
Above-Standard Survival of Hepatocellular Carcinoma as the Final Outcome of Comprehensive Hepatology Care Programs in a Remote HCV-Endemic Area
 ,
,
Abstract
:1. Introduction
2. Patients and Methods
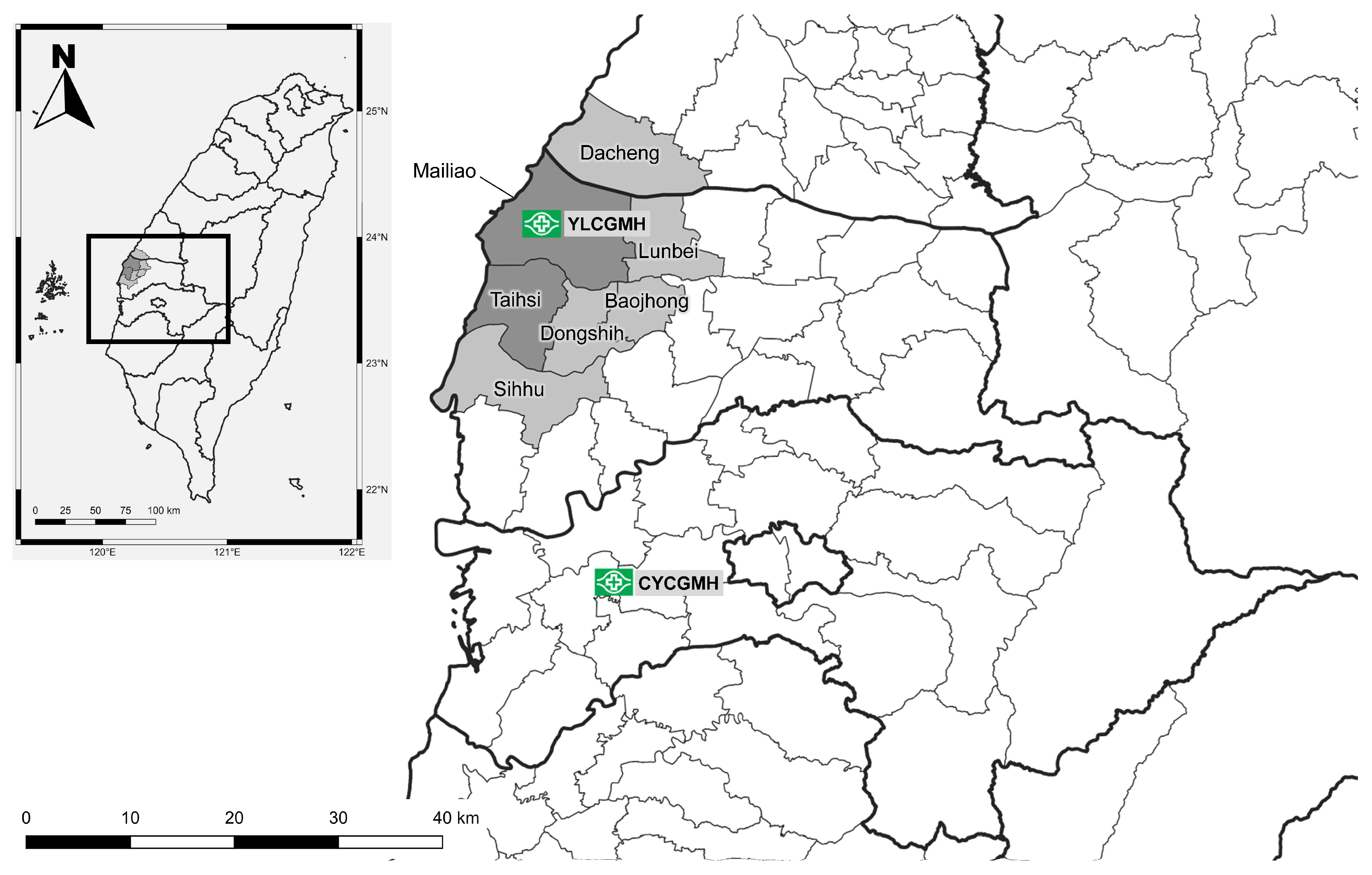
2.1. Background of Study Area
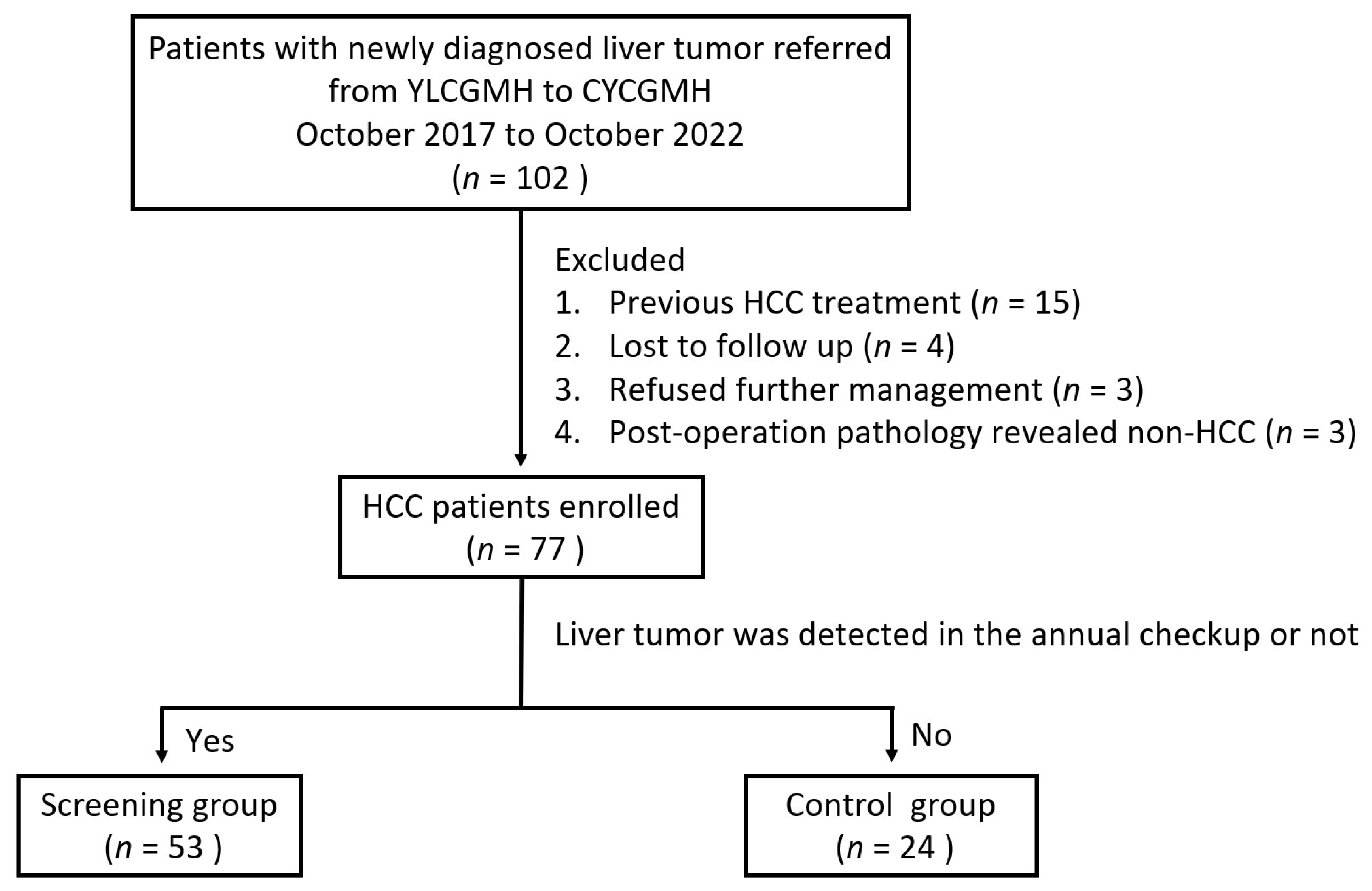
2.2. Patients
2.3. Definition
2.4. Calculation of ALBI Grades
2.5. Screening and Linkage to Accessible Care
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics of HCC Patients in the Screening and Control Groups
3.2. Antiviral Treaments for the Study Cohort
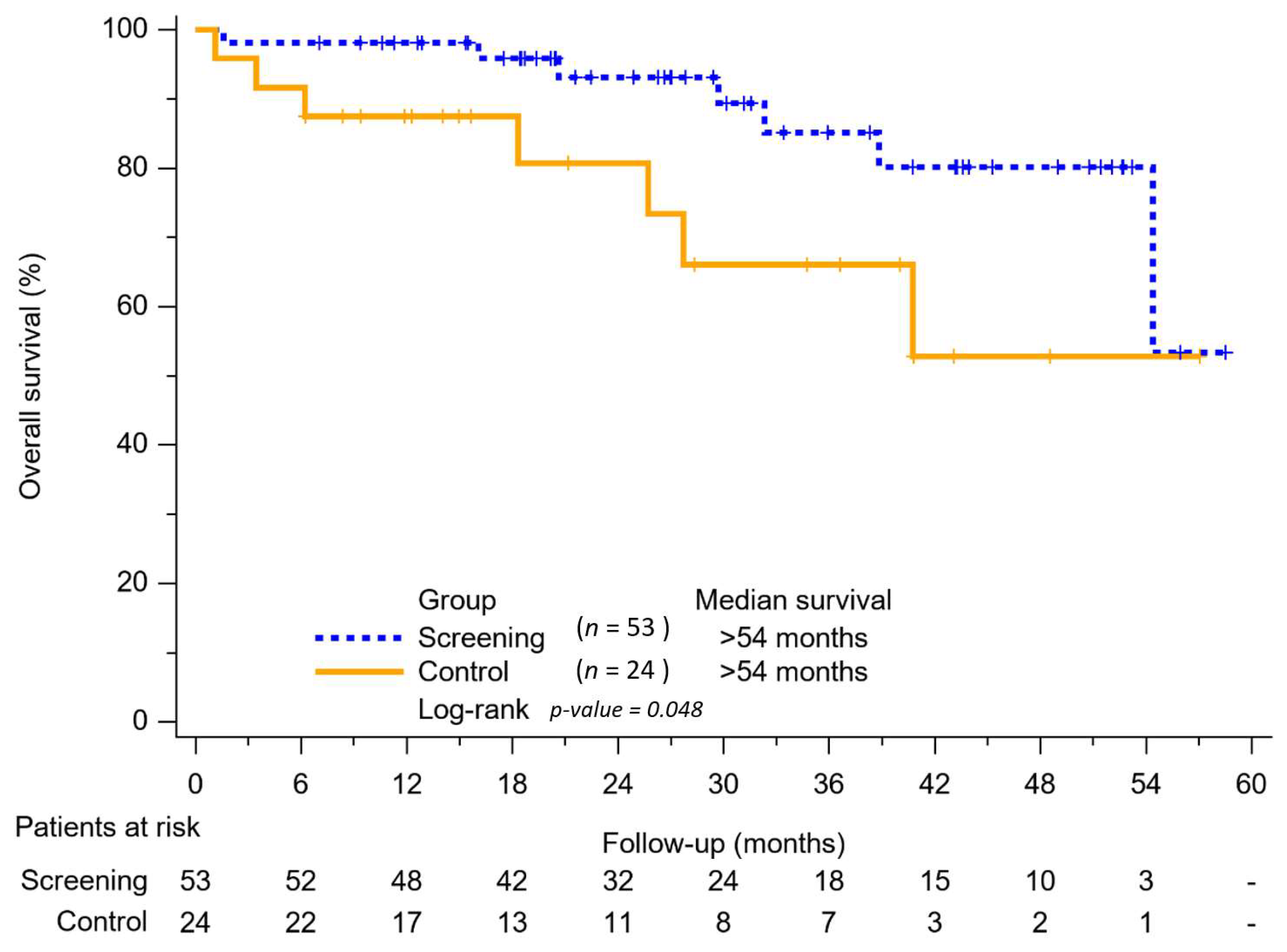
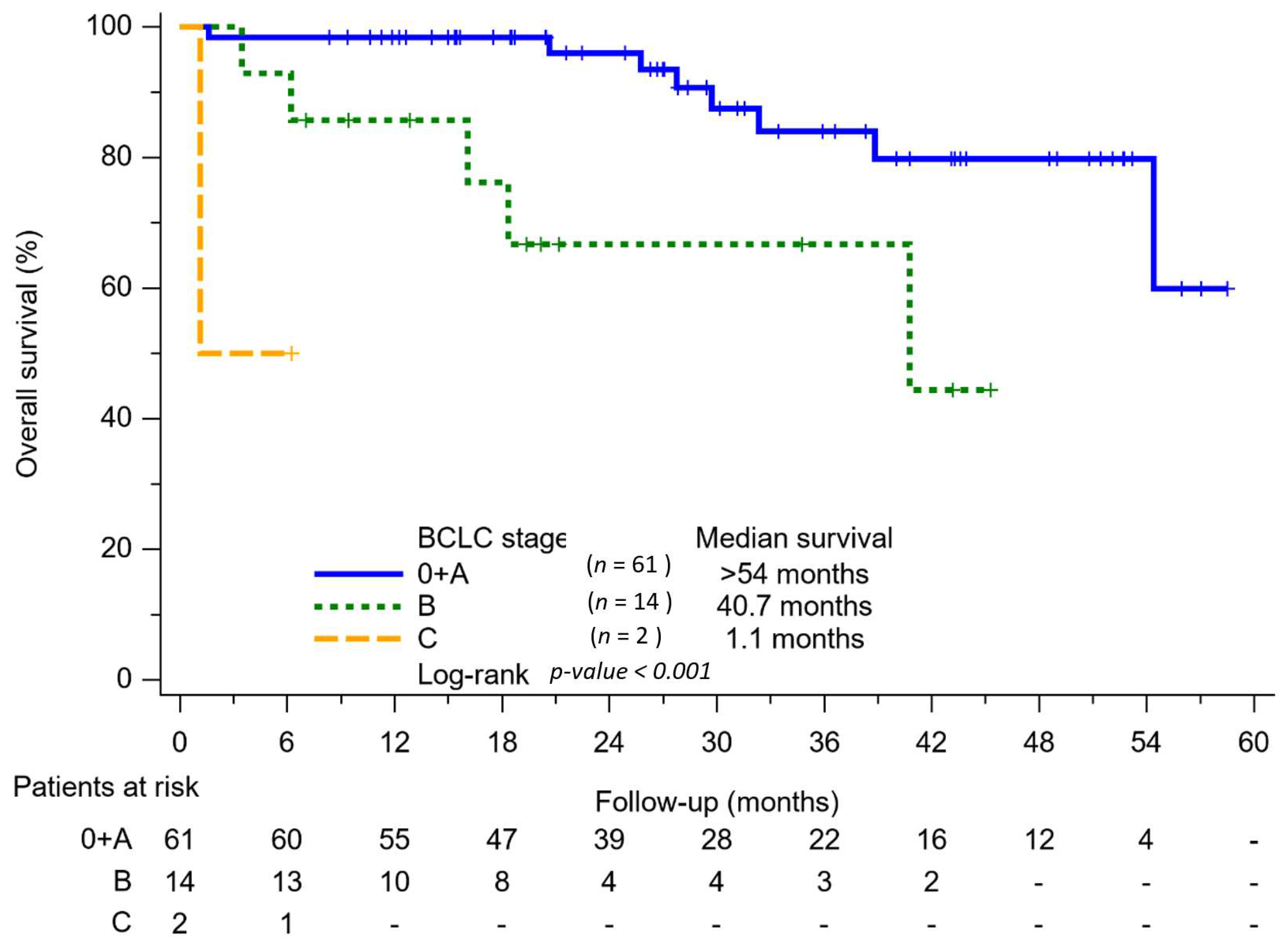
3.3. Survival Outcome of the Study Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Prim. 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Ding, X.X.; Zhu, Q.G.; Zhang, S.M.; Guan, L.; Li, T.; Zhang, L.; Wang, S.Y.; Ren, W.L.; Chen, X.M.; Zhao, J.; et al. Precision medicine for hepatocellular carcinoma: Driver mutations and targeted therapy. Oncotarget 2017, 8, 55715–55730. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.D.; Hainaut, P.; Gores, G.J.; Amadou, A.; Plymoth, A.; Roberts, L.R. A global view of hepatocellular carcinoma: Trends, risk, prevention and management. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Liaw, Y.F.; Tai, D.I.; Chu, C.M.; Lin, D.Y.; Sheen, I.S.; Chen, T.J.; Pao, C.C. Early detection of hepatocellular carcinoma in patients with chronic type B hepatitis. A prospective study. Gastroenterology 1986, 90, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.S. From hepatitis to hepatoma: Lessons from type B viral hepatitis. Science 1993, 262, 369–370. [Google Scholar] [CrossRef]
