
Epidemiologic and Clinical Characteristics of Human Bocavirus Infection in Children with or without Acute Gastroenteritis in Acre, Northern Brazil
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Specimens and Ethical Aspects
2.2. Nucleic Acid Extraction
2.3. HBoV Molecular Detection
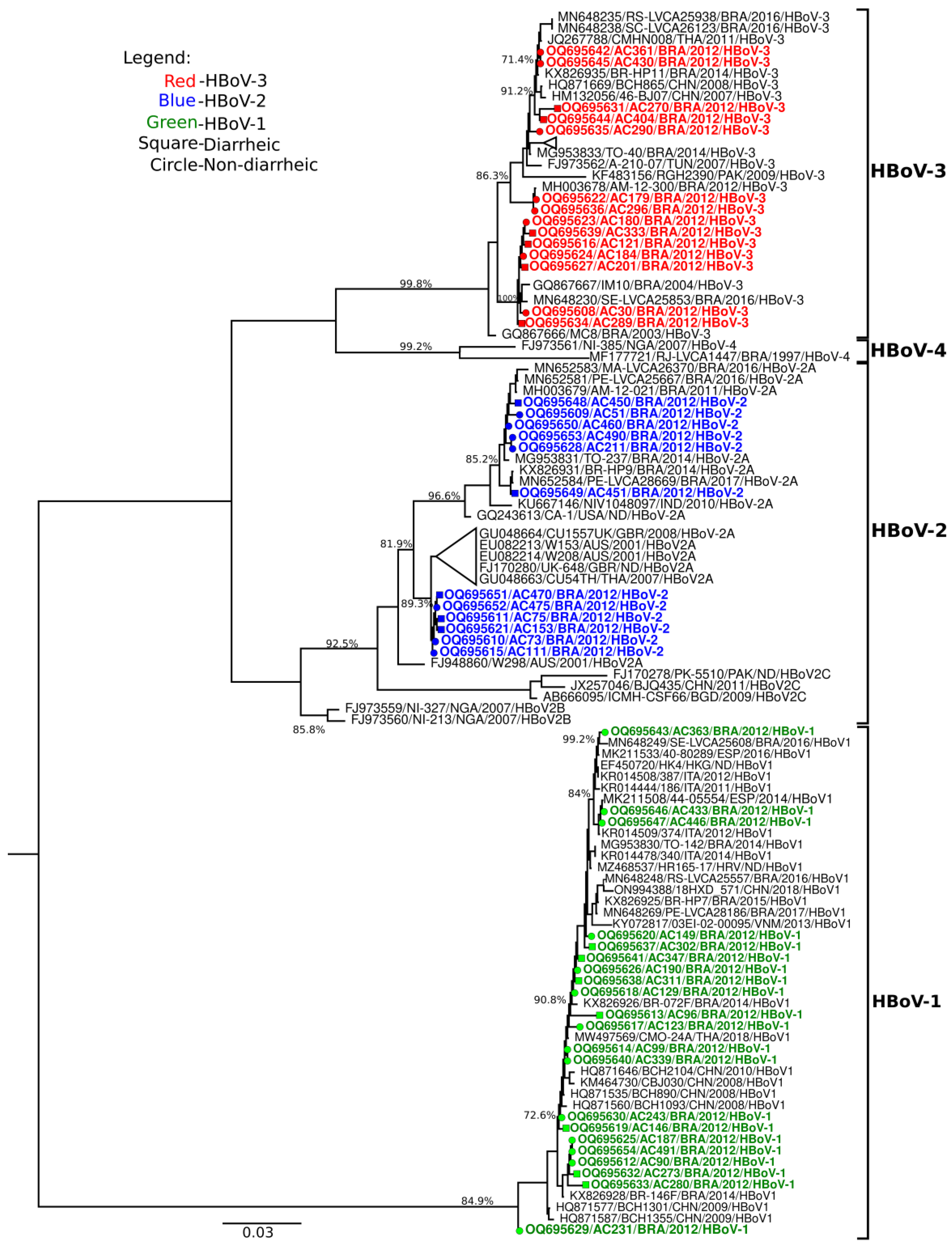
2.4. Molecular Characterization and Phylogenetic Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perin, J.; Mulick, A.; Yeung, D.; Villavicencio, F.; Lopez, G.; Strong, K.L.; Prieto-Merino, D.; Cousens, S.; Black, R.E.; Liu, L. Global, Regional, and National Causes of under-5 Mortality in 2000–19: An Updated Systematic Analysis with Implications for the Sustainable Development Goals. Lancet Child Adolesc. Health 2022, 6, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Bányai, K.; Estes, M.K.; Martella, V.; Parashar, U.D. Viral Gastroenteritis. Lancet 2018, 392, 175–186. [Google Scholar] [CrossRef] [PubMed]
- Simpson, R.; Aliyu, S.; Iturriza-Gómara, M.; Desselberger, U.; Gray, J. Infantile Viral Gastroenteritis: On the Way to Closing the Diagnostic Gap. J. Med. Virol. 2003, 70, 258–262. [Google Scholar] [CrossRef]
- Vocale, C.; Rimoldi, S.G.; Pagani, C.; Grande, R.; Pedna, F.; Arghittu, M.; Lunghi, G.; Maraschini, A.; Gismondo, M.R.; Landini, M.P.; et al. Comparative Evaluation of the New xTAG GPP Multiplex Assay in the Laboratory Diagnosis of Acute Gastroenteritis. Clinical Assessment and Potential Application from a Multicentre Italian Study. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2015, 34, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Allander, T.; Tammi, M.T.; Eriksson, M.; Bjerkner, A.; Tiveljung-Lindell, A.; Andersson, B. Cloning of a Human Parvovirus by Molecular Screening of Respiratory Tract Samples. Proc. Natl. Acad. Sci. USA 2005, 102, 12891–12896. [Google Scholar] [CrossRef] [PubMed]
- Current ICTV Taxonomy Release|ICTV. Available online: https://ictv.global/taxonomy (accessed on 23 March 2023).
- Arthur, J.L.; Higgins, G.D.; Davidson, G.P.; Givney, R.C.; Ratcliff, R.M. A Novel Bocavirus Associated with Acute Gastroenteritis in Australian Children. PLoS Pathog. 2009, 5, e1000391. [Google Scholar] [CrossRef]
- Campos, G.S.; Silva Sampaio, M.L.; Menezes, A.D.L.; Tigre, D.M.; Moura Costa, L.F.; Chinalia, F.A.; Sardi, S.I. Human Bocavirus in Acute Gastroenteritis in Children in Brazil. J. Med. Virol. 2016, 88, 166–170. [Google Scholar] [CrossRef]
- Kapoor, A.; Slikas, E.; Simmonds, P.; Chieochansin, T.; Naeem, A.; Shaukat, S.; Alam, M.M.; Sharif, S.; Angez, M.; Zaidi, S.; et al. A New Bocavirus Species in Human Stool. J. Infect. Dis. 2009, 199, 196–200. [Google Scholar] [CrossRef]
