
Comparison and Harmonization of Different Semi-Automated and Automated qRT-PCR Assays in the Assessment of SARS-CoV-2
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
2.2. Sample Pool for Imprecision Measurements
2.3. Samples for Standardization
2.4. Viral RNA Extraction
2.5. Semi-Automated Systems
2.5.1. Genesig® (Primerdesign Ltd., Chandler’s Ford, UK)
2.5.2. RIDA®GENE (R-Biopharm AG, Darmstadt, Germany)
2.6. Fully Automated Systems
2.6.1. Alinity m (Abbott Molecular Inc., Illinois, IL, USA)
2.6.2. Cobas® 6800 (Roche Molecular Systems Inc., New Jersey, NJ, USA)
2.6.3. GeneXpert (Cepheid, California, CA, USA)
2.7. Statistical Analysis
3. Results
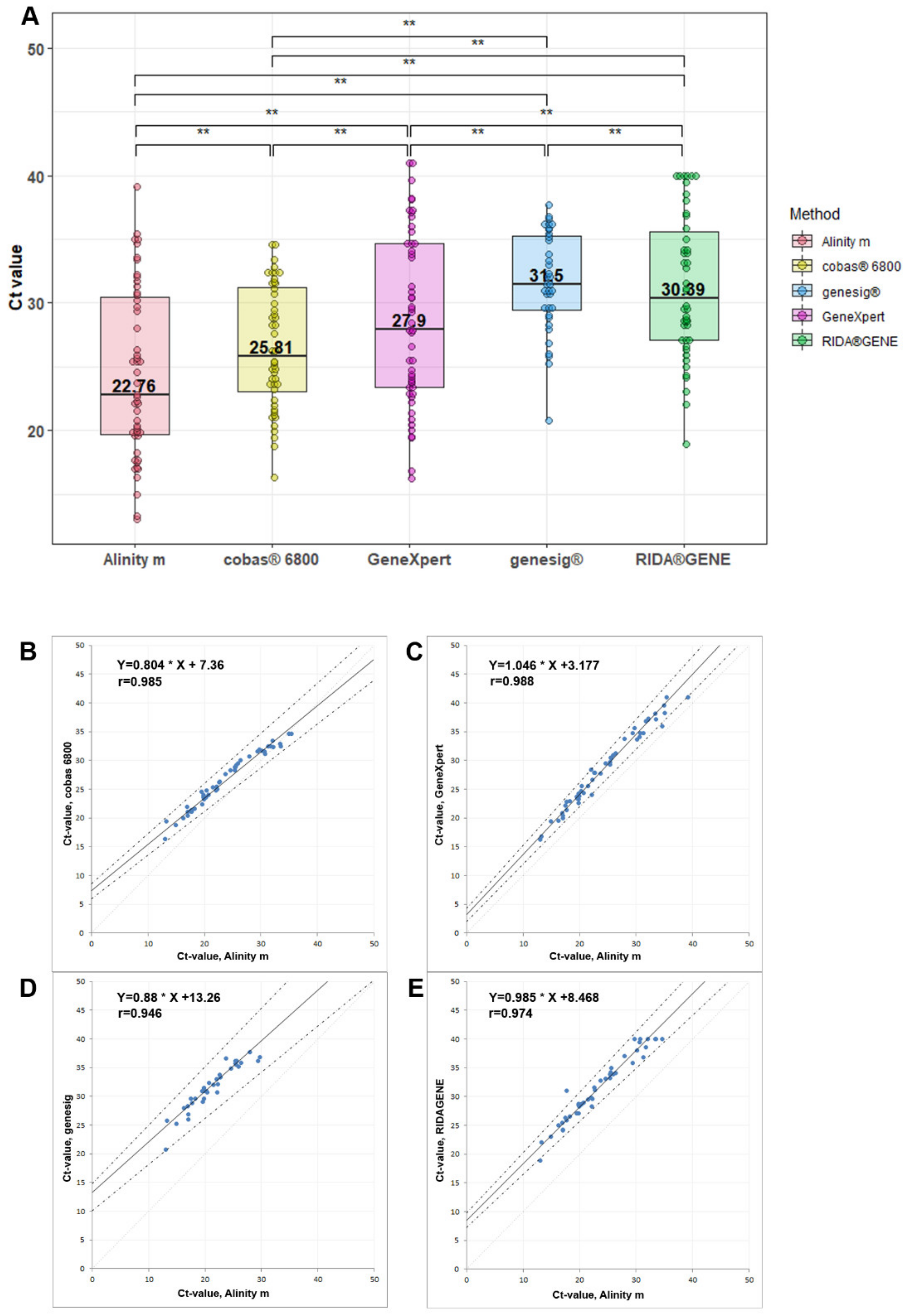
3.1. Comparability between Different Methods
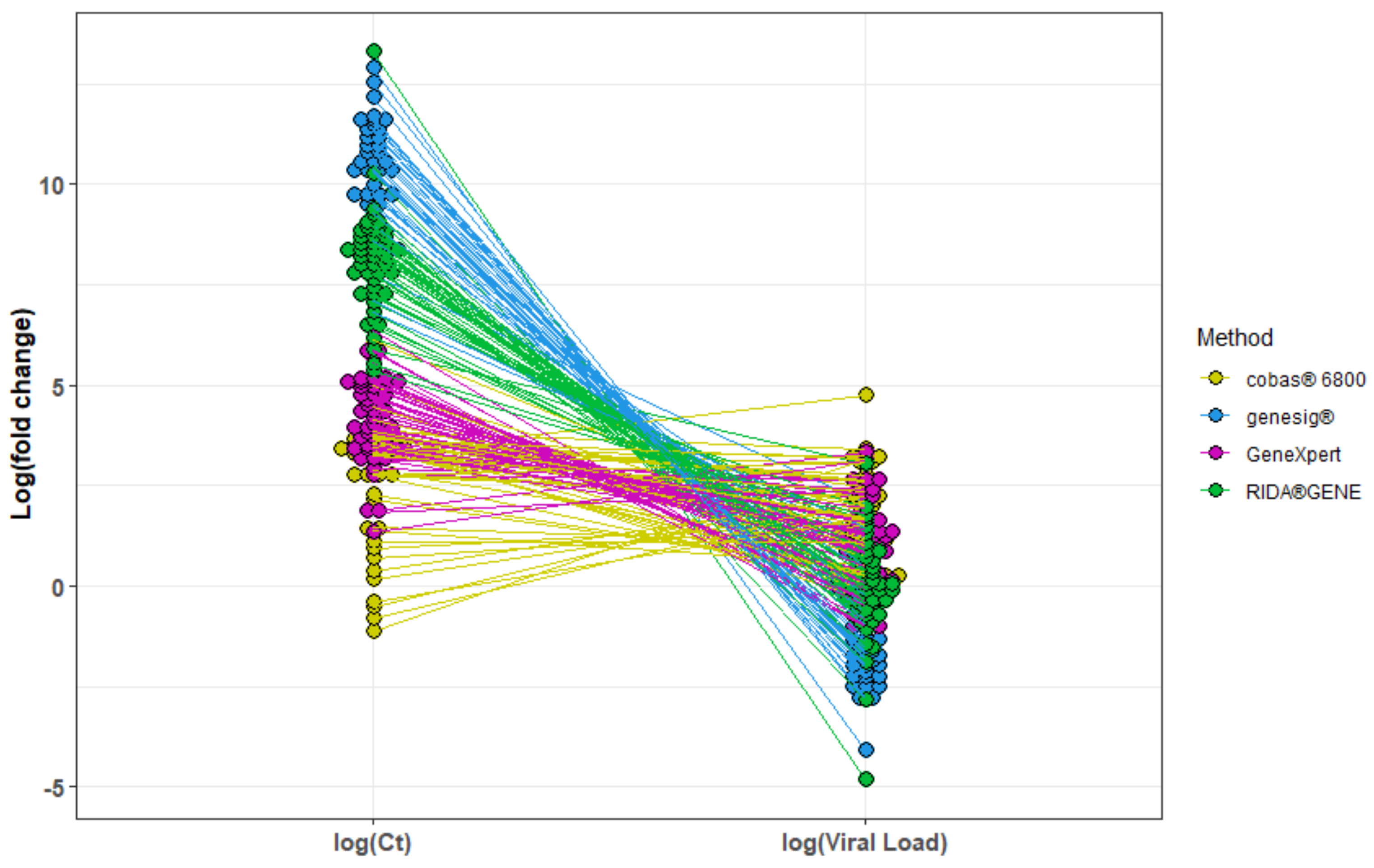
