
Avidity of IgG to SARS-CoV-2 RBD as a Prognostic Factor for the Severity of COVID-19 Reinfection

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Study Groups
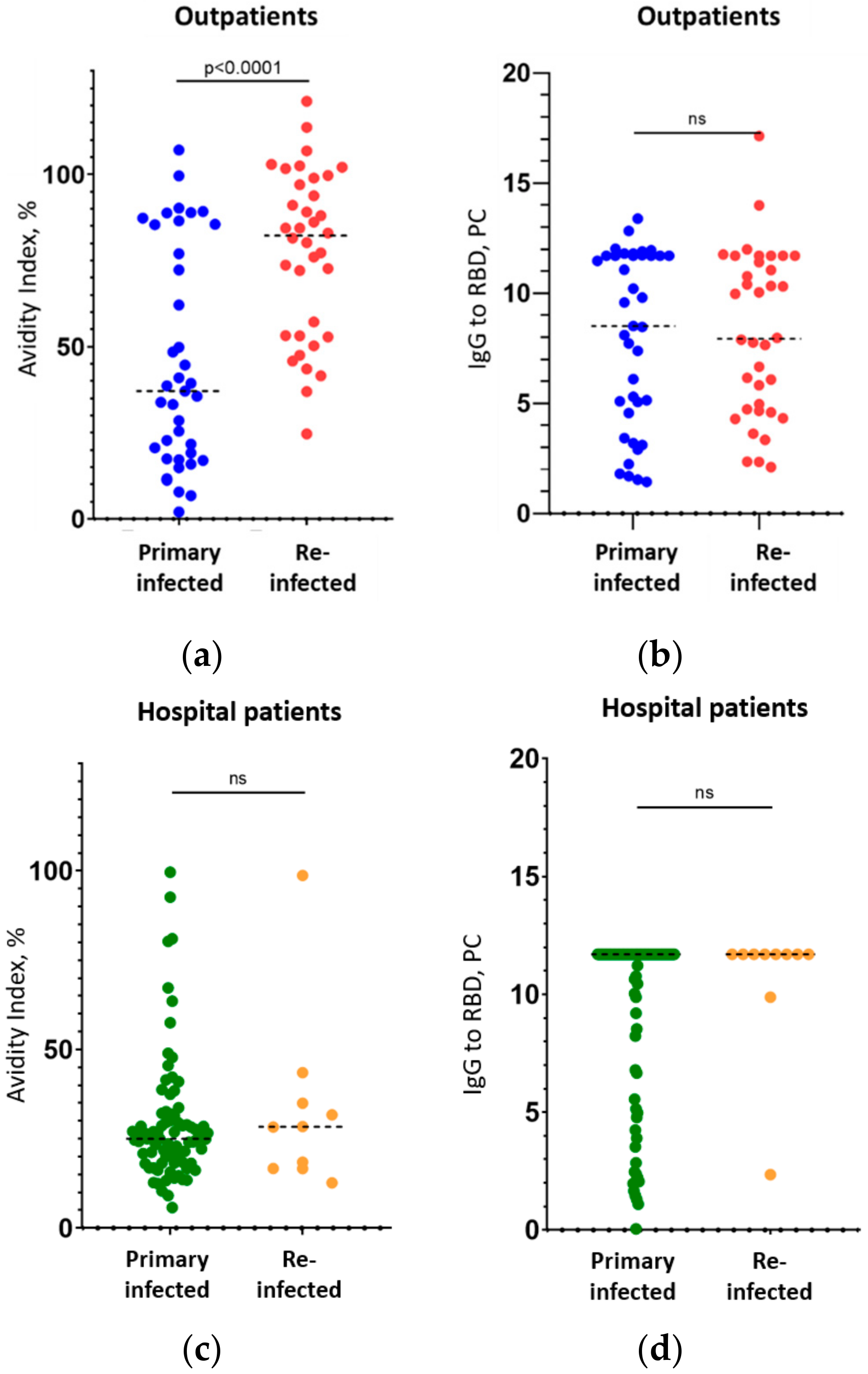
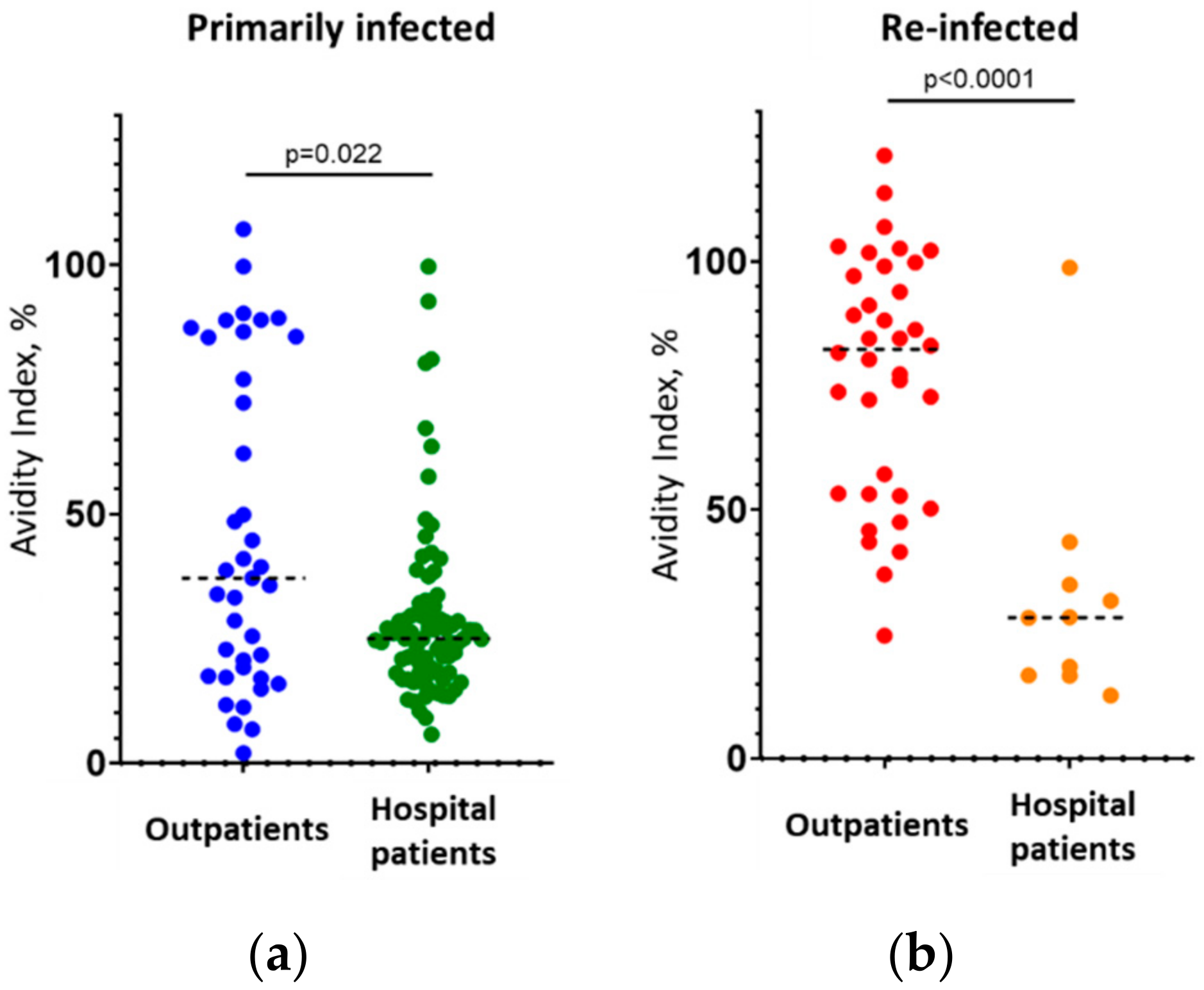
3.2. Correlation between the IgG Avidity Index and the Severity of Reinfection
- -
- If low-avidity IgG (AI ≤ 40%) is found in a repeat COVID-19 patient, there is an 89 ± 20.5% chance (p < 0.05) that the disease will be severe, and the patient will require hospitalization;
- -
- If high-avidity IgG (AI ≥ 50%) is found in a repeat COVID-19 patient, there is a 94 ± 7.9% chance (p < 0.05) that the disease will be mild, and the patient will not require hospitalization.