- Guido, M.; Tumolo, M.R.; Verri, T.; Romano, A.; Serio, F.; De Giorgi, M.; De Donno, A.; Bagordo, F.; Zizza, A. Human Bocavirus: Current Knowledge and Future Challenges. World J. Gastroenterol. 2016, 22, 8684–8697. [Google Scholar] [CrossRef]
- Ong, D.S.Y.; Schuurman, R.; Heikens, E. Human Bocavirus in Stool: A True Pathogen or an Innocent Bystander? J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2016, 74, 45–49. [Google Scholar] [CrossRef]
- Khamrin, P.; Malasao, R.; Chaimongkol, N.; Ukarapol, N.; Kongsricharoern, T.; Okitsu, S.; Hayakawa, S.; Ushijima, H.; Maneekarn, N. Circulating of Human Bocavirus 1, 2, 3, and 4 in Pediatric Patients with Acute Gastroenteritis in Thailand. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2012, 12, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, A.; Simmonds, P.; Slikas, E.; Li, L.; Bodhidatta, L.; Sethabutr, O.; Triki, H.; Bahri, O.; Oderinde, B.S.; Baba, M.M.; et al. Human Bocaviruses Are Highly Diverse, Dispersed, Recombination Prone, and Prevalent in Enteric Infections. J. Infect. Dis. 2010, 201, 1633–1643. [Google Scholar] [CrossRef] [PubMed]
- Chow, B.D.W.; Ou, Z.; Esper, F.P. Newly Recognized Bocaviruses (HBoV, HBoV2) in Children and Adults with Gastrointestinal Illness in the United States. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2010, 47, 143–147. [Google Scholar] [CrossRef]
- Paloniemi, M.; Lappalainen, S.; Salminen, M.; Kätkä, M.; Kantola, K.; Hedman, L.; Hedman, K.; Söderlund-Venermo, M.; Vesikari, T. Human Bocaviruses Are Commonly Found in Stools of Hospitalized Children without Causal Association to Acute Gastroenteritis. Eur. J. Pediatr. 2014, 173, 1051–1057. [Google Scholar] [CrossRef]
- Bitencurt, E.L.R.; Siqueira, J.A.M.; Medeiros, T.B.; Bandeira, R.D.S.; de Souza Oliveira, D.; de Paula Souza e Guimaraes, R.J.; da Silva Soares, L.; Macarenhas, J.D.A.P.; Teixeira, D.M.; Silva, R.S.; et al. Epidemiological and Molecular Investigation of Norovirus and Astrovirus Infections in Rio Branco, Acre, Northern Brazil: A Retrospective Study. J. Med. Virol. 2019, 91, 997–1007. [Google Scholar] [CrossRef] [PubMed]
- Neves, M.A.O.; Pinheiro, H.H.C.; Silva, R.S.U.; Linhares, A.C.; Silva, L.D.; Gabbay, Y.B.; Silva, M.C.M.; Loureiro, E.C.B.; Soares, L.S.; Mascarenhas, J.D.P. High Prevalence of G12P[8] Rotavirus Strains in Rio Branco, Acre, Western Amazon, in the Post-Rotavirus Vaccine Introduction Period. J. Med. Virol. 2016, 88, 782–789. [Google Scholar] [CrossRef]
- da Silva, L.D.; Rodrigues, E.L.; de Lucena, M.S.S.; de Lima, I.C.G.; de Sousa Oliveira, D.; Soares, L.S.; Mascarenhas, J.D.P.; da Costa Linhares, A.; Gabbay, Y.B. Detection of the Pandemic Norovirus Variant GII.4 Sydney 2012 in Rio Branco, State of Acre, Northern Brazil. Mem. Inst. Oswaldo Cruz 2013, 108, 1068–1070. [Google Scholar] [CrossRef]
