

Global Real-World Evidence of Sofosbuvir/Velpatasvir as a Highly Effective Treatment and Elimination Tool in People with Hepatitis C Infection Experiencing Mental Health Disorders
 , , , add
Show full author list
, , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Outcomes
2.3. Statistical Analyses
3. Results
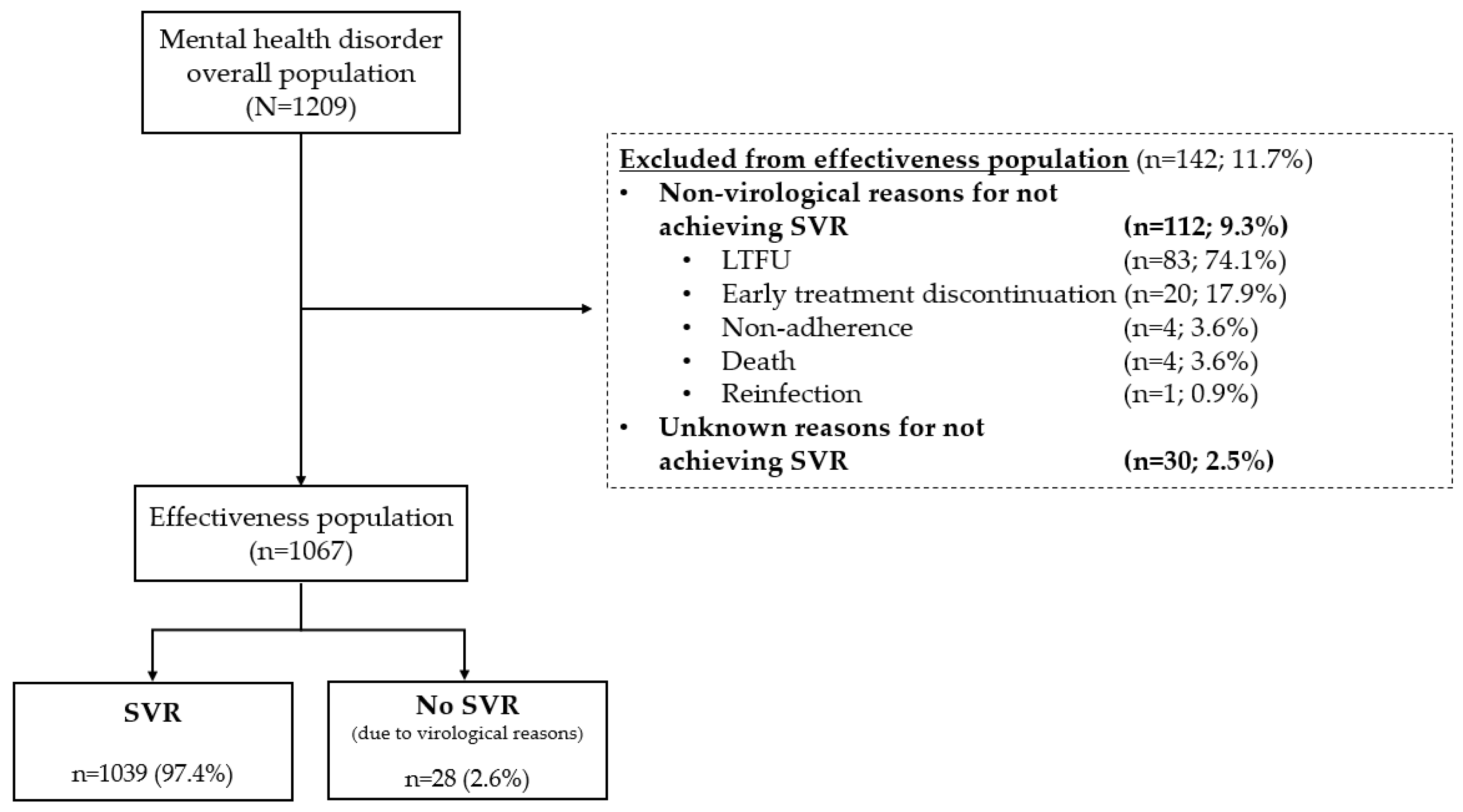
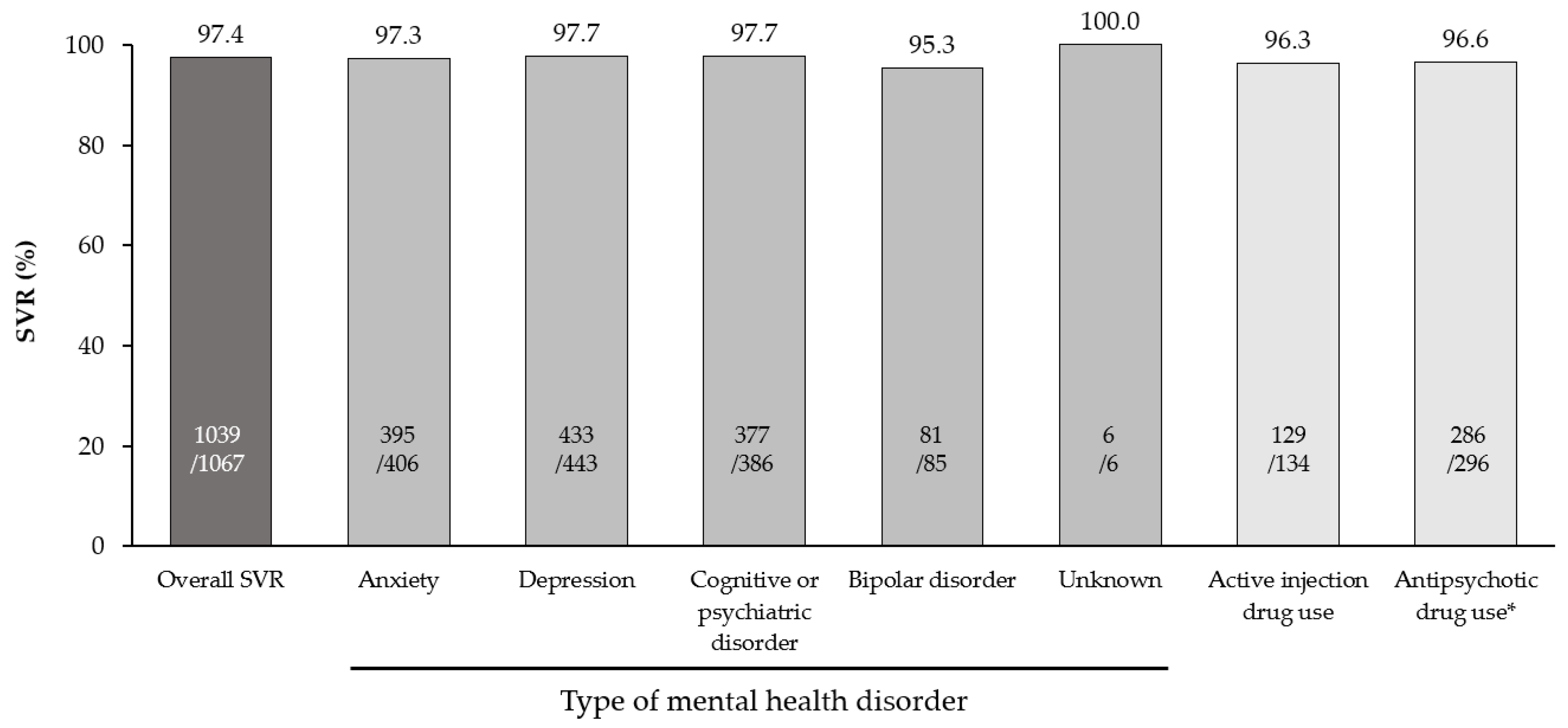
3.1. Effectiveness
3.2. Non-Virological and Unknown Reasons for Not Achieving SVR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021. Towards Ending Viral Hepatitis. 2016. Available online: https://apps.who.int/iris/bitstream/handle/10665/246177/WHO-HIV-2016.06-eng.pdf?sequence=1 (accessed on 9 November 2022).
- World Health Organization. Interim Guidance for Country Validation of Viral Hepatitis Elimination. June 2021. Available online: https://www.who.int/publications/i/item/9789240028395 (accessed on 9 November 2022).
