
Occult Hepatitis B Virus Infection: An Update


Abstract
:1. Introduction
2. Definition of OBI
3. Biology of OBI
4. Diagnosis of OBI
5. Epidemiology of OBI
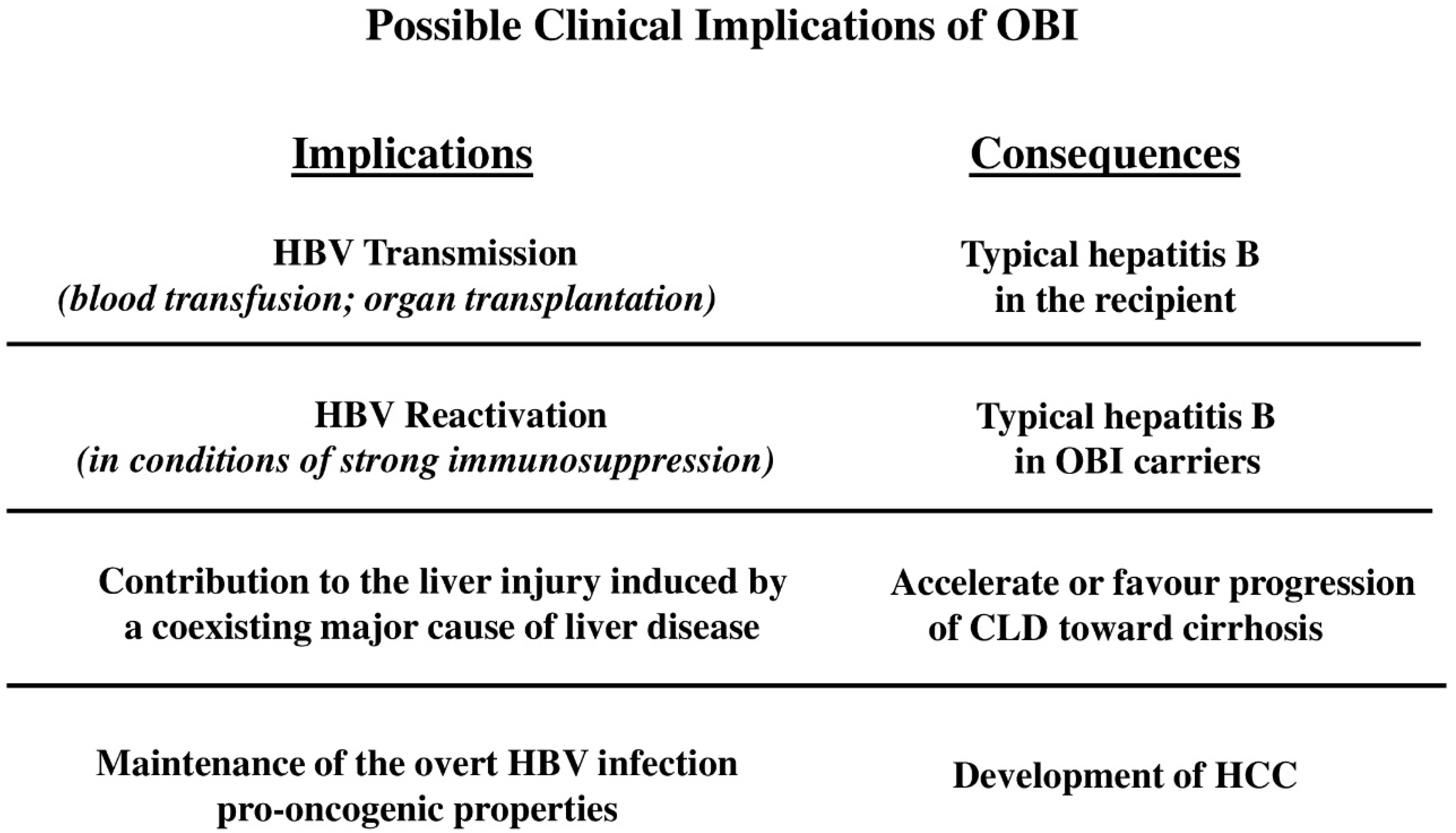
6. Clinical Implications of OBI
6.1. Risk of OBI Transmission
6.1.1. Blood Transfusion
6.1.2. Liver Transplantation
6.2. OBI Reactivation
6.3. OBI and Chronic Liver Disease

{kind=link}
| Article | Type of Study |
|---|---|
| “Hepatocellular carcinoma: the point of view of the hepatitis B virus” Pollicino, T., et al., Carcinogenesis (2011) [140] | Review |
| “Association between occult hepatitis B infection and the risk of hepatocellular carcinoma: a meta-analysis” Shi, Y., et al., Liver International (2012) [141] | Meta-analysis |
| “Occult HBV infection” Raimondo, G., et al., Seminars in Immunopathology (2013) [71] | Review |
| “Occult hepatitis B virus and the risk for chronic liver disease: a meta-analysis” Covolo, L., et al., Digestive and Liver Disease (2013) [130] | Meta-analysis |
| “Occult hepatitis B virus and hepatocellular carcinoma” Pollicino, T., and Saitta, C., World Journal of Gastroenterology (2014) [142] | Review |
| “Occult hepatitis B virus infection and hepatocellular carcinoma: a systematic review” Huang, X., and Hollinger, F.B., Journal of Viral Hepatitis (2014) [134] | Review |
| “HBsAg-negative hepatitis B virus infection and hepatocellular carcinoma” Chen, L., et al., Discovery Medicine (2014) [135] | Review |
| “Occult hepatitis B virus infection” Kwak, M.S., et al., World Journal of Hepatology (2014) [136] | Review |
| “Update on occult hepatitis B virus infection” Makvandi, M., et al., World Journal of Gastroenterology (2016) [137] | Review |
| “Current knowledge of occult hepatitis B infection and clinical implications” Yip, T.C., et al., Seminars in Liver Disease (2019) [138] | Review |
| “Update of the statements on biology and clinical impact of occult hepatitis B virus infection” Raimondo, G., et al., Journal of Hepatology (2019) [4] | Statements |
| “Occult hepatitis B infection and hepatocellular carcinoma: Epidemiology, virology, hepatocarcinogenesis and clinical significance” Mak, L.Y., et al., Journal of Hepatology (2020) [139] | Review |
| “Occult hepatitis B virus infection in hepatitis C virus negative chronic liver diseases” Franzè, M.S., et al., Liver International (2022) [131] | Review |
6.4. OBI and HCC
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raimondo, G.; Pollicino, T.; Cacciola, I.; Squadrito, G. Occult hepatitis B virus infection. J. Hepatol. 2007, 46, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Cacciola, I.; Pollicino, T.; Squadrito, G.; Cerenzia, G.; Orlando, M.E.; Raimondo, G. Occult hepatitis B virus infection in patients with chronic hepatitis C liver disease. N. Engl. J. Med. 1999, 341, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Raimondo, G.; Allain, J.P.; Brunetto, M.R.; Buendia, M.A.; Chen, D.S.; Colombo, M.; Craxì, A.; Donato, F.; Ferrari, C.; Gaeta, G.B.; et al. Statements from the Taormina expert meeting on occult hepatitis B virus infection. J. Hepatol. 2008, 49, 652–657. [Google Scholar] [CrossRef] [PubMed]
- Raimondo, G.; Locarnini, S.; Pollicino, T.; Levrero, M.; Zoulim, F.; Lok, A.S.; Taormina Workshop on Occult HBV Infection Faculty Members. Update of the statements on biology and clinical impact of occult hepatitis B virus infection. J. Hepatol. 2019, 71, 397–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazemi-Shirazi, L.; Petermann, D.; Muller, C. Hepatitis B virus DNA in sera and liver tissue of HBsAg negative patients with chronic hepatitis C. J. Hepatol. 2000, 33, 785–790. [Google Scholar] [CrossRef]
- Kannangai, R.; Vivekanandan, P.; Netski, D.; Mehta, S.; Kirk, G.D.; Thomas, D.L.; Torbenson, M. Liver enzyme flares and occult hepatitis B in persons with chronic hepatitis C infection. J. Clin. Virol. 2007, 39, 101–105. [Google Scholar] [CrossRef]
- Chemin, I.; Guillaud, O.; Queyron, P.C.; Trepo, C. Close monitoring of serum HBV DNA levels and liver enzymes levels is most useful in the management of patients with occult HBV infection. J. Hepatol. 2009, 51, 824–825. [Google Scholar] [CrossRef] [Green Version]
- Saitta, C.; Musolino, C.; Marabello, G.; Martino, D.; Leonardi, M.S.; Pollicino, T.; Altavilla, G.; Raimondo, G. Risk of occult hepatitis B virus infection reactivation in patients with solid tumours undergoing chemotherapy. Dig. Liver Dis. 2013, 45, 683–686. [Google Scholar] [CrossRef]
- Candotti, D.; Assennato, S.M.; Laperche, S.; Allain, J.P.; Levicnik-Stezinar, S. Multiple HBV transfusion transmissions from undetected occult infections: Revising the minimal infectious dose. Gut 2019, 68, 313–321. [Google Scholar] [CrossRef]
- Mulrooney-Cousins, P.M.; Michalak, T.I. Asymptomatic hepadnaviral persistence and its consequences in the woodchuck model of occult hepatitis B virus infection. J. Clin. Transl. Hepatol. 2015, 3, 211–219. [Google Scholar] [CrossRef]
- Yamamoto, K.; Horikita, M.; Tsuda, F.; Itoh, K.; Akahane, Y.; Yotsumoto, S.; Okamoto, H.; Miyakawa, Y.; Mayumi, M. Naturally occurring escape mutants of hepatitis B virus with various mutations in the S gene in carriers seropositive for antibody to hepatitis B surface antigen. J. Virol. 1994, 68, 2671–2676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, J.; Karayiannis, P.; Waters, J.; Luo, K.; Liang, C.; Thomas, H.C. A unique insertion in the S gene of surface antigen–negative hepatitis B virus Chinese carriers. Hepatology 1995, 21, 273–278. [Google Scholar] [CrossRef]
