
Real-World Safety, Effectiveness, and Patient-Reported Outcomes in Patients with Chronic Hepatitis C Virus Infection Treated with Glecaprevir/Pibrentasvir: Updated Data from the German Hepatitis C-Registry (DHC-R)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Outcomes and Endpoints
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
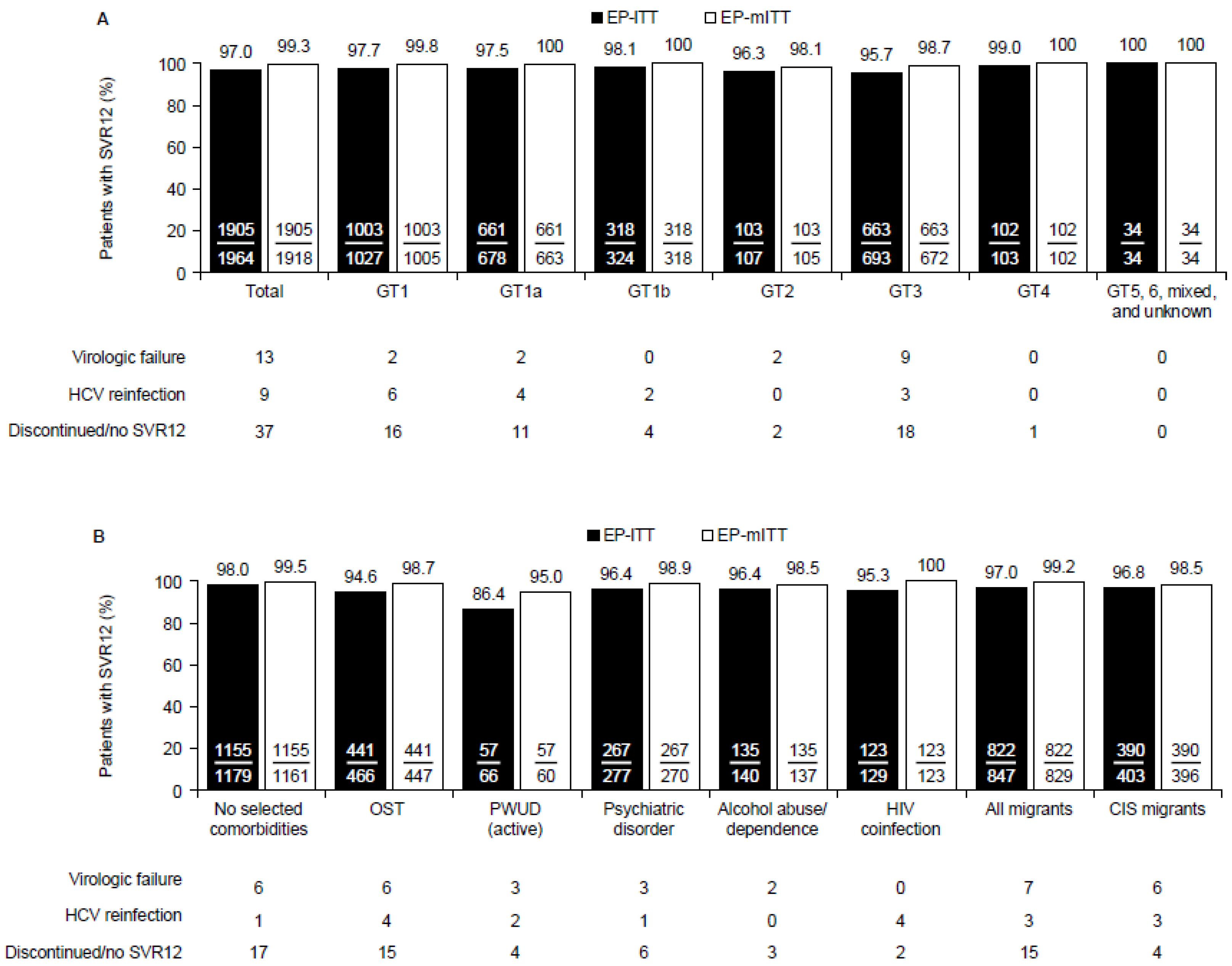
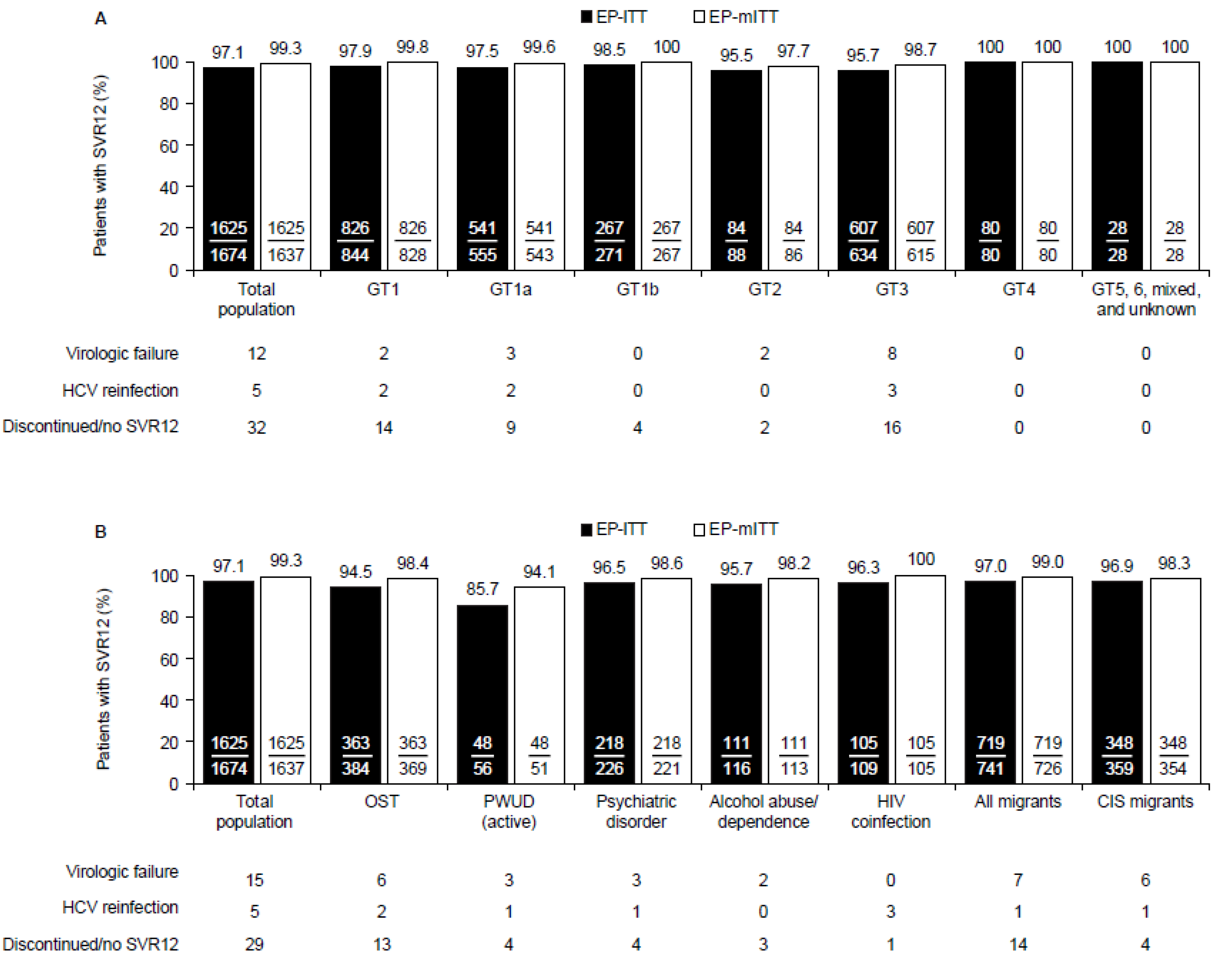
3.2. Effectiveness
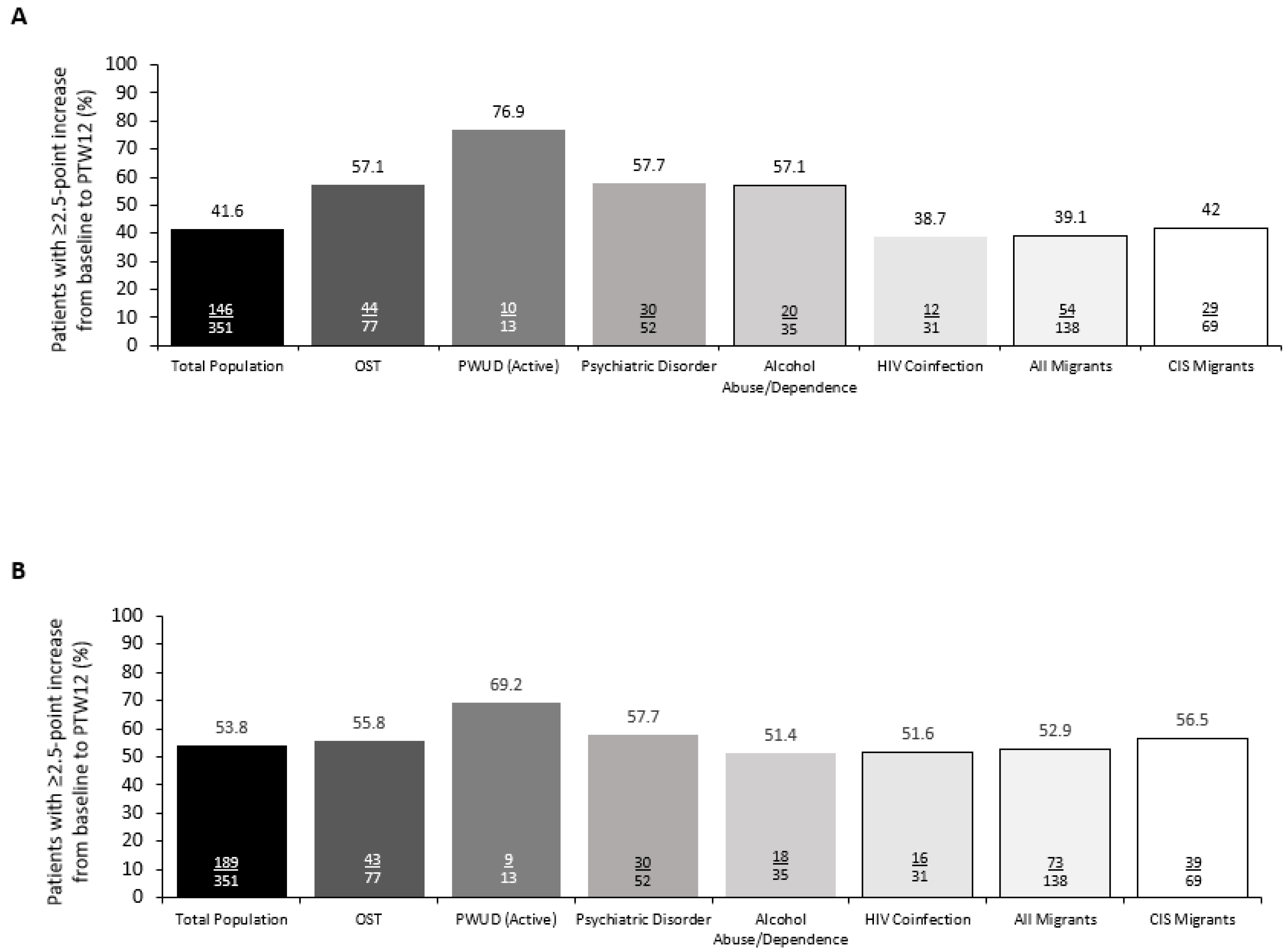
3.3. Patient-Reported Outcomes
3.4. Adherence
3.5. Safety
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections. 2021. Available online: https://www.who.int/publications/i/item/9789240027077 (accessed on 3 May 2022).