- Lu, S.N.; Su, W.W.; Yang, S.S.; Chang, T.T.; Cheng, K.S.; Wu, J.C.; Lin, H.H.; Wu, S.S.; Lee, C.M.; Changchien, C.S.; et al. Secular trends and geographic variations of hepatitis B virus and hepatitis C virus-associated hepatocellular carcinoma in Taiwan. Int. J. Cancer 2006, 119, 1946–1952. [Google Scholar] [CrossRef]
- Yu, M.-L.; Yeh, M.-L.; Tsai, P.-C.; Huang, C.-I.; Huang, J.-F.; Huang, C.-F.; Hsieh, M.-H.; Liang, P.-C.; Lin, Y.-H.; Hsieh, M.-Y. Huge gap between clinical efficacy and community effectiveness in the treatment of chronic hepatitis C: A nationwide survey in Taiwan. Medicine 2015, 94, e690. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Wu, G.H.; Pwu, R.F.; Chen, S.C. Achieving hepatitis C elimination in Taiwan-Overcoming barriers by setting feasible strategies. J. Formos. Med. Assoc. 2018, 117, 1044–1045. [Google Scholar] [CrossRef]
- Kee, K.-M.; Chen, C.-H.; Hu, J.-T.; Huang, Y.-H.; Wang, T.-E.; Chau, G.-Y.; Chen, K.-H.; Chen, Y.-L.; Lin, C.-C.; Hung, C.-F.; et al. Secular Trends of Clinical Characteristics and Survival of Hepatocellular Carcinoma in Taiwan from 2011 to 2019. Viruses 2023, 15, 126. [Google Scholar] [CrossRef]
- Lu, S.N.; Wang, J.H.; Kuo, Y.K.; Kuo, H.L.; Chen, T.M.; Tung, H.D.; Lee, C.M.; Chen, S.C. Predicting the prevalence of antibody to hepatitis C virus (HCV) in a community by the prevalence of elevated levels of alanine aminotransferase: A method to identify areas endemic for HCV. Am. J. Trop. Med. Hyg. 2002, 67, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Su, W.W.; Chen, C.H.; Lin, H.H.; Yang, S.S.; Chang, T.T.; Cheng, K.S.; Wu, J.C.; Wu, S.S.; Lee, C.M.; Changchien, C.S.; et al. Geographic variations of predominantly hepatitis C virus associated male hepatocellular carcinoma townships in Taiwan: Identification of potential high HCV endemic areas. Hepatol. Int. 2009, 3, 537–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shyu, H.J.; Lung, C.C.; Ho, C.C.; Sun, Y.H.; Ko, P.C.; Huang, J.Y.; Pan, C.C.; Chiang, Y.C.; Chen, S.C.; Liaw, Y.P. Geographic patterns of hepatocellular carcinoma mortality with exposure to iron in groundwater in Taiwanese population: An ecological study. BMC Public. Health 2013, 13, 352. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.H.; Yang, P.M.; Huang, G.T.; Lee, H.S.; Sung, J.L.; Sheu, J.C. Estimation of seroprevalence of hepatitis B virus and hepatitis C virus in Taiwan from a large-scale survey of free hepatitis screening participants. J. Formos. Med. Assoc. 2007, 106, 148–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, K.-C.; Lee, C.-Y.; Chang, T.-S.; Hung, C.-H.; Chen, W.-M.; Chen, M.-Y.; Huang, T.-J.; Chiu, W.-N.; Hu, J.-H.; Lin, Y.-C.; et al. Usefulness of quantitative hepatitis B surface antigen testing in hepatitis B community-based screening. J. Formos. Med. Assoc. 2021, 120, 847–853. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.-S.; Chang, K.-C.; Chen, W.-M.; Hsu, N.-T.; Lee, C.-Y.; Lin, Y.-C.; Huang, W.-C.; Chiu, W.-N.; Hu, J.-H.; Huang, T.-J.; et al. Village-to-village screening for hepatitis B and C using quantitative HBsAg and anti-HCV testing with reflex HCV core antigen tests in the remote communities of a resource-rich setting: A population-based prospective cohort study. BMJ Open 2021, 11, e046115. [Google Scholar] [CrossRef]
- Lee, P.L.; Wang, J.H.; Tung, H.D.; Lee, C.M.; Lu, S.N. A higher than expected recovery rate from hepatitis C infection amongst adolescents: A community study in a hepatitis C-endemic township in Taiwan. Trans. R. Soc. Trop. Med. Hyg. 2004, 98, 367–372. [Google Scholar] [CrossRef]
- Hsiao, Y.H.; Chen, W.M.; Chang, C.H.; Chen, M.Y. Future outcomes and health needs of chronic hepatitis C patients after receiving antiviral therapy. J. Adv. Nurs. 2021, 77, 3370–3378. [Google Scholar] [CrossRef]