- Carman, W.F.; Van Deursen, F.J.; Mimms, L.T.; Hardie, D.; Coppola, R.; Decker, R.; Sanders, R. The prevalence of surface antigen variants of hepatitis B virus in Papua New Guinea, South Africa, and Sardinia. Hepatology 1997, 26, 1658–1666. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, V.; Tayal, R.; Nayak, B.; Acharya, S.K.; Panda, S.K. Occult hepatitis B virus infection in chronic liver disease: Full-length genome and analysis of mutant surface promoter. Gastroenterology 2004, 127, 1356–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hass, M.; Hannoun, C.; Kalinina, T.; Sommer, G.; Manegold, C.; Gunther, S. Functional analysis of hepatitis B virus reactivating in hepatitis B surface antigen-negative individuals. Hepatology 2005, 42, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Candotti, D.; Lin, C.K.; Belkhiri, D.; Sakuldamrongpanich, T.; Biswas, S.; Lin, S.; Teo, D.; Ayob, Y.; Allain, J.P. Occult hepatitis B infection in blood donors from South East Asia: Molecular characterisation and potential mechanisms of occurrence. Gut 2012, 61, 1744–1753. [Google Scholar] [CrossRef]
- El Chaar, M.; Candotti, D.; Crowther, R.A.; Allain, J.P. Impact of hepatitis B virus surface protein mutations on the diagnosis of occult hepatitis B virus infection. Hepatology 2010, 52, 1600–1610. [Google Scholar] [CrossRef]
- Huang, C.H.; Yuan, Q.; Chen, P.J.; Zhang, Y.L.; Chen, C.R.; Zheng, Q.B.; Yeh, S.H.; Yu, H.; Xue, Y.; Chen, Y.X.; et al. Influence of mutations in hepatitis B virus surface protein on viral antigenicity and phenotype in occult HBV strains from blood donors. J. Hepatol. 2012, 57, 720–729. [Google Scholar] [CrossRef]
- Mason, A.L.; Xu, L.; Guo, L.; Kuhns, M.; Perrillo, R.P. Molecular basis for persistent hepatitis B virus infection in the liver after clearance of serum hepatitis B surface antigen. Hepatology 1998, 27, 1736–1742. [Google Scholar] [CrossRef]
- Bock, C.T.; Schwinn, S.; Locarnini, S.; Fyfe, J.; Manns, M.P.; Trautwein, C.; Zentgraf, H. Structural organization of the hepatitis B virus minichromosome. J. Mol. Biol. 2001, 307, 183–196. [Google Scholar] [CrossRef]
- Pollicino, T.; Squadrito, G.; Cerenzia, G.; Cacciola, I.; Raffa, G.; Craxi, A.; Farinati, F.; Missale, G.; Smedile, A.; Tiribelli, C.; et al. Hepatitis B virus maintains its pro-oncogenic properties in the case of occult HBV infection. Gastroenterology 2004, 126, 102–110. [Google Scholar] [CrossRef] [PubMed]
- Werle-Lapostolle, B.; Bowden, S.; Locarnini, S.; Wursthorn, K.; Petersen, J.; Lau, G.; Trepo, C.; Marcellin, P.; Goodman, Z.; Delaney IV, W.E.; et al. Persistence of cccDNA during the natural history of chronic hepatitis B and decline during adefovir dipivoxil therapy. Gastroenterology 2004, 126, 1750–1758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zoulim, F. New insight on hepatitis B virus persistence from the study of intrahepatic viral cccDNA. J. Hepatol. 2005, 42, 302–308. [Google Scholar] [CrossRef] [PubMed]
- Pollicino, T.; Belloni, L.; Raffa, G.; Pediconi, N.; Squadrito, G.; Raimondo, G.; Levrero, M. Hepatitis B virus replication is regulated by the acetylation status of hepatitis B virus cccDNA-bound H3 and H4 histones. Gastroenterology 2006, 130, 823–837. [Google Scholar] [CrossRef]
- Levrero, M.; Pollicino, T.; Petersen, J.; Belloni, L.; Raimondo, G.; Dandri, M. Control of cccDNA function in hepatitis B virus infection. J. Hepatol. 2009, 51, 581–592. [Google Scholar] [CrossRef] [Green Version]
- Locarnini, S.; Zoulim, F. Molecular genetics of HBV infection. Antivir. Ther. 2010, 15 (Suppl. S3), 3–14. [Google Scholar] [CrossRef] [Green Version]
- Dandri, M.; Locarnini, S. New insight in the pathobiology of hepatitis B virus infection. Gut 2012, 61 (Suppl. S1), i6–i17. [Google Scholar] [CrossRef]
- Glebe, D.; Bremer, C.M. The molecular virology of hepatitis B virus. Semin. Liver Dis. 2013, 33, 103–112. [Google Scholar] [CrossRef]
- Bes, M.; Vargas, V.; Piron, M.; Casamitjana, N.; Esteban, J.I.; Vilanova, N.; Pinacho, A.; Quer, J.; Puig, L.; Guardia, J.; et al. T cell responses and viral variability in blood donation candidates with occult hepatitis B infection. J. Hepatol. 2012, 56, 765–774. [Google Scholar] [CrossRef]
- Huang, X.; Qin, Y.; Li, W.; Shi, Q.; Xue, Y.; Li, J.; Liu, C.; Hollinger, F.B.; Shen, Q. Molecular analysis of the hepatitis B virus presurface and surface gene in patients from eastern China with occult hepatitis B. J. Med. Virol. 2013, 85, 979–986. [Google Scholar] [CrossRef]
- Huang, F.Y.; Wong, D.K.; Seto, W.K.; Zhang, A.Y.; Lee, C.K.; Lin, C.K.; Fung, J.; Lai, C.L.; Yuen, M.F. Sequence variations of full-length hepatitis B virus genomes in Chinese patients with HBsAg-negative hepatitis B infection. PLoS ONE 2014, 9, e99028. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Ma, C.; Zhang, Q.; Shi, Q.; Huang, T.; Liu, C.; Li, J.; Hollinger, F.B. Impact of “a” determinant mutations on detection of hepatitis B surface antigen (HBsAg) in HBV strains from Chinese patients with occult hepatitis B. J. Med. Virol. 2017, 89, 1796–1803. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.F. Hepatitis B virus pre-S/S variants in liver diseases. World J. Gastroenterol. 2018, 24, 1507–1520. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Liu, Y.; Chen, R.; Li, Q.; Xu, Z.; Si, L.; Cheng, Y.; Yang, Y.; Chen, J.; Xu, D.; et al. Antigenicity reduction contributes mostly to poor detectability of HBsAg by hepatitis B virus (HBV) S-gene mutants isolated from individuals with occult HBV infection. J. Med. Virol. 2018, 90, 263–270. [Google Scholar] [CrossRef]
- Zhang, L.; Chang, L.; Laperche, S.; Ji, H.; Zhao, J.; Jiang, X.; Wang, L.; Candotti, D. Occult HBV infection in Chinese blood donors: Role of N-glycosylation mutations and amino acid substitutions in S protein transmembrane domains. Emerg. Microbes Infect. 2019, 8, 1337–1346. [Google Scholar] [CrossRef] [Green Version]
- Pollicino, T.; Raffa, G.; Costantino, L.; Lisa, A.; Campello, C.; Squadrito, G.; Levrero, M.; Raimodno, G. Molecular and functional analysis of occult hepatitis B virus isolates from patients with hepatocellular carcinoma. Hepatology 2007, 45, 277–285. [Google Scholar] [CrossRef]
- Chazouilleres, O.; Mamish, D.; Kim, M.; Carey, K.; Ferrell, L.; Roberts, J.P.; Ascher, N.L.; Wright, T.L. “Occult” hepatitis B virus as source of infection in liver transplant recipients. Lancet 1994, 343, 142–146. [Google Scholar] [CrossRef]
