
A Review on Equine Influenza from a Human Influenza Perspective


Abstract
:1. Introduction
2. Pathogenesis, Immune Responses, and Clinical Aspects
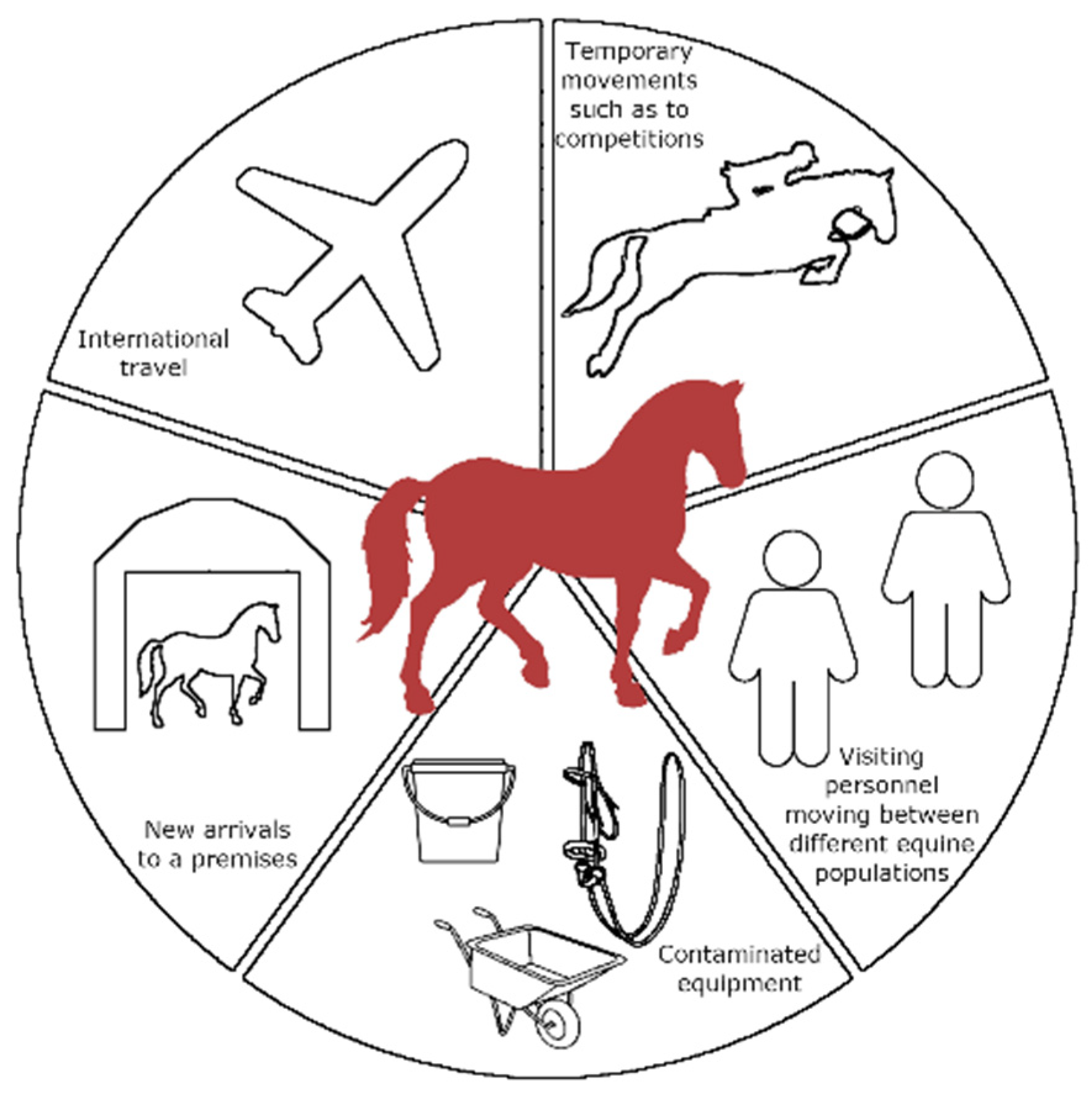
3. Epidemiology including Factors Contributing to Local, National, and International Transmission
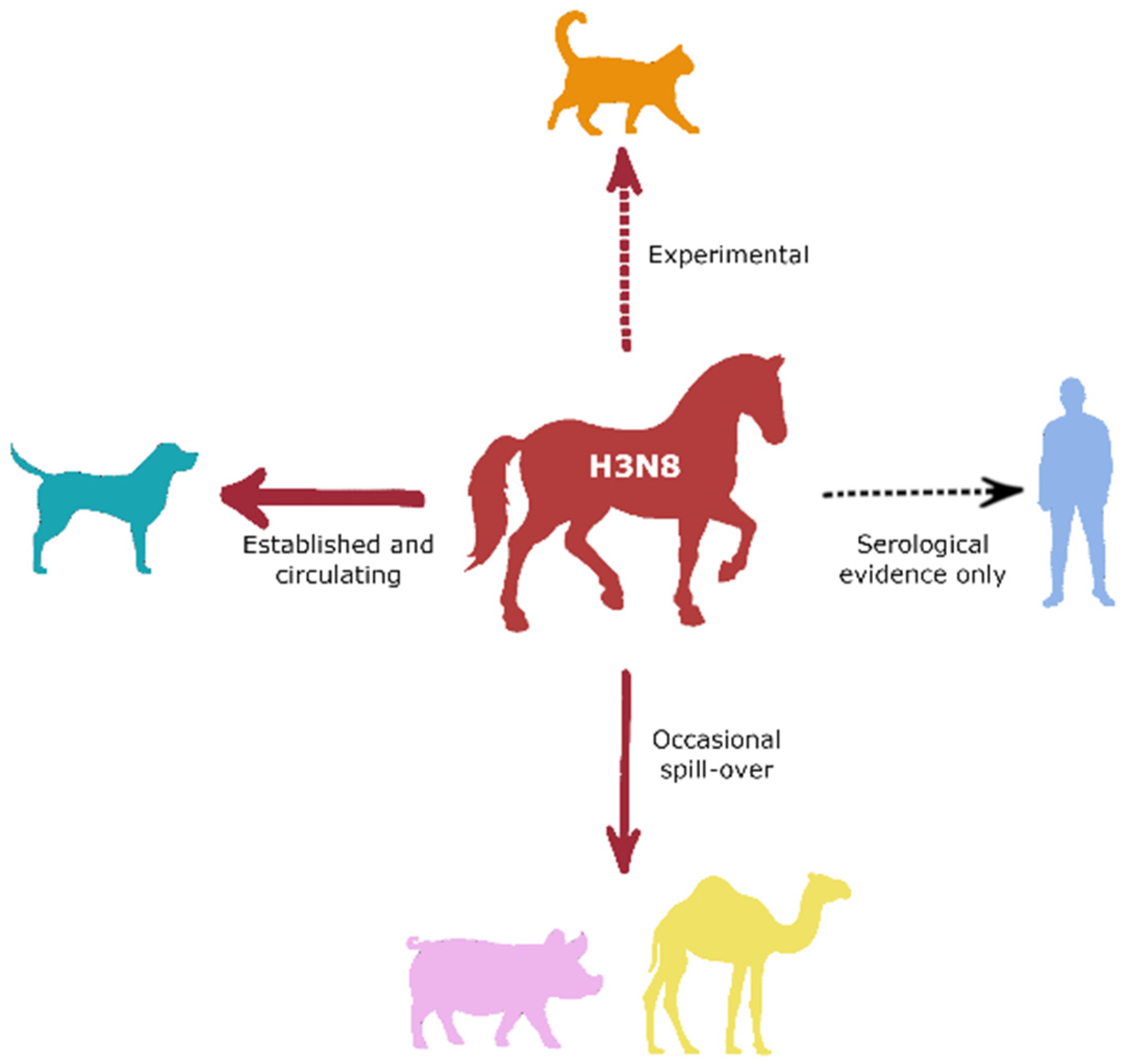
4. Cross-Species Transmission Threats
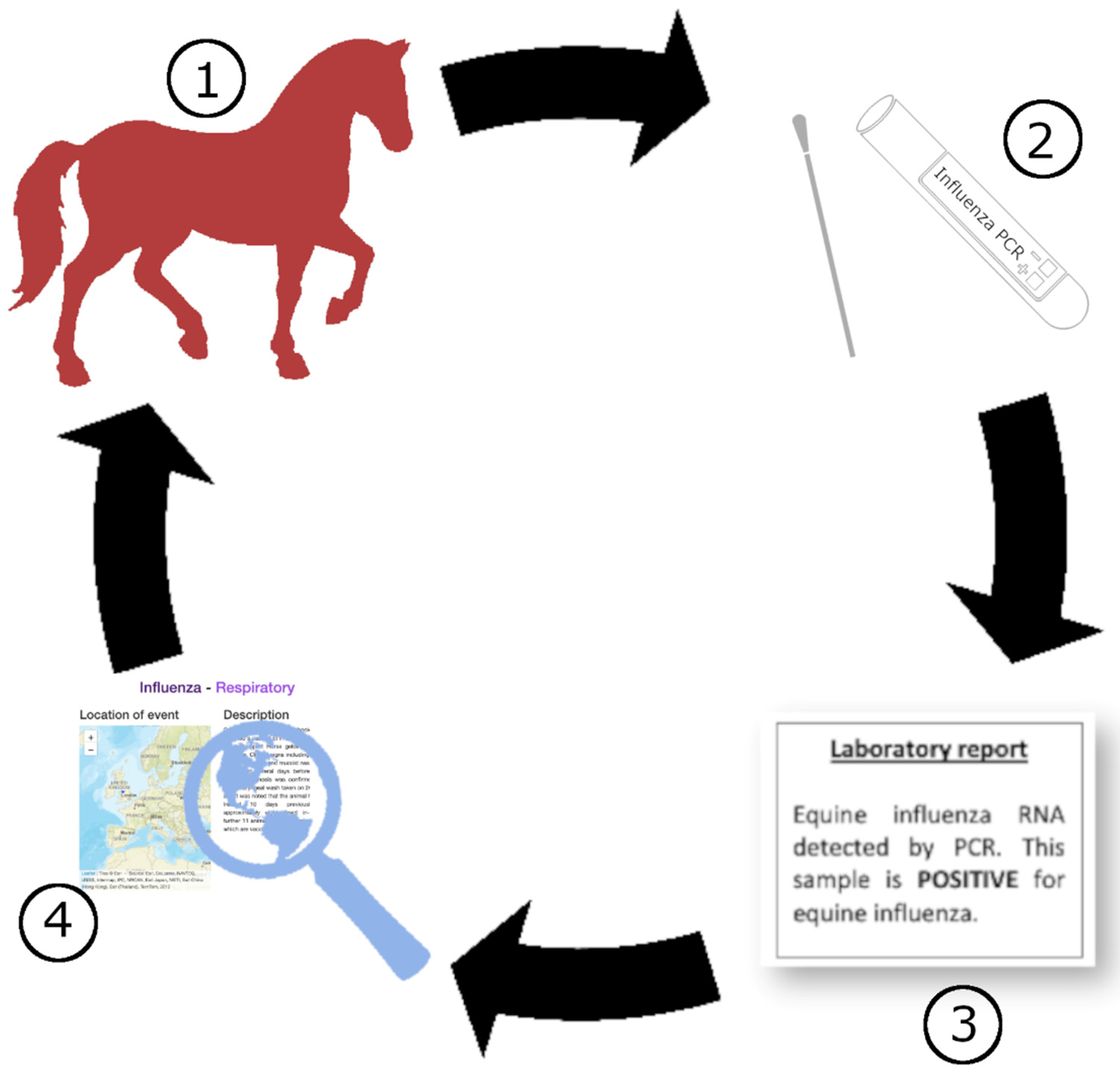
5. Surveillance
6. Preventive Measures
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Parrish, C.R.; Murcia, P.R.; Holmes, E.C. Influenza Virus Reservoirs and Intermediate Hosts: Dogs, Horses, and New Possibilities for Influenza Virus Exposure of Humans. J. Virol. 2015, 89, 2990–2994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirkland, P.D.; Finlaison, D.S.; Crispe, E.; Hurt, A.C. Influenza Virus Transmission from Horses to Dogs, Australia. Emerg. Infect. Dis. 2010, 16, 699–702. [Google Scholar] [CrossRef] [PubMed]
- Tong, S.; Li, Y.; Rivailler, P.; Conrardy, C.; Alvarez Castillo, D.A.; Chen, L.M.; Recuenco, S.; Ellison, J.A.; Davis, C.T.; York, I.A.; et al. A Distinct Lineage of Influenza A Virus from Bats. Proc. Natl. Acad. Sci. USA 2012, 109, 4269–4274. [Google Scholar] [CrossRef] [PubMed]
- Fereidouni, S.; Munoz, O.; von Dobschuetz, S.; de Nardi, M. Influenza Virus Infection of Marine Mammals. Ecohealth 2016, 13, 161–170. [Google Scholar] [CrossRef]
- Borland, S.; Gracieux, P.; Jones, M.; Mallet, F.; Yugueros-Marcos, J. Influenza A Virus Infection in Cats and Dogs: A Literature Review in the Light of the “One Health” Concept. Front. Public Health 2020, 8, 83. [Google Scholar] [CrossRef]
- Zhang, M.; Liu, M.; Bai, S.; Zhao, C.; Li, Z.; Xu, J.; Zhang, X. Influenza A Virus–Host Specificity: An Ongoing Cross-Talk Between Viral and Host Factors. Front. Microbiol. 2021, 12, 3429. [Google Scholar] [CrossRef]
- Potter, C.W. Chronicle of Influenza Pandemics. In Textbook of Influenza; Nicholson, K.G., Webster, R.F., Hay, A.J., Eds.; Blackwell Science Ltd.: Oxford, UK, 1998; pp. 3–18. [Google Scholar]
- Webster, R.G.; Bean, W.J.; Gorman, O.T.; Chambers, T.M.; Kawaoka, Y. Evolution and Ecology of Influenza A Viruses. Microbiol. Rev. 1992, 56, 152–179. [Google Scholar] [CrossRef]