- Huang, W.C.; Lin, Y.C.; Chen, P.J.; Hsu, N.T.; Tu, C.L.; Chang, T.S.; Hung, C.H.; Kee, K.M.; Chao, W.H.; Lu, S.N. Community-Based Screening for Hepatitis B and C Infectivity Using Two Quantitative Antigens to Identify Endemic Townships. Viruses 2022, 14, 304. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [Green Version]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [PubMed] [Green Version]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach—The ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Raza, S.A.; Clifford, G.M.; Franceschi, S. Worldwide variation in the relative importance of hepatitis B and hepatitis C viruses in hepatocellular carcinoma: A systematic review. Br. J. Cancer 2007, 96, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Beasley, R.P.; Hwang, L.Y.; Lin, C.C.; Chien, C.S. Hepatocellular carcinoma and hepatitis B virus. A prospective study of 22 707 men in Taiwan. Lancet 1981, 2, 1129–1133. [Google Scholar] [CrossRef]
- Chang, M.H.; Chen, C.J.; Lai, M.S.; Hsu, H.M.; Wu, T.C.; Kong, M.S.; Liang, D.C.; Shau, W.Y.; Chen, D.S. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. Taiwan Childhood Hepatoma Study Group. N. Engl. J. Med. 1997, 336, 1855–1859. [Google Scholar] [CrossRef] [Green Version]
- Lu, S.N.; Lee, C.M.; Changchien, C.S.; Chen, C.J. Excess mortality from hepatocellular carcinoma in an HCV-endemic township of an HBV-endemic country (Taiwan). Trans. R. Soc. Trop. Med. Hyg. 1999, 93, 600–602. [Google Scholar] [CrossRef] [PubMed]
- Chuang, W.L.; Yu, M.L.; Dai, C.Y.; Chang, W.Y. Treatment of chronic hepatitis C in southern Taiwan. Intervirology 2006, 49, 99–106. [Google Scholar] [CrossRef] [PubMed]
- Bennett, H.; Waser, N.; Johnston, K.; Kao, J.-H.; Lim, Y.-S.; Duan, Z.-P.; Lee, Y.-J.; Wei, L.; Chen, C.-J.; Sievert, W. A review of the burden of hepatitis C virus infection in China, Japan, South Korea and Taiwan. Hepatol. Int. 2015, 9, 378–390. [Google Scholar] [CrossRef]