- Polaris Observatory. German HCV Infections. Available online: https://cdafound.org/dashboard/polaris/dashboard.html (accessed on 11 May 2021).
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Available online: https://apps.who.int/iris/handle/10665/246177 (accessed on 3 May 2022).
- World Health Organization. Guidelines for the Care and Treatment of Persons Diagnosed with Chronic Hepatitis C Virus Infection. Available online: https://www.who.int/publications/i/item/9789241550345 (accessed on 3 May 2022).
- European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef]
- American Association for the Study of Liver Diseases. AASLD HCV Guidelines. Available online: https://www.hcvguidelines.org (accessed on 7 June 2021).
- Gamkrelidze, I.; Pawlotsky, J.M.; Lazarus, J.V.; Feld, J.J.; Zeuzem, S.; Bao, Y.; Gabriela Pires Dos Santos, A.; Sanchez Gonzalez, Y.; Razavi, H. Progress towards hepatitis C virus elimination in high-income countries: An updated analysis. Liver Int. 2021, 41, 456–463. [Google Scholar] [CrossRef]
- Madden, A.; Hopwood, M.; Neale, J.; Treloar, C. Beyond cure: Patient reported outcomes of hepatitis C treatment among people who inject drugs in Australia. Harm Reduct. J. 2018, 15, 42. [Google Scholar] [CrossRef]
- AbbVie. Maviret (Glecaprevir/Pibrentasvir) Summary of Product Characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/maviret-epar-product-information_en.pdf (accessed on 20 March 2020).
