
Early and Longitudinal Humoral Response to the SARS-CoV-2 mRNA BNT162b2 Vaccine in Healthcare Workers: Significance of BMI, Adipose Tissue and Muscle Mass on Long-Lasting Post-Vaccinal Immunity

 , , , , ,
, , , , ,
Abstract
:1. Introduction
Aims
2. Materials and Methods
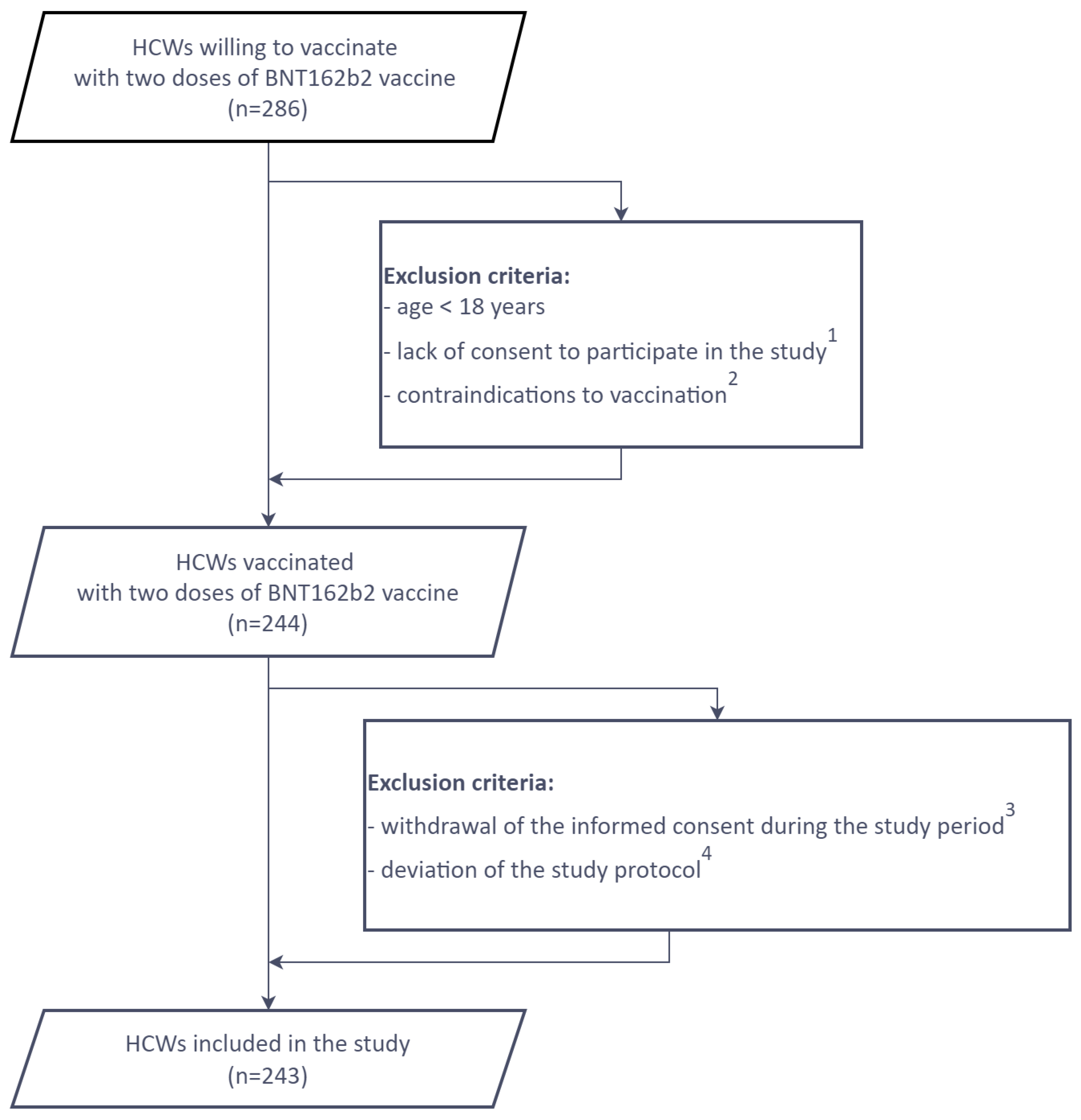
2.1. The Study Group
2.2. Participants’ Characteristics