- Blach, S.; Kondili, L.A.; Aghemo, A.; Cai, Z.; Dugan, E.; Estes, C.; Gamkrelidze, I.; Ma, S.; Pawlotsky, J.-M.; Razavi-Shearer, D.; et al. Impact of COVID-19 on global HCV elimination efforts. J. Hepatol. 2021, 74, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Pawlotsky, J.M.; Negro, F.; Aghemo, A.; Berenguer, M.; Dalgard, O.; Dusheiko, G.; Marra, F.; Puoti, M.; Wedemeyer, H.; European Association for the Study of the Liver. EASL recommendations on treatment of hepatitis C: Final update of the series. J. Hepatol. 2020, 73, 1170–1218. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, M.; Capuron, L.; Friebe, A.; Diez-Quevedo, C.; Robaeys, G.; Neri, S.; Foster, G.R.; Kautz, A.; Forton, D.; Pariante, C.M. Hepatitis C infection, antiviral treatment and mental health: A European expert consensus statement. J. Hepatol. 2012, 57, 1379–1390. [Google Scholar] [CrossRef]
- Williams, S.A.; Lindley, L.C. Characteristics of adults with hepatitis C virus: Evidence from the National Health and Nutrition Examination Survey 2011–2012. Gastroenterol. Nurs. 2020, 43, 363–374. [Google Scholar] [CrossRef]
- Hughes, E.; Bassi, S.; Gilbody, S.; Bland, M.; Martin, F. Prevalence of HIV, hepatitis B, and hepatitis C in people with severe mental illness: A systematic review and meta-analysis. Lancet Psychiatry 2016, 3, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Bauer-Staeb, C.; Jörgensen, L.; Lewis, G.; Dalman, C.; Osborn, D.P.J.; Hayes, J.F. Prevalence and risk factors for HIV, hepatitis B, and hepatitis C in people with severe mental illness: A total population study of Sweden. Lancet Psychiatry 2017, 4, 685–693. [Google Scholar] [CrossRef] [Green Version]
- Lluch, E.; Miller, B.J. Rates of hepatitis B and C in patients with schizophrenia: A meta-analysis. Gen. Hosp. Psychiatry 2019, 61, 41–46. [Google Scholar] [CrossRef]
- Braude, M.R.; Con, D.; Lubel, J.; Bidwai, A.; Nguyen, H.-T.; Sharmamiglani, S.; Clarke, D.; Dev, A.; Sievert, W. Liver disease prevalence and severity in people with serious mental illness: A cross-sectional analysis using non-invasive diagnostic tools. Hepatol. Int. 2021, 15, 812–820. [Google Scholar] [CrossRef]
- Sundberg, I.; Lannergård, A.; Ramklint, M.; Cunningham, J.L. Direct-acting antiviral treatment in real world patients with hepatitis C not associated with psychiatric side effects: A prospective observational study. BMC Psychiatry. 2018, 18, 157. [Google Scholar] [CrossRef] [Green Version]
- Ghany, M.G.; Morgan, T.R. AASLD-IDSA Hepatitis C Guidance Panel. Hepatitis C Guidance 2019 Update: American Association for the Study of Liver Diseases-Infectious Diseases Society of America Recommendations for Testing, Managing, and Treating Hepatitis C Virus Infection. Hepatology 2020, 71, 686–721. [Google Scholar] [CrossRef]
- Sackey, B.; Shults, J.G.; Moore, T.A.; Rogers, R.; Mehvar, M.; King, J.G. Evaluating psychiatric outcomes associated with direct-acting antiviral treatment in veterans with hepatitis C infection. Ment. Health Clin. 2018, 8, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Gallach, M.; Vergara, M.; da Costa, J.P.; Miquel, M.; Casas, M.; Sanchez-Delgado, J.; Dalmau, B.; Rudi, N.; Parra, I.; Monllor, T.; et al. Impact of treatment with direct-acting antivirals on anxiety and depression in chronic hepatitis C. PLoS ONE 2018, 13, e0208112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, M.K.; Thamer, M.; Therapondos, G.; Shiffman, M.L.; Kshirsagar, O.; Clark, C.; Wong, R.J. Has access to hepatitis C virus therapy changed for patients with mental health or substance use disorders in the direct-acting-antiviral period? Hepatology 2019, 69, 51–63. [Google Scholar] [CrossRef] [Green Version]