- Boom, R.; Sol, C.J.; Salimans, M.M.; Jansen, C.L.; Wertheim-van Dillen, P.M.; van der Noordaa, J. Rapid and Simple Method for Purification of Nucleic Acids. J. Clin. Microbiol. 1990, 28, 495–503. [Google Scholar] [CrossRef]
- Kearse, M.; Moir, R.; Wilson, A.; Stones-Havas, S.; Cheung, M.; Sturrock, S.; Buxton, S.; Cooper, A.; Markowitz, S.; Duran, C.; et al. Geneious Basic: An Integrated and Extendable Desktop Software Platform for the Organization and Analysis of Sequence Data. Bioinform. Oxf. Engl. 2012, 28, 1647–1649. [Google Scholar] [CrossRef]
- Katoh, K.; Misawa, K.; Kuma, K.; Miyata, T. MAFFT: A Novel Method for Rapid Multiple Sequence Alignment Based on Fast Fourier Transform. Nucleic Acids Res. 2002, 30, 3059–3066. [Google Scholar] [CrossRef]
- Soares, L.S.; Lima, A.B.F.; Pantoja, K.C.; Lobo, P.S.; Cruz, J.F.; Guerra, S.F.S.; Bezerra, D.A.M.; Bandeira, R.S.; Mascarenhas, J.D.P. Molecular Epidemiology of Human Bocavirus in Children with Acute Gastroenteritis from North Region of Brazil. J. Med. Microbiol. 2019, 68, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Castro, L.R.P.; Calvet, F.C.; Sousa, K.L.; Silva, V.P.; Lobo, P.S.; Penha, E.T.; Guerra, S.F.S.; Bezerra, D.A.M.; Mascarenhas, J.D.P.; Pinheiro, H.H.C.; et al. Prevalence of Rotavirus and Human Bocavirus in Immunosuppressed Individuals after Renal Transplantation in the Northern Region of Brazil. J. Med. Virol. 2019, 91, 2125–2133. [Google Scholar] [CrossRef] [PubMed]
- Malta, F.C.; Varella, R.B.; Guimarães, M.A.A.M.; Miagostovich, M.P.; Fumian, T.M. Human Bocavirus in Brazil: Molecular Epidemiology, Viral Load and Co-Infections. Pathogens 2020, 9, 645. [Google Scholar] [CrossRef] [PubMed]
- Risku, M.; Kätkä, M.; Lappalainen, S.; Räsänen, S.; Vesikari, T. Human Bocavirus Types 1, 2 and 3 in Acute Gastroenteritis of Childhood. Acta Paediatr. 2012, 101, e405–e410. [Google Scholar] [CrossRef] [PubMed]
- Leitão, G.A.A.; Olivares, A.I.O.; Pimenta, Y.C.; Delgado, I.F.; Miagostovich, M.P.; Leite, J.P.G.; de Moraes, M.T.B. Human Bocavirus Genotypes 1 and 2 Detected in Younger Amazonian Children with Acute Gastroenteritis or Respiratory Infections, Respectively. Int. J. Infect. Dis. 2020, 95, 32–37. [Google Scholar] [CrossRef]
- Tymentsev, A.; Tikunov, A.; Zhirakovskaia, E.; Kurilschikov, A.; Babkin, I.; Klemesheva, V.; Netesov, S.; Tikunova, N. Human Bocavirus in Hospitalized Children with Acute Gastroenteritis in Russia from 2010 to 2012. Infect. Genet. Evol. J. Mol. Epidemiol. Evol. Genet. Infect. Dis. 2016, 37, 143–149. [Google Scholar] [CrossRef]
