
A Testing Campaign Intervention Consisting of Peer-Facilitated Engagement, Point-of-Care HCV RNA Testing, and Linkage to Nursing Support to Enhance Hepatitis C Treatment Uptake among People Who Inject Drugs: The ETHOS Engage Study

 , , ,
on behalf of the ETHOS Engage Study Groupadd
Show full author list
, , ,
on behalf of the ETHOS Engage Study Groupadd
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting, and Participants
2.2. Procedures
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Prevalence and Characteristics of HCV Treatment Initiation at Three Months Post-Enrolment
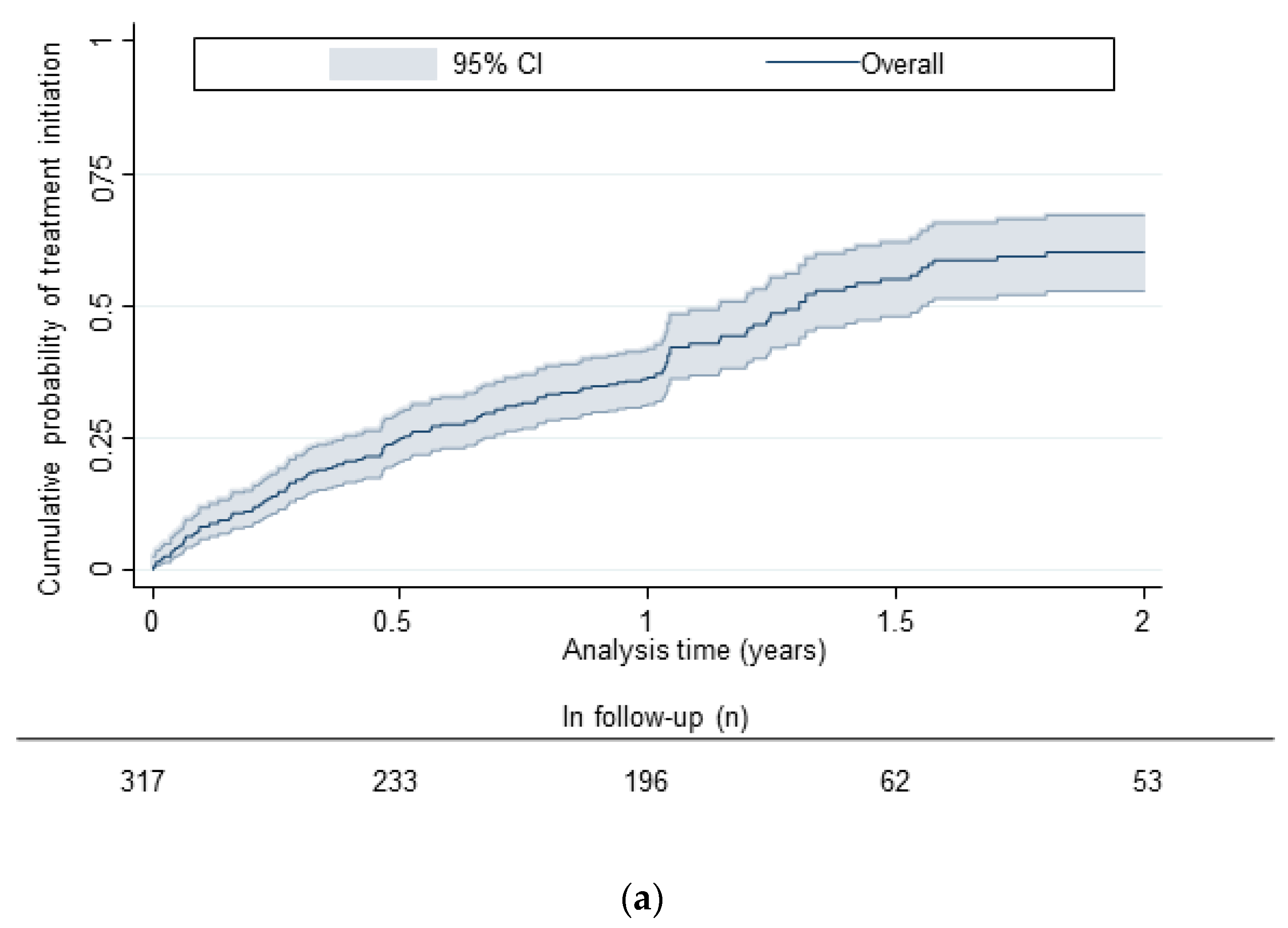
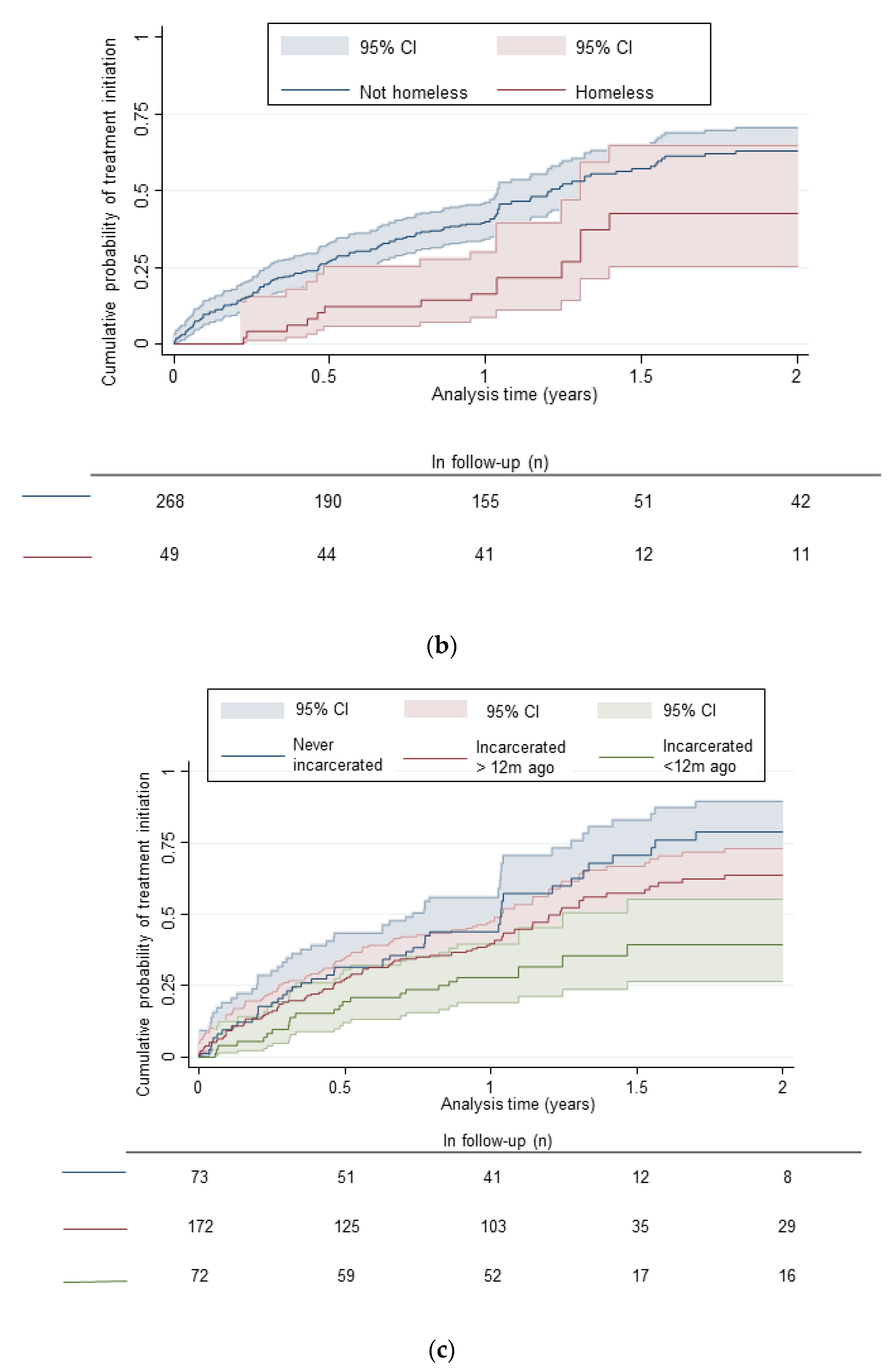
3.3. Factors Associated with Time to HCV Treatment Initiation
3.4. Progress towards Elimination Targets
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016-2021: Towards Ending Viral Hepatitis; World Health Organization: Geneva, Switzerland, 2016.