- Davidson, K.; Boyle, A.; Barclay, S.; Boxall, E.; Fleming, C.; Gossman, P.; McAvennie, J.; Reilly, E.; Sheridan, E.; Sommerville, A.; et al. The quetiapine question: Management strategies for drug-drug interactions with antipsychotics and direct acting antivirals; a multicentre review. In Proceedings of the Digital International Liver Congress, 27–29 August 2020. Poster #THU424. [Google Scholar]
- Sicras-Mainar, A.; Morillo-Verdugo, R. Concomitant use of direct-acting antivirals (DAA) and central nervous system drugs in patients with hepatitis C virus infection. Adicciones 2020, 34, 279–284. [Google Scholar] [CrossRef]
- Smolders, E.J.; de Kanter, C.T.M.M; de Knegt, R.J.; van der Valk, M.; Drenth, J.P.H.; Burger, D.M. Drug-drug interactions between direct-acting antivirals and psychoactive medications. Clin. Pharmacokinet. 2016, 55, 1471–1494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liverpool HEP Interactions. Available online: https://www.hep-druginteractions.org/checker (accessed on 9 November 2022).
- Feld, J.J.; Jacobson, I.M.; Hézode, C.; Asselah, T.; Ruane, P.J.; Gruener, N.; Abergel, A.; Mangia, A.; Lai, C.-L.; Chan, H.L.Y.; et al. Sofosbuvir and Velpatasvir for HCV Genotype 1, 2, 4, 5, and 6 Infection. N. Engl. J. Med. 2015, 373, 2599–2607. [Google Scholar] [CrossRef] [Green Version]
- Foster, G.R.; Afdhal, N.; Roberts, S.K.; Bräu, N.; Gane, E.J.; Pianko, S.; Lawitz, E.; Thompson, A.; Shiffman, M.L.; Cooper, C.; et al. Sofosbuvir and Velpatasvir for HCV Genotype 2 and 3 Infection. N. Engl. J. Med. 2015, 373, 2608–2617. [Google Scholar] [CrossRef] [Green Version]
- Curry, M.P.; O’Leary, J.G.; Bzowej, N.; Muir, A.J.; Korenblat, K.M.; Fenkel, J.M.; Reddy, K.R.; Lawitz, E.; Flamm, S.L.; Schiano, T.; et al. Sofosbuvir and Velpatasvir for HCV in Patients with Decompensated Cirrhosis. N. Engl. J. Med. 2015, 373, 2618–2628. [Google Scholar] [CrossRef]
- Wyles, D.; Bräu, N.; Kottilil, S.; Daar, E.S.; Ruane, P.; Workowski, K.; Luetkemeyer, A.; Adeyemi, O.; Kim, A.Y.; Doehle, B.; et al. Sofosbuvir and Velpatasvir for the Treatment of Hepatitis C Virus in Patients Coinfected With Human Immunodeficiency Virus Type 1: An Open-Label, Phase 3 Study. Clin. Infect. Dis. 2017, 65, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Mangia, A.; Milligan, S.; Khalili, M.; Fagiuoli, S.; Shafran, S.D.; Carrat, F.; Ouzan, D.; Papatheodoridis, G.; Ramji, A.; Borgia, S.M.; et al. Global real-world evidence of sofosbuvir/velpatasvir as simple, effective HCV treatment: Analysis of 5552 patients from 12 cohorts. Liver Int. 2020, 40, 1841–1852. [Google Scholar] [CrossRef]
- Cheng, P.-N.; Mo, L.-R.; Chen, C.-T.; Chen, C.-Y.; Huang, C.-F.; Kuo, H.-T.; Lo, C.-C.; Tseng, K.-C.; Huang, Y.-H.; Tai, C.-M.; et al. Sofosbuvir/Velpatasvir for Hepatitis C Virus Infection: Real-World Effectiveness and Safety from a Nationwide Registry in Taiwan. Infect. Dis. Ther. 2021, 11, 485–500. [Google Scholar] [CrossRef] [PubMed]
- Conway, B.; Rodriguez-Tajes, S.; Garcia-Retortillo, M.; Pérez-Hernandez, P.; Teti, E.; Ryan, P.; Fraser, C.; Macedo, G.; Amado, L.E.M.; de Lédinghen, V.; et al. Real-world evidence of sofosbuvir/velpatasvir as an effective and simple hepatitis C virus treatment and elimination tool in homeless populations. Future Virol. 2022, 17, 77–86. [Google Scholar] [CrossRef]