- Yuen, M.F.; Wong, D.K.; Lee, C.K.; Tanaka, Y.; Allain, J.P.; Fung, J.; Leung, J.; Lin, C.K.; Sugiyama, M.; Sugauchi, F.; et al. Transmissibility of hepatitis B virus (HBV) infection through blood transfusion from blood donors with occult HBV infection. Clin. Infect. Dis. 2011, 52, 624–632. [Google Scholar] [CrossRef]
- Seto, W.K.; Chan, T.S.; Hwang, Y.Y.; Wong, D.K.; Fung, J.; Liu, K.S.; Gill, H.; Lam, Y.F.; Lie, A.K.W.; Lai, C.L.; et al. Hepatitis B reactivation in patients with previous hepatitis B virus exposure undergoing rituximab-containing chemotherapy for lymphoma: A prospective study. J. Clin. Oncol. 2014, 32, 3736–3743. [Google Scholar] [CrossRef]
- Seto, W.K.; Sau-Yan Chan, T.; Hwang, Y.Y.; Wong, D.K.; Fung, J.; Liu, K.S.; Gill, H.; Lam, Y.F.; Lau, E.H.Y.; Cheung, K.S.; et al. Hepatitis B reactivation in occult viral carriers undergoing hematopoietic stem cell transplantation: A prospective study. Hepatology 2017, 65, 1451–1461. [Google Scholar] [CrossRef] [Green Version]
- Loomba, R.; Liang, T.J. Hepatitis B reactivation associated with immune suppressive and biological modififier therapies: Current concepts, management strategies, and future directions. Gastroenterology 2017, 152, 1297–1309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blum, H.; Galun, E.; Liang, T.J.; von Weizsacker, F.; Wands, J.R. Naturally occurring missense mutation in the polymerase gene terminating hepatitis B virus replication. J. Virol. 1991, 65, 1836–1842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, D.K.; Huang, F.Y.; Lai, C.L.; Poon, R.T.; Seto, W.K.; Fung, J.; Hung, I.F.N.; Yuen, M.F. Occult hepatitis B infection and HBV replicative activity in patients with cryptogenic cause of hepatocellular carcinoma. Hepatology 2011, 54, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Vivekanandan, P.; Kannangai, R.; Ray, S.C.; Thomas, D.L.; Torbenson, M. Comprehensive genetic and epigenetic analysis of occult hepatitis B from liver tissue samples. Clin. Infect. Dis. 2008, 46, 1227–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, Y.; Li, Y.; Mu, S.; Zhang, J.; Yan, Z. Evidence that methylation of hepatitis B virus covalently closed circular DNA in liver tissues of patients with chronic hepatitis B modulates HBV replication. J. Med. Virol. 2009, 81, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Hong, X.; Kim, E.S.; Guo, H. Epigenetic regulation of hepatitis B virus covalently closed circular DNA: Implications for epigenetic therapy against chronic hepatitis B. Hepatology 2017, 66, 2066–2077. [Google Scholar] [CrossRef] [PubMed]
- Belloni, L.; Pollicino, T.; De Nicola, F.; Guerrieri, F.; Raffa, G.; Fanciulli, M.; Raimondo, G.; Levrero, M. Nuclear HBx binds the HBV minichromosome and modifies the epigenetic regulation of cccDNA function. Proc. Natl. Acad. Sci. USA 2009, 106, 19975–19979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, C.K.; Cheng, C.Y.S.; Tsoi, S.Y.J.; Huang, F.Y.; Liu, F.; Seto, W.K.; Lai, C.L.; Yuen, M.F.; Wong, D.K. Role of hepatitis B core protein in HBV transcription and recruitment of histone acetyltransferases to cccDNA minichromosome. Antivir. Res. 2017, 144, 1–7. [Google Scholar] [CrossRef]
- Belloni, L.; Allweiss, L.; Guerrieri, F.; Pediconi, N.; Volz, T.; Pollicino, T.; Petersen, J.; Raimondo, G.; Dandri, M.; Levrero, M. IFN-alpha inhibits HBV transcription and replication in cell culture and in humanized mice by targeting the epigenetic regulation of the nuclear cccDNA minichromosome. J. Clin. Investig. 2012, 122, 529–537. [Google Scholar] [CrossRef] [Green Version]
- Benhenda, S.; Ducroux, A.; Riviere, L.; Sobhian, B.; Ward, M.D.; Dion, S.; Hantz, O.; Protzer, U.; Michel, M.L.; Benkirane, M.; et al. Methyltransferase PRMT1 is a binding partner of HBx and a negative regulator of hepatitis B virus transcription. J. Virol. 2013, 87, 4360–4371. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Chen, J.; Wu, M.; Zhang, X.; Zhang, M.; Yue, L.; Li, Y.; Liu, J.; Li, B.; Shen, F.; et al. PRMT5 restricts hepatitis B virus replication through epigenetic repression of covalently closed circular DNA transcription and interference with pregenomic RNA encapsidation. Hepatology 2017, 66, 398–415. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.J.; Kong, K.E.; Gao, W.W.; Tang, H.V.; Chaudhary, V.; Cheng, Y.; Zhou, J.; Chan, C.P.; Wong, D.K.H.; Yuen, M.F.; et al. Interplay between SIRT1 and hepatitis B virus X protein in the activation of viral transcription. Biochim. Biophys. Acta Gene Regul. Mech. 2017, 1860, 491–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, C.K.; Cheng, C.Y.S.; Tsoi, S.Y.J.; Huang, F.Y.; Liu, F.; Fung, J.; Seto, W.K.; Lai, K.K.Y.; Lai, C.L.; Yuen, M.F.; et al. HBV X protein mutations affect HBV transcription and association of histone modifying enzymes with covalently closed circular DNA. Sci. Rep. 2020, 10, 802. [Google Scholar] [CrossRef] [PubMed]
- Rehermann, B.; Ferrari, C.; Pasquinelli, C.; Chisari, F.V. The hepatitis B virus persists for decades after patients’ recovery from acute viral hepatitis despite active maintenance of a cytotoxic T-lymphocyte response. Nat. Med. 1996, 2, 1104–1108. [Google Scholar] [CrossRef]
- Penna, A.; Artini, M.; Cavalli, A.; Levrero, M.; Bertoletti, A.; Pilli, M.; Chisari, F.V.; Rehermann, B.; Del Prete, G.; Fiaccadori, F.; et al. Long-lasting memory T cell responses following self-limited acute hepatitis B. J. Clin. Investig. 1996, 98, 1185–1194. [Google Scholar] [CrossRef] [Green Version]
- Zerbini, A.; Pilli, M.; Boni, C.; Fisicaro, P.; Penna, A.; Di Vincenzo, P.; Giuberti, T.; Orlandini, A.; Raffa, G.; Pollicino, T.; et al. The characteristics of the cell-mediated immune response identify different profiles of occult hepatitis B virus infection. Gastroenterology 2008, 134, 1470–1481. [Google Scholar] [CrossRef]
- Korba, B.E.; Wells, F.V.; Baldwin, B.; Cote, P.J.; Tennant, B.C.; Popper, H.; Gerin, J.L. Hepatocellular carcinoma in woodchuck hepatitis virus-infected woodchucks: Presence of viral DNA in tumor tissue from chronic carriers and animals serologically recovered from acute infections. Hepatology 1989, 9, 461–470. [Google Scholar] [CrossRef]