- Grebely, J.; Larney, S.; Peacock, A.; Colledge, S.; Leung, J.; Hickman, M.; Vickerman, P.; Blach, S.; Cunningham, E.B.; Dumchev, K.; et al. Global, regional, and country-level estimates of hepatitis C infection among people who have recently injected drugs. Addiction 2019, 114, 150–166. [Google Scholar] [CrossRef] [Green Version]
- UNAIDS-Joint United Nations Programme on HIV/AIDS. Health, Rights and Drugs-Harm Reduction, Decriminalization and Zero Discrimination for People Who Use Drugs; UNAIDS: Geneva, Switzerland, 2019. [Google Scholar]
- Hopwood, M.; Treloar, C.; Bryant, J. Hepatitis C and injecting-related discrimination in New South Wales, Australia. Drugs Educ. Prev. Policy 2006, 13, 61–75. [Google Scholar] [CrossRef]
- Harris, M.; Rhodes, T. Hepatitis C treatment access and uptake for people who inject drugs: A review mapping the role of social factors. Harm Reduct. J. 2013, 10, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Hajarizadeh, B.; Grebely, J.; Matthews, G.; Martinello, M.; Dore, G.J. Uptake of direct-acting antiviral treatment for chronic hepatitis C in Australia. J. Viral Hepat. 2017, 25, 640–648. [Google Scholar] [CrossRef]
- Valerio, H.; Alavi, M.; Silk, D.; Treloar, C.; Martinello, M.; Milat, A.; Dunlop, A.; Holden, J.; Henderson, C.; Amin, J.; et al. Progress Towards Elimination of Hepatitis C Infection Among People Who Inject Drugs in Australia: The ETHOS Engage Study. Clin. Infect. Dis. 2020, 73, e69–e78. [Google Scholar] [CrossRef]
- Valerio, H.; Alavi, M.; Conway, A.; Silk, D.; Treloar, C.; Martinello, M.; Milat, A.; Dunlop, A.; Murray, C.; Henderson, C.; et al. Declining Prevalence of Current HCV Infection and Increased Treatment Uptake Among People Who Inject Drugs: The ETHOS Engage Study. Int. J. Drug Policy 2022, 105, 103706. [Google Scholar] [CrossRef]
- Bajis, S.; Dore, G.J.; Hajarizadeh, B.; Cunningham, E.B.; Maher, L.; Grebely, J. Interventions to enhance testing, linkage to care and treatment uptake for hepatitis C virus infection among people who inject drugs: A systematic review. Int. J. Drug Policy 2017, 47, 34–46. [Google Scholar] [CrossRef]
- Oru, E.; Trickey, A.; Shirali, R.; Kanters, S.; Easterbrook, P. Decentralisation, integration, and task-shifting in hepatitis C virus infection testing and treatment: A global systematic review and meta-analysis. Lancet Glob. Health 2021, 9, e431–e445. [Google Scholar] [CrossRef]
- Bajis, S.; Grebely, J.; Hajarizadeh, B.; Applegate, T.; Marshall, A.D.; Ellen Harrod, M.; Byrne, J.; Bath, N.; Read, P.; Edwards, M.; et al. Hepatitis C virus testing, liver disease assessment and treatment uptake among people who inject drugs pre- and post-universal access to direct-acting antiviral treatment in Australia: The LiveRLife study. J. Viral Hepat. 2020, 27, 281–293. [Google Scholar] [CrossRef]
- Gasbarrini, N.; Dubravić, D.; Combs, L.; Dišković, A.; Ankiersztejn-Bartczak, M.; Colaiaco, F.; Wawer, I.; Wysocki, P.; Rosińska, M.; Marzec-Boguslawska, A.; et al. Increasing integrated testing in community settings through interventions for change, including the Spring European Testing Week. BMC Infect. Dis. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, E.; Wheeler, A.; Hajarizadeh, B.; French, C.; Roche, R.; Marshall, A.; Fontaine, G.; Conway, A.; Valencia, B.M.; Bajis, S.; et al. Interventions to enhance testing and linkage to treatment for hepatitis C infection: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2021, 7, 426–445. [Google Scholar] [CrossRef]
- EASL. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef] [PubMed]