- Palese, P.; Schulman, J.L. Mapping of the Influenza Virus Genome: Identification of the Hemagglutinin and the Neuraminidase Genes. Proc. Natl. Acad. Sci. USA 1976, 73, 2142–2146. [Google Scholar] [CrossRef] [Green Version]
- Shao, W.; Li, X.; Goraya, M.U.; Wang, S.; Chen, J.L. Evolution of Influenza A Virus by Mutation and Re-Assortment. Int. J. Mol. Sci. 2017, 18, 1650. [Google Scholar] [CrossRef] [Green Version]
- Murcia, P.R.; Wood, J.L.N.; Holmes, E.C. Genome-Scale Evolution and Phylodynamics of Equine H3N8 Influenza A Virus. J. Virol. 2011, 85, 5312–5322. [Google Scholar] [CrossRef] [Green Version]
- Ma, W.; Kahn, R.E.; Richt, J.A. The Pig as a Mixing Vessel for Influenza Viruses: Human and Veterinary Implications. J. Mol. Med. 2009, 3, 158–166. [Google Scholar] [CrossRef]
- Cullinane, A.; Elton, D.; Mumford, J. Equine Influenza—Surveillance and Control. Influenza Other Respir. Viruses 2010, 4, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Monto, A.S.; Gravenstein, S.; Elliott, M.; Colopy, M.; Schweinle, J. Clinical Signs and Symptoms Predicting Influenza Infection. Arch. Intern. Med. 2000, 160, 3243–3247. [Google Scholar] [CrossRef] [Green Version]
- Sellon, D.C.; Long, M.T. Equine Infectious Diseases, 2nd ed.; Saunders: Philadelphia, PA, USA, 2013. [Google Scholar]
- Salathé, M.; Kazandjieva, M.; Lee, J.W.; Levis, P.; Feldman, M.W.; Jones, J.H. A High-Resolution Human Contact Network for Infectious Disease Transmission. Proc. Natl. Acad. Sci. USA 2010, 107, 22020–22025. [Google Scholar] [CrossRef] [Green Version]
- Newton, J.R.; Daly, J.M.; Spencer, L.; Mumford, J.A. Description of the Outbreak of Equine Influenza (H3N8) in the United Kingdom in 2003, during Which Recently Vaccinated Horses in Newmarket Developed Respiratory Disease. Vet. Rec. 2006, 158, 185–192. [Google Scholar] [CrossRef]
- Morley, P.S.; Townsend, H.G.G.; Bogdan, J.R.; Haines, D.M. Risk Factors for Disease Associated with Influenza Virus Infections during Three Epidemics in Horses. J. Am. Vet. Med. Assoc. 2000, 216, 545–550. [Google Scholar] [CrossRef]
- Cullinane, A. Equine Influenza and Air Transport. Equine Vet. Educ. 2014, 26, 456–457. [Google Scholar] [CrossRef] [PubMed]
- ICC Viewer. Available online: https://equinesurveillance.org/iccview/ (accessed on 8 December 2021).
- Influenza (Seasonal). Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 8 December 2021).