- Global prevalence and genotype distribution of hepatitis C virus infection in 2015: A modelling study. Lancet Gastroenterol. Hepatol. 2017, 2, 161–176. [CrossRef] [Green Version]
- Pawlotsky, J.-M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H.; European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- Tien, H.M.; Cheng, T.C.; Lien, H.C.; Yang, K.F.; Shy, C.G.; Chen, Y.L.; Hsu, N.T.; Lu, S.N.; Wang, J.H. Liver Disease Screening and Hepatitis C Virus Elimination in Taiwan Rural Indigenous Townships: Village-By-Village Screening and Linking to Outreach Hepatology Care. Int. J. Environ. Res. Public. Health 2022, 19, 3269. [Google Scholar] [CrossRef]
- Li, W.; Chang, T.S.; Chang, S.Z.; Chen, C.H.; Chen, M.Y. Challenges of transferring rural adults with chronic HCV infection for further HCV RNA confirmation and free DAAs treatment: A success story of the interdisciplinary collaboration approach. BMC Infect. Dis. 2020, 20, 737. [Google Scholar] [CrossRef]
- Singal, A.K.; Singh, A.; Jaganmohan, S.; Guturu, P.; Mummadi, R.; Kuo, Y.F.; Sood, G.K. Antiviral therapy reduces risk of hepatocellular carcinoma in patients with hepatitis C virus-related cirrhosis. Clin. Gastroenterol. Hepatol. 2010, 8, 192–199. [Google Scholar] [CrossRef]
- Yu, M.L.; Lin, S.M.; Chuang, W.L.; Dai, C.Y.; Wang, J.H.; Lu, S.N.; Sheen, I.S.; Chang, W.Y.; Lee, C.M.; Liaw, Y.F. A sustained virological response to interferon or interferon/ribavirin reduces hepatocellular carcinoma and improves survival in chronic hepatitis C: A nationwide, multicentre study in Taiwan. Antivir. Ther. 2006, 11, 985–994. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.K.; Kim, D.Y.; Han, K.H.; Seong, J. Changes in real-life practice for hepatocellular carcinoma patients in the Republic of Korea over a 12-year period: A nationwide random sample study. PLoS ONE 2019, 14, e0223678. [Google Scholar] [CrossRef] [Green Version]