- Valerio, H.; Alavi, M.; Law, M.; Tillakeratne, S.; Amin, J.; Janjua, N.Z.; Krajden, M.; George, J.; Matthews, G.V.; Hajarizadeh, B.; et al. High hepatitis C treatment uptake among people with recent drug dependence in New South Wales, Australia. J. Hepatol. 2021, 74, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Bradley, K.A.; McDonell, M.B.; Bush, K.; Kivlahan, D.R.; Diehr, P.; Fihn, S.D. The AUDIT Alcohol Consumption Questions. Alcohol. Clin. Exp. Res. 1998, 22, 1842. [Google Scholar] [CrossRef]
- Mauss, S.; Pol, S.; Buti, M.; Duffell, E.; Gore, C.; Lazarus, J.V.; Logtenberg-van der Grient, H.L.; Lundgren, J.; Mozalevskis, A.; Raben, D.; et al. Late presentation of chronic viral hepatitis for medical care: A consensus definition. BMC Med. 2017, 15, 92. [Google Scholar] [CrossRef] [Green Version]
- Yousafzai, M.T.; Alavi, M.; Valerio, H.; Hajarizadeh, B.; Grebely, J.; Dore, G.J. Time to hepatitis C RNA testing and treatment in the era of direct-acting antiviral therapy among people with hepatitis C in New South Wales, Australia. Viruses. 2022, 14, 1496. [Google Scholar] [CrossRef]
- Grebely, J.; Gilliver, R.; Mcnaughton, T.; Henderson, C.; Hadlow, B.; Molloy, K.; Tillakeratne, S.; Pepolim, L.; Harrod, M.E.; Dore, G.J.; et al. Point-of-care HCV RNA testing, linkage to nursing care, and peer-supported engagement and delivery to enhance HCV treatment among people with recent injecting drug use at a community-led needle and syringe program: The TEMPO pilot study. In Proceedings of the International Conference on Hepatitis Care in Substance Users, Virtual conference, 13–15 October 2021. [Google Scholar]
- Macisaac, M.B.; Whitton, B.; Anderson, J.; Hornung, M.; Elmore, K.; Pemberton, D.; Penn, M.; Hellard, M.; Stoove, M.; Wilson, D.; et al. Rapid point of care HCV testing allows high throughout HCV screening and rapid treatment uptake among PWID attending a medically supervised injecting room. In Proceedings of the International Conference on Hepatitis Care in Substance Users, Virtual conference, 13–15 October 2021. [Google Scholar]
- O’Loan, J.; Young, M.; Mooney, M.; O’Flynn, M. Same day delivery! HCV point of care testing in South East Queensland marginalised communities simplifies diagnosis and ensures rapid access to treatment. In Proceedings of the International Conference on Hepatitis Care in Substance Users, Virtual conference, 13–15 October 2021. [Google Scholar]
- Ralton, L.; McCartney, E.M.; Ferguson, C.; Dawe, J.; Richmond, J.; Tse, E.; Wigg, A.; Cock, V.; Rees, T.; Sha, D. Prompt-point of care testing for hepatitis C in the priority settings of mental health, prisons and drug & alcohol facilities. In Proceedings of the International Conference on Hepatitis Care in Substance Users, Virtual conference, 13–15 October 2021. [Google Scholar]
- Bajis, S.; Maher, L.; Treloar, C.; Hajarizadeh, B.; Lamoury, F.M.J.; Mowat, Y.; Hajarizadeh, B.; Martinello, M.; Adey, S.; Read, P.; et al. Acceptability and preferences of point-of-care finger-stick whole-blood and venepuncture hepatitis C virus testing among people who inject drugs in Australia. Int. J. Drug Policy 2018, 61, 23–30. [Google Scholar] [CrossRef]
- Bajis, S.; Grebely, J.; Cooper, L.; Smith, J.; Owen, G.; Chudleigh, A.; Hajarizadeh, B.; Martinello, M.; Adey, S.; Read, P.; et al. Hepatitis C virus testing, liver disease assessment and direct-acting antiviral treatment uptake and outcomes in a service for people who are homeless in Sydney, Australia: The LiveRLife homelessness study. J. Viral Hepat. 2019, 26, 969–979. [Google Scholar] [CrossRef]