- Long, J.S.; Mistry, B.; Haslam, S.M.; Barclay, W.S. Host and Viral Determinants of Influenza A Virus Species Specificity. Nat. Rev. Microbiol. 2019, 17, 67–81. [Google Scholar] [CrossRef] [PubMed]
- Bailey, E.S.; Choi, J.Y.; Fieldhouse, J.K.; Borkenhagen, L.K.; Zemke, J.; Zhang, D.; Gray, G.C. The Continual Threat of Influenza Virus Infections at the Human–Animal Interface What Is New from a One Health Perspective? Evol. Med. Public Health 2018, 2018, 192–198. [Google Scholar] [CrossRef]
- Treanor, J.J. Influenza (Including Avian Influenza and Swine Influenza). In Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 8th ed.; Bennett, J.E., Dolin, R., Blaser, M.J., Eds.; W.B. Saunders: Philadelphia, PA, USA, 2015; Volume 2, pp. 2000–2024.e6. [Google Scholar] [CrossRef]
- Kuiken, T.; Riteau, B.; Fouchier, R.A.M.; Rimmelzwaan, G.F. Pathogenesis of Influenza Virus Infections: The Good, the Bad and the Ugly. Curr. Opin. Virol. 2012, 2, 276–286. [Google Scholar] [CrossRef]
- Zambon, M.C. The Pathogenesis of Influenza in Humans. Rev. Med. Virol. 2001, 11, 227–241. [Google Scholar] [CrossRef] [PubMed]
- Rogers, G.N.; Paulson, J.C. Receptor Determinants of Human and Animal Influenza Virus Isolates: Differences in Receptor Specificity of the H3 Hemagglutinin Based on Species of Origin. Virol. J. 1983, 127, 361–373. [Google Scholar] [CrossRef]
- Suzuki, Y.; Ito, T.; Suzuki, T.; Holland, R.E.; Chambers, T.M.; Kiso, M.; Ishida, H.; Kawaoka, Y. Sialic Acid Species as a Determinant of the Host Range of Influenza A Viruses. J. Virol. 2000, 74, 11825–11831. [Google Scholar] [CrossRef] [Green Version]
- Reperant, L.A.; Kuiken, T.; Grenfell, B.T.; Osterhaus, A.D.M.E.; Dobson, A.P. Linking Influenza Virus Tissue Tropism to Population-Level Reproductive Fitness. PLoS ONE 2012, 7, e43115. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, K.G. Viral Tropism and the Pathogenesis of Influenza in the Mammalian Host. Am. J. Pathol. 2007, 171, 1089–1092. [Google Scholar] [CrossRef] [Green Version]
- Fujikura, D.; Miyazaki, T. Programmed Cell Death in the Pathogenesis of Influenza. Int. J. Mol. Sci. 2018, 19, 2065. [Google Scholar] [CrossRef] [Green Version]
- Iwasaki, A.; Pillai, P.S. Innate Immunity to Influenza Virus Infection. Nat. Rev. Immunol. 2014, 14, 315–328. [Google Scholar] [CrossRef]
- Kreijtz, J.H.C.M.; Fouchier, R.A.M.; Rimmelzwaan, G.F. Immune Responses to Influenza Virus Infection. Virus Res. 2011, 162, 19–30. [Google Scholar] [CrossRef]
- Horohov, D.W. The Equine Immune Responses to Infectious and Allergic Disease: A Model for Humans? Mol. Immunol. 2015, 66, 89–96. [Google Scholar] [CrossRef]
- Ricketts, S.; Troedsson, M.H.T. Fertility Expectations and Management for Optimal Fertility. In Current Therapy in Equine Reproduction; Elsevier: Amsterdam, The Netherlands, 2007; pp. 53–69. [Google Scholar] [CrossRef]
- Bahadoran, A.; Lee, S.H.; Wang, S.M.; Manikam, R.; Rajarajeswaran, J.; Raju, C.S.; Sekaran, S.D. Immune Responses to Influenza Virus and Its Correlation to Age and Inherited Factors. Front. Microbiol. 2016, 7, 1841. [Google Scholar] [CrossRef] [Green Version]
- McFarlane, D. Immune Dysfunction in Aged Horses. Vet. Clin. N. Am. Equine Pract. 2016, 32, 333–341. [Google Scholar] [CrossRef]
- Sasaki, S.; Sullivan, M.; Narvaez, C.F.; Holmes, T.H.; Furman, D.; Zheng, N.Y.; Nishtala, M.; Wrammert, J.; Smith, K.; James, J.A.; et al. Limited Efficacy of Inactivated Influenza Vaccine in Elderly Individuals Is Associated with Decreased Production of Vaccine-Specific Antibodies. J. Clin. Invest. 2011, 121, 3109–3119. [Google Scholar] [CrossRef] [Green Version]
- Muirhead, T.L.; McClure, J.T.; Wichtel, J.J.; Stryhn, H.; Markham, R.J.F.; McFarlane, D.; Lunn, D.P. The Effect of Age on the Immune Response of Horses to Vaccination. J. Comp. Pathol. 2010, 142, S85–S90. [Google Scholar] [CrossRef]
- Folsom, R.W.; Littlefield-Chabaud, M.A.; French, D.D.; Pourciau, S.S.; Mistric, L.; Horohov, D.W. Exercise Alters the Immune Response to Equine Influenza Virus and Increases Susceptibility to Infection. Equine Vet. J. 2001, 33, 664–669. [Google Scholar] [CrossRef]
- Murphy, E.A.; Davis, J.M.; Carmichael, M.D.; Gangemi, J.D.; Ghaffar, A.; Mayer, E.P. Exercise Stress Increases Susceptibility to Influenza Infection. Brain Behav. Immun. 2008, 22, 1152–1155. [Google Scholar] [CrossRef]
- Meijer, W.J.; Linn, F.H.H.; Wensing, A.M.J.; Leavis, H.L.; van Riel, D.; GeurtsvanKessel, C.H.; Wattjes, M.P.; Murk, J.L. Acute Influenza Virus-Associated Encephalitis and Encephalopathy in Adults: A Challenging Diagnosis. JMM Case Rep. 2016, 3, e005076. [Google Scholar] [CrossRef]
- Daly, J.M.; Whitwell, K.E.; Miller, J.; Dowd, G.; Cardwell, J.M.; Smith, K.C. Investigation of Equine Influenza Cases Exhibiting Neurological Disease: Coincidence or Association? J. Comp. Pathol. 2006, 134, 231–235. [Google Scholar] [CrossRef]
- Hancock, K.; Veguilla, V.; Lu, X.; Zhong, W.; Butler, E.N.; Sun, H.; Liu, F.; Dong, L.; DeVos, J.R.; Gargiullo, P.M.; et al. Cross-Reactive Antibody Responses to the 2009 Pandemic H1N1 Influenza Virus. N. Engl. J. Med. 2009, 361, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Dilai, M.; Piro, M.; el Harrak, M.; Fougerolle, S.; Dehhaoui, M.; Dikrallah, A.; Legrand, L.; Paillot, R.; Fihri, O.F. Impact of Mixed Equine Influenza Vaccination on Correlate of Protection in Horses. Vaccines 2018, 6, 71. [Google Scholar] [CrossRef] [Green Version]
- Daly, J.M.; Yates, P.J.; Browse, G.; Swann, Z.; Newton, J.R.; Jessett, D.; Davis-Poynter, N.; Mumford, J.A. Comparison of Hamster and Pony Challenge Models for Evaluation of Effect of Antigenic Drift on Cross Protection Afforded by Equine Influenza Vaccines. Equine Vet. J. 2003, 35, 458–462. [Google Scholar] [CrossRef]
- Miller, E.; Hoschler, K.; Hardelid, P.; Stanford, E.; Andrews, N.; Zambon, M. Incidence of 2009 Pandemic Influenza A H1N1 Infection in England: A Cross-Sectional Serological Study. Lancet 2010, 375, 62126–66217. [Google Scholar] [CrossRef]
- Kilbourne, E.D.; Smith, C.; Brett, I.; Pokorny, B.A.; Johansson, B.; Cox, N. The Total Influenza Vaccine Failure of 1947 Revisited: Major Intrasubtypic Antigenic Change Can Explain Failure of Vaccine in a Post-World War II Epidemic. Proc. Natl. Acad. Sci. USA 2002, 99, 10748–10752. [Google Scholar] [CrossRef] [Green Version]
- de Jong, J.C.; Smith, D.J.; Lapedes, A.S.; Donatelli, I.; Campitelli, L.; Barigazzi, G.; van Reeth, K.; Jones, T.C.; Rimmelzwaan, G.F.; Osterhaus, A.D.M.E.; et al. Antigenic and Genetic Evolution of Swine Influenza A (H3N2) Viruses in Europe. J. Virol. 2007, 81, 4315–4322. [Google Scholar] [CrossRef] [Green Version]
- EIDS. Available online: https://equinesurveillance.org/landing/ (accessed on 20 December 2021).