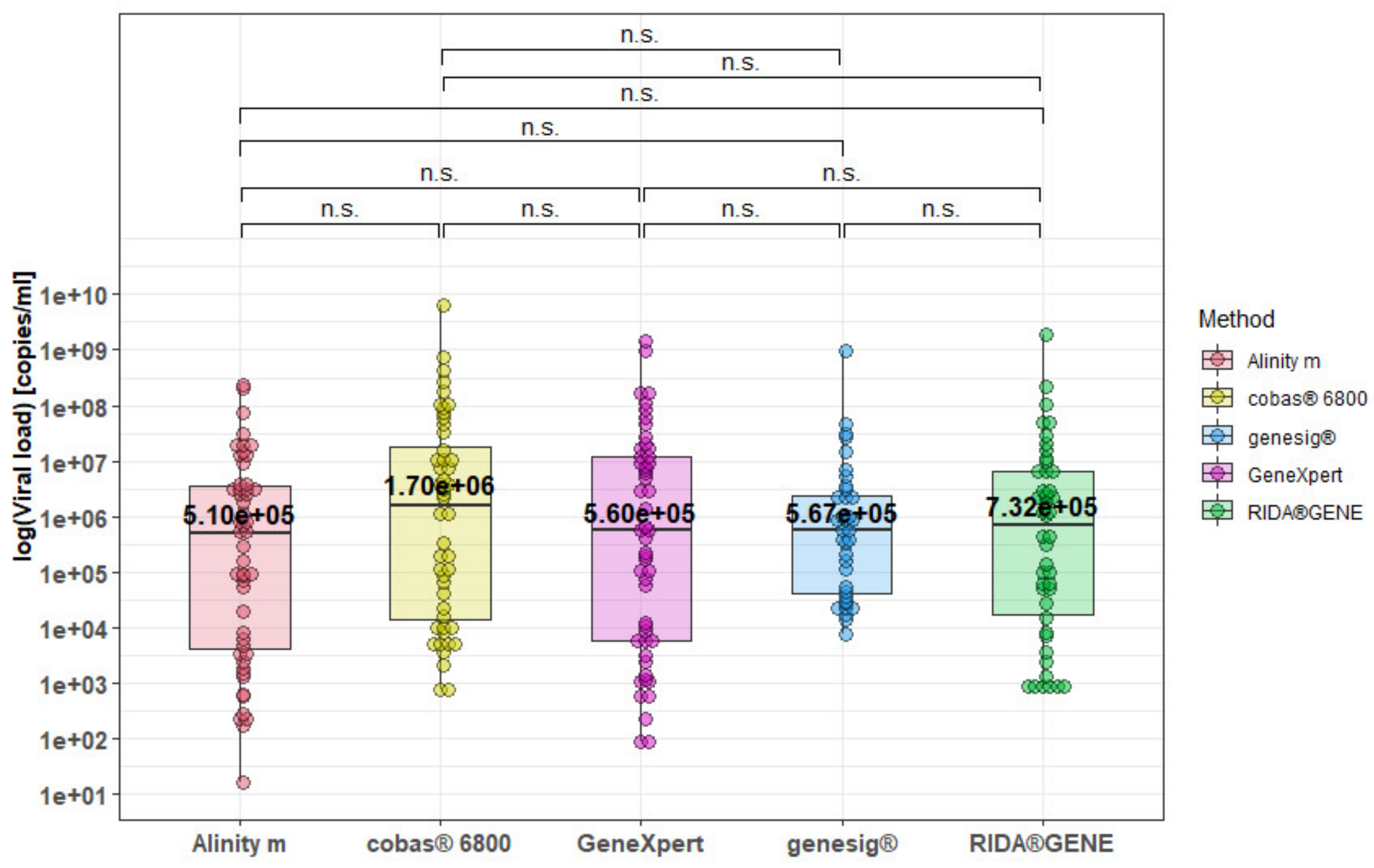
3.2. Harmonization of Different SARS-CoV-2 qRT-PCR Assays
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bentley, E.; Mee, E.T.; Routley, S.; Mate, R.; Fritzsche, M.; Hurley, M.; Le Duff, Y.; Anderson, R.; Hockley, J.; Rigsby, P.; et al. Collaborative Study for the Establishment of a WHO International Standard for SARS-CoV-2 RNA; WHO Expert Committee on Biological Standardization: Geneva, Switzerland, 2020. [Google Scholar]
- Vierbaum, L.; Wojtalewicz, N.; Grunert, H.-P.; Lindig, V.; Duehring, U.; Drosten, C.; Corman, V.; Niemeyer, D.; Ciesek, S.; Rabenau, H.F.; et al. RNA reference materials with defined viral RNA loads of SARS-CoV-2-A useful tool towards a better PCR assay harmonization. PLoS ONE 2022, 17, e0262656. [Google Scholar] [CrossRef]
- Stang, A.; Robers, J.; Schonert, B.; Jöckel, K.-H.; Spelsberg, A.; Keil, U.; Cullen, P. The performance of the SARS-CoV-2 RT-PCR test as a tool for detecting SARS-CoV-2 infection in the population. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef]
- Buchta, C.; Görzer, I.; Chiba, P.; Camp, J.V.; Holzmann, H.; Puchhammer-Stöckl, E.; Mayerhofer, M.; Müller, M.M.; Aberle, S.W. Variability of cycle threshold values in an external quality assessment scheme for detection of the SARS-CoV-2 virus genome by RT-PCR. Clin. Chem. Lab. Med. 2021, 59, 987–994. [Google Scholar] [CrossRef]
- Robert Koch Institute. Empfehlungen zu Isolierung und Quarantäne bei SARS-CoV-2-Infektion und -Exposition, Stand 2.5.2022. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Quarantaene/Absonderung.html (accessed on 17 August 2022).
