar] [CrossRef]
- Essaidi-Laziosi, M.; Alvarez, C.; Puhach, O.; Sattonnet-Roche, P.; Torriani, G.; Tapparel, C.; Kaiser, L.; Eckerle, I. Sequential infections with rhinovirus and influenza modulate the replicative capacity of SARS-CoV-2 in the upper respiratory tract. Emerg. Microbes. Infect. 2022, 11, 412–423. [Google Scholar] [CrossRef]
- Fage, C.; Henaut, M.; Carbonneau, J.; Piret, J.; Boivin, G. Influenza A(H1N1)pdm09 Virus but Not Respiratory Syncytial Virus Interferes with SARS-CoV-2 Replication during Sequential Infections in Human Nasal Epithelial Cells. Viruses 2022, 14, 395. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Pavli, A.; Tsakris, A. Post-COVID Syndrome: An Insight on Its Pathogenesis. Vaccines 2021, 9, 497. [Google Scholar] [CrossRef] [PubMed]
- Cau, A.; Cheng, M.P.; Lee, T.; Levin, A.; Lee, T.C.; Vinh, D.C.; Lamontagne, F.; Singer, J.; Walley, K.R.; Murthy, S.; et al. Acute Kidney Injury and Renal Replacement Therapy in COVID-19 Versus Other Respiratory Viruses: A Systematic Review and Meta-Analysis. Can. J. Kidney Health Dis. 2021, 8, 20543581211052185. [Google Scholar] [CrossRef] [PubMed]
- Jones, N. How COVID-19 is changing the cold and flu season. Nature 2020, 588, 388–390. [Google Scholar] [CrossRef]
- Covin, S.; Rutherford, G.W. Coinfection, Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), and Influenza: An Evolving Puzzle. Clin. Infect. Dis. 2021, 72, e993–e994. [Google Scholar] [CrossRef]
- Ni, M.; Xu, H.; Luo, J.; Liu, W.; Zhou, D. Simultaneous detection and differentiation of SARS-CoV-2, influenza A virus and influenza B virus by one-step quadruplex real-time RT-PCR in patients with clinical manifestations. Int. J. Infect. Dis. 2021, 103, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.Y.; Jian, M.J.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Chen, C.W.; Chiu, S.K.; Wang, Y.H.; Liao, S.J.; Li, S.Y.; et al. Novel dual multiplex real-time RT-PCR assays for the rapid detection of SARS-CoV-2, influenza A/B, and respiratory syncytial virus using the BD MAX open system. Emerg. Microbes. Infect. 2021, 10, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Mancini, F.; Barbanti, F.; Scaturro, M.; Fontana, S.; Di Martino, A.; Marsili, G.; Puzelli, S.; Calzoletti, L.; Facchini, M.; Di Mario, G.; et al. Multiplex Real-Time Reverse-Transcription Polymerase Chain Reaction Assays for Diagnostic Testing of Severe Acute Respiratory Syndrome Coronavirus 2 and Seasonal Influenza Viruses: A Challenge of the Phase 3 Pandemic Setting. J. Infect. Dis. 2021, 223, 765–774. [Google Scholar] [CrossRef]
- Chung, H.Y.; Jian, M.J.; Chang, C.K.; Lin, J.C.; Yeh, K.M.; Yang, Y.S.; Chen, C.W.; Hsieh, S.S.; Tang, S.H.; Perng, C.L.; et al. Multicenter study evaluating one multiplex RT-PCR assay to detect SARS-CoV-2, influenza A/B, and respiratory syncytial virus using the LabTurbo AIO open platform: Epidemiological features, automated sample-to-result, and high-throughput testing. Aging 2021, 13, 24931–24942. [Google Scholar] [CrossRef]