4. Discussion
- -
- -
- -
- (1)
- If a patient who has had immunization in the past returns with a diagnosis of COVID-19 reinfection, they should be immediately tested for the avidity of their IgG to Spike/RBD. If IgG of low avidity are found (AI ≤ 40%, if the test used is similar to that used in the present study), the patient needs close monitoring since, according to our data, 89 ± 20.5% (p < 0.05) of these patients will suffer a severe course of the repeated disease and will require hospitalization.
- (2)
- Where possible, all healthy patients immunized against SARS-CoV-2 more than 4 months ago should be tested for their antibody avidity. If the patient still carries IgG of low avidity, preventive revaccination may be recommended [40] because it is highly likely that the patient has not developed sustained immunity and, if reinfected, the patient has a high probability of a severe course of repeated COVID-19.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lumley, S.F.; O’Donnell, D.; Stoesser, N.E.; Matthews, P.C.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; Cox, S.; James, T.; Warren, F.; et al. Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers. N. Engl. J. Med. 2021, 384, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Narrainen, F.; Shakeshaft, M.; Asad, H.; Holborow, A.; Blyth, I.; Healy, B. The protective effect of previous COVID-19 infection in a high-prevalence hospital setting. Clin. Med. 2021, 21, e470–e474. [Google Scholar] [CrossRef] [PubMed]
- Iversen, K.; Kristensen, J.H.; Hasselbalch, R.B.; Pries-Heje, M.; Nielsen, P.B.; Knudsen, A.D.; Fogh, K.; Norsk, J.B.; Andersen, O.; Fischer, T.K.; et al. Seroprevalence of SARS-CoV-2 antibodies and reduced risk of reinfection through six months: A Danish observational cohort study of 44,000 healthcare workers. Clin. Microbiol. Infect. 2021; in press. [Google Scholar] [CrossRef]
- Slezak, J.; Bruxvoort, K.; Fischer, H.; Broder, B.; Ackerson, B.; Tartof, S. Rate and severity of suspected SARS-CoV-2 reinfection in a cohort of PCR-positive COVID-19 patients. Clin. Microbiol. Infect. 2021, 27, 1860.e7–1860.e10. [Google Scholar] [CrossRef] [PubMed]
- Wilkins, J.T.; Hirschhorn, L.R.; Gray, E.L.; Wallia, A.; Carnethon, M.; Zembower, T.R.; Ho, J.; DeYoung, B.J.; Zhu, A.; Rasmussen-Torvik, L.J.; et al. Serologic Status and SARS-CoV-2 Infection over 6 Months of Follow Up in Healthcare Workers in Chicago: A Cohort Study. Infect. Control Hosp. Epidemiol. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sanaie, S.; Golipour, E.; Shamekh, A.; Sadaie, M.R.; Mahmoodpoor, A.; Yousefi, M. Immune response variables and viral mutations impact on COVID-19 reinfection and relapse. Int. Immunopharmacol. 2021, 100, 108108. [Google Scholar] [CrossRef]
- Santiago-Espinosa, O.; Prieto-Torres, M.E.; Cabrera-Gaytán, D.A. Laboratory-confirmed SARS-CoV-2 reinfection in the population treated at social security. Respir. Med. Case Rep. 2021, 34, 101493. [Google Scholar] [CrossRef]
- Wu, L.P.; Wang, N.C.; Chang, Y.H.; Tian, X.Y.; Na, D.Y.; Zhang, L.Y.; Zheng, L.; Lan, T.; Wang, L.F.; Liang, G.D. Duration of antibody responses after severe acute respiratory syndrome. Emerg. Infect. Dis. 2007, 13, 1562–1564. [Google Scholar] [CrossRef]