- Rosati, S.; Wong, A.; Di Marco, V.; Pérez-Hernandez, P.; Macedo, G.; Brixko, C.; Ranieri, R.; Campanale, F.; Basciá, A.; Fernández-Rodríguez, C.; et al. Real-world effectiveness of sofosbuvir/velpatasvir for the treatment of hepatitis C virus in prison settings. Future Virol. 2022, 17, 419–428. [Google Scholar] [CrossRef]
- Ifeachor, A.P.; Houck, K.K.; Schulte, S.; Ansara, E.; Johnson, A.J.; Carr, T.A.; Liangpunsakul, S. HCV eradication in veterans with underlying mental health disorders and substance use. J. Am. Pharm. Assoc. 2020, 60, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Darvishian, M.; Wong, S.; Binka, M.; Yu, A.; Ramji, A.; Yoshida, E.M.; Wong, J.; Rossi, C.; Butt, Z.A.; Bartlett, S.; et al. Loss to follow-up: A significant barrier in the treatment cascade with direct-acting therapies. J. Viral Hepat. 2020, 27, 243–260. [Google Scholar] [CrossRef] [PubMed]
- Christensen, S.; Buggisch, P.; Mauss, S.; Böker, K.H.W.; Schott, E.; Klinker, H.; Zimmermann, T.; Weber, B.; Reimer, J.; Serfert, Y.; et al. Direct-acting antiviral treatment of chronic HCV-infected patients on opioid substitution therapy: Still a concern in clinical practice? Addiction 2018, 113, 868–882. [Google Scholar] [CrossRef] [PubMed]
- Christensen, S.; Buggisch, P.; Mauss, S.; Böker, K.H.W.; Müller, T.; Klinker, H.; Zimmermann, T.; Serfert, Y.; Weber, B.; Reimer, J.; et al. Alcohol and Cannabis Consumption Does Not Diminish Cure Rates in a Real-World Cohort of Chronic Hepatitis C Virus Infected Patients on Opioid Substitution Therapy—Data From the German Hepatitis C-Registry (DHC-R). Subst. Abus. Res. Treat. 2019, 13, 1178221819835847. [Google Scholar] [CrossRef]
- Sulkowski, M.; Feld, J.; Reau, N.; Scherbakovsky, S.; Hernández, C.; Vanstraelen, K.; Hammond, K.; Kreter, B.; Suri, V.; Ni, L.; et al. Concordance between SVR4, SVR12, and SVR24 in HCV-infected patients who received fixed-dose combination sofosbuvir/velpatasvir in Phase 3 clinical trials. In Proceedings of the International Liver Congress, Virtual Event, 23–26 June 2021. Poster #983. [Google Scholar]
- Gane, E.; de Ledinghen, V.; Dylla, D.E.; Rizzardini, G.; Shiffman, M.L.; Barclay, S.T.; Calleja, J.L.; Xue, Z.; Burroughs, M.; Gutierrez, J.A. Positive predictive value of sustained virologic response 4 weeks posttreatment for achieving sustained virologic response 12 weeks posttreatment in patients receiving glecaprevir/pibrentasvir in Phase 2 and 3 clinical trials. J. Viral. Hepat. 2021, 28, 1635–1642. [Google Scholar] [CrossRef]
- Mangia, A.; Scaglione, F.; Toniutto, P.; Pirisi, M.; Coppola, N.; Di Perri, G.; Nieto, G.A.; Calabrese, S.; Hernandez, C.; Perrone, V.; et al. Drug–Drug Interactions in Italian Patients with Chronic Hepatitis C Treated with Pangenotypic Direct Acting Agents: Insights from a Real-World Study. Int. J. Environ. Res. Public Health 2021, 18, 7144. [Google Scholar] [CrossRef]
- Fagiouli, S.; Milligan, S.; Turnés, J.; Mangia, A.; Hintz, A.; Wick, N.; Sicras, A.; Esposti, LD.; Tacke, F.; Morillo, R.; et al. Multinational evaluation of comedication and drug–drug interactions in hepatitis C patients treated with pangenotypic direct-acting antivirals. In Proceedings of the Global Hepatitis Summit, Taipei, Taiwan, 18–20 June 2021. [Google Scholar]
- AASLD/EASL/APASL/ALEH. Call to Action for Liver Associations to Advance Progress Towards Viral Hepatitis Elimination: A Focus on Simplified Approaches to HCV Testing and Cure. 2019. Available online: https://www.aasld.org/call-action-advance-progress-towards-viral-hepatitis-elimination (accessed on 9 November 2022).