- Hall, W.J.; Douglas, R.G.; Hyde, R.W.; Roth, F.K.; Cross, A.S.; Speers, D.M. Pulmonary Mechanics after Uncomplicated Influenza A Infection. Am. Rev. Resp. Dis. 1976, 113, 141–148. [Google Scholar] [CrossRef]
- Willoughby, R.; Ecker, G.; McKee, S.; Riddolls, L.; Vernaillen, C.; Dubovi, E.; Lein, D.; Mahony, J.B.; Chernesky, M.; Nagy, E. The Effects of Equine Rhinovirus, Influenza Virus and Herpesvirus Infection on Tracheal Clearance Rate in Horses. Can. J. Vet. Res. 1992, 56, 115–121. [Google Scholar]
- Ong, A.K.; Chen, M.I.; Lin, L.; Tan, A.S.; New, N.W.; Barkham, T.; Tay, S.Y.; Leo, Y.S. Improving the Clinical Diagnosis of Influenza—A Comparative Analysis of New Influenza a (H1N1) Cases. PLoS ONE 2009, 4, e8453. [Google Scholar] [CrossRef] [Green Version]
- Kash, J.C.; Taubenberger, J.K. The Role of Viral, Host, and Secondary Bacterial Factors in Influenza Pathogenesis. Am. J. Pathol. 2015, 185I, 1528–1536. [Google Scholar] [CrossRef] [Green Version]
- Gounder, A.P.; Boon, A.C.M. Influenza Pathogenesis: The Effect of Host Factors on Severity of Disease. J. Immunol. 2019, 202, 341–345. [Google Scholar] [CrossRef] [Green Version]
- Wright, P.F.; Thompson, J.; Karzon, D.T. Differing Virulence of H1N1 and H3N2 Influenza Strains. Am. J. Epidemiol. 1980, 112, 814–819. [Google Scholar] [CrossRef]
- Chambers, T.M. A Brief Introduction to Equine Influenza and Equine Influenza Viruses. Methods Mol. Biol. 2020, 2123, 355–360. [Google Scholar] [CrossRef]
- Writing Committee of the WHO Consultation on Clinical Aspects of Pandemic (H1N1) 2009 Influenza*. Clinical Aspects of Pandemic 2009 Influenza A (H1N1) Virus Infection. N. Engl. J. Med. 2010, 362, 1708–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uyeki, T.M. Preventing and Controlling Influenza with Available Interventions. N. Engl. J. Med. 2014, 370, 789–791. [Google Scholar] [CrossRef]
- Paillot, R.; El-Hage, C.M. The Use of a Recombinant Canarypox-Based Equine Influenza Vaccine during the 2007 Australian Outbreak: A Systematic Review and Summary. Pathogens 2016, 5, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putri, W.C.W.S.; Muscatello, D.J.; Stockwell, M.S.; Newall, A.T. Economic Burden of Seasonal Influenza in the United States. Vaccine 2018, 36, 3960–3966. [Google Scholar] [CrossRef] [PubMed]
- De Francisco Shapovalova, N.; Donadel, M.; Jit, M.; Hutubessy, R. A Systematic Review of the Social and Economic Burden of Influenza in Low- and Middle-Income Countries. Vaccine 2015, 33, 6537–6544. [Google Scholar] [CrossRef] [PubMed]
- Punpanich, W.; Chotpitayasunondh, T. A Review on the Clinical Spectrum and Natural History of Human Influenza. Int. J. Infect. Dis. 2012, 16, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Shittu, I.; Meseko, C.A.; Sulaiman, L.P.; Inuwa, B.; Mustapha, M.; Zakariya, P.S.; Muhammad, A.A.; Muhammad, U.; Atuman, Y.J.; Barde, I.J.; et al. Fatal Multiple Outbreaks of Equine Influenza H3N8 in Nigeria, 2019: The First Introduction of Florida Clade 1 to West Africa. Vet. Microbiol. 2020, 248, 108820. [Google Scholar] [CrossRef]
- Gilkerson, J.R. Equine Influenza in Australia: A Clinical Overview. Aust. Vet. J. 2011, 89, 11–13. [Google Scholar] [CrossRef]
- Peek, S.F.; Landolt, G.; Karasin, A.I.; Slack, J.A.; Steinberg, H.; Semrad, S.D.; Olsen, C.W. Acute Respiratory Distress Syndrome and Fatal Interstitial Pneumonia Associated with Equine Influenza in a Neonatal Foal. J. Vet. Intern. Med. 2004, 18, 132–134. [Google Scholar] [CrossRef]
- Alexanders, D.J.; Brown, I.H. Recent Zoonoses Caused by Influenza a Viruses. OIE Rev. Sci. Tech. 2000, 12, 197–225. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention Disease Burden of Flu. Available online: https://www.cdc.gov/flu/about/burden/index.html (accessed on 8 December 2021).
- Stöhr, K. Influenza--WHO Cares. Lancet Infect. Dis. 2002, 2, 517. [Google Scholar] [CrossRef]
- The Signature Features of Influenza Pandemics—Implications for Policy. N. Engl. J. Med. 2012, 366, 2595–2958. [CrossRef]
- Kourtis, A.P.; Read, J.S.; Jamieson, D.J. Pregnancy and Infection. N. Engl. J. Med. 2014, 370, 2211–2218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgon, O.W.; Bramley, A.; Fowlkes, A.; Freedman, D.S.; Taylor, T.H.; Gargiullo, P.; Belay, B.; Jain, S.; Cox, C.; Kamimoto, L.; et al. Morbid Obesity as a Risk Factor for Hospitalization and Death Due to 2009 Pandemic Influenza A(H1N1) Disease. PLoS ONE 2010, 5, e9694. [Google Scholar] [CrossRef]
- Everitt, A.R.; Clare, S.; Pertel, T.; John, S.P.; Wash, R.S.; Smith, S.E.; Chin, C.R.; Feeley, E.M.; Sims, J.S.; Adams, D.J.; et al. IFITM3 Restricts the Morbidity and Mortality Associated with Influenza. Nature 2012, 484, 519–523. [Google Scholar] [CrossRef] [Green Version]
- Thiemann, A.K. Respiratory Disease in the Donkey. Equine Vet. Ed. 2012, 24, 469–478. [Google Scholar] [CrossRef]
- Yang, H.; Xiao, Y.; Meng, F.; Sun, F.; Chen, M.; Cheng, Z.; Chen, Y.; Liu, S.; Chen, H. Emergence of H3N8 equine influenza virus in donkeys in China in 2017. Vet. Microbiol. 2018, 214, 1–6. [Google Scholar] [CrossRef]
- Muranaka, M.; Yamanaka, T.; Katayama, Y.; Niwa, H.; Oku, K.; Matsumura, T.; Oyamada, T. Time-Related Pathological Changes in Horses Experimentally Inoculated with Equine Influenza A Virus. J. Equine Sci. 2012, 23, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Begg, A.P.; Reece, R.L.; Hum, S.; Townsend, W.; Gordon, A.; Carrick, J. Pathological Changes in Horses Dying with Equine Influenza in Australia, 2007. Aust. Vet. J. 2011, 89, 19–22. [Google Scholar] [CrossRef]
- Van der Sluijs, K.F.; van der Poll, T.; Lutter, R.; Juffermans, N.P.; Schultz, M.J. Bench-to-Bedside Review: Bacterial Pneumonia with Influenza—Pathogenesis and Clinical Implications. Crit. Care 2010, 14, 219. [Google Scholar] [CrossRef] [Green Version]
- Patterson-Kane, J.C.; Carrick, J.B.; Axon, J.E.; Wilkie, I.; Begg, A.P. The Pathology of Bronchointerstitial Pneumonia in Young Foals Associated with the First Outbreak of Equine Influenza in Australia. Equine Vet. J. 2008, 40, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Kalil, A.C.; Thomas, P.G. Influenza Virus-Related Critical Illness: Pathophysiology and Epidemiology. Crit. Care 2019, 23, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Short, K.R.; Kroeze, E.J.B.V.; Fouchier, R.A.M.; Kuiken, T. Pathogenesis of Influenza-Induced Acute Respiratory Distress Syndrome. Lancet Infect. Dis. 2014, 14, 57–69. [Google Scholar] [CrossRef]
- Denholm, J.T.; Gordon, C.L.; Johnson, P.D.; Hewagama, S.S.; Stuart, R.L.; Aboltins, C.; Jeremiah, C.; Knox, J.; Lane, G.P.; Tramontana, A.R.; et al. Hospitalised Adult Patients with Pandemic (H1N1) 2009 Influenza in Melbourne, Australia. Med. J. Aust. 2010, 192, 84–86. [Google Scholar] [CrossRef] [PubMed]
- Waddell, G.H.; Teigland, M.B.; Sigel, M.M. A New Influenza Virus Associated with Equine Respiratory Disease. J. Am. Vet. Med. Assoc. 1963, 143, 587–590. [Google Scholar]
- Wada, T.; Morishima, T.; Okumura, A.; Tashiro, M.; Hosoya, M.; Shiomi, M.; Okuno, Y. Differences in Clinical Manifestations of Influenza-Associated Encephalopathy by Age. Microbiol. Immunol. 2009, 53, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Sovinova, O.; Tumova, B.; Pouska, F.; Nemec, J. Isolation of a virus causing respiratory disease in horses. Acta Virol. 1958, 2, 52–61. [Google Scholar]
- Scholtens, R.G.; Steele, J.H.; Dowdle, W.R.; Yarbrough, W.B.; Robinson, R.Q. U.S. Epizootic of Equine Influenza. Public Health Rep. 1964, 79, 393–402. [Google Scholar] [CrossRef]
- Virmani, N.; Singh, B.K.; Gulati, B.R.; Kumar, S. Equine Influenza Outbreak in India. Vet. Rec. 2008, 163, 607–608. [Google Scholar] [CrossRef]
- Legrand, L.J.; Pitel, P.H.Y.; Cullinane, A.A.; Fortier, G.D.; Pronost, S.L. Genetic Evolution of Equine Influenza Strains Isolated in France from 2005 to 2010. Equine Vet. J. 2015, 47, 207–211. [Google Scholar] [CrossRef]
- Bryant, N.A.; Rash, A.S.; Russell, C.A.; Ross, J.; Cooke, A.; Bowman, S.; MacRae, S.; Lewis, N.S.; Paillot, R.; Zanoni, R.; et al. Antigenic and Genetic Variations in European and North American Equine Influenza Virus Strains (H3N8) Isolated from 2006 to 2007. Vet. Microbiol. 2009, 138, 41–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whitlock, F.; Newton, J.R.; Grewar, J. Descriptive Epidemiology of the 2019 Equine Influenza Epidemic in Great Britain. In Proceedings of the 11th International Equine Infectious Diseases Conference, Virtual, 27 September–1 October 2021. [Google Scholar]
- OIE Expert Surveillance Panel on Equine Influenza Vaccine Composition—Videoconference, 16 April 2020. Available online: https://oiebulletin.fr/?officiel=08-4-2-2020-1-panel&edition=12827&pdf=officiel&article=15169 (accessed on 10 December 2021).