- Wigg, A.J.; Narayana, S.K.; Hartel, G.; Medlin, L.; Pratt, G.; Powell, E.E.; Clark, P.; Davies, J.; Campbell, K.; Toombs, M.; et al. Hepatocellular carcinoma amongst Aboriginal and Torres Strait Islander peoples of Australia. eClinicalMedicine 2021, 36, 100919. [Google Scholar] [CrossRef]
- Wong, R.J.; Kim, D.; Ahmed, A.; Singal, A.K. Patients with hepatocellular carcinoma from more rural and lower-income households have more advanced tumor stage at diagnosis and significantly higher mortality. Cancer 2021, 127, 45–55. [Google Scholar] [CrossRef]
- Sapena, V.; Enea, M.; Torres, F.; Celsa, C.; Rios, J.; Rizzo, G.E.M.; Nahon, P.; Mariño, Z.; Tateishi, R.; Minami, T.; et al. Hepatocellular carcinoma recurrence after direct-acting antiviral therapy: An individual patient data meta-analysis. Gut 2022, 71, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Celsa, C.; Calvaruso, V.; Petta, S.; Cacciola, I.; Cannavò, M.R.; Madonia, S.; Rossi, M.; Magro, B.; Rini, F.; et al. Direct-acting antivirals after successful treatment of early hepatocellular carcinoma improve survival in HCV-cirrhotic patients. J. Hepatol. 2019, 71, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Celsa, C.; Stornello, C.; Giuffrida, P.; Giacchetto, C.M.; Grova, M.; Rancatore, G.; Pitrone, C.; Di Marco, V.; Cammà, C.; Cabibbo, G. Direct-acting antiviral agents and risk of Hepatocellular carcinoma: Critical appraisal of the evidence. Ann. Hepatol. 2022, 27 (Suppl. 1), 100568. [Google Scholar] [CrossRef] [PubMed]