- Mowrer, C.T.; Creager, H.; Cawcutt, K.; Birge, J.; Lyden, E.; van Schooneveld, T.C.; Rupp, M.E.; Hewlett, A. Evaluation of cycle threshold values at deisolation. Infect. Control Hosp. Epidemiol. 2022, 43, 794–796. [Google Scholar] [CrossRef]
- Engelmann, I.; Alidjinou, E.K.; Ogiez, J.; Pagneux, Q.; Miloudi, S.; Benhalima, I.; Ouafi, M.; Sane, F.; Hober, D.; Roussel, A.; et al. Preanalytical Issues and Cycle Threshold Values in SARS-CoV-2 Real-Time RT-PCR Testing: Should Test Results Include These? ACS Omega 2021, 6, 6528–6536. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Tirupathi, R.; Sule, A.A.; Aldali, J.; Mutair, A.A.; Alhumaid, S.; Muzaheed; Gupta, N.; Koritala, T.; Adhikari, R.; et al. Viral Dynamics and Real-Time RT-PCR Ct Values Correlation with Disease Severity in COVID-19. Diagnostics 2021, 11, 1091. [Google Scholar] [CrossRef] [PubMed]
- Wickham, H. ggplot2: Elegant Graphics for Data Analysis; Springer: New York, NY, USA, 2016; ISBN 978-3-319-24277-4. Available online: https://ggplot2.tidyverse.org (accessed on 28 August 2022).
- RStudio Team. RStudio: Integrated Development for R; RStudio, PBC: Boston, MA, USA, 2020; Available online: http://www.rstudio.com/ (accessed on 8 August 2022).
- Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Rahbari, R.; Moradi, N.; Abdi, M. rRT-PCR for SARS-CoV-2: Analytical considerations. Clin. Chim. Acta 2021, 516, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vandenberg, O.; Martiny, D.; Rochas, O.; van Belkum, A.; Kozlakidis, Z. Considerations for diagnostic COVID-19 tests. Nat. Rev. Microbiol. 2021, 19, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Kogoj, R.; Kmetič, P.; Oštrbenk Valenčak, A.; Fujs Komloš, K.; Seme, K.; Sagadin, M.; Korva, M.; Poljak, M. Real-Life Head-to-Head Comparison of Performance of Two High-Throughput Automated Assays for the Detection of SARS-CoV-2 RNA in Nasopharyngeal Swabs: The Alinity m and cobas 6800 SARS-CoV-2 Assays. J. Mol. Diagn. 2021, 23, 920–928. [Google Scholar] [CrossRef] [PubMed]
- Perchetti, G.A.; Pepper, G.; Shrestha, L.; LaTurner, K.; Yae Kim, D.; Huang, M.-L.; Jerome, K.R.; Greninger, A.L. Performance characteristics of the Abbott Alinity m SARS-CoV-2 assay. J. Clin. Virol. 2021, 140, 104869. [Google Scholar] [CrossRef]
- Malecki, M.; Luesebrink, J.; Wendel, A.F.; Mattner, F. Analysis of external quality assessment samples revealed crucial performance differences between commercial RT-PCR assays for SARS-CoV-2 detection when taking extraction methods and real-time-PCR instruments into account. J. Virol. Methods 2021, 295, 114202. [Google Scholar] [CrossRef] [PubMed]
- Matheeussen, V.; Corman, V.M.; Donoso Mantke, O.; McCulloch, E.; Lammens, C.; Goossens, H.; Niemeyer, D.; Wallace, P.S.; Klapper, P.; Niesters, H.G.; et al. International external quality assessment for SARS-CoV-2 molecular detection and survey on clinical laboratory preparedness during the COVID-19 pandemic, April/May 2020. Eurosurveillance 2020, 25, 2001223. [Google Scholar] [CrossRef] [PubMed]