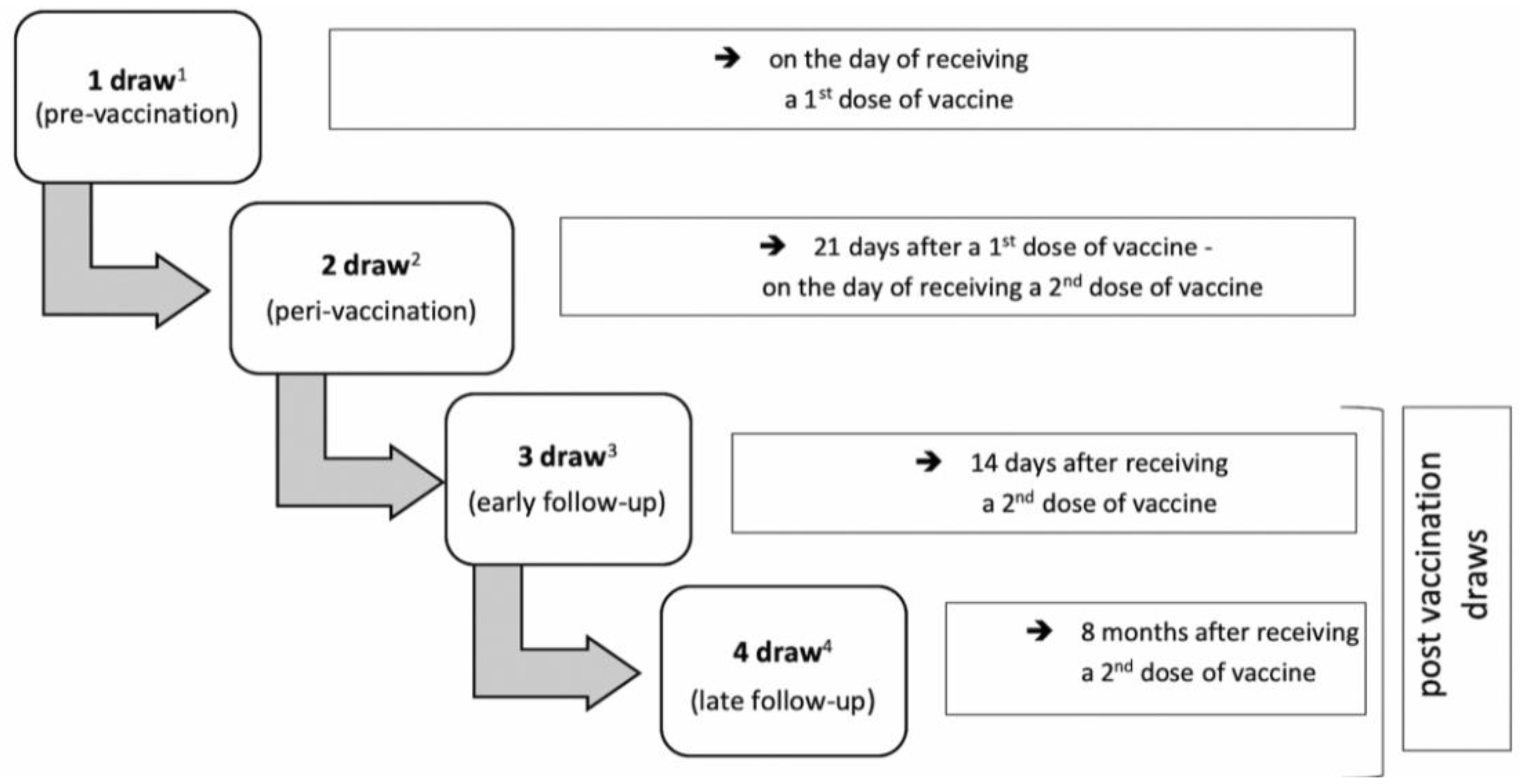
2.3. Anti-SARS-CoV-2 IgG Measurement
2.4. Body Composition Measurement Using the TANITA Analyzer
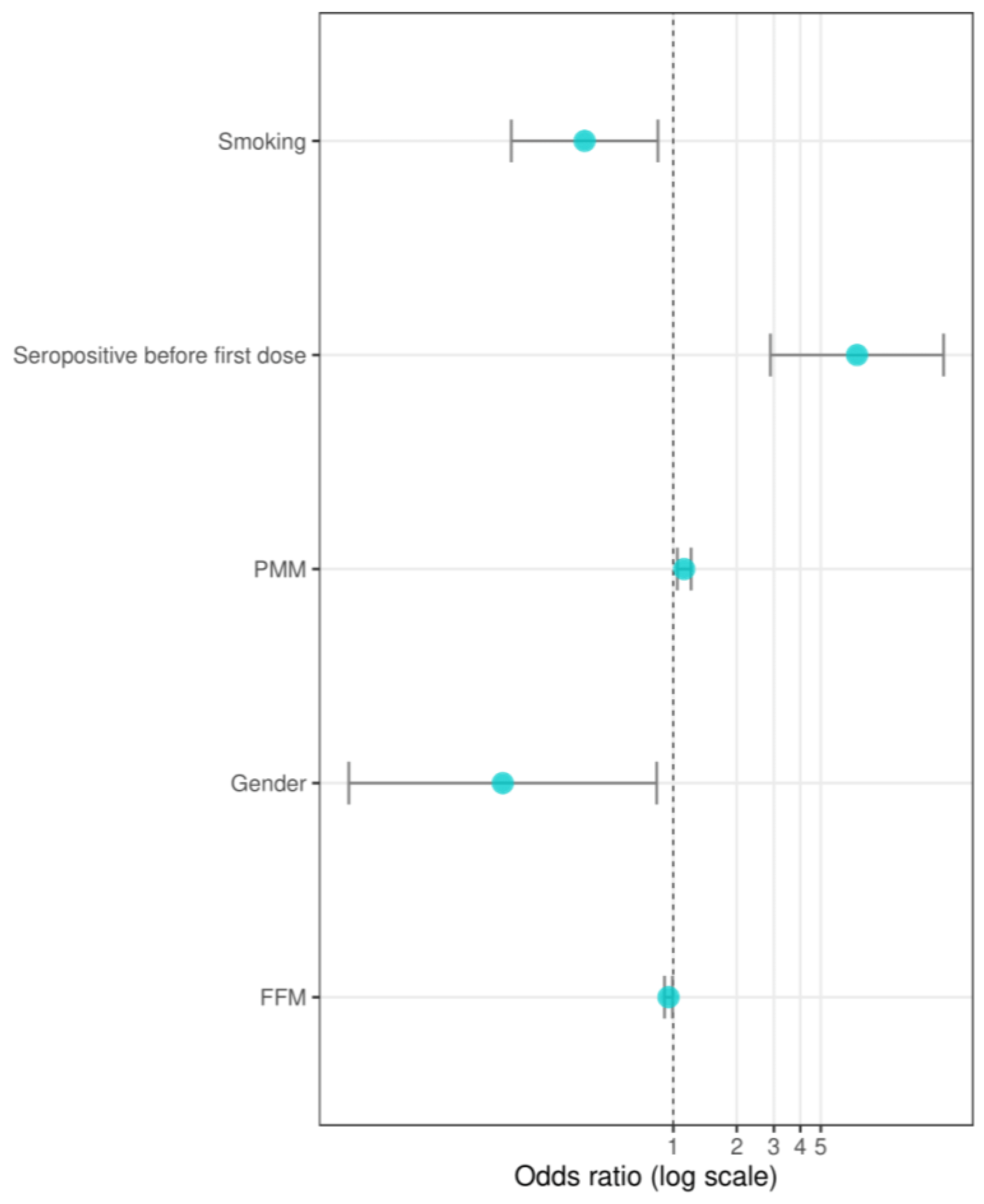
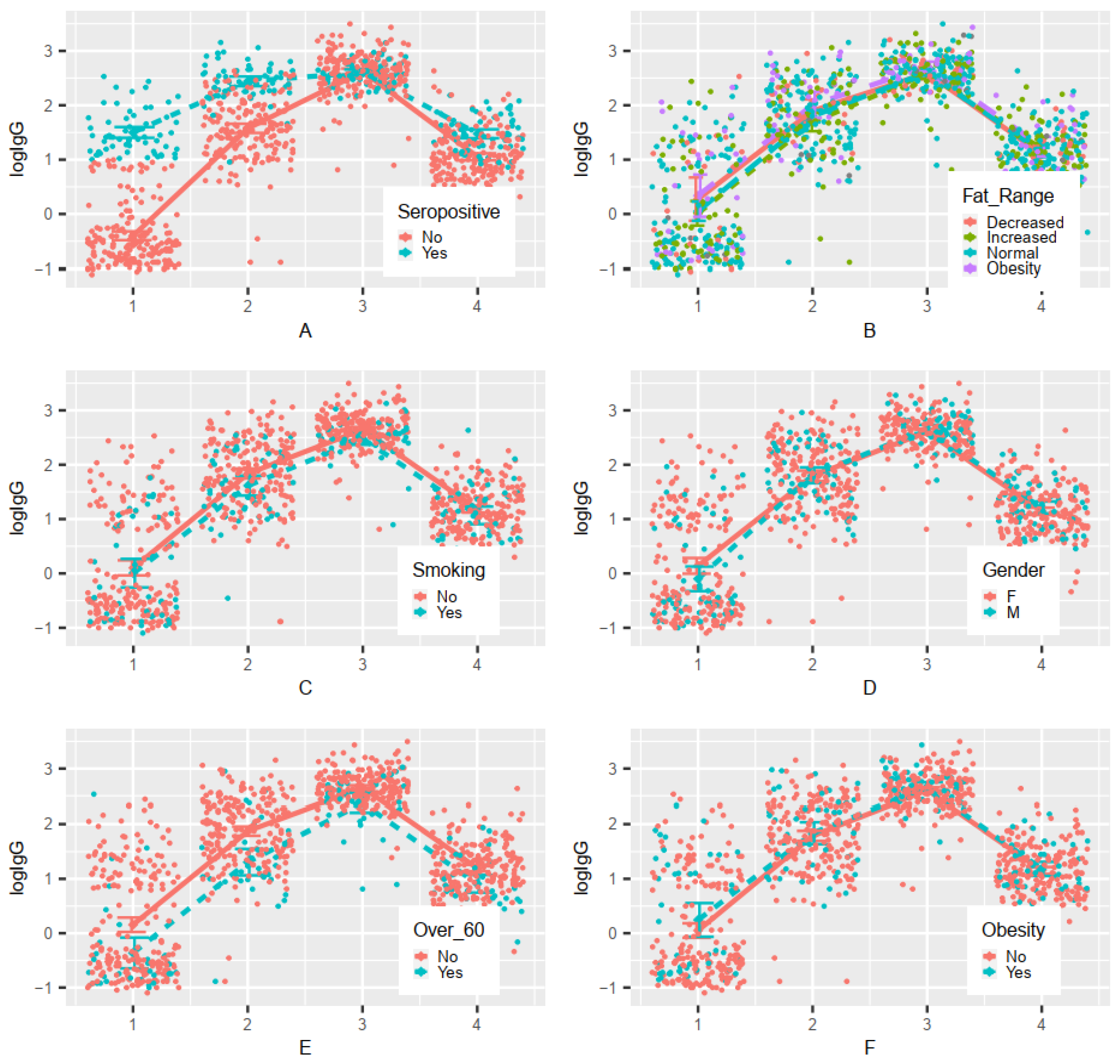
2.5. Statistical Analysis
3. Results
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, Z.; Lian, X.; Su, X.; Wu, W.; Marraro, G.A.; Zeng, Y. From SARS and MERS to COVID-19: A brief summary and comparison of severe acute respiratory infections caused by three highly pathogenic human coronaviruses. Respir. Res. 2020, 21, 224. [Google Scholar] [CrossRef] [PubMed]
- WHO Website: WHO COVID-19 Dashboard. Available online: https://covid19.who.int (accessed on 19 December 2021).