- Schildgen, O. Human Bocavirus: Lessons Learned to Date. Pathogens 2013, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rikhotso, M.C.; Kabue, J.P.; Ledwaba, S.E.; Traoré, A.N.; Potgieter, N. Prevalence of Human Bocavirus in Africa and Other Developing Countries between 2005 and 2016: A Potential Emerging Viral Pathogen for Diarrhea. J. Trop. Med. 2018, 2018, 7875482. [Google Scholar] [CrossRef]
- Liu, L.; Hill, K.; Oza, S.; Hogan, D.; Chu, Y.; Cousens, S.; Mathers, C.; Stanton, C.; Lawn, J.; Robert, B.E. Levels and Causes of Mortality under Age Five Years. In Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, 3rd ed.; Black, R.E., Laxminarayan, R., Temmerman, M., Walker, N., Eds.; The International Bank for Reconstruction and Development/The World Bank: Washington, DC, USA, 2016; Volume 2, ISBN 978-1-4648-0348-2. [Google Scholar]
- Ali, G.M.; Hussein, A.A.; kadim, J.I.; Aufi, I.M. Detecting and Genotyping of Human Bocavirus among Children with Gastroenteritis in Diyala Governorate. Proc. Ann. Trop. Med. Public Health 2020, 23. [Google Scholar] [CrossRef]
- Lasure, N.; Gopalkrishna, V. Molecular Epidemiology and Clinical Severity of Human Bocavirus (HBoV) 1-4 in Children with Acute Gastroenteritis from Pune, Western India. J. Med. Virol. 2017, 89, 17–23. [Google Scholar] [CrossRef]
- Proenca-Modena, J.L.; Martinez, M.; Amarilla, A.A.; Espínola, E.E.; Galeano, M.E.; Fariña, N.; Russomando, G.; Aquino, V.H.; Parra, G.I.; Arruda, E. Viral Load of Human Bocavirus-1 in Stools from Children with Viral Diarrhoea in Paraguay. Epidemiol. Infect. 2013, 141, 2576–2580. [Google Scholar] [CrossRef] [PubMed]
- Lekana-Douki, S.E.; Behillil, S.; Enouf, V.; Leroy, E.M.; Berthet, N. Detection of Human Bocavirus-1 in Both Nasal and Stool Specimens from Children under 5 Years Old with Influenza-like Illnesses or Diarrhea in Gabon. BMC Res. Notes 2018, 11, 495. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Epidemiological Variables | HBoV Infection | ||||||
|---|---|---|---|---|---|---|---|
| Negative | Positive | Total | |||||
| N | % | N | % | N | % | p | |
| Gender | |||||||
| Female | 204 | 47.2 | 23 | 47.9 | 227 | 47.3 | 0.427 |
| Male | 228 | 52.8 | 25 | 52.1 | 253 | 52.7 | |
| Age group | |||||||
| <6 months | 94 | 21.7 | 5 | 10.4 | 99 | 20.6 | 0.252 |
| 7 to 24 months | 171 | 39.6 | 24 | 50.0 | 195 | 40.6 | |
| 25 to 60 months | 165 | 38.2 | 19 | 39.6 | 184 | 38.4 | |
| NI | 2 | 0.5 | 0 | 0 | 2 | 0.4 | |
| Area | |||||||
| Urban | 386 | 89.4 | 41 | 85.4 | 427 | 89.0 | 0.433 |
| Rural | 41 | 9.5 | 6 | 12.5 | 47 | 9.8 | |
| NI | 5 | 1.2 | 1 | 2.1 | 6 | 1.3 | |
| Consumer water | |||||||
| Public network supply | 228 | 52.8 | 27 | 56.3 | 255 | 53.1 | 0.826 |
| Well, river | 201 | 46.5 | 21 | 43.7 | 222 | 46.3 | |