- Paillot, R.; Pitel, P.H.; Pronost, S.; Legrand, L.; Fougerolle, S.; Jourdan, M.; Marcillaud-Pitel, C. Florida Clade 1 Equine Influenza Virus in France. Vet. Rec. 2019, 184, 101. [Google Scholar] [CrossRef] [PubMed]
- Koelle, K.; Khatri, P.; Kamradt, M.; Kepler, T.B. A Two-Tiered Model for Simulating the Ecological and Evolutionary Dynamics of Rapidly Evolving Viruses, with an Application to Influenza. J. R. Soc. Interface 2010, 7, 1257. [Google Scholar] [CrossRef] [Green Version]
- Influenza A (H1N1) Outbreak. Available online: https://www.who.int/emergencies/situations/influenza-a-(h1n1)-outbreak (accessed on 21 December 2021).
- Yang, H.; Carney, P.J.; Chang, J.C.; Villanueva, J.M.; Stevens, J. Structure and Receptor Binding Preferences of Recombinant Hemagglutinins from Avian and Human H6 and H10 Influenza A Virus Subtypes. J. Virol. 2015, 89, 4612–4623. [Google Scholar] [CrossRef] [Green Version]
- Jester, B.J.; Uyeki, T.M.; Jernigan, D.B. Fifty Years of Influenza A(H3N2) Following the Pandemic of 1968. Am. J. Public Health 2020, 110, 669–676. [Google Scholar] [CrossRef] [PubMed]
- Harrington, W.N.; Kackos, C.M.; Webby, R.J. The Evolution and Future of Influenza Pandemic Preparedness. Exp. Mol. Med. 2021, 53, 737–749. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.C.; Baranovich, T.; Marathe, B.M.; Danner, A.F.; Seiler, J.P.; Franks, J.; Govorkova, E.A.; Krauss, S.; Webster, R.G. Risk Assessment of H2N2 Influenza Viruses from the Avian Reservoir. J. Virol. 2014, 88, 1175–1188. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Wang, M.; Kawaoka, Y.; Gorman, O.; Ito, T.; Saito, T.; Webster, R.G. Characterization of a New Avian-like Influenza A Virus from Horses in China. Virology 1992, 188, 245–255. [Google Scholar] [CrossRef]
- Zhu, H.; Damdinjav, B.; Gonzalez, G.; Patrono, L.V.; Ramirez-Mendoza, H.; Amat, J.A.R.; Crispell, J.; Parr, Y.A.; Hammond, T.A.; Shiilegdamba, E.; et al. Absence of Adaptive Evolution Is the Main Barrier against Influenza Emergence in Horses in Asia despite Frequent Virus Interspecies Transmission from Wild Birds. PLoS Pathog. 2019, 15, e1007531. [Google Scholar] [CrossRef]
- Abdel-Moneim, A.S.; Abdel-Ghany, A.E.; Shany, S.A.S. Isolation and Characterization of Highly Pathogenic Avian Influenza Virus Subtype H5N1 from Donkeys. J. Biomed. Sci. 2010, 17, 25. [Google Scholar] [CrossRef] [Green Version]
- Zhou, P.; Luo, A.; Xiao, X.; Hu, X.; Shen, D.; Li, J.; Wu, X.; Xian, X.; Wei, C.; Fu, C.; et al. Serological Evidence of H3N2 Canine Influenza Virus Infection among Horses with Dog Exposure. Transbound. Emerg. Dis. 2019, 66, 915–920. [Google Scholar] [CrossRef] [PubMed]
- Lewis, N.S.; Daly, J.M.; Russell, C.A.; Horton, D.L.; Skepner, E.; Bryant, N.A.; Burke, D.F.; Rash, A.S.; Wood, J.L.N.; Chambers, T.M.; et al. Antigenic and Genetic Evolution of Equine Influenza A (H3N8) Virus from 1968 to 2007. J. Virol. 2011, 85, 12742–12749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, W.D. Equine Influenza. Vet. Clin. N. Am.-Equine 1993, 9, 257–282. [Google Scholar] [CrossRef]
- Smith, D.J.; Lapedes, A.S.; de Jong, J.C.; Bestebroer, T.M.; Rimmelzwaan, G.F.; Osterhaus, A.D.M.E.; Fouchier, R.A.M. Mapping the Antigenic and Genetic Evolution of Influenza Virus. Science 2004, 305, 371–376. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.H. Complete Genome Sequencing of Influenza A Viruses Using Next-Generation Sequencing. Methods Mol. Biol. 2020, 2123, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Killingley, B.; Nguyen-Van-Tam, J. Routes of Influenza Transmission. Influenza Other Resp. 2013, 7, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Cowled, B.; Ward, M.P.; Hamilton, S.; Garner, G. The Equine Influenza Epidemic in Australia: Spatial and Temporal Descriptive Analyses of a Large Propagating Epidemic. Prev. Vet. Med. 2009, 92, 60–70. [Google Scholar] [CrossRef]
- Dominguez, M.; Münstermann, S.; de Guindos, I.; Timoney, P. Equine Disease Events Resulting from International Horse Movements: Systematic Review and Lessons Learned. Equine Vet. J. 2016, 48, 641–653. [Google Scholar] [CrossRef] [Green Version]
- Gildea, S.; Arkins, S.; Cullinane, A. Management and Environmental Factors Involved in Equine Influenza Outbreaks in Ireland 2007–2010. Equine Vet. J. 2011, 43, 608–617. [Google Scholar] [CrossRef] [Green Version]
- Schemann, K.; Taylor, M.R.; Toribio, J.A.L.M.L.; Dhand, N.K. Horse Owners’ Biosecurity Practices Following the First Equine Influenza Outbreak in Australia. Prev. Vet. Med. 2011, 102, 304–314. [Google Scholar] [CrossRef] [Green Version]
- Hodgkinson, C.R.; Slater, J.; Brennan, M.L.; Robin, C.A.; Dyson, S.; Ireland, J.L. Implementation of Biosecurity on Equestrian Premises in Great Britain. Equine Vet. J. 2018, 50, 8. [Google Scholar] [CrossRef] [Green Version]
- The Hon. Ian Callinan AC The August 2007 Outbreak in Australia. Report of the Equine Influenza Inquiry. Available online: https://nla.gov.au/nla.obj-961843962/view?partId=nla.obj-962287573#page/n15/mode/1up (accessed on 24 January 2022).
- Travelers’ Health. Chapter 4—Travel-Related Infectious Diseases. Available online: https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/influenza (accessed on 10 May 2022).
- Lessler, J.; Reich, N.G.; Brookmeyer, R.; Perl, T.M.; Nelson, K.E.; Cummings, D.A. Incubation Periods of Acute Respiratory Viral Infections: A Systematic Review. Lancet Infect. Dis. 2009, 9, 291–300. [Google Scholar] [CrossRef]
- Singh, R.K.; Dhama, K.; Karthik, K.; Khandia, R.; Munjal, A.; Khurana, S.K.; Chakraborty, S.; Malik, Y.S.; Virmani, N.; Singh, R.; et al. A Comprehensive Review on Equine Influenza Virus: Etiology, Epidemiology, Pathobiology, Advances in Developing Diagnostics, Vaccines, and Control Strategies. Front. Microbiol. 2018, 9, 1941. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Daleno, C.; Baldanti, F.; Scala, A.; Campanini, G.; Taroni, F.; Fossali, E.; Pelucchi, C.; Principi, N. Viral Shedding in Children Infected by Pandemic A/H1N1/2009 Influenza Virus. Virol. J. 2011, 8, 349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brankston, G.; Gitterman, L.; Hirji, Z.; Lemieux, C.; Gardam, M. Transmission of Influenza A in Human Beings. Lancet. Infect. Dis. 2007, 7, 257–265. [Google Scholar] [CrossRef]
- Bennett, J.E.; Dolin, R.; Blaser, M.J. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 8th ed.; Saunders: Philadelphia, PA, USA, 2015; Volume 1–2. [Google Scholar]
- Daly, J.M.; MacRae, S.; Newton, J.R.; Wattrang, E.; Elton, D.M. Equine Influenza: A Review of an Unpredictable Virus. Vet. J. 2011, 189, 7–14. [Google Scholar] [CrossRef]
- Yassi, A.; Bryce, E.; Moore, D.; Copes, J.R.; Bartlett, K.; Fitzgerald, M.; Gilbert, M.; Hon, C.; Perry, T.; Saunders, S.; et al. Protecting the Faces of Health Care Workers: Knowledge Gaps and Research Priorities for Effective Protection Against Occupationally-Acquired Respiratory Infectious Diseases. Available online: https://www.paho.org/hq/dmdocuments/2009/Protecting%20the%20faces%20of%20health%20care%20workers.pdf (accessed on 15 December 2021).