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/covid-cases#licence (accessed on 20 October 2021).
- European Centre for Disease Prevention and Control Website: COVID-19—Latest evidence—Risk factors and risk groups. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/risk-factors-risk-groups (accessed on 20 June 2021).
- Földi, M.; Farkas, N.; Kiss, S.; Dembrovszky, F.; Szakács, Z.; Balaskó, M.; Erőss, B.; Hegyi, P.; Szentesi, A. Visceral Adiposity Elevates the Risk of Critical Condition in COVID-19: A Systematic Review and Meta-Analysis. Obesity 2021, 29, 521–528. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Rostami, A.; Sepidarkish, M.; Leeflang, M.M.G.; Riahi, S.M. Nourollahpour Shiadeh, M.; Esfandyari, S.; Mokdad, A.H.; Hotez, P.J.; Gasser, R.B. SARS-CoV-2 seroprevalence worldwide: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 331–340. [Google Scholar] [CrossRef]
- Wolff, F.; Dahma, H.; Duterme, C.; Van den Wijngaert, S.; Vandenberg, O.; Cotton, F.; Montesinos, I. Monitoring antibody response following SARS-CoV-2 infection: Diagnostic efficiency of 4 automated immunoassays. Diagn. Microbiol. Infect. Dis. 2020, 98, 115140. [Google Scholar] [CrossRef]
- Huang, A.T.; Garcia-Carreras, B.; Hitchings, M.D.T.; Yang, B.; Katzelnick, L.C.; Rattigan, S.M.; Borgert, B.A.; Moreno, C.A.; Solomon, B.D.; Trimmer-Smith, L.; et al. A systematic review of antibody mediated immunity to coronaviruses: Kinetics, correlates of protection, and association with severity. Nat. Commun. 2020, 11, 4704. [Google Scholar] [CrossRef]
- Pollán, M.; Pérez-Gómez, B.; Pastor-Barriuso, R.; Oteo, J.; Hernán, M.A.; Pérez-Olmeda, M.; Sanmartín, J.L.; Fernández-García, A.; Cruz, I.; Fernández de Larrea, N.; et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): A nationwide, population-based seroepidemiological study. Lancet 2020, 396, 535–544. [Google Scholar] [CrossRef]
- Xu, X.; Sun, J.; Nie, S.; Li, H.; Kong, Y.; Liang, M.; Hou, J.; Huang, X.; Li, D.; Ma, T.; et al. Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China. Nat. Med. 2020, 26, 1193–1195. [Google Scholar] [CrossRef]
- Thomas, S.N.; Altawallbeh, G.; Zaun, C.P.; Pape, K.A.; Peters, J.M.; Titcombe, P.J.; Dileepan, T.; Rapp, M.J.; Bold, T.D.; Schacker, T.W.; et al. Initial determination of COVID-19 seroprevalence among outpatients and healthcare workers in Minnesota using a novel SARS-CoV-2 total antibody ELISA. Clin. Biochem. 2021, 90, 15–22. [Google Scholar] [CrossRef]
- Nguyen, L.H.; Drew, D.A.; Joshi, A.D.; Guo, C.-G.; Ma, W.; Mehta, R.S.; Sikavi, D.R.; Lo, C.-H.; Kwon, S.; Song, M.; et al. Risk of COVID-19 among frontline healthcare workers and the general community: A prospective cohort study. Lancet Public Health 2020, 5, e475–e483. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Moghadas, S.M.; Fitzpatrick, M.C.; Sah, P.; Pandey, A.; Shoukat, A.; Singer, B.H.; Galvani, A.P. The implications of silent transmission for the control of COVID-19 outbreaks. Proc. Natl. Acad. Sci. USA 2020, 117, 17513–17515. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Protocol for Assessment of Potential Risk Factors for 2019-Novel Coronavirus (COVID-19) Infection among Health Care Workers in a Health Care Setting. 2020. Available online: https://www.who.int/publications/i/item/protocol-for-assessment-of-potential-risk-factors-for-2019-novel-coronavirus-(2019-ncov)-infection-among-health-care-workers-in-a-health-care-setting (accessed on 2 March 2022).
- European Centre for Disease Prevention and Control Website: SARS-CoV-2 Variants Dashboard. 2022. Available online: https://www.ecdc.europa.eu/en/covid-19/situation-updates/variants-dashboard (accessed on 12 March 2022).
- SARS-CoV-2 w Polsce. 2022. Available online: https://sarswpolsce.pl (accessed on 12 March 2022).
- ACCESS SARS-CoV-2 IgG—Instructions for Use. Available online: https://www.fda.gov/media/139627/download (accessed on 20 January 2022).
- WHO Website: Body Mass Index—BMI. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 20 October 2020).
- RStudio Team. RStudio: Integrated Development for R. RStudio, PBC, Boston, 2020. Available online: http://www.rstudio.com/ (accessed on 20 December 2021).
- Wickham, H. Ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; Volume 2. [Google Scholar]
- Healthcare in Europe. Available online: https://healthcare-in-europe.com/en/news/should-covid-19-vaccination-be-mandatory-for-health-care-staff.html (accessed on 10 August 2021).