- Michalak, T.I.; Pardoe, I.U.; Coffin, C.S.; Churchill, N.D.; Freake, D.S.; Smith, P.; Trelegan, C.L. Occult lifelong persistence of infectious hepadnavirus and residual liver inflammation in woodchucks convalescent from acute viral hepatitis. Hepatology 1999, 29, 928–938. [Google Scholar] [CrossRef]
- Michalak, T.I.; Mulrooney, P.M.; Coffin, C.S. Low doses of hepadnavirus induce infection of the lymphatic system that does not engage the liver. J. Virol. 2004, 78, 1730–1738. [Google Scholar] [CrossRef] [Green Version]
- Gujar, S.A.; Mulrooney-Cousins, P.M.; Michalak, T.I. Repeated exposure to trace amounts of woodchuck hepadnavirus induces molecularly evident infection and virus-specific T cell response in the absence of serological infection markers and hepatitis. J. Virol. 2013, 87, 1035–1048. [Google Scholar] [CrossRef] [Green Version]
- Mitka, M. FDA: Increased HBV reactivation risk with ofatumumab or rituximab. JAMA 2013, 310, 1664. [Google Scholar] [CrossRef]
- Williams, J.B.; Huppner, A.; Mulrooney-Cousins, P.M.; Michalak, T.I. Differential expression of woodchuck toll-like receptors 1-10 in distinct forms of infection and stages of hepatitis in experimental hepatitis B virus infection. Front. Microbiol. 2018, 9, 3007. [Google Scholar] [CrossRef]
- Seto, W.K.; Tanaka, Y.; Wong, D.K.; Lai, C.L.; Shinkai, N.; Yuen, J.C.; Tong, T.; Fung, J.; Hung, I.F.; Yuen, M.F. Evidence of serologic activity in chronic hepatitis B after surface antigen (HBsAg) seroclearance documented by conventional HBsAg assay. Hepatol. Int. 2012, 7, 98–105. [Google Scholar] [CrossRef] [Green Version]
- Shinkai, N.; Matsuura, K.; Sugauchi, F.; Watanabe, T.; Murakami, S.; Iio, E.; Ogawa, S.; Nojiri, S.; Joh, T.; Tanaka, Y. Application of a newly developed high-sensitivity HBsAg chemiluminescent enzyme immunoassay for hepatitis B patients with HBsAg seroclearance. J. Clin. Microbiol. 2013, 51, 3484–3491. [Google Scholar] [CrossRef] [Green Version]
- Takeda, K.; Maruki, M.; Yamagaito, T.; Muramatsu, M.; Sakai, Y.; Tobimatsu, H.; Kobayashi, H.; Mizuno, Y.; Hamaguchi, Y. Highly sensitive detection of hepatitis B virus surface antigen by use of a semiautomated immune complex transfer chemiluminescence enzyme immunoassay. J. Clin. Microbiol. 2013, 51, 2238–2244. [Google Scholar] [CrossRef] [Green Version]
- Yang, R.; Song, G.; Guan, W.; Wang, Q.; Liu, Y.; Wei, L. The Lumipulse G HBsAg-Quant assay for screening and quantification of the hepatitis B surface antigen. J. Virol. Methods 2016, 228, 39–47. [Google Scholar] [CrossRef]
- Ozeki, I.; Nakajima, T.; Suii, H.; Tatsumi, R.; Yamaguchi, M.; Kimura, M.; Arakawa, T.; Kuwata, Y.; Ohmura, T.; Hige, S.; et al. Analysis of hepatitis B surface antigen (HBsAg) using high-sensitivity HBsAg assays in hepatitis B virus carriers in whom HBsAg seroclearance was confirmed by conventional assays. Hepatol. Res. 2018, 48, E263–E274. [Google Scholar] [CrossRef] [Green Version]
- Candotti, D.; Laperche, S. Hepatitis B virus blood screening: Need for reappraisal of blood safety measures? Front. Med. 2018, 5, 29. [Google Scholar] [CrossRef] [Green Version]
- Akram, A.; Islam, S.M.R.; Munshi, S.U.; Tabassum, S. Detection of hepatitis B virus DNA among chronic and potential occult HBV patients in resource-limited settings by loop-mediated isothermal amplifification assay. J. Viral. Hepat. 2018, 25, 1306–1311. [Google Scholar] [CrossRef]
- Caviglia, G.P.; Abate, M.L.; Tandoi, F.; Ciancio, A.; Amoroso, A.; Salizzoni, M.; Saracco, G.M.; Rizzetto, M.; Romagnoli, R.; Smedile, A. Quantitation of HBV cccDNA in anti-HBc-positive liver donors by droplet digital PCR: A new tool to detect occult infection. J. Hepatol. 2018, 69, 301–307. [Google Scholar] [CrossRef]
- Raimondo, G.; Caccamo, G.; Filomia, R.; Pollicino, T. Occult HBV infection. Semin. Immunopathol. 2013, 35, 39–52. [Google Scholar] [CrossRef] [Green Version]
- Ji, D.Z.; Pang, X.Y.; Shen, D.T.; Liu, S.N.; Goyal, H.; Xu, H.G. Global prevalence of occult hepatitis B: A systematic review and meta-analysis. J. Viral. Hepat. 2022, 29, 317–329. [Google Scholar] [CrossRef]
- Torbenson, M.; Thomas, D.L. Occult hepatitis B. Lancet Infect. Dis. 2002, 2, 479–486. [Google Scholar] [CrossRef]
- Behzad-Behbahani, A.; Mafi-Nejad, A.; Tabei, S.Z.; Lankarani, K.B.; Torab, A.; Moaddeb, A. Anti-HBc & HBV-DNA detection in blood donors negative for hepatitis B virus surface antigen in reducing risk of transfusion associated HBV infection. Indian J. Med. Res. 2006, 123, 37–42. [Google Scholar]
- El-Zayadi, A.R.; Ibrahim, E.H.; Badran, H.M.; Saeid, A.; Moneib, N.A.; Shemis, M.A.; Abdel-Sattar, R.M.; Ahmady, A.M.; El-Nakeebet, A. Anti-HBc screening in Egyptian blood donors reduces the risk of hepatitis B virus transmission. Transfus. Med. 2008, 18, 55–61. [Google Scholar] [CrossRef]
- Yuen, M.F.; Lee, C.K.; Wong, D.K.; Fung, J.; Hung, I.; Hsu, A.; But, D.Y.; Cheung, T.K.; Chan, P.; Yuen, J.C.; et al. Prevalence of occult hepatitis B infection in a highly endemic area for chronic hepatitis B: A study of a large blood donor population. Gut 2010, 59, 1389–1393. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Ye, X.; Zhang, L.; Wang, W.; Shuai, L.; Wang, A.; Zeng, J.; Candotti, D.; Allain, J.P.; Li, C. Characterization of occult hepatitis B virus infection from blood donors in China. J. Clin. Microbiol. 2011, 49, 1730–1737. [Google Scholar] [CrossRef] [Green Version]
- Torbenson, M.; Kannangai, R.; Astemborski, J.; Strathdee, S.A.; Vlahov, D.; Thomas, D.L. High prevalence of occult hepatitis B in Baltimore injection drug users. Hepatology 2004, 39, 51–57. [Google Scholar] [CrossRef]
- Kao, J.H.; Chen, P.J.; Lai, M.Y.; Chen, D.S. Occult hepatitis B virus infection and clinical outcomes of patients with chronic hepatitis C. J. Clin. Microbiol. 2002, 40, 4068–4071. [Google Scholar] [CrossRef] [Green Version]
- Lo Re, V., 3rd; Frank, I.; Gross, R.; Dockter, J.; Linnen, J.M.; Giachetti, C.; Tebas, P.; Stern, J.; Synnestvedt, M.; Localio, A.R.; et al. Prevalence, risk factors, and outcomes for occult hepatitis B virus infection among HIV-infected patients. J. Acquir. Immune Defic. Syndr. 2007, 44, 315–320. [Google Scholar] [CrossRef]