- Mitchell, C.A.; Guerin, L.F. Influenza A of Human, Swine, Equine and Avian Origin: Comparison of Survival in Aerosol Form. Can. J. Comp. Med. 1972, 36, 9–11. [Google Scholar]
- Librado, P.; Khan, N.; Fages, A.; Kusliy, M.A.; Suchan, T.; Tonasso-Calvière, L.; Schiavinato, S.; Alioglu, D.; Fromentier, A.; Perdereau, A.; et al. The Origins and Spread of Domestic Horses from the Western Eurasian Steppes. Nature 2021, 598, 634–640. [Google Scholar] [CrossRef]
- Busby, D.; Rutland, C. The Horse: A Natural History; Ivy Press: Brighton, UK, 2019; pp. 1–224. [Google Scholar]
- Jones, K.E.; Patel, N.G.; Levy, M.A.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global Trends in Emerging Infectious Diseases. Nature 2008, 451, 990–993. [Google Scholar] [CrossRef]
- Larson, K.R.L.; Heil, G.L.; Chambers, T.M.; Capuano, A.; White, S.K.; Gray, G.C. Serological Evidence of Equine Influenza Infections among Persons with Horse Exposure, Iowa. J. Clin. Virol. 2015, 67, 78–83. [Google Scholar] [CrossRef]
- Burnell, F.J.; Holmes, M.A.; Roiko, A.H.; Lowe, J.B.; Heil, G.L.; White, S.K.; Gray, G.C. Little Evidence of Human Infection with Equine Influenza during the 2007 Epizootic, Queensland, Australia. J. Clin. Virol. 2014, 59, 100–103. [Google Scholar] [CrossRef]
- Masurel, N.; Mulder, J. Studies on the Content of Antibodies for Equine Influenza Viruses in Human Sera. Bull. World Health Organ. 1966, 34, 885–893. [Google Scholar]
- Kasel, J.A.; Couch, R.B. Experimental Infection in Man and Horses with Influenza A Viruses. Bull. World Health Organ. 1969, 41, 447–452. [Google Scholar]
- Kuchipudi, S.V.; Nelli, R.K.; Gontu, A.; Satyakumar, R.; Nair, M.S.; Subbiah, M. Sialic Acid Receptors: The Key to Solving the Enigma of Zoonotic Virus Spillover. Viruses 2021, 13, 262. [Google Scholar] [CrossRef] [PubMed]
- Cauldwell, A.V.; Long, J.S.; Moncorgé, O.; Barclay, W.S. Viral Determinants of Influenza A Virus Host Range. J. Gen. Virol. 2014, 95, 1193–1210. [Google Scholar] [CrossRef] [Green Version]
- Gibbs, E.P.J.; Anderson, T.C. Equine and Canine Influenza: A Review of Current Events. Animal Health Res. Rev. 2010, 11, 43–51. [Google Scholar] [CrossRef]
- Crawford, P.C.; Dubovi, E.J.; Castleman, W.L.; Stephenson, I.; Gibbs, E.P.J.; Chen, L.; Smith, C.; Hill, R.C.; Ferro, P.; Pompey, J.; et al. Transmission of Equine Influenza Virus to Dogs. Science 2005, 310, 482–485. [Google Scholar] [CrossRef] [Green Version]
- Daly, J.M.; Blunden, A.S.; MacRae, S.; Miller, J.; Bowman, S.J.; Kolodziejek, J.; Nowotny, N.; Smith, K.C. Transmission of Equine Influenza Virus to English Foxhounds. Emerg. Infect. Dis. 2008, 14, 461–464. [Google Scholar] [CrossRef]
- Crispe, E.; Finlaison, D.S.; Hurt, A.C.; Kirkland, P.D. Infection of Dogs with Equine Influenza Virus: Evidence for Transmission from Horses during the Australian Outbreak. Aust. Vet. J. 2011, 89, 27–28. [Google Scholar] [CrossRef]
- Newton, R.; Cooke, A.; Elton, D.; Bryant, N.; Rash, A.; Bowman, S.; Blunden, T.; Miller, J.; Hammond, T.A.; Camm, I.; et al. Canine Influenza Virus: Cross-Species Transmission from Horses. Vet. Rec. 2007, 161, 142–143. [Google Scholar] [CrossRef]
- Yondon, M.; Zayat, B.; Nelson, M.I.; Heil, G.L.; Anderson, B.D.; Lin, X.; Halpin, R.A.; McKenzie, P.P.; White, S.K.; Wentworth, D.E.; et al. Equine Influenza A(H3N8) Virus Isolated from Bactrian Camel, Mongolia. Emerg. Infect. Dis. 2014, 20, 2144–2147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, S.; Wang, L.; Fu, X.; He, S.; Hong, M.; Zhou, P.; Lai, A.; Gray, G.; Li, S. Equine Influenza A(H3N8) Virus Infection in Cats. Emerg. Infect. Dis. 2014, 20, 2096–2099. [Google Scholar] [CrossRef]
- Tu, J.; Zhou, H.; Jiang, T.; Li, C.; Zhang, A.; Guo, X.; Zou, W.; Chen, H.; Jin, M. Isolation and Molecular Characterization of Equine H3N8 Influenza Viruses from Pigs in China. Arch. Virol. 2009, 154, 887–890. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, T.; Mamahit, A.; Cox, N.J. 65 Years of Influenza Surveillance by a World Health Organization-coordinated Global Network. Other Respir. Viruses 2018, 12, 558–565. [Google Scholar] [CrossRef]
- Sources of UK Flu Data: Influenza Surveillance in the UK. Available online: https://www.gov.uk/guidance/sources-of-uk-flu-data-influenza-surveillance-in-the-uk (accessed on 5 January 2022).
- Daly, J.M.; Lai, A.C.K.; Binns, M.M.; Chambers, T.M.; Barrandeguy, M.; Mumford, J.A. Antigenic and Genetic Evolution of Equine H3N8 Influenza A Viruses. J. Gen. Virol. 1996, 77, 661–671. [Google Scholar] [CrossRef]
- Sack, A.; Cullinane, A.; Daramragchaa, U.; Chuluunbaatar, M.; Gonchigoo, B.; Gray, G.C. Equine Influenza Virus—A Neglected, Reemergent Disease Threat. Emerg. Infect. Dis. 2019, 25, 1185–1191. [Google Scholar] [CrossRef] [Green Version]
- Whitlock, F. Equine Infectious Disease Surveillance Initiatives in the UK. Vet. Rec. 2020, 186, 241–243. [Google Scholar] [CrossRef]
- Woodward, A.L.; Rash, A.S.; Blinman, D.; Bowman, S.; Chambers, T.M.; Daly, J.M.; Damiani, A.; Joseph, S.; Lewis, N.; McCauley, J.W.; et al. Development of a Surveillance Scheme for Equine Influenza in the UK and Characterisation of Viruses Isolated in Europe, Dubai and the USA from 2010–2012. Vet. Microbiol. 2014, 169, 113–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Equiflunet Viewer. Available online: https://equinesurveillance.org/equiflunet/ (accessed on 20 December 2021).
- Tell-Tail Disease Outbreak Alerts. Available online: www.telltail.co.uk (accessed on 20 December 2021).
- OIE-WAHIS. Available online: https://wahis.oie.int/#/home (accessed on 26 January 2022).