- Leggat, C.; Costantino, C.; Motta, G.; Cunsolo, R.; Stracquadanio, P.; Liberti, G.; Maltezou, H.C.; Rapisarda, V. SARS-CoV-2 mRNA Vaccine Breakthrough Infections in Fully Vaccinated Healthcare Personnel: A Systematic Review. Trop. Med. Infect. Dis. 2022, 7, 9. [Google Scholar]
- Chandan, S.; Chan, S.R.; Deliwala, S.; Mohana, B.P.; Ramai, D.; Chandan, O.C.; Facciorusso, A. Postvaccination SARS-CoV-2 infection among healthcare workers—A Systematic Review and meta-analysis. J. Med. Virol. 2022, 94, 1428–1441. [Google Scholar] [CrossRef]
- Marra, A.R.; Kobayashi, T.; Suzuki, H.; Alsuhaibani, M.; Tofaneto, B.M.; Bariani, L.M.; Auler, M.; Salinas, J.L.; Edmond, M.B.; Pinho, J.R.; et al. The short-term effectiveness of coronavirus disease 2019 (COVID-19) vaccines among healthcare workers: A systematic literature review and meta-analysis. ASHE 2021, 1, e33. [Google Scholar] [CrossRef]
- Hossain, A.; Nasrullah, S.M.; Tasnim, Z.; Hasan, K.; Hasan, M. Seroprevalence of SARS-CoV-2 IgG antibodies among health care workers prior to vaccine administration in Europe, the USA and East Asia: A systematic review and meta-analysis. EClinicalMedicine 2021, 33, 100770. [Google Scholar] [CrossRef]
- Liu, Q.; Qin, C.; Liu, M.; Liu, J. Effectiveness and safety of SARS-CoV-2 vaccine in real-world studies: A systematic review and meta-analysis. Infect. Dis. Poverty 2021, 10, 132. [Google Scholar] [CrossRef]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 COVID-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef]
- Novello, S.; Terzolo, M.; Paola, B.; Gianetta, M.; Bianco, V.; Arizio, F.; Brero, D.; Perini, A.M.E.; Boccuzzi, A.; Caramello, V. Humoral immune response to SARS-CoV-2 in five different groups of individuals at different environmental and professional risk of infection. Sci. Rep. 2021, 11, 24503. [Google Scholar] [CrossRef]
- Yi, H. 2019 Novel Coronavirus Is Undergoing Active Recombination. Clin. Infect. Dis. 2020, 71, 884–887. [Google Scholar] [CrossRef]
- Haynes, L. Aging of the Immune System: Research Challenges to Enhance the Health Span of Older Adults. Front. Aging 2020, 1, 602108. [Google Scholar] [CrossRef]
- Ortona, E.; Pierdominici, M.; Rider, V. Editorial: Sex Hormones and Gender Differences in Immune Responses. Front. Immunol. 2019, 10, 1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shreeves, R. COVID-19: The Need for a Gendered Response. European Parliamentary Research Service—Briefing. Brussels: PE 68348. Available online: https://www.europarl.europa.eu/RegData/etudes/BRIE/2021/689348/EPRS_BRI(2021)689348_EN.pdf (accessed on 8 February 2021).
- Klein, S.; Flanagan, K. Sex differences in immune responses. Nat. Rev. Immunol. 2016, 16, 626–638. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention Website. Evidence Used to Update the List of Underlying Medical Conditions That Increase a Person’s Risk of Severe Illness from COVID-19; Center for Disease Control and Prevention: Atlanta, GA, USA, 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extraprecautions/evidence-table.html (accessed on 15 June 2021).
- Figliozzi, S.; Masci, P.G.; Ahmadi, N.; Tondi, L.; Koutli, E.; Aimo, A.; Stamatelopoulos, K.; Dimopoulos, M.A.; Caforio, A.L.P.; Georgiopoulos, G. Predictors of adverse prognosis in COVID-19: A systematic review and meta-analysis. Eur. J. Clin. Investig. 2020, 50, e13362. [Google Scholar] [CrossRef]
- Powell, T.; Bellin, E.; Enrich, A.R. Older Adults and COVID-19: The Most Vulnerable, the Hardest Hit. Hastings Cent. Rep. 2020, 50, 61–63. [Google Scholar] [CrossRef]
- Amodio, E.; Capra, G.; Casuccio, A.; Grazia, S.; Genovese, D.; Pizzo, S.; Calamusa, G.; Ferraro, D.; Giammanco, G.M.; Vitale, F.; et al. Antibodies Responses to SARS-CoV-2 in a Large Cohort of Vaccinated Subjects and Seropositive Patients. Vaccines 2021, 9, 714. [Google Scholar] [CrossRef]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Müller, L.; Andrée, M.; Moskorz, W.; Drexler, I.; Walotka, L.; Grothmann, R.; Ptok, J.; Hillebrandt, J.; Ritchie, A.; Rabl, D.; et al. Age-dependent Immune Response to the BioNTech/Pfizer BNT162b2 Coronavirus Disease 2019 Vaccination. Clin. Infect. Dis. 2021, 73, 2065–2072. [Google Scholar] [CrossRef]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. J. Med. Virol. 2021, 93, 250–256. [Google Scholar] [CrossRef]