- Madden, A.; Hopwood, M.; Neale, J.; Treloar, C. Beyond interferon side effects: What residual barriers exist to DAA hepatitis C treatment for people who inject drugs? PLoS ONE 2018, 13, 1–10. [Google Scholar] [CrossRef]
- Paisi, M.; Crombag, N.; Burns, L.; Bogaerts, A.; Withers, L.; Bates, L.; Crowley, D.; Witton, R.; Shawe, J. Barriers and facilitators to hepatitis C screening and treatment for people with lived experience of homelessness: A mixed-methods systematic review. Health Expect. 2021, 25, 48–60. [Google Scholar] [CrossRef]
- Stone, J.; Artenie, A.; Hickman, M.; Martin, N.K.; Degenhardt, L.; Fraser, H.; Vickerman, P. The contribution of unstable housing to HIV and hepatitis C virus transmission among people who inject drugs globally, regionally, and at country level: A modelling study. Lancet Public Health 2022, 7, e136–e145. [Google Scholar] [CrossRef]
- Rolfe, S.; Garnham, L.; Godwin, J.; Anderson, I.; Seaman, P.; Donaldson, C. Housing as a social determinant of health and wellbeing: Developing an empirically-informed realist theoretical framework. BMC Public Health 2020, 20, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Valencia, J.; Lazarus, J.V.; Ceballos, F.C.; Troya, J.; Cuevas, G.; Resino, S.; Torres-Macho, J.; Ryan, P. Differences in the hepatitis C virus cascade of care and time to initiation of therapy among vulnerable subpopulations using a mobile unit as point-of-care. Liver Int. 2021, 42, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Ryan, P.; Valencia, J.; Cuevas, G.; Torres-Macho, J.; Troya, J.; Pueyo, Á.; Muñoz-Gómez, M.J.; Muñoz-Rivas, N.; Vázquez-Morón, S.; Martinez, I.; et al. Detection of active hepatitis C in a single visit and linkage to care among marginalized people using a mobile unit in Madrid, Spain. Int. J. Drug Policy 2021, 96, 103424. [Google Scholar] [CrossRef]
- Marshall, A.D.; Conway, A.; Cunningham, E.B.; Valerio, H.; Silk, D.; Alavi, M.; Wade, A.; Lam, T.; Zohrab, K.; Dunlop, A.; et al. Willingness of people who inject drugs to participate in a randomised controlled trial involving financial incentives to initiate hepatitis C treatment. Drug Alcohol Depend. 2022, 235, 109438. [Google Scholar] [CrossRef]
- Valerio, H.; Alavi, M.; Law, M.; McManus, H.; Tillakeratne, S.; Bajis, S.; Martinello, M.; Matthews, G.V.; Amin, J.; Janjua, N.Z.; et al. Opportunities to Enhance Linkage to Hepatitis C Care Among Hospitalized People With Recent Drug Dependence in New South Wales, Australia: A Population-based Linkage Study. Clin. Infect. Dis. 2021, 73, 2037–2044. [Google Scholar] [CrossRef]
- Hajarizadeh, B.; Grebely, J.; Byrne, M.; Marks, P.; Amin, J.; McManus, H.; Butler, T.; Cunningham, E.; Vickerman, P.; Martin, N.; et al. Evaluation of hepatitis C treatment-as-prevention within Australian prisons (SToP-C): A prospective cohort study. Lancet Gastroenterol. Hepatol. 2021, 6, 533–546. [Google Scholar] [CrossRef]
- Treloar, C.; Schroeder, S.; Lafferty, L.; Marshall, A.; Drysdale, K.; Higgs, P.; Baldry, E.; Stoove, M.; Dietze, P. Structural competency in the post-prison period for people who inject drugs: A qualitative case study. Int. J. Drug Policy 2021, 95, 103261. [Google Scholar] [CrossRef]
- Akiyama, M.J.; Columbus, D.; MacDonald, R.; Jordan, A.O.; Schwartz, J.; Litwin, A.H.; Eckhardt, B.; Carmody, E. Linkage to hepatitis C care after incar-ceration in jail: A prospective, single arm clinical trial. BMC Infect. Dis. 2019, 19, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Franco-Paredes, C.; Ghandnoosh, N.; Latif, H.; Krsak, M.; Henao-Martinez, A.F.; Robins, M.; Barahona, L.V.; Poeschla, E.M. Decarceration and community re-entry in the COVID-19 era. Lancet Infect. Dis. 2021, 21, e11–e16. [Google Scholar] [CrossRef]