- Dugas, A.F.; Valsamakis, A.; Atreya, M.R.; Thind, K.; Alarcon Manchego, P.; Faisal, A.; Gaydos, C.A.; Rothman, R.E. Clinical Diagnosis of Influenza in the ED. Am. J. Emerg. Med. 2015, 33, 770–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santillana, M.; Nguyen, A.T.; Dredze, M.; Paul, M.J.; Nsoesie, E.O.; Brownstein, J.S. Combining Search, Social Media, and Traditional Data Sources to Improve Influenza Surveillance. PLoS Comput. Biol. 2015, 11, e1004513. [Google Scholar] [CrossRef] [Green Version]
- Polansky, L.S.; Outin-Blenman, S.; Moen, A.C. Improved Global Capacity for Influenza Surveillance. Emerg. Infect. Dis. 2016, 22, 993–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steffen, C.; Debellut, F.; Gessner, B.D.; Kasolo, F.C.; Yahaya, A.A.; Ayebazibwe, N.; Bassong, O.; Cardoso, Y.; Kebede, S.; Manoncourt, S.; et al. Improving Influenza Surveillance in Sub-Saharan Africa. Bull. World Health Organ. 2012, 90, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Boni, M.F. Vaccination and Antigenic Drift in Influenza. Vaccine 2008, 26, C8–C14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, B.D.; Ma, M.; Xia, Y.; Wang, T.; Shu, B.; Lednicky, J.A.; Ma, M.J.; Lu, J.; Gray, G.C. Bioaerosol Sampling in Modern Agriculture: A Novel Approach for Emerging Pathogen Surveillance? J. Infect. Dis. 2016, 214, 537–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.T.; Poh, M.K.; Low, J.; Kalimuddin, S.; Thoon, K.C.; Ng, W.C.; Anderson, B.D.; Gray, G.C. Bioaerosol Sampling in Clinical Settings: A Promising, Noninvasive Approach for Detecting Respiratory Viruses. Open Forum Infect. Dis. 2016, 4, ofw259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, B.; Crosby, A.W. Epidemic and Peace 1918. Popul. Stud. 1978, 32, 199. [Google Scholar] [CrossRef]
- Fukumi, H. Summary Report on the Asian Influenza Epidemic in Japan, 1957. Bull. World Health Organ. 1959, 20, 187–198. [Google Scholar]
- McClure, R.; Smith, A. Diseases of the Horse, and Cattle and Sheep: Their Treatment with a List and Full Description of the Medicines Employed. With Treatment of the Late Epizootic Influenza or “Canadian Horse Distemper”; A. H. Hovey and Co.: Toronto, ON, Canada, 1873. [Google Scholar]
- Powell, D.G.; Watkins, K.L.; Li, P.H.; Shortridge, K.F. Outbreak of Equine Influenza among Horses in Hong Kong during 1992. Vet. Rec. 1995, 136, 531–536. [Google Scholar] [CrossRef]
- Doherty, P.C.; Turner, S.J.; Webby, R.G.; Thomas, P.G. Influenza and the Challenge for Immunology. Nat. Immunol. 2006, 7, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Paillot, R. A Systematic Review of Recent Advances in Equine Influenza Vaccination. Vaccines 2014, 2, 797–831. [Google Scholar] [CrossRef] [Green Version]
- Barberis, I.; Myles, P.; Ault, S.K.; Bragazzi, N.L.; Martini, M. History and Evolution of Influenza control through Vaccination: From the First Monovalent vaccine to Universal Vaccines. J. Prev. Med. Hyg. 2016, 57, E115–E120. [Google Scholar] [PubMed]
- Grohskopf, L.A.; Alyanak, E.; Ferdinands, J.M.; Broder, K.R.; Blanton, L.H.; Talbot, H.K.; Fry, A.M. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices, United States, 2021–2022 Influenza Season. MMWR Recomm. Rep. 2021, 70, 1–32. [Google Scholar] [CrossRef]
- Chambers, T.M.; Holland, R.E.; Tudor, L.R.; Townsend, H.G.G.; Cook, A.; Bogdan, J.; Lunn, D.P.; Hussey, S.; Whitaker-Dowling, P.; Youngner, J.S.; et al. A New Modified Live Equine Influenza Virus Vaccine: Phenotypic Stability, Restricted Spread and Efficacy against Heterologous Virus Challenge. Equine Vet. J. 2001, 33, 630–636. [Google Scholar] [CrossRef]
- Ault, A.; Zajac, A.M.; Kong, W.P.; Gorres, J.P.; Royals, M.; Wei, C.J.; Bao, S.; Yang, Z.-y.; Reedy, S.E.; Sturgill, T.L.; et al. Immunogenicity and Clinical Protection against Equine Influenza by DNA Vaccination of Ponies. Vaccine 2012, 30, 3965–3974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.R.; Liu, Y.M.; Tseng, Y.C.; Ma, C. Better Influenza Vaccines: An Industry Perspective. J. Biomed. Sci. 2020, 27, 33. [Google Scholar] [CrossRef] [PubMed]
- Rudenko, L.G.; Arden, N.H.; Grigorieva, E.; Naychin, A.; Rekstin, A.; Klimov, A.I.; Donina, S.; Desheva, J.; Holman, R.C.; Deguzman, A.; et al. Immunogenicity and Efficacy of Russian Live Attenuated and US Inactivated Influenza Vaccines Used Alone and in Combination in Nursing Home Residents. Vaccine 2000, 19, 308–318. [Google Scholar] [CrossRef]
- Oladunni, F.S.; Oseni, S.O.; Martinez-Sobrido, L.; Chambers, T.M. Equine Influenza Virus and Vaccines. Viruses 2021, 13, 1657. [Google Scholar] [CrossRef]
- Paillot, R.; Prowse, L.; Montesso, F.; Huang, C.M.; Barnes, H.; Escala, J. Whole Inactivated Equine Influenza Vaccine: Efficacy against a Representative Clade 2 Equine Influenza Virus, IFNgamma Synthesis and Duration of Humoral Immunity. Vet. Microbiol. 2013, 162, 396–407. [Google Scholar] [CrossRef]
- Treanor, J.J.; Campbell, J.D.; Zangwill, K.M.; Rowe, T.; Wolff, M. Safety and Immunogenicity of an Inactivated Subvirion Influenza A (H5N1) Vaccine. N. Engl. J. Med. 2006, 354, 1343–1351. [Google Scholar] [CrossRef]
- Paillot, R.; Prowse, L. ISCOM-Matrix-Based Equine Influenza (EIV) Vaccine Stimulates Cell-Mediated Immunity in the Horse. Vet. Immunol. Immunopathol. 2012, 145, 516–521. [Google Scholar] [CrossRef]
- Treanor, J.J.; Schiff, G.M.; Couch, R.B.; Cate, T.R.; Brady, R.C.; Hay, C.M.; Wolff, M.; She, D.; Cox, M.M.J. Dose-Related Safety and Immunogenicity of a Trivalent Baculovirus-Expressed Influenza-Virus Hemagglutinin Vaccine in Elderly Adults. J. Infect. Dis. 2006, 193, 1223–1228. [Google Scholar] [CrossRef]
- Ellebedy, A.H.; Webby, R.J. Influenza Vaccines. Vaccine 2009, 27, D65–D68. [Google Scholar] [CrossRef] [PubMed]
- Trombetta, C.M.; Gianchecchi, E.; Montomoli, E. Influenza Vaccines: Evaluation of the Safety Profile. Hum. Vaccin. Immunother. 2018, 14, 657–670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Wang, J.; Zhang, J.; Ly, H. Advances in Development and Application of Influenza Vaccines. Front. Immunol. 2021, 12, 711997. [Google Scholar] [CrossRef] [PubMed]
- Types of Seasonal Influenza Vaccine. Available online: https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/vaccination/types-of-seasonal-influenza-vaccine#:~:text=Two%20types%20of%20influenza%20vaccine (accessed on 10 December 2021).
- Recommended Composition of Influenza Virus Vaccines for Use in the 2021–2022 Northern Hemisphere Influenza Season. Available online: https://www.who.int/publications/m/item/recommended-composition-of-influenza-virus-vaccines-for-use-in-the-2021-2022-northern-hemisphere-influenza-season (accessed on 7 December 2021).
- Selecting Viruses for the Seasonal Influenza Vaccine. CDC. Available online: https://www.cdc.gov/flu/prevent/vaccine-selection.htm (accessed on 21 December 2021).
- Bambery, B.; Douglas, T.; Selgelid, M.J.; Maslen, H.; Giubilini, A.; Pollard, A.J.; Savulescu, J. Influenza Vaccination Strategies Should Target Children. Public Health Ethics 2018, 11, 221–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- BHA Confirms Changes to the Rules of Racing—The British Horseracing Authority. Available online: https://www.britishhorseracing.com/press_releases/bha-confirms-changes-to-the-rules-of-racing/ (accessed on 21 December 2021).