- Asselah, T.; Kowdley, K.V.; Zadeikis, N.; Wang, S.; Hassanein, T.; Horsmans, Y.; Colombo, M.; Calinas, F.; Aguilar, H.; de Ledinghen, V.; et al. Efficacy of Glecaprevir/Pibrentasvir for 8 or 12 Weeks in Patients With Hepatitis C Virus Genotype 2, 4, 5, or 6 Infection Without Cirrhosis. Clin. Gastroenterol. Hepatol. 2018, 16, 417–426. [Google Scholar] [CrossRef]
- Asselah, T.; Lee, S.S.; Yao, B.B.; Nguyen, T.; Wong, F.; Mahomed, A.; Lim, S.G.; Abergel, A.; Sasadeusz, J.; Gane, E.; et al. Efficacy and safety of glecaprevir/pibrentasvir in patients with chronic hepatitis C virus genotype 5 or 6 infection (ENDURANCE-5,6): An open-label, multicentre, phase 3b trial. Lancet Gastroenterol. Hepatol. 2019, 4, 45–51. [Google Scholar] [CrossRef]
- Brown, R.S., Jr.; Buti, M.; Rodrigues, L.; Chulanov, V.; Chuang, W.L.; Aguilar, H.; Horvath, G.; Zuckerman, E.; Carrion, B.R.; Rodriguez-Perez, F.; et al. Glecaprevir/pibrentasvir for 8 weeks in treatment-naive patients with chronic HCV genotypes 1-6 and compensated cirrhosis: The EXPEDITION-8 trial. J. Hepatol. 2020, 72, 441–449. [Google Scholar] [CrossRef] [Green Version]
- Forns, X.; Lee, S.S.; Valdes, J.; Lens, S.; Ghalib, R.; Aguilar, H.; Felizarta, F.; Hassanein, T.; Hinrichsen, H.; Rincon, D.; et al. Glecaprevir plus pibrentasvir for chronic hepatitis C virus genotype 1, 2, 4, 5, or 6 infection in adults with compensated cirrhosis (EXPEDITION-1): A single-arm, open-label, multicentre phase 3 trial. Lancet Infect. Dis. 2017, 17, 1062–1068. [Google Scholar] [CrossRef]
- Gane, E.; Poordad, F.; Zadeikis, N.; Valdes, J.; Lin, C.W.; Liu, W.; Asatryan, A.; Wang, S.; Stedman, C.; Greenbloom, S.; et al. Safety and Pharmacokinetics of Glecaprevir/Pibrentasvir in Adults With Chronic Genotype 1-6 Hepatitis C Virus Infections and Compensated Liver Disease. Clin. Infect. Dis. 2019, 69, 1657–1664. [Google Scholar] [CrossRef] [Green Version]
- Poordad, F.; Pol, S.; Asatryan, A.; Buti, M.; Shaw, D.; Hézode, C.; Felizarta, F.; Reindollar, R.W.; Gordon, S.C.; Pianko, S.; et al. Glecaprevir/Pibrentasvir in patients with hepatitis C virus genotype 1 or 4 and past direct-acting antiviral treatment failure. Hepatology 2018, 67, 1253–1260. [Google Scholar] [CrossRef]
- Hellard, M.; Sacks-Davis, R.; Gold, J. Hepatitis C treatment for injection drug users: A review of the available evidence. Clin. Infect. Dis. 2009, 49, 561–573. [Google Scholar] [CrossRef] [Green Version]
- Mehta, S.H.; Genberg, B.L.; Astemborski, J.; Kavasery, R.; Kirk, G.D.; Vlahov, D.; Strathdee, S.A.; Thomas, D.L. Limited uptake of hepatitis C treatment among injection drug users. J. Community Health 2008, 33, 126–133. [Google Scholar] [CrossRef]
- Norton, B.L.; Akiyama, M.J.; Zamor, P.J.; Litwin, A.H. Treatment of Chronic Hepatitis C in Patients Receiving Opioid Agonist Therapy: A Review of Best Practice. Infect. Dis. Clin. N. Am. 2018, 32, 347–370. [Google Scholar] [CrossRef]