- Singal, A.G.; Rich, N.E.; Mehta, N.; Branch, A.D.; Pillai, A.; Hoteit, M.; Volk, M.; Odewole, M.; Scaglione, S.; Guy, J.; et al. Direct-Acting Antiviral Therapy for Hepatitis C Virus Infection Is Associated With Increased Survival in Patients With a History of Hepatocellular Carcinoma. Gastroenterology 2019, 157, 1253–1263.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 77) | Screening Group (n = 53) | Control Group (n = 24) | p-Value |
|---|---|---|---|---|
| Age, years (mean | 65.7 ± 11.1 | 66 ± 11.0 | 65.3 ± 115 | p = 0.809 |
| Gender | p = 0.994 | |||
| Male, n (%) | 61 (79.2%) | 42 (79.2%) | 19 (79.1%) | |
| Female, n (%) | 16 (20.8%) | 11 (20.8%) | 5 (20.8%) | |
| Residence | p = 0.000 | |||
| Mailiao/Taihsi, n (%) | 66 (85.7%) | 53 (100%) | 13 (54.2%) | |
| Others, n (%) | 11 (14.3) | 0 | 11 (45.8%) | |
| Hepatitis | p = 0.523 | |||
| NBNC, n (%) | 8 (10.3%) | 6 (11.3%) | 2 (8.3%) | |
| HBV, (%) | 15 (19.4%) | 10 (18.8%) | 5 (20.8%) | |
| HCV, n (%) | 41 (53.2%) | 26 (49.0%) | 15 (62.5%) | |
| HBV + HCV, n (%) | 13 (16.8%) | 11 (20.7%) | 2 (8.3%) | |
| Bilirubin (g/dL; median, IQR) | 0.9 (0.6–1.2) | 0.9 (0.6–1.2) | 1.0 (0.6–1.3) | p = 0.466 |
| Albumin (g/dL; median, IQR) | 4.2 (3.9–4.6) | 4.3 (4.1–4.6) | 3.9 (3.4–4.6) | p = 0.040 |
| AST (U/L; median, IQR) | 45.9 (26.0–55.5) | 37.2 (24.5–44.5) | 65.2 (29–77.2) | p = 0.044 |
| ALT (U/L; median, IQR) | 43.5 (21.5–59.0) | 39.9 (21–47.5) | 51.4 (25.2–69.2) | p = 0.140 |
| AFP (ng/mL; median, IQR) | 8.4 (3.6–54.3) | 5.5 (2.8–33.4) | 17.2 (9.6–316.2) | p = 0.07 |
| <20 ng/mL, n (%) | 50 (64.9%) | 37 (69.8%) | 13 (54.1%) | |
| <400 ng/mL, n (%) | 17 (22.0%) | 12 (22.6%) | 5 (20.8%) | |
| >400 ng/mL, n (%) | 10 (12.9%) | 4 (7.5%) | 6 (25.0%) | |
| Child–Pugh grade | p = 0.052 | |||
| A, n (%) | 73 (94.8%) | 52 (98.1%) | 21 (87.5%) | |
| B, n (%) | 4 (5.1%) | 1 (1.8%) | 3 (12.5%) | |
| Albumin–Bilirubib (ALBI) grade | p = 0.031 | |||
| I | 53 (68.8%) | 41 (77.3%) | 12 (50%) | |
| II | 23 (29.8%) | 12 (22.6%) | 11 (45.8%) | |