- Wilson, W.D. Vaccination Programs for Foals and Weanlings. In Proceedings of the Presented at 45th Annual Convention of the American Association of Equine Practitioners, Albuquerque, NM, USA, 8 December 1999. [Google Scholar]
- Daly, J.M.; Newton, J.R.; Wood, J.L.N.; Park, A.W. What Can Mathematical Models Bring to the Control of Equine Influenza? Equine Vet. J. 2013, 45, 784–788. [Google Scholar] [CrossRef] [Green Version]
- Gildea, S.; Quinlivan, M.; Murphy, B.A.; Cullinane, A. Humoral Response and Antiviral Cytokine Expression Following Vaccination of Thoroughbred Weanlings-A Blinded Comparison of Commercially Available Vaccines. Vaccine 2013, 31, 5216–5222. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.M.; Yates, P.J.; Newton, J.R.; Park, A.; Henley, W.; Wood, J.L.N.; Davis-Poynter, N.; Mumford, J.A. Evidence Supporting the Inclusion of Strains from Each of the Two Co-Circulating Lineages of H3N8 Equine Influenza Virus in Vaccines. Vaccine 2004, 22, 4101–4109. [Google Scholar] [CrossRef] [PubMed]
- Ryan, M.; Gildea, S.; Walsh, C.; Cullinane, A. The Impact of Different Equine Influenza Vaccine Products and Other Factors on Equine Influenza Antibody Levels in Thoroughbred Racehorses. Equine Vet. J. 2015, 47, 662–666. [Google Scholar] [CrossRef] [PubMed]
- Baker, D.J. Rationale for the Use of Influenza Vaccines in Horses and the Importance of Antigenic Drift. Equine Vet. J. 1986, 18, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Park, A.W.; Daly, J.M.; Lewis, N.S.; Smith, D.J.; Wood, J.L.N.; Grenfell, B.T. Quantifying the Impact of Immune Escape on Transmission Dynamics of Influenza. Science 2009, 326, 726–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reber, A.; Katz, J. Immunological Assessment of Influenza Vaccines and Immune Correlates of Protection. Expert Rev. Vaccines 2013, 12, 519. [Google Scholar] [CrossRef] [PubMed]
- Newton, J.R.; Lakhani, K.H.; Wood, J.L.N.; Baker, D.J. Risk Factors for Equine Influenza Serum Antibody Titres in Young Thoroughbred Racehorses given an Inactivated Vaccine. Prev. Vet. Med. 2000, 46, 129–141. [Google Scholar] [CrossRef]
- Rouse, B.T.; Ditchfield, W.J.B. The Response of Ponies to Myxovirus Influenzae A-Equi 2 1. Serum and Nasal Antibody Titres Following Exposure. Can. J. Comp. Med. 1970, 34, 1–5. [Google Scholar]
- Delem, A.; Jovanovic, D. Correlation between Rate of Infection and Preexisting Titer of Serum Antibody as Determined by Single Radial Hemolysis during and Epidemic of Influenza A/Victoria/3/75. J. Infect. Dis 1978, 137, 194–196. [Google Scholar] [CrossRef]
- Cox, R.J. Correlates of Protection to Influenza Virus, Where Do We Go from Here? Hum. Vaccin. Immunother. 2013, 9, 405. [Google Scholar] [CrossRef] [Green Version]
- Flannery, B.; Chung, J.R.; Belongia, E.A.; McLean, H.Q.; Gaglani, M.; Murthy, K.; Zimmerman, R.K.; Nowalk, M.P.; Jackson, M.L.; Jackson, L.A.; et al. Interim Estimates of 2017-18 Seasonal Influenza Vaccine Effectiveness—United States, February 2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Gildea, S.; Garvey, M.; Lyons, P.; Lyons, R.; Gahan, J.; Walsh, C.; Cullinane, A. Multifocal Equine Influenza Outbreak with Vaccination Breakdown in Thoroughbred Racehorses. Pathogens 2018, 7, 43. [Google Scholar] [CrossRef] [Green Version]
- Barquero, N.; Daly, J.M.; Newton, J.R. Risk Factors for Influenza Infection in Vaccinated Racehorses: Lessons from an Outbreak in Newmarket, UK in 2003. Vaccine 2007, 25, 7520–7529. [Google Scholar] [CrossRef]
- Binns, M.M.; Daly, J.M.; Chirnside, E.D.; Mumford, J.A.; Wood, J.M.; Richards, C.M.; Daniels, R.S. Genetic and Antigenic Analysis of an Equine Influenza H 3 Isolate from the 1989 Epidemic. Arch. Virol. 1993, 130, 33–43. [Google Scholar] [CrossRef]
- Wong, S.S.; Webby, R.J. Traditional and New Influenza Vaccines. Clin. Microbiol. Rev. 2013, 26, 476–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tregoning, J.S.; Russell, R.F.; Kinnear, E. Adjuvanted Influenza Vaccines. Hum. Vaccines Immunother. 2018, 14, 550–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hussain, A.; Ali, S.; Ahmed, M.; Hussain, S. The Anti-Vaccination Movement: A Regression in Modern Medicine. Cureus 2018, 10, e2919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, I.A.; Cox, N.J. Structural Basis of Immune Recognition of Influenza Virus Hemagglutinin. Annu. Rev. Immunol. 1990, 8, 737–771. [Google Scholar] [CrossRef] [PubMed]
- Nachbagauer, R.; Feser, J.; Naficy, A.; Bernstein, D.I.; Guptill, J.; Walter, E.B.; Berlanda-Scorza, F.; Stadlbauer, D.; Wilson, P.C.; Aydillo, T.; et al. A Chimeric Hemagglutinin-Based Universal Influenza Virus Vaccine Approach Induces Broad and Long-Lasting Immunity in a Randomized, Placebo-Controlled Phase I Trial. Nat. Med. 2020, 27, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Burgess, B.A.; Traub-Dargatz, J.L. Chapter 62—Biosecurity and Control of Infectious Disease Outbreaks. In Equine Infectious Diseases, 2nd ed.; Sellon, D.C., Long, M.T., Eds.; Saunders: Philadelphia, PA, USA, 2013; pp. 530–543. [Google Scholar]
- OIE—World Organisation for Animal Health. Terrestrial Animal Health Code. Available online: https://www.oie.int/en/what-we-do/standards/codes-and-manuals/terrestrial-code-online-access/ (accessed on 8 December 2021).
- Department of Communicable Disease Surveillance and Response Global Influenza Programme WHO Checklist for Influenza Pandemic Preparedness Planning. Available online: https://www.who.int/influenza/resources/documents/FluCheck6web.pdf (accessed on 15 January 2022).
- Dutta, A.; The World Bank. The Effectiveness of Policies to Control a Human Influenza Pandemic: A Literature Review. Available online: https://openknowledge.worldbank.org/handle/10986/6397 (accessed on 16 January 2022).
- Fricke, L.M.; Glöckner, S.; Dreier, M.; Lange, B. Impact of Non-Pharmaceutical Interventions Targeted at COVID-19 Pandemic on Influenza Burden—A Systematic Review. J. Infect. 2021, 82, 1–35. [Google Scholar] [CrossRef]
- WHO Pandemic Preparedness. 2022. Available online: https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/pandemic-influenza/pandemic-preparedness (accessed on 26 January 2022).
- UK Pandemic Preparedness—GOV.UK. Available online: https://www.gov.uk/government/publications/uk-pandemic-preparedness/uk-pandemic-preparedness (accessed on 26 January 2022).




{kind=link}
{kind=link}
{kind=link}
| Vaccine Technologies | Humans | Equines | ||
|---|---|---|---|---|
| Available | Particulars | Available | Particulars | |
| Inactivated whole virus | Yes | Egg-based vaccine with excellent production capacity and low production cost but requires a supply of embryonated eggs and thus affected by shortages [166]. Contains complete virus antigenic components. Invokes a greater humoral immune response than a cellular one. Poorer cross-protection to viruses of different subtypes to that in the vaccine. Effectiveness in the elderly <50% [167]. High safety profile but not advisable for use in children as can cause a high fever. Used less now as subunit and split-virion vaccines are comparable immunologically and safer. | Yes | Requires multiple administrations to obtain a protective immune response and mainly invokes a humoral immune response [168]. Adjuvant added to improve immunogenicity [169] |
| Subunit | Yes | Produced using embryonated eggs. Safe vaccine [170] | Yes | Invokes a humoral and cell-mediated immune response [171]. Requires adjuvant to boost immunogenicity |
| Inactivated, split virus | Yes | Produced using embryonated eggs. Safe but poorer immunogenicity so requires two doses to overcome this. | No | Not available |
| Recombinant virus vector | Yes | Produced using virus vectors such as baculovirus (most successful) [172]. Higher cost of production than vaccines produced using eggs [166]. Induces cellular and humoral response and long duration of immunity. | Yes | Virus vectors used include canarypox. Immunity of a longer duration obtained. Invokes a robust cell-mediated response in addition to a humoral response. Has DIVA capability. Requires adjuvant to boost immunogenicity |
| Modified live-attenuated | Yes | Produced using embryonated eggs. As administered intranasally, produces local neutralizing antibody and a cell-mediated response [173]. Variable efficacy in adults but better efficacy in children [174]. Reversion to virulence or recombination with field virus is a possibility [175]. | Yes | Invokes a long lasting, robust cell-mediated response in addition to a humoral response, without the requirement of adjuvants. Reversion to virulence or recombination with field virus is a possibility [162] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Whitlock, F.; Murcia, P.R.; Newton, J.R. A Review on Equine Influenza from a Human Influenza Perspective. Viruses 2022, 14, 1312. https://doi.org/10.3390/v14061312
Whitlock F, Murcia PR, Newton JR. A Review on Equine Influenza from a Human Influenza Perspective. Viruses. 2022; 14(6):1312. https://doi.org/10.3390/v14061312
Chicago/Turabian StyleWhitlock, Fleur, Pablo R. Murcia, and J. Richard Newton. 2022. "A Review on Equine Influenza from a Human Influenza Perspective" Viruses 14, no. 6: 1312. https://doi.org/10.3390/v14061312