- Edridge, A.W.D.; Kaczorowska, J.; Hoste, A.C.R.; Bakker, M.; Klein, M.; Loens, K.; Jebbink, M.F.; Matser, A.; Kinsella, C.M.; Rueda, P.; et al. Seasonal coronavirus protective immunity is short-lasting. Nat. Med. 2020, 26, 1691–1693. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Barnes, C.O.; West, A.P.; Huey-Tubman, K.E.; Hoffmann, M.A.G.; Sharaf, N.G.; Hoffman, P.R.; Koranda, N.; Gristick, H.B.; Gaebler, C.; Muecksch, F.; et al. Structures of Human Antibodies Bound to SARS-CoV-2 Spike Reveal Common Epitopes and Recurrent Features of Antibodies. Cell 2020, 182, 828–842. [Google Scholar] [CrossRef] [PubMed]
- Wajnberg, A.; Amanat, F.; Firpo, A.; Altman, D.R.; Bailey, M.J.; Mansour, M.; McMahon, M.; Meade, P.; Mendu, D.R.; Muellers, K.; et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science 2020, 370, 1227–1230. [Google Scholar] [CrossRef] [PubMed]
- Bauer, G. The variability of the serological response to SARS-corona virus-2: Potential resolution of ambiguity through determination of avidity (functional affinity). J. Med. Virol. 2020, 93, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Hedman, K.; Seppälä, I. Recent rubella virus infection indicated by a low avidity of specific IgG. J. Clin. Immunol. 1988, 8, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, J.; Maroto, C. Are IgG antibody avidity assays useful in the diagnosis of infectious diseases? A review. Microbios 1996, 87, 113–121. [Google Scholar] [PubMed]
- Dörner, T.; Radbruch, A. Antibodies and B cell memory in viral immunity. Immunity 2007, 27, 384–392. [Google Scholar] [CrossRef] [Green Version]
- Chan, P.K.; Lim, P.L.; Liu, E.Y.; Cheung, J.L.; Leung, D.T.; Sung, J.J. Antibody avidity maturation during severe acute respiratory syndrome-associated coronavirus infection. J. Infect. Dis. 2005, 192, 166–169. [Google Scholar] [CrossRef]
- Chan, K.H.; Sonnenberg, K.; Niedrig, M.; Lam, S.Y.; Pang, C.M.; Chan, K.M.; Ma, S.K.; Seto, W.H.; Peiris, J.S. Use of antibody avidity assays for diagnosis of severe acute respiratory syndrome coronavirus infection. Clin. Vaccine Immunol. 2007, 14, 1433–1436. [Google Scholar] [CrossRef] [Green Version]
- Klein, S.L.; Pekosz, A.; Park, H.S.; Ursin, R.L.; Shapiro, J.R.; Benner, S.E.; Littlefield, K.; Kumar, S.; Naik, H.M.; Betenbaugh, M.J.; et al. Sex, age, and hospitalization drive antibody responses in a COVID-19 convalescent plasma donor population. J. Clin. Investig. 2020, 130, 6141–6150. [Google Scholar] [CrossRef]
- Liu, T.; Hsiung, J.; Zhao, S.; Kost, J.; Sreedhar, D.; Hanson, C.V.; Olson, K.; Keare, D.; Chang, S.T.; Bliden, K.P.; et al. Quantification of antibody avidities and accurate detection of SARS-CoV-2 antibodies in serum and saliva on plasmonic substrates. Nat. Biomed. Eng. 2020, 4, 1188–1196. [Google Scholar] [CrossRef]
- Luo, Y.R.; Chakraborty, I.; Yun, C.; Wu, A.H.B.; Lynch, K.L. Kinetics of SARS-CoV-2 antibody avidity maturation and association with disease severity. Clin. Infect. Dis. 2020, 73, e3095–e3097. [Google Scholar] [CrossRef] [PubMed]