- Puoti, M.; Foster, G.R.; Wang, S.; Mutimer, D.; Gane, E.; Moreno, C.; Chang, T.T.; Lee, S.S.; Marinho, R.; Dufour, J.F.; et al. High SVR12 with 8-week and 12-week glecaprevir/pibrentasvir therapy: An integrated analysis of HCV genotype 1-6 patients without cirrhosis. J. Hepatol. 2018, 69, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Huppe, D.; Serfert, Y.; Buggisch, P.; Mauss, S.; Boker, K.H.W.; Muller, T.; Klinker, H.; Gunther, R.; Berg, T.; Cornberg, M.; et al. 4 years of direct-acting antivirals (DAAs) in the German Hepatitis C-Registry (DHC-R). Z. Gastroenterol. 2019, 57, 27–36. [Google Scholar] [CrossRef]
- Berg, T.; Naumann, U.; Stoehr, A.; Sick, C.; John, C.; Teuber, G.; Schiffelholz, W.; Mauss, S.; Lohmann, K.; Konig, B.; et al. Real-world effectiveness and safety of glecaprevir/pibrentasvir for the treatment of chronic hepatitis C infection: Data from the German Hepatitis C-Registry. Aliment. Pharmacol. Ther. 2019, 49, 1052–1059. [Google Scholar] [CrossRef]
- Ware, J. SF-36 Health Survey Update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef]
- Coteur, G.; Feagan, B.; Keininger, D.L.; Kosinski, M. Evaluation of the meaningfulness of health-related quality of life improvements as assessed by the SF-36 and the EQ-5D VAS in patients with active Crohn’s disease. Aliment. Pharmacol. Ther. 2009, 29, 1032–1041. [Google Scholar] [CrossRef]
- Strand, V.; Fiorentino, D.; Hu, C.; Day, R.M.; Stevens, R.M.; Papp, K.A. Improvements in patient-reported outcomes with apremilast, an oral phosphodiesterase 4 inhibitor, in the treatment of moderate to severe psoriasis: Results from a phase IIb randomized, controlled study. Health Qual. Life Outcomes 2013, 11, 82. [Google Scholar] [CrossRef] [Green Version]
- Buggisch, P.; Vermehren, J.; Mauss, S.; Gunther, R.; Schott, E.; Pathil, A.; Boeker, K.; Zimmermann, T.; Teuber, G.; Vornkahl, H.P.; et al. Real-world effectiveness of 8-week treatment with ledipasvir/sofosbuvir in chronic hepatitis C. J. Hepatol. 2018, 68, 663–671. [Google Scholar] [CrossRef]
- Lampertico, P.; Carrion, J.A.; Curry, M.; Turnes, J.; Cornberg, M.; Negro, F.; Brown, A.; Persico, M.; Wick, N.; Porcalla, A.; et al. Real-world effectiveness and safety of glecaprevir/pibrentasvir for the treatment of patients with chronic HCV infection: A meta-analysis. J. Hepatol. 2020, 72, 1112–1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huppe, D.; Stoehr, A.; Buggisch, P.; Mauss, S.; Klinker, H.; Teuber, G.; Hidde, D.; Lohmann, K.; Bondin, M.; Wedemeyer, H. The changing characteristics of patients infected with chronic hepatitis C virus from 2014 to 2019: Real-world data from the German Hepatitis C-Registry (DHC-R). J. Viral Hepat. 2021, 28, 1474–1483. [Google Scholar] [CrossRef]
- Wilton, J.; Wong, S.; Yu, A.; Ramji, A.; Cook, D.; Butt, Z.A.; Alvarez, M.; Binka, M.; Darvishian, M.; Jeong, D.; et al. Real-world Effectiveness of Sofosbuvir/Velpatasvir for Treatment of Chronic Hepatitis C in British Columbia, Canada: A Population-Based Cohort Study. Open Forum Infect. Dis. 2020, 7, ofaa055. [Google Scholar] [CrossRef]
- Darvishian, M.; Wong, S.; Binka, M.; Yu, A.; Ramji, A.; Yoshida, E.M.; Wong, J.; Rossi, C.; Butt, Z.A.; Bartlett, S.; et al. Loss to follow-up: A significant barrier in the treatment cascade with direct-acting therapies. J. Viral Hepat. 2020, 27, 243–260. [Google Scholar] [CrossRef]
- Edmunds, B.L.; Miller, E.R.; Tsourtos, G. The distribution and socioeconomic burden of Hepatitis C virus in South Australia: A cross-sectional study 2010-2016. BMC Public Health 2019, 19, 527. [Google Scholar] [CrossRef] [Green Version]