- Solomon, S.S.; Wagner-Cardoso, S.; Smeaton, L.; Sowah, L.A.; Wimbish, C.; Robbins, G.; Brates, I.; Scello, C.; Son, A.; Avihingsanon, A.; et al. A minimal monitoring approach for the treatment of hepatitis C virus infection (ACTG A5360 [MINMON]): A phase 4, open-label, single-arm trial. Lancet Gastroenterol. Hepatol. 2022, 7, 307–317. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Overall Population (N = 1209) | Effectiveness Population (n = 1067) |
|---|---|---|
| Age, years, mean (SD) * | 53.4 (13.4) | 54.2 (13.7) |
| Sex, male, n (%) | 730 (60.4) | 595 (55.8) |
| Fibrosis stage, n (%) | ||
| F0–F2 | 647 (53.5) | 559 (52.4) |
| F3 | 169 (14.0) | 151 (14.2) |
| F4 | 261 (21.6) | 202 (18.9) |
| Unknown | 132 (10.9) | 155 (14.5) |
| Treatment history, n (%) | ||
| Treatment-naïve | 1047 (86.6) | 920 (86.2) |
| Treatment-experienced (DAA-naïve) | 162 (13.4) | 147 (13.8) |
| HCV, n (%) | ||
| GT1 | 532 (44.0) | 482 (45.2) |
| GT2 | 199 (16.5) | 185 (17.3) |
| GT3 | 385 (31.8) | 319 (29.9) |
| GT4–6 | 69 (5.7) | 61 (5.7) |
| GT mixed/unknown | 24 (2.0) | 20 (1.9) |
| Injection drug use, former or current, n (%) | ||
| Yes | 545 (45.1) | 424 (39.7) |
| Active drug use, n (%) | 209 (17.3) | 134 (12.6) |
| No | 446 (36.9) | 386 (36.2) |
| Unknown | 218 (18.0) | 257 (24.1) |
| Type of mental health disorder †, n (%) | ||
| Anxiety | 467 (38.6) | 406 (38.1) |
| Depression | 505 (41.8) | 443 (41.5) |
| Bipolar disorder | 99 (8.2) | 85 (8.0) |
| Cognitive or psychiatric disorder | 440 (36.4) | 386 (36.2) |
| Unspecified ‡ | 7 (0.6) | 6 (0.6) |
| Number of specified mental health disorders § | ||
| 1 | 847 (70.1) | 764 (71.6) |
| 2 | 249 (20.6) | 207 (19.4) |
| 3 | 29 (2.4) | 25 (2.3) |
| Use of 1 or more antipsychotic drugs, n (%) | ||
| Yes | 357 (29.5) | 317 (29.7) |
| Quetiapine ‖ | 133 (11) | 116 (10.9) |
| Aripiprazole ‖ | 41 (3.4) | 34 (3.2) |
| Clozapine ‖ | 26 (2.2) | 22 (2.1) |
| Paliperidone ‖ | 27 (2.2) | 26 (2.4) |
| No | 653 (54.0) | 575 (53.9) |
| Unknown | 199 (16.5) | 175 (16.4) |
| Adherence ¶ | ||
| ≥90% | 512 (96.6) | 451 (97.8) |
| <90% | 18 (3.4) | 10 (2.2) |
| ≥80% | 519 (97.9) | 456 (98.9) |
| <80% | 11 (2.1) | 5 (1.1) |
| Time from HCV RNA diagnosis to SOF/VEL treatment start, mean (SD), days ** | 156 (607) | 152 (625) |
| Time from HCV RNA diagnosis to SOF/VEL treatment start, days, n (%) # | ||
| <1 | 30 (3.6) | 27 (3.6) |
| ≤7 | 54 (6.5) | 49 (6.4) |