- Nelke, C.; Dziewas, R.; Minnerup, J.; Meuth, S.G.; Ruck, T. Skeletal muscle as a potential central link between sarcopenia and immune senescence. EBioMedicine 2019, 49, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Piqueras, P.; Ballester, A.; Durá-Gil, J.V.; Martinez-Hervas, S.; Redón, J.; Real, J.T. Anthropometric Indicators as a Tool for Diagnosis of Obesity and Other Health Risk Factors: A Literature Review. Front. Psychol. 2021, 12, 631179. [Google Scholar] [CrossRef] [PubMed]
- Lamas, O.; Marti, A.; Martínez, J.A. Obesity and immunocompetence. Eur. J. Clin. Nutr. 2002, 56, 42–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karchynskaya, V.; Kopcakova, J.; Klein, D.; Gába, A.; Madarasova-Geckova, A.; van Dijk, J.P.; de Winter, A.F.; Reijneveld, S.A. Is BMI a Valid Indicator of Overweight and Obesity for Adolescents? Int. J. Environ. Res. Public Health 2020, 17, 4815. [Google Scholar] [CrossRef]
- Frankenfield, D.C.; Rowe, W.A.; Cooney, R.N.; Smith, J.S.; Becker, D. Limits of body mass index to detect obesity and predict body composition. Nutrition 2001, 17, 26–30. [Google Scholar] [CrossRef]
- Sattar, N.; Valabhji, J. Obesity as a Risk Factor for Severe COVID-19: Summary of the Best Evidence and Implications for Health Care. Curr. Obes. Rep. 2021, 10, 282–289. [Google Scholar] [CrossRef]
- Kompaniyets, L.; Goodman, A.B.; Belay, B.; Freedman, D.S.; Sucosky, M.S.; Lange, S.J.; Gundlapalli, A.V.; Boehmer, T.K.; Blanck, H.M. Body Mass Index and Risk for COVID-19–Related Hospitalization, Intensive Care Unit Admission, Invasive Mechanical Ventilation, and Death—United States, March–December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 355–361. [Google Scholar] [CrossRef]
- Samartín, S.; Chandra, R.K. Obesity, overnutrition and the immune system. Nutr. Res. 2001, 21, 243–262. [Google Scholar] [CrossRef]
- Chandra, R.K.; Sarchielli, P. Body size and immune responses. Nutr. Res. 1996, 16, 1813–1819. [Google Scholar] [CrossRef]
- de Heredia, F.P.; Gómez-Martínez, S.; Marcos, A. Obesity, inflammation and the immune system. Proc. Nutr. Soc. 2012, 71, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Muscogiuri, G.; Pugliese, G.; Laudisio, D.; Castellucci, B.; Barrea, L.; Savastano, S.; Colao, A. The impact of obesity on immune response to infection: Plausible mechanisms and outcomes. Obes. Rev. 2021, 22, e13216. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Zorita, S.; Milton-Laskibar, I.; García-Arellano, L.; González, M.; Portillo, M.P. An Overview of Adipose Tissue ACE2 Modulation by Diet and Obesity. Potential Implications in COVID-19 Infection and Severity. Int. J. Mol. Sci. 2021, 22, 7975. [Google Scholar] [CrossRef] [PubMed]
- Ferrante, A.W., Jr. The immune cells in adipose tissue. Diabetes Obes. Metab. 2013, 15, 34–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauri, C.; Bosma, A. Immune regulatory function of B cells. Annu. Rev. Immunol. 2012, 30, 221–241. [Google Scholar] [CrossRef]
- Ko, J.Y.; Danielson, M.L.; Town, M.; Derano, G.; Greenlund, K.J.; Kirley, P.D.; Alden, N.B.; Yousey-Hindes, K.; Anderson, E.J.; Ryan, P.A.; et al. Risk factors for coronavirus disease 2019 (COVID-19)–associated hospitalization: COVID-19—Associated Hospitalization Surveillance Network and Behavioral Risk Factor Surveillance System. Clin. Infect. Dis. 2021, 72, e695–e703. [Google Scholar] [CrossRef]
- Ledford, H. Could obesity could create problems for a COVID vaccine? Nature 2020, 586, 488–489. [Google Scholar] [CrossRef]
- Frasca, D.; Ferracci, F.; Diaz, A.; Romero, M.; Lechner, S.; Blomberg, B.B. Obesity decreases B cell responses in young and elderly individuals. Obesity 2016, 24, 615–625. [Google Scholar] [CrossRef]
- Weber, D.J.; Rutala, W.A.; Samsa, G.P.; Santimaw, J.E.; Lemon, S.M. Obesity as a predictor of poor antibody response to hepatitis B plasma vaccine. JAMA 1985, 254, 3187–3189. [Google Scholar] [CrossRef]
- Weber, D.J.; Rutala, W.A.; Samsa, G.P.; Bradshaw, S.E.; Lemon, S.M. Impaired immunogenicity of hepatitis B vaccine in obese persons. N. Engl. J. Med. 1986, 314, 1393. [Google Scholar]