- Greenaway, C.; Makarenko, I.; Chakra, C.N.A.; Alabdulkarim, B.; Christensen, R.; Palayew, A.; Tran, A.; Staub, L.; Pareek, M.; Meerpohl, J.J.; et al. The Effectiveness and Cost-Effectiveness of Hepatitis C Screening for Migrants in the EU/EEA: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2013. [Google Scholar] [CrossRef] [Green Version]
- Degenhardt, L.; Peacock, A.; Colledge, S.; Leung, J.; Grebely, J.; Vickerman, P.; Stone, J.; Cunningham, E.B.; Trickey, A.; Dumchev, K.; et al. Global prevalence of injecting drug use and sociodemographic characteristics and prevalence of HIV, HBV, and HCV in people who inject drugs: A multistage systematic review. Lancet Glob. Health 2017, 5, e1192–e1207. [Google Scholar] [CrossRef] [Green Version]
- Zibbell, J.E.; Asher, A.K.; Patel, R.C.; Kupronis, B.; Iqbal, K.; Ward, J.W.; Holtzman, D. Increases in Acute Hepatitis C Virus Infection Related to a Growing Opioid Epidemic and Associated Injection Drug Use, United States, 2004 to 2014. Am. J. Public Health 2018, 108, 175–181. [Google Scholar] [CrossRef]
- Ryerson, A.B.; Schillie, S.; Barker, L.K.; Kupronis, B.A.; Wester, C. Vital Signs: Newly Reported Acute and Chronic Hepatitis C Cases—United States, 2009–2018. MMWR Morb. Morb. Wkly. Rep. 2020, 69, 399–404. [Google Scholar] [CrossRef] [Green Version]
- Schmidbauer, C.; Schubert, R.; Schutz, A.; Schwanke, C.; Luhn, J.; Gutic, E.; Pirker, R.; Lang, T.; Reiberger, T.; Haltmayer, H.; et al. Directly observed therapy for HCV with glecaprevir/pibrentasvir alongside opioid substitution in people who inject drugs-First real world data from Austria. PLoS ONE 2020, 15, e0229239. [Google Scholar] [CrossRef]
- Fiore, V.; Ranieri, R.; Dell’Isola, S.; Pontali, E.; Barbarini, G.; Prestileo, T.; Marri, D.; Starnini, G.; Sotgiu, G.; Madeddu, G.; et al. Feasibility and efficacy of 8 week Glecaprevir/Pibrentasvir to treat incarcerated viraemic HCV patients: A case-control study. Liver Int. 2021, 41, 271–275. [Google Scholar] [CrossRef]
- Schulte, B.; Schmidt, C.S.; Manthey, J.; Strada, L.; Christensen, S.; Cimander, K.; Gorne, H.; Khaykin, P.; Scherbaum, N.; Walcher, S.; et al. Clinical and Patient-Reported Outcomes of Direct-Acting Antivirals for the Treatment of Chronic Hepatitis C Among Patients on Opioid Agonist Treatment: A Real-world Prospective Cohort Study. Open Forum Infect. Dis. 2020, 7, ofaa317. [Google Scholar] [CrossRef]
- Smith-Palmer, J.; Cerri, K.; Valentine, W. Achieving sustained virologic response in hepatitis C: A systematic review of the clinical, economic and quality of life benefits. BMC Infect. Dis. 2015, 15, 19. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Population N = 2354 | Key Comorbidities 1 | Migrant Status | |||||||
|---|---|---|---|---|---|---|---|---|---|
| None 2 N = 1378 | OST N = 609 | PWUD (Active) N = 87 | Psychiatric Disorder N = 322 | Alcohol Abuse/ Dependence N = 170 | HIV Coinfection N = 142 | All Migrants 3 N = 977 | CIS Migrants N = 474 | ||
| Male, n (%) | 1634 (69.4%) | 868 (63.0%) | 492 (80.8%) | 72 (82.8%) | 225 (69.9%) | 132 (77.6%) | 125 (88.0%) | 728 (74.5%) | 349 (73.6%) |