- Shu, B.; Kirby, M.K.; Davis, W.G.; Warnes, C.; Liddell, J.; Liu, J.; Wu, K.H.; Hassell, N.; Benitez, A.J.; Wilson, M.M.; et al. Multiplex Real-Time Reverse Transcription PCR for Influenza A Virus, Influenza B Virus, and Severe Acute Respiratory Syndrome Coronavirus 2. Emerg. Infect. Dis. 2021, 27, 1821–1830. [Google Scholar] [CrossRef]
- Cohen, R.; Babushkin, F.; Finn, T.; Geller, K.; Alexander, H.; Datnow, C.; Uda, M.; Shapiro, M.; Paikin, S.; Lellouche, J. High Rates of Bacterial Pulmonary Co-Infections and Superinfections Identified by Multiplex PCR among Critically Ill COVID-19 Patients. Microorganisms 2021, 9, 2483. [Google Scholar] [CrossRef]
- Kim, T.Y.; Kim, J.Y.; Shim, H.J.; Yun, S.A.; Jang, J.H.; Huh, H.J.; Kim, J.W.; Lee, N.Y. Comparison of the PowerChek SARS-CoV-2, Influenza A&B, RSV Multiplex Real-time PCR Kit and BioFire Respiratory Panel 2.1 for simultaneous detection of SARS-CoV-2, influenza A and B, and respiratory syncytial virus. J. Virol. Methods 2021, 298, 114304. [Google Scholar] [PubMed]
- Rothe, K.; Spinner, C.D.; Panning, M.; Pletz, M.W.; Rohde, G.; Rupp, J.; Witzenrath, M.; Erber, J.; Eberhardt, F.; Essig, A.; et al. Evaluation of a multiplex PCR screening approach to identify community-acquired bacterial co-infections in COVID-19: A multicenter prospective cohort study of the German competence network of community-acquired pneumonia (CAPNETZ). Infection 2021, 49, 1299–1306. [Google Scholar] [CrossRef] [PubMed]
- Sahajpal, N.S.; Mondal, A.K.; Ananth, S.; Njau, A.; Jones, K.; Ahluwalia, P.; Oza, E.; Ross, T.M.; Kota, V.; Kothandaraman, A.; et al. Clinical validation of a multiplex PCR-based detection assay using saliva or nasopharyngeal samples for SARS-Cov-2, influenza A and B. Sci. Rep. 2022, 12, 3480. [Google Scholar] [CrossRef] [PubMed]
- McKimm-Breschkin, J.L.; Hay, A.J.; Cao, B.; Cox, R.J.; Dunning, J.; Moen, A.C.; Olson, D.; Pizzorno, A.; Hayden, F.G. COVID-19, Influenza and RSV: Surveillance-informed prevention and treatment—Meeting report from an isirv-WHO virtual conference. Antiviral. Res. 2022, 197, 105227. [Google Scholar] [CrossRef] [PubMed]
- Faury, H.; Courboules, C.; Payen, M.; Jary, A.; Hausfater, P.; Luyt, C.; Dres, M.; Pourcher, V.; Abdi, B.; Wirden, M.; et al. Medical features of COVID-19 and influenza infection: A comparative study in Paris, France. J. Infect. 2021, 82, e36–e39. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maltezou, H.C.; Papanikolopoulou, A.; Vassiliu, S.; Theodoridou, K.; Nikolopoulou, G.; Sipsas, N.V. COVID-19 and Respiratory Virus Co-Infections: A Systematic Review of the Literature. Viruses 2023, 15, 865. https://doi.org/10.3390/v15040865
Maltezou HC, Papanikolopoulou A, Vassiliu S, Theodoridou K, Nikolopoulou G, Sipsas NV. COVID-19 and Respiratory Virus Co-Infections: A Systematic Review of the Literature. Viruses. 2023; 15(4):865. https://doi.org/10.3390/v15040865
Chicago/Turabian StyleMaltezou, Helena C., Amalia Papanikolopoulou, Sofia Vassiliu, Kalliopi Theodoridou, Georgia Nikolopoulou, and Nikolaos V. Sipsas. 2023. "COVID-19 and Respiratory Virus Co-Infections: A Systematic Review of the Literature" Viruses 15, no. 4: 865. https://doi.org/10.3390/v15040865