- Sheridan, P.A.; Paich, H.A.; Handy, J.; Karlsson, E.A.; Hudgens, M.G.; Sammon, A.B.; Holland, L.A.; Weir, S.; Noah, T.L.; Beck, M.A. Obesity is associated with impaired immune response to influenza vaccination in humans. Int. J. Obes. 2012, 36, 1072–1077. [Google Scholar] [CrossRef] [Green Version]
- Banga, N.; Guss, P.; Banga, A.; Rosenman, K.D. Incidence and variables associated with inadequate antibody titers after pre-exposure rabies vaccination among veterinary medical students. Vaccine 2014, 32, 979–983. [Google Scholar] [CrossRef] [PubMed]
- Green, W.D.; Beck, M.A. Obesity impairs the adaptive immune response to influenza virus. Ann. Am. Thorac. Soc. 2017, 14, S406–S409. [Google Scholar] [CrossRef] [PubMed]
- Butsch, W.S.; Hajduk, A.; Cardel, M.I.; Donahoo, W.T.; Kyle, T.K.; Stanford, F.C.; Zeltser, L.M.; Kotz, C.M.; Jastreboff, A.M. COVID-19 vaccines are effective in people with obesity: A position statement from the Obesity Society. Obesity 2021, 29, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Hagiwara, E.; Takahashi, K.I.; Okubo, T.; Ohno, S.; Ueda, A.; Aoki, A.; Odagiri, S.; Ishigatsubo, Y. Cigarette smoking depletes cells spontaneously secreting Th (1) cytokines in the human airway. Cytokine 2001, 14, 121–126. [Google Scholar] [CrossRef]
- Qiu, F.; Liang, C.L.; Liu, H.; Zeng, Y.Q.; Hou, S.; Huang, S.; Lai, X.; Dai, Z. Impacts of cigarette smoking on immune responsiveness: Up and down or upside down? Oncotarget 2017, 8, 268–284. [Google Scholar] [CrossRef] [Green Version]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Tsatsakis, A.; Vakonaki, E.; Tzatzarakis, M.; Flamourakis, M.; Nikolouzakis, T.K.; Poulas, K.; Papazoglou, G.; Hatzidaki, E.; Papanikolaou, N.C.; Drakoulis, N. Immune response (IgG) following full inoculation with BNT162b2 COVID-19 mRNA among healthcare professionals. Int. J. Mol. Med. 2021, 48, 200. [Google Scholar] [CrossRef]
- Parthymou, A.; Habeos, E.E.; Habepr, G.I.; Deligakis, A.; Livieratos, E.; Marangos, M.; Chartoumpekis, D.V. SARS-CoV-2 antibody titer 3 months post-vaccination is affected by age, gender, smoking and vitamin D. MedRxiv 2021, 21262913. [Google Scholar]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Kurihara, M.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; et al. Age and Smoking Predict Antibody Titres at 3 Months after the Second Dose of the BNT162b2 COVID-19 Vaccine. Vaccines 2021, 9, 1042. [Google Scholar] [CrossRef]
- MacKenzie, J.; MacKenzie, I.; Holt, P. The effect of cigarette smoking on susceptibility to epidemic influenza and on serological responses to live attenuated and killed subunit influenza vaccines. J. Hyg. 1976, 77, 409–417. [Google Scholar] [CrossRef] [Green Version]
- Lippi, G.; Sanchis-Gomar, F.; Henry, B.M. Coronavirus disease 2019 (COVID-19): The portrait of a perfect storm. Ann. Transl. Med. 2020, 8, 497. [Google Scholar] [CrossRef] [PubMed]
- WHO Website. Weekly Epidemiological Update on COVID-19; WHO: Geneva, Switzerland, 8 June 2021; Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---8-june-2021 (accessed on 10 June 2021).
- Dejnirattisai, W.; Shaw, R.H.; Supasa, P.; Liu, C.; Stuart, A.S.V.; Pollard, A.J.; Liu, X.; Lambe, T.; Crook, D.; Stuart, D.I.; et al. Reduced neutralization of SARS-CoV-2 Omicron-B.1.1.529 variant by post-immunisation serum. Lancet 2022, 399, 234–236. [Google Scholar] [CrossRef]
- Wang, P.; Nair, M.S.; Liu, L.; Iketani, S.; Luo, Y.; Guo, Y.; Wang, M.; Yu, J.; Zhang, B.; Kwong, P.D.; et al. Antibody Resistance of SARS-CoV-2 Variants B.1.351 and B.1.1.7. Nature 2021, 593, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Nasreen, S.; Chung, H.; He, S.; Brown, K.A.; Gubbay, J.B.; Buchan, S.A.; Fell, D.B.; Austin, P.C.; Schwartz, K.L.; Sundaram, M.E.; et al. Canadian Immunization Research Network (CIRN) Provincial Collaborative Network (PCN) Investigators. Effectiveness of COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe outcomes with variants of concern in Ontario. Nat. Micr-obiol. 2022, 7, 379–385. [Google Scholar] [CrossRef]