- La Scola, B.; Le Bideau, M.; Andreani, J.; van Hoang, T.; Grimaldier, C.; Colson, P.; Gautret, P.; Raoult, D. Viral RNA load as determined by cell culture as a management tool for discharge of SARS-CoV-2 patients from infectious disease wards. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 39, 1059–1061. [Google Scholar] [CrossRef] [PubMed]
- Platten, M.; Hoffmann, D.; Grosser, R.; Wisplinghoff, F.; Wisplinghoff, H.; Wiesmüller, G.; Schildgen, O.; Schildgen, V. SARS-CoV-2, CT-Values, and Infectivity-Conclusions to Be Drawn from Side Observations. Viruses 2021, 13, 1459. [Google Scholar] [CrossRef] [PubMed]
- Matsuyama, S.; Nao, N.; Shirato, K.; Kawase, M.; Saito, S.; Takayama, I.; Nagata, N.; Sekizuka, T.; Katoh, H.; Kato, F.; et al. Enhanced isolation of SARS-CoV-2 by TMPRSS2-expressing cells. Proc. Natl. Acad. Sci. USA 2020, 117, 7001–7003. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cobas® 6800 | GeneXpert | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | Total | OA | Positive | Negative | Total | OA | ||
| Alinity m | Positive | 50 | 1 | 51 | 98.04% | 51 | 0 | 51 | 100.00% |
| Negative | 0 | 34 | 34 | κ = 0.98 | 0 | 34 | 34 | κ = 1.00 | |
| Total | 50 | 35 | 85 | 51 | 34 | 85 | |||
| genesig® | RIDA®GENE | ||||||||
| Positive | Negative | Total | OA | Positive | Negative | Total | OA | ||
| Alinity m | Positive | 36 | 15 | 51 | 70.59% | 46 | 5 | 51 | 90.20% |
| Negative | 0 | 34 | 34 | κ = 0.66 | 0 | 34 | 34 | κ = 0.88 | |
| Total | 36 | 49 | 85 | 46 | 39 | 85 | |||
| Alinity m | Cobas® 6800 | GeneXpert | Genesig® | RIDA®GENE | ||
|---|---|---|---|---|---|---|
| Mean Ct | 15.67 | 18.69 | 20.03 | 25.47 | 23.99 | |
| Imprecision: | Within Run | 0.30 | 0.08 | 0.65 | 0.21 | 0.14 |
| Total | 0.35 (%CV = 2.2) | 0.13 (%CV = 0.7) | 0.64 (%CV = 3.2) | 1.68 (%CV = 6.6) | 1.40 (%CV = 5.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dierks, S.; Thiele, K.; Bohne, W.; Lugert, R.; Weig, M.; Groß, U.; von Ahsen, N.; Schanz, J.; Fischer, A.; Schnelle, M. Comparison and Harmonization of Different Semi-Automated and Automated qRT-PCR Assays in the Assessment of SARS-CoV-2. Viruses 2022, 14, 2239. https://doi.org/10.3390/v14102239
Dierks S, Thiele K, Bohne W, Lugert R, Weig M, Groß U, von Ahsen N, Schanz J, Fischer A, Schnelle M. Comparison and Harmonization of Different Semi-Automated and Automated qRT-PCR Assays in the Assessment of SARS-CoV-2. Viruses. 2022; 14(10):2239. https://doi.org/10.3390/v14102239
Chicago/Turabian StyleDierks, Sascha, Karin Thiele, Wolfgang Bohne, Raimond Lugert, Michael Weig, Uwe Groß, Nicolas von Ahsen, Julie Schanz, Andreas Fischer, and Moritz Schnelle. 2022. "Comparison and Harmonization of Different Semi-Automated and Automated qRT-PCR Assays in the Assessment of SARS-CoV-2" Viruses 14, no. 10: 2239. https://doi.org/10.3390/v14102239