| Age Years, median (range) > 65 years, n (%) | 46 (18–87) 156 (6.6%) | 47 (18–87) 131 (11.1) | 44 (21–69) 3 (0.5%) | 44 (23–65) 0 | 47 (18–83) 11 (3.4%) | 47 (18–66) 1 (0.6%) | 44 (37–66) 1 (0.7%) | 41 (18–82) 48 (4.9%) | 40 (18–82) 17 (3.6%) |
| Race, n (%) | |||||||||
| White Other 4 | 2242 (95.2) 112 (4.8) | 1291 (93.7) 87 (6.3) | 601 (98.7) 8 (1.3) | 86 (98.9) 1 (1.1) | 313 (97.2) 9 (2.8) | 166 (97.6) 4 (2.4) | 132 (93.0) 10 (7.0) | 867 (88.7) 110 (11.3) | 469 (98.9) 5 (1.1) |
| Body weight (kg), median (range) | 75.0 (35.0–180.0) | 75.0 (39.3–180.0) | 76.0 (40.0–180.0) | 72.0 (35.0–143.0) | 75.0 (45.5–180.0) | 75.0 (45.0–133.0) | 71.5 (43.0–121.5) | 75.0 (43.0–178.0) | 77.4 (43.0–135.0) |
| BMI (kg/m2), mean (SD) | 25.6 (5.0) | 25.8 (4.9) | 25.3 (5.6) | 24.5 (5.4) | 25.6 (5.3) | 25.2 (4.6) | 23.7 (4.2) | 25.9 (4.8) | 26.2 (4.6) |
| HCV genotype, n (%) | |||||||||
| 1 1a5 1b5 other5,6 2 3 4 5 6 Mixed7 Unknown | 1231 (52.3) 841 (68.3) 361 (29.3) 29 (2.4) 131 (5.6) 837 (35.6) 112 (4.8) 2 (0.1) 8 (0.3) 20 (0.8) 13 (0.6) | 736 (53.4) 440 (59.8) 277 (37.6) 19 (2.6) 78 (5.7) 474 (34.4) 58 (4.2) 2 (0.1) 7 (0.5) 15 (1.1) 8 (0.6) | 293 (48.1) 248 (84.6) 38 (13.0) 7 (2.4) 31 (5.1) 261 (42.9) 18 (3.0) 0 1 (0.2) 2 (0.3) 3 (0.5) | 43 (49.4) 39 (90.7) 4 (9.3) 0 6 (6.9) 36 (41.4) 2 (2.3) 0 0 0 0 | 175 (54.3) 137 (78.3) 35 (20.0) 3 (1.7) 22 (6.8) 105 (32.6) 18 (5.6) 0 0 1 (0.3) 1 (0.3) | 85 (50.0) 68 (80.0) 15 (17.6) 2 (2.4) 9 (5.3) 65 (38.2) 7 (4.1) 0 0 3 (1.8) 1 (0.6) | 80 (56.3) 69 (86.3) 11 (13.8) 0 6 (4.2) 27 (19.0) 28 (19.7) 0 0 1 (0.7) 0 | 438 (44.8) 231 (52.7) 193 (44.1) 14 (3.2) 53 (5.4) 407 (41.7) 51 (5.2) 1 (0.1) 8 (0.8) 14 (1.4) 5 (0.5) | 193 (40.7) 69 (35.8) 117 (60.6) 7 (3.6) 28 (5.9) 240 (50.6) 2 (0.4) 0 0 7 (1.5) 4 (0.8) |
| HCV RNA, median (IQR), Log10 IU/mL | |||||||||
| 6.1 (5.5–6.6) | 6.1 (5.5–6.6) | 6.1 (5.5–6.7) | 6.3 (5.6–6.8) | 6.2 (5.4–6.7) | 6.1 (5.6–6.7) | 6.1 (5.5–6.7) | 6.1 (5.5–6.6) | 6.0 (5.4–6.6) | |
| Platelets per μL, median (range) 8 | 218,000 (17,500–616,000) | 220,000 (31,000–616,000) | 210,000 (17,500–564,000) | 198,000 (47,000–362,000) | 224,500 (79,000–564,000) | 207,000 (51,000–468,000) | 210,000 (17,500–372,000) | 219,000 (45,000–557,000) | 223,000 (51,000–369,000) |
| Non-cirrhotic 9 | 2033 (86.4%) | 1211 (87.9%) | 507 (83.3%) | 74 (85.1%) | 279 (86.6%) | 126 (74.1%) | 119 (83.8%) | 870 (89.0%) | 432 (91.1%) |
| METAVIR Fibrosis stage, n (%) | |||||||||
| F0–F1 F2 F3 F4 Missing stage data | 469 (19.9) 191 (8.1) 58 (2.5) 321 (13.6) 1315 | 264 (19.2) 116 (8.4) 34 (2.5) 167 (12.1) 797 | 116 (19.0) 47 (7.7) 13 (2.1) 102 (16.7) 331 | 17 (19.5) 8 (9.2) 3 (3.4) 13 (14.9) 46 | 73 (22.7) 23 (7.1) 12 (3.7) 43 (13.4) 171 | 38 (22.4) 19 (11.2) 7 (4.1) 44 (25.9) 62 | 36 (25.4) 8 (5.6) 3 (2.1) 23 (16.2) 72 | 182 (18.6) 67 (6.9) 26 (2.7) 107 (11.0) 595 | 72 (15.2) 34 (7.2) 15 (3.2) 42 (8.9) 311 |
| HCV TN | 2133 (90.6%) 9 | 1257 (91.2%) | 551 (90.5%) | 81 (93.1%) | 284 (88.2%) | 159 (93.5%) | 125 (88.0%) | 900 (92.1%) | 443 (93.5%) |
| Estimated duration of infection (years), mean (SD) | |||||||||
| 15.7 (11.3) | 17.1 (12.5) | 14.2 (8.7) | 12.3 (8.9) | 14.9 (10.4) | 15.5 (9.6) | 8.0 (9.9) | 13.5 (10.1) | 14.3 (8.9) | |