- Gupta, S.; Singh, S. Occult hepatitis B virus infection in ART-naive HIV infected patients seen at a tertiary care centre in north India. BMC Infect. Dis. 2010, 10, 53. [Google Scholar] [CrossRef] [Green Version]
- Bell, T.G.; Makondo, E.; Martinson, N.A.; Kramvis, A. Hepatitis B virus infection in human immunodeficiency virus infected southern African adults: Occult or overt–that is the question. PLoS ONE 2012, 7, e45750. [Google Scholar] [CrossRef] [Green Version]
- Mudawi, H.; Hussein, W.; Mukhtar, M.; Yousif, M.; Nemeri, O.; Glebe, D.; Kramvis, A. Overt and occult hepatitis B virus infection in adult Sudanese HIV patients. Int. J. Infect. Dis. 2014, 29, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Di Stefano, M.; Volpe, A.; Stallone, G.; Tartaglia, L.; Prato, R.; Martinelli, D.; Pastore, G.; Gesualdo, L.; Fiore, J.R. Occult HBV infection in hemodialysis setting is marked by presence of isolated antibodies to HBcAg and HCV. J. Nephrol. 2009, 22, 381–386. [Google Scholar]
- Hassan, Z.K.; Hafez, M.M.; Mansor, T.M.; Zekri, A.R. Occult HBV infection among Egyptian hepatocellular carcinoma patients. Virol. J. 2011, 8, 90. [Google Scholar] [CrossRef] [Green Version]
- Chan, H.L.; Tsang, S.W.; Leung, N.W.; Tse, C.H.; Hui, Y.; Tam, J.S.; Chan, F.K.; Sung, J.J. Occult HBV infection in cryptogenic liver cirrhosis in an area with high prevalence of HBV infection. Am. J. Gastroenterol. 2002, 97, 1211–1215. [Google Scholar] [CrossRef]
- Ghisetti, V.; Marzano, A.; Zamboni, F.; Barbui, A.; Franchello, A.; Gaia, S.; Marchiaro, G.; Salizzoni, M.; Rizzetto, M. Occult hepatitis B virus infection in HBsAg negative patients undergoing liver transplantation: Clinical significance. Liver Transpl. 2004, 10, 356–362. [Google Scholar] [CrossRef]
- Saitta, C.; Caruso, A.; Maimone, S.; Filomia, R.; Cacciola, I.; Caccamo, G.; Franzè, M.S.; Pitrone, C.; Alibrandi, A.; Gaeta, M.; et al. Antibody to hepatitis B virus core antigen positivity is a predictor of non-alcoholic fatty liver disease severity. Intern. Emerg. Med. 2022, in press. [Google Scholar] [CrossRef]
- Raimondo, G.; Saitta, C.; Lombardo, D.; Giraudi, P.J.; Rosso, N.; Ieni, A.; Lazzara, S.; Palmisano, S.; Bonazza, D.; Alibrandi, A.; et al. Occult hepatitis B virus infection predicts non-alcoholic steatohepatitis in severely obese individuals from Italy. Liver Int. 2020, 40, 1601–1609. [Google Scholar] [CrossRef]
- Raimondo, G.; Navarra, G.; Mondello, S.; Costantino, L.; Colloredo, G.; Cucinotta, E.; Di Vita, G.; Scisca, C.; Squadrito, G.; Pollicino, T. Occult hepatitis B virus in liver tissue of individuals without hepatic disease. J. Hepatol. 2008, 48, 743–746. [Google Scholar] [CrossRef]
- Spreafico, M.; Berzuini, A.; Foglieni, B.; Candotti, D.; Raffaele, L.; Guarnori, I.; Colli, A.; Maldini, F.F.; Allain, J.P.; Prati, D. Poor efficacy of nucleic acid testing in identifying occult HBV infection and consequences for safety of blood supply in Italy. J. Hepatol. 2015, 63, 1068–1076. [Google Scholar] [CrossRef]
- Cholongitas, E.; Haidich, A.B.; Apostolidou-Kiouti, F.; Chalevas, P.; Papatheodoridis, G.V. Hepatitis B virus reactivation in HBsAg-negative, anti-HBc-positive patients receiving immunosuppressive therapy: A systematic review. Ann. Gastroenterol. 2018, 31, 480–490. [Google Scholar] [CrossRef]
- Liu, C.J.; Chen, D.S.; Chen, P.J. Epidemiology of HBV infection in Asian blood donors: Emphasis on occult HBV infection and the role of NAT. J. Clin. Virol. 2006, 36 (Suppl. S1), S33–S44. [Google Scholar] [CrossRef]
- Candotti, D.; Grabarczyk, P.; Ghiazza, P.; Roig, R.; Casamitjana, N.; Iudicone, P.; Schmidt, M.; Bird, A.; Crookes, R.; Brojer, E.; et al. Characterization of occult hepatitis B virus from blood donors carrying genotype A2 or genotype D strains. J. Hepatol. 2008, 49, 537–547. [Google Scholar] [CrossRef]
- Hollinger, F.B. Hepatitis B virus infection and transfusion medicine: Science and the occult. Transfusion 2008, 48, 1001–1026. [Google Scholar] [CrossRef]
- Candotti, D.; Allain, J.P. Transfusion-transmitted hepatitis B virus infection. J. Hepatol. 2009, 51, 798–809. [Google Scholar] [CrossRef] [Green Version]
- Hollinger, F.B.; Sood, G. Occult hepatitis B virus infection: A covert operation. J. Viral. Hepat. 2010, 17, 1–15. [Google Scholar] [CrossRef]
- Stramer, S.L.; Wend, U.; Candotti, D.; Foster, G.A.; Hollinger, F.B.; Dodd, R.Y.; Allain, J.P.; Gerlich, W. Nucleic acid testing to detect HBV infection in blood donors. N. Engl. J. Med. 2011, 364, 236–247. [Google Scholar] [CrossRef] [Green Version]
- Allain, J.P.; Cox, L. Challenges in hepatitis B detection among blood donors. Curr. Opin. Hematol. 2011, 18, 461–466. [Google Scholar] [CrossRef]
- Allain, J.P.; Mihaljevic, I.; Gonzalez-Fraile, M.I.; Gubbe, K.; Holm-Harritshoj, L.; Garcia, J.M.; Brojer, E.; Erikstrup, C.; Saniewski, M.; Wernish, L.; et al. Infectivity of blood products from donors with occult hepatitis B virus infection. Transfusion 2013, 53, 1405–1415. [Google Scholar] [CrossRef]
- Cholongitas, E.; Papatheodoridis, G.V.; Burroughs, A.K. Liver grafts from anti-hepatitis B core positive donors: A systematic review. J. Hepatol. 2010, 52, 272–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, C.K.; Lo, C.M.; Man, K.; Lau, G.K. Occult hepatitis B virus infection of donor and recipient origin after liver transplantation despite nucleoside analogue prophylaxis. Liver Transpl. 2010, 16, 1314–1323. [Google Scholar] [CrossRef]
- Coffin, C.S.; Mulrooney-Cousins, P.M.; van Marle, G.; Roberts, J.P.; Michalak, T.I.; Terrault, N.A. Hepatitis B virus quasispecies in hepatic and extrahepatic viral reservoirs in liver transplant recipients on prophylactic therapy. Liver Transpl. 2011, 17, 955–962. [Google Scholar] [CrossRef] [PubMed]