- Jain, M.K.; Thamer, M.; Therapondos, G.; Shiffman, M.L.; Kshirsagar, O.; Clark, C.; Wong, R.J. Has Access to Hepatitis C Virus Therapy Changed for Patients With Mental Health or Substance Use Disorders in the Direct-Acting-Antiviral Period? Hepatology 2019, 69, 51–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, M.; Rhodes, T.; Martin, A. Taming systems to create enabling environments for HCV treatment: Negotiating trust in the drug and alcohol setting. Soc. Sci. Med. 2013, 83, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Henderson, C.; Madden, A.; Kelsall, J. Beyond the willing & the waiting—The role of peer-based approaches in hepatitis C diagnosis & treatment. Int. J. Drug Policy 2017, 50, 111–115. [Google Scholar] [CrossRef]
- Treloar, C.; Rance, J.; Bath, N.; Everingham, H.; Micallef, M.; Day, C.; Hazelwood, S.; Grebely, J.; Dore, G.J. Evaluation of two community-controlled peer support services for assessment and treatment of hepatitis C virus infection in opioid substitution treatment clinics: The ETHOS study, Australia. Int. J. Drug Policy 2015, 26, 992–998. [Google Scholar] [CrossRef]
- Marshall, A.D.; Grebely, J.; Dore, G.J.; Treloar, C. Barriers and facilitators to engaging in hepatitis C management and DAA therapy among general practitioners and drug and alcohol specialists—The practitioner experience. Drug Alcohol Depend. 2020, 206, 107705. [Google Scholar] [CrossRef]
- O’Flynn, M.; Young, M.; White, S.; Grimstrup, D.; Mooney, M.; O’Loan, J. HCV Blitzing in Corrections with Just a Fingerstick. In Proceedings of the International Network on Health and Hepatitis in Substance Users Conference, Virtual conference, 13–15 October 2021. [Google Scholar]
- DeBeck, K.; Cheng, T.; Montaner, J.S.; Beyrer, C.; Elliott, R.; Sherman, S.; Wood, E.; Baral, S. HIV and the criminalisation of drug use among people who inject drugs: A systematic review. Lancet HIV 2017, 4, e357–e374. [Google Scholar] [CrossRef]
- Aldridge, R.W.; Story, A.; Hwang, S.W.; Nordentoft, M.; Luchenski, S.A.; Hartwell, G.; Tweed, E.J.; Lewer, D.; Katikireddi, S.V.; Hayward, A.C. Morbidity and mortality in homeless individuals, prisoners, sex workers, and individuals with substance use disorders in high-income countries: A systematic review and meta-analysis. Lancet 2018, 391, 241–250. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Current HCV Infection | No Treatment Initiation within Three Months or Lost to Follow-Up | Initiated Treatment Three Months Post Diagnosis | ||
|---|---|---|---|---|---|
| n (col%) | n (% of Current HCV Infection) | n (% of Current HCV Infection) | p Value | ||
| Total (N) | 317 (100%) | 270 (85%) | 47 (15%) | ||
| Age at enrolment | <45 | 184 (58%) | 159 (86%) | 25 (14%) | |
| ≥45 | 133 (42%) | 111 (83%) | 22 (17%) | 0.465 | |
| Gender | Male | 205 (65%) | 177 (86%) | 28 (14%) | |
| Female | 110 (35%) | 91 (83%) | 19 (17%) | ||
| Other | 2 (1%) | 2 (100%) | 0 (0%) | 0.580 | |
| Aboriginal or Torres Strait Islander | No | 241 (76%) | 204 (85%) | 37 (15%) | |
| Yes | 76 (24%) | 66 (87%) | 10 (13%) | 0.639 | |
| Homeless | No | 268 (85%) | 223 (83%) | 45 (17%) | |
| Yes | 49 (15%) | 47 (96%) | 2 (4%) | 0.021 | |
| Currently receiving OAT | No | 98 (31%) | 80 (82%) | 18 (18%) | |
| Yes | 219 (69%) | 190 (87%) | 29 (13%) | 0.235 | |