| Employment status, n (%) | |||||||||
| Employed Unemployed Unknown | 952 (40.4) 1015 (43.1) 387 (16.4) | 658 (47.8) 500 (36.3) 220 (16.0) | 143 (23.5) 358 (58.8) 108 (17.7) | 20 (23.0) 50 (57.5) 17 (19.5) | 81 (25.2) 191 (59.3) 50 (15.5) | 53 (31.2) 85 (50.0) 32 (18.8) | 68 (47.9) 46 (32.4) 28 (19.7) | 476 (48.7) 363 (37.2) 138 (14.1) | 244 (51.5) 169 (35.7) 61 (12.9) |
| Suspected route of transmission, n (%) | |||||||||
| Blood products Drugs (IV, nasal) Sexual transmission Surgical/medical procedure Other Unknown | 169 (7.2) 1178 (50.0) 138 (5.9) 103 (4.4) 64 (2.7) 702 (29.8) | 145 (10.5) 432 (31.3) 54 (3.9) 94 (6.8) 52 (3.8) 601(43.6) | 5 (0.8) 568 (93.3) 12 (2.0) 1 (0.2) 4 (0.7) 19 (3.1) | 1 (1.1) 77 (88.5) 1 (1.1) 1 (1.1) 1 (1.1) 6 (6.9) | 15 (4.7) 212 (65.8) 28 (8.7) 6 (1.9) 7 (2.2) 54 (16.8 | 4 (2.4) 128 (75.3) 8 (4.7) 1 (0.6) 3 (1.8) 26 (15.3) | 2 (1.4) 58 (40.8) 62 (43.7) 0 0 20 (14.1) | 70 (7.2) 376 (38.5) 42 (4.3) 70 (7.2) 36 (3.7) 383 (39.2) | 29 (6.1) 205 (43.2) 14 (3.0) 41 (8.6) 16 (3.4) 169 (35.7) |
| Mean SF-36 mental component summary score 10 | |||||||||
| 39 | 42 | 34 11 | 33 11 | 31 12 | 37 12 | 41 | 40 | 40 | |
| Mean SF-36 physical component summary score 10 | |||||||||
| 49 | 50 | 48 11 | 48 | 48 | 48 | 49 | 50 | 50 | |
| Patients (N = 2354) | |
|---|---|
| Adverse events | |
| Any AE | 631 (26.8) |
| Any serious AE 1 | 44 (1.9) |
| Any AE leading to study drug discontinuation 2 | 3 (0.1) |
| AEs occurring in ≥ 1% of patients | |
| Fatigue | 215 (9.1) |
| Headache | 142 (6.0) |
| Nausea | 74 (3.1) |
| Abdominal discomfort | 51 (2.2) |
| Pruritus | 45 (1.9) |
| Diarrhea | 38 (1.6) |
| Arthralgia | 27 (1.1) |
| Deaths | 4 (0.2) |
| Laboratory abnormalities | |
| Alanine aminotransferase, any grade | 2144 (91.1) |
| >5 × ULN | 3 (0.1) |
| Aspartate aminotransferase, any grade | 2007 (85.3) |
| >5 × ULN | 5 (0.2) |
| Total bilirubin, any grade | 1918 (81.5) |
| >5 × ULN | 7 (0.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cornberg, M.; Stoehr, A.; Naumann, U.; Teuber, G.; Klinker, H.; Lutz, T.; Möller, H.; Hidde, D.; Lohmann, K.; Simon, K.-G. Real-World Safety, Effectiveness, and Patient-Reported Outcomes in Patients with Chronic Hepatitis C Virus Infection Treated with Glecaprevir/Pibrentasvir: Updated Data from the German Hepatitis C-Registry (DHC-R). Viruses 2022, 14, 1541. https://doi.org/10.3390/v14071541
Cornberg M, Stoehr A, Naumann U, Teuber G, Klinker H, Lutz T, Möller H, Hidde D, Lohmann K, Simon K-G. Real-World Safety, Effectiveness, and Patient-Reported Outcomes in Patients with Chronic Hepatitis C Virus Infection Treated with Glecaprevir/Pibrentasvir: Updated Data from the German Hepatitis C-Registry (DHC-R). Viruses. 2022; 14(7):1541. https://doi.org/10.3390/v14071541
Chicago/Turabian StyleCornberg, Markus, Albrecht Stoehr, Uwe Naumann, Gerlinde Teuber, Hartwig Klinker, Thomas Lutz, Hjördis Möller, Dennis Hidde, Kristina Lohmann, and Karl-Georg Simon. 2022. "Real-World Safety, Effectiveness, and Patient-Reported Outcomes in Patients with Chronic Hepatitis C Virus Infection Treated with Glecaprevir/Pibrentasvir: Updated Data from the German Hepatitis C-Registry (DHC-R)" Viruses 14, no. 7: 1541. https://doi.org/10.3390/v14071541