| ≤30 | 195 (23.3) | 182 (23.9) |
| ≤90 | 510 (60.9) | 463 (60.9) |
| >90 | 327 (39.1) | 297 (39.1) |
| Unknown | 372 (30.8) | 307 (28.8) |
| Characteristics | Non-Virological Failures (n = 112) * | Patients LTFU (n = 83) † |
|---|---|---|
| Sex, male, n (%) | 69 (61.6) | 54 (65.1) |
| Fibrosis stage, n (%) | ||
| F0–F2 | 64 (57.1) | 54 (65.1) |
| F3 | 11 (9.8) | 8 (9.6) |
| F4 | 17 (15.2) | 9 (10.8) |
| Unknown | 20 (17.9) | 12 (14.5) |
| Treatment history, n (%) | ||
| Treatment-naïve | 93 (83.0) | 70 (84.3) |
| Treatment-experienced (DAA-naïve) | 7 (6.2) | 7 (8.4) |
| HCV, n (%) | ||
| GT1 | 41 (36.6) | 34 (41.0) |
| GT2 | 11 (9.8) | 6 (7.2) |
| GT3 | 45 (40.2) | 35 (42.2) |
| GT4–6 | 6 (5.4) | 5 (6.0) |
| GT mixed/unknown | 9 (8.0) | 3 (3.6) |
| Injection drug use, former or current, n (%) | ||
| Yes | 72 (64.3) | 63 (75.9) |
| Active drug use, n (%) | 43 (38.4) | 36 (43.4) |
| No | 9 (8.0) | 7 (8.4) |
| Unknown | 31 (27.7) | 13 (15.7) |
| Use of 1 or more antipsychotic drugs, n (%) | ||
| Yes | 28 (25.0) | 21 (25.3) |
| No | 48 (42.9) | 35 (42.2) |
| Unknown | 36 (32.1) | 27 (32.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wedemeyer, H.; Di Marco, V.; Garcia-Retortillo, M.; Teti, E.; Fraser, C.; Morano Amado, L.E.; Rodriguez-Tajes, S.; Acosta-López, S.; O’Loan, J.; Milella, M.; et al. Global Real-World Evidence of Sofosbuvir/Velpatasvir as a Highly Effective Treatment and Elimination Tool in People with Hepatitis C Infection Experiencing Mental Health Disorders. Viruses 2022, 14, 2493. https://doi.org/10.3390/v14112493
Wedemeyer H, Di Marco V, Garcia-Retortillo M, Teti E, Fraser C, Morano Amado LE, Rodriguez-Tajes S, Acosta-López S, O’Loan J, Milella M, et al. Global Real-World Evidence of Sofosbuvir/Velpatasvir as a Highly Effective Treatment and Elimination Tool in People with Hepatitis C Infection Experiencing Mental Health Disorders. Viruses. 2022; 14(11):2493. https://doi.org/10.3390/v14112493
Chicago/Turabian StyleWedemeyer, Heiner, Vito Di Marco, Montserrat Garcia-Retortillo, Elisabetta Teti, Chris Fraser, Luis Enrique Morano Amado, Sergio Rodriguez-Tajes, Silvia Acosta-López, Joss O’Loan, Michele Milella, and et al. 2022. "Global Real-World Evidence of Sofosbuvir/Velpatasvir as a Highly Effective Treatment and Elimination Tool in People with Hepatitis C Infection Experiencing Mental Health Disorders" Viruses 14, no. 11: 2493. https://doi.org/10.3390/v14112493