- Vauloup-Fellous, C.; Grangeot-Keros, L. Humoral immune response after primary rubella virus infection and after vaccination. Clin. Vaccine Immunol. 2007, 14, 644–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revello, M.G.; Zavattoni, M.; Furione, M.; Lilleri, D.; Gorini, G.; Gerna, G. Diagnosis and outcome of preconceptional and periconceptional primary human cytomegalovirus infections. J. Infect. Dis. 2002, 186, 553–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Souza, V.A.; Fernandes, S.; Araújo, E.S.; Tateno, A.F.; Oliveira, O.M.; Oliveira, R.R.; Pannuti, C.S. Use of an immunoglobulin G avidity test to discriminate between primary and secondary dengue virus infections. J. Clin. Microbiol. 2004, 42, 1782–1784. [Google Scholar] [CrossRef] [Green Version]
- Zhang, B.; Pinsky, B.A.; Ananta, J.S.; Zhao, S.; Arulkumar, S.; Wan, H.; Sahoo, M.K.; Abeynayake, J.; Waggoner, J.J.; Hopes, C.; et al. Diagnosis of Zika virus infection on a nanotechnology platform. Nat. Med. 2017, 23, 548–550. [Google Scholar] [CrossRef]
- Amaro, F.; Sánchez-Seco, M.P.; Vázquez, A.; Alves, M.J.; Zé-Zé, L.; Luz, M.T.; Minguito, T.; De La Fuente, J.; De Ory, F. The Application and Interpretation of IgG Avidity and IgA ELISA Tests to Characterize Zika Virus Infections. Viruses 2019, 11, 179. [Google Scholar] [CrossRef] [Green Version]
- Piccoli, L.; Park, Y.J.; Tortorici, M.A.; Czudnochowski, N.; Walls, A.C.; Beltramello, M.; Silacci-Fregni, C.; Pinto, D.; Rosen, L.E.; Bowen, J.E.; et al. Mapping Neutralizing and Immunodominant Sites on the SARS-CoV-2 Spike Receptor-Binding Domain by Structure-Guided High-Resolution Serology. Cell 2020, 183, 1024–1042.e21. [Google Scholar] [CrossRef]
- Moriyama, S.; Adachi, Y.; Sato, T.; Tonouchi, K.; Sun, L.; Fukushi, S.; Yamada, S.; Kinoshita, H.; Nojima, K.; Kanno, T.; et al. Temporal maturation of neutralizing antibodies in COVID-19 convalescent individuals improves potency and breadth to circulating SARS-CoV-2 variants. Immunity 2021, 54, 1841–1852.e4. [Google Scholar] [CrossRef]
- Barnes, C.O.; Jette, C.A.; Abernathy, M.E.; Dam, K.A.; Esswein, S.R.; Gristick, H.B.; Malyutin, A.G.; Sharaf, N.G.; Huey-Tubman, K.E.; Lee, Y.E.; et al. SARS-CoV-2 neutralizing antibody structures inform therapeutic strategies. Nature 2020, 588, 682–687. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, Function, and Antigenicity of the SARS-CoV-2 Spike Glycoprotein. Cell 2020, 181, 281–292.e6. [Google Scholar] [CrossRef] [PubMed]
- Khatri, I.; Staal, F.J.T.; van Dongen, J.J.M. Blocking of the High-Affinity Interaction-Synapse Between SARS-CoV-2 Spike and Human ACE2 Proteins Likely Requires Multiple High-Affinity Antibodies: An Immune Perspective. Front. Immunol. 2020, 11, 570018. [Google Scholar] [CrossRef] [PubMed]
- Benner, S.E.; Patel, E.U.; Laeyendecker, O.; Pekosz, A.; Littlefield, K.; Eby, Y.; Fernandez, R.E.; Miller, J.; Kirby, C.S.; Keruly, M.; et al. SARS-CoV-2 Antibody Avidity Responses in COVID-19 Patients and Convalescent Plasma Donors. J. Infect. Dis. 2020, 222, 1974–1984. [Google Scholar] [CrossRef] [PubMed]
- Bauer, G. The potential significance of high avidity immunoglobulin G (IgG) for protective immunity towards SARS-CoV-2. Int. J. Infect. Dis. 2021, 106, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Gaspar, E.B.; De Gaspari, E. Avidity assay to test functionality of anti-SARS-CoV-2 antibodies. Vaccine 2021, 39, 1473–1475. [Google Scholar] [CrossRef] [PubMed]