| Incarceration history | Never | 73 (23%) | 59 (81%) | 14 (19%) | |
| More than 12 months ago | 172 (54%) | 145 (84%) | 27 (16%) | ||
| In last 12 months | 72 (23%) | 66 (92%) | 6 (8%) | 0.165 | |
| Recency of injecting | More than a month ago | 96 (30%) | 81 (84%) | 15 (16%) | |
| Within last month | 221 (70%) | 189 (86%) | 32 (14%) | 0.792 | |
| Hazardous alcohol consumption † | No | 188 (59%) | 160 (85%) | 28 (15%) | |
| Yes | 127 (40%) | 108 (85%) | 19 (15%) | 0.839 | |
| Fibrosis -Fibroscan result (kpa) | <7.0 | 184 (58%) | 154 (84%) | 30 (16%) | |
| >7.0 | 115 (36%) | 101 (88%) | 14 (12%) | ||
| Unknown | 18 (6%) | 15 (83%) | 3 (17%) | 0.604 | |
| No | 61 (19%) | 56 (92%) | 5 (8%) | ||
| Diagnosed with HCV prior to study | Yes, never treated | 204 (64%) | 173 (85%) | 31 (15%) | |
| Yes, ever treated | 52 (16%) | 41 (79%) | 11 (21%) | 0.150 | |
| Characteristic | Person-Years Observation | Incidence Rate | Unadjusted Hazard Ratio (95% CI) | Adjusted Hazard Ratio (95%CI) | |
|---|---|---|---|---|---|
| Age at enrolment | Year | 1.30 (0.95–1.78) | 1.00 (0.98–1.01) | ||
| Gender | Male | 199 | 0.48 | Ref | |
| Female | 104 | 0.54 | 1.12 (0.80–1.55) | ||
| Transgender | 1 | 2.00 | 2.88 (0.71–11.73) | ||
| Aboriginal or Torres Strait Islander | No | 226 | 0.55 | Ref | Ref |
| Yes | 79 | 0.37 | 0.67 (0.45–1.00) | 0.66 (0.44–0.99) | |
| Homeless | No | 247 | 0.57 | Ref | Ref |
| Yes | 57 | 0.23 | 0.41 (0.23–0.72) | 0.40 (0.23–0.71) | |
| Currently receiving OAT | No | 94 | 0.41 | Ref | |
| Yes | 211 | 0.54 | 1.29 (0.90–1.86) | ||
| Incarceration history | Never | 64 | 0.70 | Ref | Ref |
| More than 12 months ago | 164 | 0.52 | 0.77 (0.54–1.10) | 0.83 (0.58–1.19) | |
| In last 12 months | 77 | 0.30 | 0.44 (0.27–0.73) | 0.46 (0.28–0.76) | |
| Recency of injecting | More than a month ago | 98 | 0.58 | Ref | |
| Within last month | 206 | 0.47 | 0.84 (0.61–1.17) | ||
| Hazardous alcohol consumption † | No | 183 | 0.49 | Ref | |
| Yes | 120 | 0.52 | 1.07 (0.78–1.48) | ||
| Fibrosis-Fibroscan result (kpa) | <7.0 | 171 | 0.54 | Ref | |
| >7.0 | 116 | 0.46 | 0.84 (0.60–1.17) | ||
| Unknown | 18 | 0.44 | 0.82 (0.40–1.69) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conway, A.; Valerio, H.; Alavi, M.; Silk, D.; Treloar, C.; Hajarizadeh, B.; Marshall, A.D.; Martinello, M.; Milat, A.; Dunlop, A.; et al. A Testing Campaign Intervention Consisting of Peer-Facilitated Engagement, Point-of-Care HCV RNA Testing, and Linkage to Nursing Support to Enhance Hepatitis C Treatment Uptake among People Who Inject Drugs: The ETHOS Engage Study. Viruses 2022, 14, 1555. https://doi.org/10.3390/v14071555
Conway A, Valerio H, Alavi M, Silk D, Treloar C, Hajarizadeh B, Marshall AD, Martinello M, Milat A, Dunlop A, et al. A Testing Campaign Intervention Consisting of Peer-Facilitated Engagement, Point-of-Care HCV RNA Testing, and Linkage to Nursing Support to Enhance Hepatitis C Treatment Uptake among People Who Inject Drugs: The ETHOS Engage Study. Viruses. 2022; 14(7):1555. https://doi.org/10.3390/v14071555
Chicago/Turabian StyleConway, Anna, Heather Valerio, Maryam Alavi, David Silk, Carla Treloar, Behzad Hajarizadeh, Alison D. Marshall, Marianne Martinello, Andrew Milat, Adrian Dunlop, and et al. 2022. "A Testing Campaign Intervention Consisting of Peer-Facilitated Engagement, Point-of-Care HCV RNA Testing, and Linkage to Nursing Support to Enhance Hepatitis C Treatment Uptake among People Who Inject Drugs: The ETHOS Engage Study" Viruses 14, no. 7: 1555. https://doi.org/10.3390/v14071555