- Roche, B.; Feray, C.; Gigou, M.; Roque-Afonso, A.M.; Arulnaden, J.L.; Delvart, V.; Dussaix, E.; Guettier, C.; Bismuth, H.; Samuel, D. HBV DNA persistence 10 years after liver transplantation despite successful anti-HBS passive immunoprophylaxis. Hepatology 2003, 38, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Soldevila-Pico, C.; Emre, S.; Luketic, V.; Lok, A.S.; NIH HBV-OLT Study Group. Presence of intrahepatic (total and ccc) HBV DNA is not predictive of HBV recurrence after liver transplantation. Liver Transpl. 2007, 13, 1137–1144. [Google Scholar] [CrossRef] [Green Version]
- Toniutto, P.; Minisini, R.; Fabris, C.; De Feo, T.; Marangoni, F.; Burlone, M.; Avellini, C.; Bitetto, D.; Fornasiere, E.; Fumolo, E.; et al. Occult hepatitis B virus infection in liver transplant recipients with recurrent hepatitis C: Relationship with donor age and fibrosis progression. Clin. Transplant. 2009, 23, 184–190. [Google Scholar] [CrossRef]
- Kusumoto, S.; Tanaka, Y.; Mizokami, M.; Ueda, R. Reactivation of hepatitis B virus following systemic chemotherapy for malignant lymphoma. Int. J. Hematol. 2009, 90, 13–23. [Google Scholar] [CrossRef]
- Hammond, S.P.; Borchelt, A.M.; Ukomadu, C.; Ho, V.T.; Baden, L.R.; Marty, F.M. Hepatitis B virus reactivation following allogeneic hematopoietic stem cell transplantation. Biol. Blood Marrow Transplant. 2009, 15, 1049–1059. [Google Scholar] [CrossRef] [Green Version]
- Yeo, W.; Chan, T.C.; Leung, N.W.; Lam, W.Y.; Mo, F.K.; Chu, M.T.; Chan, H.L.; Hui, E.P.; Lei, K.I.; Mok, T.S.; et al. Hepatitis B virus reactivation in lymphoma patients with prior resolved hepatitis B undergoing anticancer therapy with or without rituximab. J. Clin. Oncol. 2009, 27, 605–611. [Google Scholar] [CrossRef]
- Pei, S.N.; Chen, C.H.; Lee, C.M.; Wang, M.C.; Ma, M.C.; Hu, T.H.; Kuo, C.Y. Reactivation of hepatitis B virus following rituximab-based regimens: A serious complication in both HBsAg-positive and HBsAg-negative patients. Ann. Hematol. 2010, 89, 255–262. [Google Scholar] [CrossRef]
- Hsu, C.; Tsou, H.H.; Lin, S.J.; Wang, M.C.; Yao, M.; Hwang, W.L.; Kao, W.Y.; Chiu, C.F.; Lin, S.F.; Lin, J.; et al. Chemotherapy-induced hepatitis B reactivation in lymphoma patients with resolved HBV infection: A prospective study. Hepatology 2014, 59, 2092–2100. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Saxena, A.; Terrin, N.; Viveiros, K.; Balk, E.M.; Wong, J.B. Hepatitis B virus reactivation and prophylaxis during solid tumor chemotherapy: A systematic review and meta-analysis. Ann. Intern. Med. 2016, 164, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Giannitti, C.; Lopalco, G.; Vitale, A.; Rigante, D.; Anelli, M.G.; Fabbroni, M.; Manganelli, S.; Galeazzi, M.; Frediani, B.; Barone, M.; et al. Long-term safety of anti-TNF agents on the liver of patients with spondyloarthritis and potential occult hepatitis B viral infection: An observational multicentre study. Clin. Exp. Rheumatol. 2017, 35, 93–97. [Google Scholar] [PubMed]
- Pauly, M.P.; Tucker, L.Y.; Szpakowski, J.L.; Ready, J.B.; Baer, D.; Hwang, J.; Lok, A.S. Incidence of hepatitis B virus reactivation and hepatotoxicity in patients receiving long-term treatment with tumor necrosis factor antagonists. Clin. Gastroenterol. Hepatol. 2018, 16, 1964–1973. [Google Scholar] [CrossRef] [Green Version]
- Mucke, M.M.; Backus, L.I.; Mucke, V.T.; Coppola, N.; Preda, C.M.; Yeh, M.L.; Tang, L.S.; Belperio, P.S.; Wilson, E.M.; Yu, M.L.; et al. Hepatitis B virus reactivation during direct-acting antiviral therapy for hepatitis C: A systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 2018, 3, 172–180. [Google Scholar] [CrossRef]
- Tamori, A.; Abiru, S.; Enomoto, H.; Kioka, K.; Korenaga, M.; Tani, J.; Enomoto, M.; Sugiyama, M.; Masaki, T.; Kawada, N.; et al. Low incidence of hepatitis B virus reactivation and subsequent hepatitis in patients with chronic hepatitis C receiving direct-acting antiviral therapy. J. Viral Hepat. 2018, 25, 608–611. [Google Scholar] [CrossRef]
- Bloquel, B.; Jeulin, H.; Burty, C.; Letranchant, L.; Rabaud, C.; Venard, V. Occult hepatitis B infection in patients infected with HIV: Report of two cases of hepatitis B reactivation and prevalence in a hospital cohort. J. Med. Virol. 2010, 82, 206–212. [Google Scholar] [CrossRef]
- Soriano, V.; Aguilera, A.; Gonzalez, R.; Gomez-Gallego, F.; Barea, L.; Treviño, M.; Corral, O. Occult hepatitis B and HIV infection. Eur. J. Gastroenterol. Hepatol. 2019, 31, 1403–1407. [Google Scholar] [CrossRef]
- Onozawa, M.; Hashino, S.; Izumiyama, K.; Kahata, K.; Chuma, M.; Mori, A.; Kondo, T.; Toyoshima, N.; Ota, S.; Kobayashi, S.; et al. Progressive disappearance of anti-hepatitis B surface antigen antibody and reverse seroconversion after allogeneic hematopoietic stem cell transplantation in patients with previous hepatitis B virus infection. Transplantation 2005, 79, 616–619. [Google Scholar] [CrossRef]
- Viganò, M.; Vener, C.; Lampertico, P.; Annaloro, C.; Pichoud, C.; Zoulim, F.; Facchetti, F.; Poli, F.; Scalamogna, M.; Deliliers, G.L.; et al. Risk of hepatitis B surface antigen seroreversion after allogeneic hematopoietic SCT. Bone Marrow Transplant. 2011, 46, 125–131. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL 2017 clinical practice guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bréchot, C.; Thiers, V.; Kremsdorf, D.; Nalpas, B.; Pol, S.; Paterlini-Bréchot, P. Persistent hepatitis B virus infection in subjects without hepatitis B surface antigen: Clinically significant or purely “occult”? Hepatology 2001, 34, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Blackberg, J.; Kidd-Ljunggren, K. Occult hepatitis B virus after acute self-limited infection persisting for 30 years without sequence variation. J. Hepatol. 2000, 33, 992–997. [Google Scholar] [CrossRef]
- Yuki, N.; Nagaoka, T.; Yamashiro, M.; Mochizuki, K.; Kaneko, A.; Yamamoto, K.; Omura, M.; Hikiji, K.; Kato, M. Long-term histologic and virologic outcomes of acute self-limited hepatitis B. Hepatology 2003, 37, 1172–1179. [Google Scholar] [CrossRef]
- Coffin, C.S.; Pham, T.N.; Mulrooney, P.M.; Churchill, N.D.; Michalak, T.I. Persistence of isolated antibodies to woodchuck hepatitis virus core antigen is indicative of occult infection. Hepatology 2004, 40, 1053–1061. [Google Scholar] [CrossRef]