| III | 1 (1.2%) | - | 1 (4.1%) | |
| Tumor number | p = 0.001 | |||
| Single | 60 (77.9%) | 46 (86.7%) | 14 (58.3%) | |
| Multiple | 17 (22.1%) | 7 (13.2%) | 10 (41.7%) | |
| Tumor size | p = 0.113 | |||
| >2 cm, n (%) | 26 (33.7%) | 18 (34.0%) | 9 (37.5%) | |
| >2.1–5 cm, n (%) | 46 (59.7%) | 33 (62.3%) | 11 (45.8%) | |
| >5 cm, n (%) | 5 (6.4%) | 2 (3.8%) | 4 (16.6%) | |
| Barcelona Clinic Liver Cancer (BCLC) stage | p = 0.028 | |||
| 0, n (%) | 21 (27.2%) | 14 (26.4%) | 7 (29.2%) | |
| A, n (%) | 40 (51.9%) | 32 (60.4%) | 8 (33.3%) | |
| B, n (%) | 14 (18.1%) | 7 (13.2%) | 7 (29.2%) | |
| HBV DNR (+) | 21 | 16 | 5 | p = 0.839 |
| NUC | 21 | 16 | 5 | |
| HCV RNA (+) | 45 | 30 | 15 | p = 0.512 |
| DAA treatment | 33 | 23 | 10 | |
| Peginterferon-based therapy | 9 | 6 | 3 | |
| No treatment | 3 | 1 | 2 | |
| Treatment effect for HCV, n | 45 | 30 | 15 | p = 0.423 |
| SVR (+), n (%) | 37 (88.1%) | 25 (86.2%) | 12 (92.3%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, W.-R.; Huang, H.-L.; Hsu, N.-T.; Huang, T.-J.; Chang, T.-S. Above-Standard Survival of Hepatocellular Carcinoma as the Final Outcome of Comprehensive Hepatology Care Programs in a Remote HCV-Endemic Area. Viruses 2023, 15, 786. https://doi.org/10.3390/v15030786
Cho W-R, Huang H-L, Hsu N-T, Huang T-J, Chang T-S. Above-Standard Survival of Hepatocellular Carcinoma as the Final Outcome of Comprehensive Hepatology Care Programs in a Remote HCV-Endemic Area. Viruses. 2023; 15(3):786. https://doi.org/10.3390/v15030786
Chicago/Turabian StyleCho, Wei-Ru, Hui-Ling Huang, Nien-Tzu Hsu, Tung-Jung Huang, and Te-Sheng Chang. 2023. "Above-Standard Survival of Hepatocellular Carcinoma as the Final Outcome of Comprehensive Hepatology Care Programs in a Remote HCV-Endemic Area" Viruses 15, no. 3: 786. https://doi.org/10.3390/v15030786