- Charmet, T.; Schaeffer, L.; Grant, R.; Galmiche, S.; Chény, O.; Von Platen, C.; Maurizot, A.; Rogoff, A.; Omar, F.; David, C.; et al. Impact of original, B.1.1.7, and B.1.351/P.1 SARS-CoV-2 lineages on vaccine effectiveness of two doses of COVID-19 mRNA vaccines: Results from a nationwide case-control study in France. Lancet Reg. Health 2021, 8, 100171. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | |
|---|---|---|
| Women | 187 | 76.95 |
| Men | 56 | 23.05 |
| Age over 60 years | 33 | 13.58 |
| Medical staff * | 203 | 83.54 |
| Administrative staff ** | 29 | 11.93 |
| Diagnostic/sterilization staff *** | 11 | 4.53 |
| Chronic diseases | 73 | 30.04 |
| Smoking | 45 | 18.52 |
| Obesity (BMI ≥ 30.00) | 44 | 18.11 |
| Seropositivity before the first dose | 62 | 25.51 |
| Seropositivity eight months after the second dose | 150 | 61.73 |
| Parameters | Mean | SD |
| Age (years) | 47.42 | 12.45 |
| Metabolic age (years) | 43.14 | 15.75 |
| BFM (kg) | 21.81 | 9.80 |
| FFM (kg) | 51.68 | 11.35 |
| Body fat percentage (%) | 28.92 | 8.03 |
| Body fat range (level) | 6.82 | 4.16 |
| TBW (kg) | 36.76 | 7.88 |
| PMM (kg) | 49.13 | 10.60 |
| Bone tissue mass (kg) | 2.61 | 0.53 |
| Impedance (Ohm) | 615.97 | 115.18 |
| BMR (kJ) | 6446.18 | 1371.61 |
| IgG (pre-vaccination) (AU/mL) | 14.16 | 40.14 |
| IgG (peri-vaccination) (AU/mL) | 147.08 | 200.96 |
| IgG (post-vaccination—early FU) (AU/mL) | 538.81 | 423.28 |
| IgG (post-vaccination—late FU) (AU/mL) | 26.01 | 40.57 |
| IgG (AU/mL) | before the First Dose | before the Second Dose | Early FU | Late FU | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| <10.00 seronegative | 181 | 74.49 | 22 | 9.05 | 2 | 0.82 | 93 | 38.27 |
| ≥10.00–50.00 (low response) | 46 | 18.93 | 88 | 36.21 | 3 | 1.23 | 122 | 50.21 |
| >50.00–100.00 | 7 | 2.88 | 30 | 12.35 | 3 | 1.23 | 19 | 7.82 |
| >100.00–200.00 | 5 | 2.06 | 41 | 16.87 | 23 | 9.47 | 7 | 2.88 |
| >200.00–350.00 | 4 | 1.65 | 36 | 14.81 | 64 | 26.34 | 1 | 0.41 |
| >350.00 (high response) | 0 | 0.00 | 26 | 10.70 | 148 | 60.91 | 1 | 0.41 |
| ≥10.00 seropositive (in all) | 62 | 25.51 | 221 | 90.95 | 241 | 99.18 | 150 | 61.73 |
| Variable | n (%) | p Value | OR | 95% CI |
|---|---|---|---|---|
| Gender | ||||
| Male | 56 (23.05) | 0.45 | 1.28 | 0.68–2.38 |
| Female | 187 (76.95) | 1.00 | ||
| Age (years) | ||||
| >60 | 33 (13.58) | 0.00 | 0.30 | 0.14–0.64 |
| <60 | 210 (86.42) | 1.00 | ||
| Smoking | ||||
| Yes | 45 (18.52) | 0.11 | 0.58 | 0.30–1.12 |
| No | 198 (81.48) | 1.00 | ||
| BMI (kg/m2) | ||||
| ≥25.00 | 133 (54.73) | 0.61 | 1.14 | 0.68–1.92 |
| <25.00 | 110 (45.27) | 1.00 | ||
| Obesity (BMI ≥ 30.00) | ||||
| Yes | 44 (18.11) | 0.77 | 1.10 | 0.56–2.17 |
| No | 199 (81.89) | 1.00 | ||
| Seropositivity before the 1. dose of vaccine | 62 (25.51) | 0.00 | 8.64 | 3.54–21.06 |
| BFM (kg) | 0.96 | 1.00 | 0.97–1.03 | |
| FFM (kg) | 0.08 | 1.02 | 1.00–1.05 | |
| TBW (kg) | 0.06 | 1.03 | 1.00–1.07 | |
| PMM (kg) | 0.06 | 1.03 | 1.00–1.05 | |
| Bone mass (kg) | 0.09 | 1.56 | 0.93–2.64 | |
| Impedance (Ohm) | 0.44 | 1.00 | 1.00–1.00 | |
| BMR (kJ) | 0.06 | 1.00 | 1.00–1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golec, M.; Fronczek, M.; Zembala-John, J.; Chrapiec, M.; Konka, A.; Wystyrk, K.; Botor, H.; Brzoza, Z.; Kasperczyk, S.; Bułdak, R.J. Early and Longitudinal Humoral Response to the SARS-CoV-2 mRNA BNT162b2 Vaccine in Healthcare Workers: Significance of BMI, Adipose Tissue and Muscle Mass on Long-Lasting Post-Vaccinal Immunity. Viruses 2022, 14, 868. https://doi.org/10.3390/v14050868
Golec M, Fronczek M, Zembala-John J, Chrapiec M, Konka A, Wystyrk K, Botor H, Brzoza Z, Kasperczyk S, Bułdak RJ. Early and Longitudinal Humoral Response to the SARS-CoV-2 mRNA BNT162b2 Vaccine in Healthcare Workers: Significance of BMI, Adipose Tissue and Muscle Mass on Long-Lasting Post-Vaccinal Immunity. Viruses. 2022; 14(5):868. https://doi.org/10.3390/v14050868
Chicago/Turabian StyleGolec, Marlena, Martyna Fronczek, Joanna Zembala-John, Martyna Chrapiec, Adam Konka, Karolina Wystyrk, Hanna Botor, Zenon Brzoza, Sławomir Kasperczyk, and Rafał Jakub Bułdak. 2022. "Early and Longitudinal Humoral Response to the SARS-CoV-2 mRNA BNT162b2 Vaccine in Healthcare Workers: Significance of BMI, Adipose Tissue and Muscle Mass on Long-Lasting Post-Vaccinal Immunity" Viruses 14, no. 5: 868. https://doi.org/10.3390/v14050868