- Mulrooney-Cousins, P.M.; Michalak, T.I. Persistent occult hepatitis B virus infection: Experimental findings and clinical implications. World J. Gastroenterol. 2007, 13, 5682–5686. [Google Scholar] [CrossRef] [Green Version]
- Shetty, K.; Hussain, M.; Nei, L.; Reddy, K.R.; Lok, A.S. Prevalence and significance of occult hepatitis B in a liver transplant population with chronic hepatitis C. Liver Transpl. 2008, 14, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Squadrito, G.; Cacciola, I.; Alibrandi, A.; Pollicino, T.; Raimondo, G. Impact of occult hepatitis B virus infection on the outcome of chronic hepatitis C. J. Hepatol. 2013, 59, 696–700. [Google Scholar] [CrossRef]
- Wang, H.; Swann, R.; Thomas, E.; Innes, H.A.; Valerio, H.; Hayes, P.C.; Allen, S.; Barclay, S.T.; Wilks, D.; Fox, R.; et al. Impact of previous hepatitis B infection on the clinical outcomes from chronic hepatitis C? A population-level analysis. J. Viral Hepat. 2018, 25, 930–938. [Google Scholar] [CrossRef]
- Covolo, L.; Pollicino, T.; Raimondo, G.; Donato, F. Occult hepatitis B virus and the risk for chronic liver disease: A meta-analysis. Dig. Liver. Dis. 2013, 45, 238–244. [Google Scholar] [CrossRef]
- Franzè, M.S.; Pollicino, T.; Raimondo, G.; Squadrito, G. Occult hepatitis B virus infection in hepatitis C virus negative chronic liver diseases. Liver Int. 2022, 42, 963–972. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.; Everhart, J.E.; Di Bisceglie, A.M.; Kim, H.Y.; Hussain, M.; Morgan, T.R.; HALT-C trial group. Occult and previous hepatitis B virus infection are not associated with hepatocellular carcinoma in United States patients with chronic hepatitis C. Hepatology 2011, 54, 434–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raimondo, G.; Pollicino, T.; Squadrito, G. What is the clinical impact of occult hepatitis B virus infection? Lancet 2005, 365, 638–640. [Google Scholar] [CrossRef]
- Huang, X.; Hollinger, F.B. Occult hepatitis B virus infection and hepatocellular carcinoma: A systematic review. J. Viral Hepat. 2014, 21, 153–162. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zhao, H.; Yang, X.; Gao, J.Y.; Cheng, J. HBsAg-negative hepatitis B virus infection and hepatocellular carcinoma. Discov. Med. 2014, 18, 189–193. [Google Scholar] [PubMed]
- Kwak, M.S.; Kim, Y.J. Occult hepatitis B virus infection. World J. Hepatol. 2014, 6, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Makvandi, M. Update on occult hepatitis B virus infection. World J. Gastroenterol. 2016, 22, 8720–8734. [Google Scholar] [CrossRef]
- Yip, T.C.; Wong, G.L. Current knowledge of occult hepatitis B infection and clinical implications. Semin. Liver Dis. 2019, 39, 249–260. [Google Scholar] [CrossRef]
- Mak, L.Y.; Wong, D.K.; Pollicino, T.; Raimondo, G.; Hollinger, F.B.; Yuen, M.F. Occult hepatitis B infection and hepatocellular carcinoma: Epidemiology, virology, hepatocarcinogenesis and clinical significance. J. Hepatol. 2020, 73, 952–964. [Google Scholar] [CrossRef]
- Pollicino, T.; Saitta, C.; Raimondo, G. Hepatocellular carcinoma: The point of view of the hepatitis B virus. Carcinogenesis 2011, 32, 1122–1132. [Google Scholar] [CrossRef]
- Shi, Y.; Wu, Y.H.; Wu, W.; Zhang, W.J.; Yang, J.; Chen, Z. Association between occult hepatitis B infection and the risk of hepatocellular carcinoma: A meta-analysis. Liver Int. 2012, 32, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Pollicino, T.; Saitta, C. Occult hepatitis B virus and hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 5951–5961. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Shang, Q.L.; Liu, J.Y.; Li, D.; Xu, W.Z.; Teng, X.; Zhao, H.W.; Fu, L.J.; Zhang, F.M.; Gu, H.X. Prevalence of occult hepatitis B virus infection among hepatopathy patients and healthy people in China. J. Infect. 2009, 58, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Kobayashi, M.; Someya, T.; Saitoh, S.; Hosaka, T.; Akuta, N.; Suzuki, F.; Arase, Y.; Kumada, H. Occult hepatitis B virus infection increases hepatocellular carcinogenesis by eight times in patients with non-B, non-C liver cirrhosis: A cohort study. J. Viral Hepat. 2009, 16, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Wong, D.K.; Cheng, S.C.Y.; Mak, L.L.; To, E.W.; Lo, R.C.; Cheung, T.T.; Seto, W.K.; Fung, J.; Man, K.; Lai, C.L.; et al. Among patients with undetectable hepatitis B surface antigen and hepatocellular carcinoma, a high proportion has integration of HBV DNA into hepatocyte DNA and no cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 18, 449–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yotsuyanagi, H.; Shintani, Y.; Moriya, K.; Fujie, H.; Tsutsumi, T.; Kato, T.; Nishioka, K.; Takayama, T.; Makuuchi, M.; Iino, S.; et al. Virologic analysis of non-B, non-C hepatocellular carcinoma in Japan: Frequent involvement of hepatitis B virus. J. Infect. Dis. 2000, 181, 1920–1928. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.H.; Changchien, C.S.; Lee, C.M.; Tung, W.C.; Hung, C.H.; Hu, T.H.; Wang, J.H.; Wang, J.C.; Lu, S.N. A study on sequence variations in pre-S/surface, X and enhancer II/core promoter/precore regions of occult hepatitis B virus in non-B, non-C hepatocellular carcinoma patients in Taiwan. Int. J. Cancer 2009, 125, 621–629. [Google Scholar] [CrossRef]
- Koike, K.; Shimotouno, K.; Okada, S.; Okamoto, H.; Hayashi, N.; Ueda, K.; Kaneko, S.; Koike, K.; Yokosuka, O.; Chiba, T.; et al. Survey of hepatitis B virus co-infection in hepatitis C virus-infected patients suffering from chronic hepatitis and hepatocellular carcinoma in Japan. Jpn. J. Cancer Res. 1999, 90, 1270–1272. [Google Scholar] [CrossRef]
- Tanaka, T.; Inoue, K.; Hayashi, Y.; Abe, A.; Tsukiyama-Kohara, K.; Nuriya, H.; Aoki, Y.; Kawaguchi, R.; Kubota, K.; Yoshiba, M.; et al. Virological significance of low-level hepatitis B virus infection in patients with hepatitis C virus associated liver disease. J. Med. Virol. 2004, 72, 223–229. [Google Scholar] [CrossRef]