| NI | 3 | 0.7 | 0 | 0 | 3 | 0.6 | |
| Destination of waste | |||||||
| Sewage network | 261 | 60.4 | 24 | 50.0 | 285 | 59.4 | 0.112 |
| Septic tank | 145 | 33.6 | 18 | 37.5 | 163 | 34.6 | |
| Others | 20 | 4.6 | 6 | 12.5 | 26 | 5.4 | |
| NI | 6 | 1.4 | 0 | 0 | 6 | 1.2 | |
| Income | |||||||
| (minimum wage) | |||||||
| <1 | 222 | 51.4 | 25 | 52.1 | 247 | 51.5 | 0.866 |
| 2 to 3 | 157 | 36.3 | 17 | 35.4 | 174 | 36.2 | |
| >4 | 34 | 7.9 | 5 | 10.4 | 39 | 8.1 | |
| NI | 19 | 4.4 | 1 | 2.1 | 20 | 4.2 | |
| Total | 432 | 100 | 48 | 100 | 480 | 100 | |
| Clinical Features | Group | ||||||
|---|---|---|---|---|---|---|---|
| Diarrheic | Non-Diarrheic | Total | |||||
| N | % | N | % | N | % | p | |
| Fever | |||||||
| No | 8 | 42.1 | 22 | 75.9 | 30 | 62.5 | 0.032 |
| Yes | 11 | 57.9 | 7 | 24.1 | 18 | 37.5 | |
| Vomiting | |||||||
| No | 12 | 63.2 | 28 | 96.6 | 40 | 83.3 | 0.004 |
| Yes | 7 | 36.8 | 1 | 3.4 | 8 | 16.7 | |
| Total | 19 | 100 | 29 | 100 | 48 | 100 | |
| ID | Group | Specie | Coinfection | Frequency |
|---|---|---|---|---|
| AC-121 | Diarrheic | HBoV-3 | Rotavirus | 50% (4/8) |
| AC-280 | Diarrheic | HBoV-1 | ||
| AC-289 | Diarrheic | HBoV-3 | ||
| AC-404 | Diarrheic | HBoV-3 | ||
| AC-270 | Diarrheic | HBoV-3 | Norovirus | 37.5% (3/8) |
| AC-430 | Non-diarrheic | HBoV-3 | ||
| AC-490 | Non-diarrheic | HBoV-2 | ||
| AC-475 | Non-diarrheic | HBoV-2 | Astrovirus | 12.5% (1/8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trindade, F.D.T.B.; Ramos, E.S.F.; Lobo, P.S.; Cardoso, J.F.; Penha Júnior, E.T.; Bezerra, D.A.M.; Neves, M.A.O.; Andrade, J.A.A.; Moraes Silva, M.C.; Mascarenhas, J.D.P.; et al. Epidemiologic and Clinical Characteristics of Human Bocavirus Infection in Children with or without Acute Gastroenteritis in Acre, Northern Brazil. Viruses 2023, 15, 1024. https://doi.org/10.3390/v15041024
Trindade FDTB, Ramos ESF, Lobo PS, Cardoso JF, Penha Júnior ET, Bezerra DAM, Neves MAO, Andrade JAA, Moraes Silva MC, Mascarenhas JDP, et al. Epidemiologic and Clinical Characteristics of Human Bocavirus Infection in Children with or without Acute Gastroenteritis in Acre, Northern Brazil. Viruses. 2023; 15(4):1024. https://doi.org/10.3390/v15041024
Chicago/Turabian StyleTrindade, Fábyla D’ Tácia Brito, Endrya Socorro Foro Ramos, Patrícia Santos Lobo, Jedson Ferreira Cardoso, Edvaldo Tavares Penha Júnior, Delana Andreza Melo Bezerra, Mayara Annanda Oliveira Neves, Jorge Alberto Azevedo Andrade, Monica Cristina Moraes Silva, Joana D’Arc Pereira Mascarenhas, and et al. 2023. "Epidemiologic and Clinical Characteristics of Human Bocavirus Infection in Children with or without Acute Gastroenteritis in Acre, Northern Brazil" Viruses 15, no. 4: 1024. https://doi.org/10.3390/v15041024