- Struck, F.; Schreiner, P.; Staschik, E.; Wochinz-Richter, K.; Schulz, S.; Soutschek, E.; Motz, M.; Bauer, G. Incomplete IgG avidity maturation after seasonal coronavirus infections. J. Med. Virol. 2021, 94, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Tsibin, A.N.; Latypova, M.F.; Strebkov, V.G.; Ivanushkina, O.I. Development and implementation of Single Reference Laboratory Testing Directory, as the basis for the digitalization of the laboratory service of Moscow. Probl. Soc. Hyg. Public Health Hist. Med. 2019, 27, 715–720. (In Russian) [Google Scholar] [CrossRef]
- Gushchin, V.A.; Dolzhikova, I.V.; Shchetinin, A.M.; Odintsova, A.S.; Siniavin, A.E.; Nikiforova, M.A.; Pochtovyi, A.A.; Shidlovskaya, E.V.; Kuznetsova, N.A.; Burgasova, O.A.; et al. Neutralizing Activity of Sera from Sputnik V-Vaccinated People against Variants of Concern (VOC: B.1.1.7, B.1.351, P.1, B.1.617.2, B.1.617.3) and Moscow Endemic SARS-CoV-2 Variants. Vaccines 2021, 9, 779. [Google Scholar] [CrossRef]
- Moura, A.D.; da Costa, H.H.M.; Correa, V.A.; de S. Lima, A.K.; Lindoso, J.A.L.; De Gaspari, E.; Hong, M.A.; Cunha-Junior, J.P.; Prudencio, C.R. Assessment of avidity related to IgG subclasses in SARS-CoV-2 Brazilian infected patients. Sci. Rep. 2021, 11, 17642. [Google Scholar] [CrossRef]
- Struck, F.; Schreiner, P.; Staschik, E.; Wochinz-Richter, K.; Schulz, S.; Soutschek, E.; Motz, M.; Bauer, G. Vaccination versus infection with SARS-CoV-2: Establishment of a high avidity IgG response versus incomplete avidity maturation. J. Med. Virol. 2021, 93, 6765–6777. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group | Outpatients (Mild Course) | Hospital (Severe Course) | ||
|---|---|---|---|---|
| Primarily Infected | Reinfected | Primarily Infected | Reinfected | |
| Number of patients | 39 | 36 | 82 | 10 |
| Median time passed between the first and second COVID-19 infections, days (CI 95%) | - | 213 (192–229) | - | 217 (191–386) |
| Median avidity index, % (CI 95%) | 37.14 (21.72–62.13) | 82.29 (72.1–91.1) | 24.99 (22.89–27.05) | 28.35 (16.63–43.52) |
| Median quantity of IgG to the RBD, PC (CI 95%) | 8.51 (5.3–11.7) | 7.93 (5.82–10.77) | >11.7 (10.45–11.7) | >11.7 (9.88–11.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manuylov, V.; Burgasova, O.; Borisova, O.; Smetanina, S.; Vasina, D.; Grigoriev, I.; Kudryashova, A.; Semashko, M.; Cherepovich, B.; Kharchenko, O.; et al. Avidity of IgG to SARS-CoV-2 RBD as a Prognostic Factor for the Severity of COVID-19 Reinfection. Viruses 2022, 14, 617. https://doi.org/10.3390/v14030617
Manuylov V, Burgasova O, Borisova O, Smetanina S, Vasina D, Grigoriev I, Kudryashova A, Semashko M, Cherepovich B, Kharchenko O, et al. Avidity of IgG to SARS-CoV-2 RBD as a Prognostic Factor for the Severity of COVID-19 Reinfection. Viruses. 2022; 14(3):617. https://doi.org/10.3390/v14030617
Chicago/Turabian StyleManuylov, Victor, Olga Burgasova, Olga Borisova, Svetlana Smetanina, Daria Vasina, Igor Grigoriev, Alexandra Kudryashova, Maria Semashko, Bogdan Cherepovich, Olga Kharchenko, and et al. 2022. "Avidity of IgG to SARS-CoV-2 RBD as a Prognostic Factor for the Severity of COVID-19 Reinfection" Viruses 14, no. 3: 617. https://doi.org/10.3390/v14030617