- Momosaki, S.; Nakashima, Y.; Kojiro, M.; Tabor, E. HBsAg-negative hepatitis B virus infections in hepatitis C virus-associated hepatocellular carcinoma. J. Viral Hepat. 2005, 12, 325–329. [Google Scholar] [CrossRef]
- Obika, M.; Shinji, T.; Fujioka, S.; Terada, R.; Ryuko, H.; Lwin, A.A.; Shiraha, H.; Koide, N. Hepatitis B virus DNA in liver tissue and risk for hepatocarcinogenesis in patients with hepatitis C virus-related chronic liver disease. A prospective study. Intervirology 2008, 51, 59–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Maksoud, M.A.; Habeeb, M.R.; Ghazy, H.F.; Nomir, M.M.; Elalfy, H.; Abed, S.; Zaki, M.E.S. Clinicopathological study of occult hepatitis B virus infection in hepatitis C virus-associated hepatocellular carcinoma. Eur. J. Gastroenterol. Hepatol. 2019, 31, 716–722. [Google Scholar] [CrossRef] [PubMed]
- Squadrito, G.; Pollicino, T.; Cacciola, I.; Caccamo, G.; Villari, D.; La Masa, T.; Restuccia, T.; Cucinotta, E.; Scisca, C.; Magazzu, D.; et al. Occult hepatitis B virus infection is associated with the development of hepatocellular carcinoma in chronic hepatitis C patients. Cancer 2006, 106, 1326–1330. [Google Scholar] [CrossRef] [PubMed]
- Brechot, C. Pathogenesis of hepatitis B virus-related hepatocellular carcinoma: Old and new paradigms. Gastroenterology 2004, 127, S56–S61. [Google Scholar] [CrossRef]
- Tamori, A.; Nishiguchi, S.; Kubo, S.; Enomoto, M.; Koh, N.; Takeda, T.; Shiomi, S.; Hirohashi, K.; Kinoshita, H.; Otani, S. Sequencing of human-viral DNA junctions in hepatocellular carcinoma from patients with HCV and occult HBV infection. J. Med. Virol. 2003, 69, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Saigo, K.; Takashima, H.; Minami, M.; Okanoue, T.; Bréchot, C.; Paterlini-Bréchot, P. Large scaled analysis of hepatitis B virus (HBV) DNA integration in HBV related hepatocellular carcinomas. Gut 2005, 54, 1162–1168. [Google Scholar] [CrossRef]
- Saitta, C.; Tripodi, G.; Barbera, A.; Bertuccio, A.; Smedile, A.; Ciancio, A.; Raffa, G.; Sangiovanni, A.; Navarra, G.; Raimondo, G.; et al. Hepatitis B virus (HBV) DNA integration in patients with occult HBV infection and hepatocellular carcinoma. Liver Int. 2015, 35, 2311–2317. [Google Scholar] [CrossRef] [Green Version]
- Fujimoto, A.; Furuta, M.; Totoki, Y.; Tsunoda, T.; Kato, M.; Shiraishi, Y.; Tanaka, H.; Taniguchi, H.; Kawakami, Y.; Ueno, M.; et al. Whole-genome mutational landscape and characterization of noncoding and structural mutations in liver cancer. Nat. Genet. 2016, 48, 500–509. [Google Scholar] [CrossRef]
- Chen, X.P.; Long, X.; Jia, W.L.; Wu, H.J.; Zhao, J.; Liang, H.F.; Laurence, A.; Zhu, J.; Dong, D.; Chen, Y.; et al. Viral integration drives multifocal HCC during the occult HBV infection. J. Exp. Clin. Cancer Res. 2019, 38, 261. [Google Scholar] [CrossRef] [Green Version]
- Bonilla Guerrero, R.; Roberts, L.R. The role of hepatitis B virus integrations in the pathogenesis of human hepatocellular carcinoma. J. Hepatol. 2005, 42, 760–777. [Google Scholar] [CrossRef]
- Levrero, M.; Zucman-Rossi, J. Mechanisms of HBV-induced hepatocellular carcinoma. J. Hepatol. 2016, 64, S84–S101. [Google Scholar] [CrossRef] [PubMed]
- Urashima, T.; Saigo, K.; Kobayashi, S.; Imaseki, H.; Matsubara, H.; Koide, Y.; Asano, T.; Kondo, Y.; Koike, K.; Isono, K. Identification of hepatitis B virus integration in hepatitis C virus-infected hepatocellular carcinoma tissues. J. Hepatol. 1997, 26, 771–778. [Google Scholar] [CrossRef]
- Poussin, K.; Dienes, H.; Sirma, H.; Urban, S.; Beaugrand, M.; Franco, D.; Schirmacher, P.; Bréchot, C.; Paterlini Bréchot, P. Expression of mutated hepatitis B virus X genes in human hepatocellular carcinomas. Int. J. Cancer 1999, 80, 497–505. [Google Scholar] [CrossRef]
- Chami, M.; Gozuacik, D.; Saigo, K.; Capiod, T.; Falson, P.; Lecoeur, H.; Urashima, T.; Beckman, J.; Gougeon, M.L.; Claret, M.; et al. Hepatitis B virus-related insertional mutagenesis implicates SERCA1 gene in the control of apoptosis. Oncogene 2000, 19, 2877–2886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamori, A.; Nishiguchi, S.; Kubo, S.; Narimatsu, T.; Habu, D.; Takeda, T.; Hirohashi, H.; Shiomi, S. HBV DNA integration and HBV-transcript expression in non-B, non-C hepatocellular carcinoma in Japan. J. Med. Virol. 2003, 71, 492–498. [Google Scholar] [CrossRef]
- Pollicino, T.; Vegetti, A.; Saitta, C.; Ferrara, F.; Corradini, E.; Raffa, G.; Pietrangelo, A.; Raimondo, G. Hepatitis B virus DNA integration in tumour tissue of a non-cirrhotic HFE-haemochromatosis patient with hepatocellular carcinoma. J. Hepatol. 2013, 58, 190–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuzaki, Y.; Chiba, T.; Hadama, T.; Asaoka, H.; Doy, M.; Shoda, J.; Tanaka, N.; Kinoshita, M. HBV genome integration and genetic instability in HBsAg-negative and anti-HCV-positive hepatocellular carcinoma in Japan. Cancer Lett. 1997, 119, 53–61. [Google Scholar] [CrossRef]
- Saitta, C.; Lanza, M.; Bertuccio, A.; Lazzara, S.; Navarra, G.; Raimondo, G.; Pollicino, T. Evaluation of CTNNB1 and TP53 variability in patients with hepatocellular carcinoma and occult hepatitis B virus infection. Cancer Genet. 2015, 208, 513–516. [Google Scholar] [CrossRef]
- Hatazawa, Y.; Yano, Y.; Okada, R.; Tanahashi, T.; Hayashi, H.; Hirano, H.; Minami, A.; Kawano, Y.; Tanaka, M.; Fukumoto, T.; et al. Quasispecies variant of pre-S/S gene in HBV-related hepatocellular carcinoma with HBs antigen positive and occult infection. Infect. Agents Cancer 2018, 13, 7. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saitta, C.; Pollicino, T.; Raimondo, G. Occult Hepatitis B Virus Infection: An Update. Viruses 2022, 14, 1504. https://doi.org/10.3390/v14071504
Saitta C, Pollicino T, Raimondo G. Occult Hepatitis B Virus Infection: An Update. Viruses. 2022; 14(7):1504. https://doi.org/10.3390/v14071504
Chicago/Turabian StyleSaitta, Carlo, Teresa Pollicino, and Giovanni Raimondo. 2022. "Occult Hepatitis B Virus Infection: An Update" Viruses 14, no. 7: 1504. https://doi.org/10.3390/v14071504