
Model-Based Analysis of SARS-CoV-2 Infections, Hospitalization and Outcome in Germany, the Federal States and Districts
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Epidemiological Data
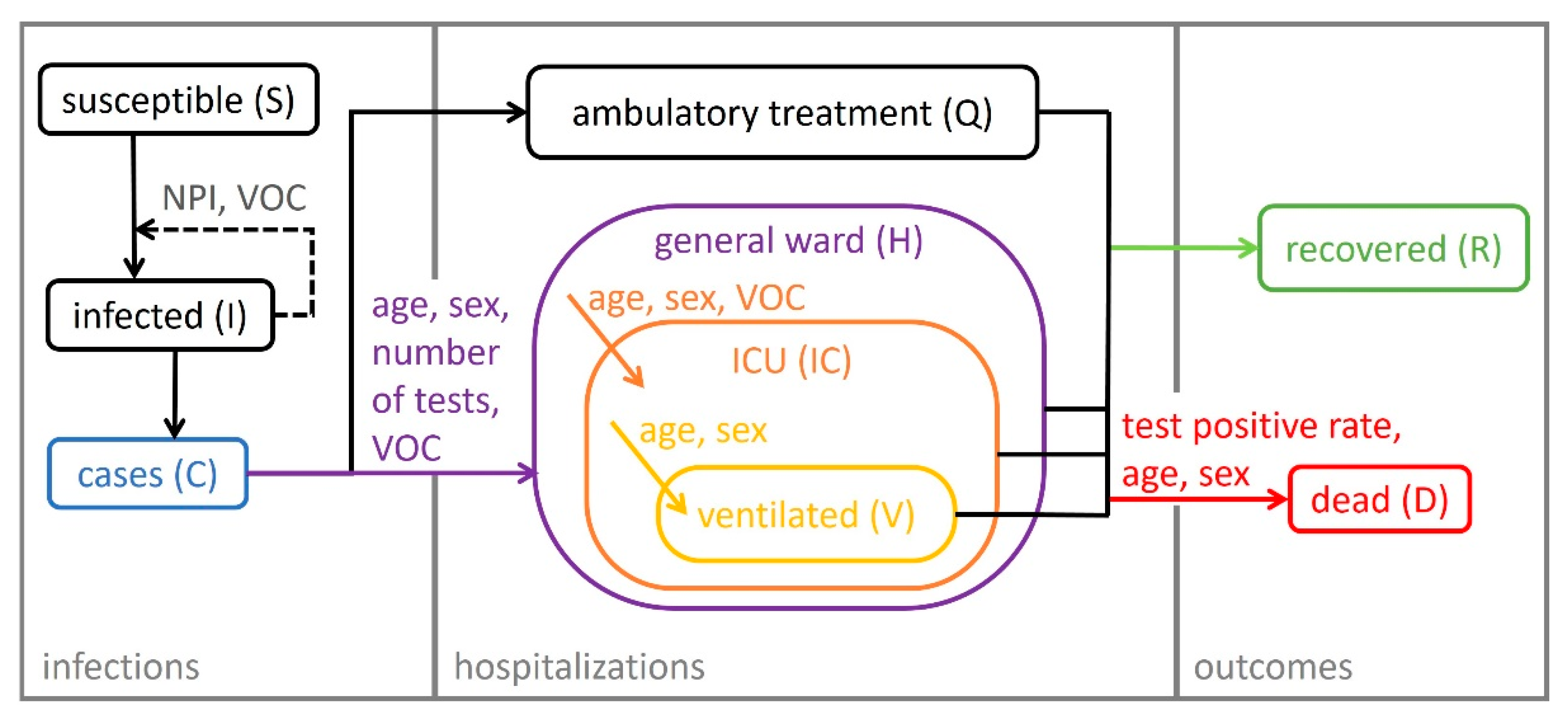
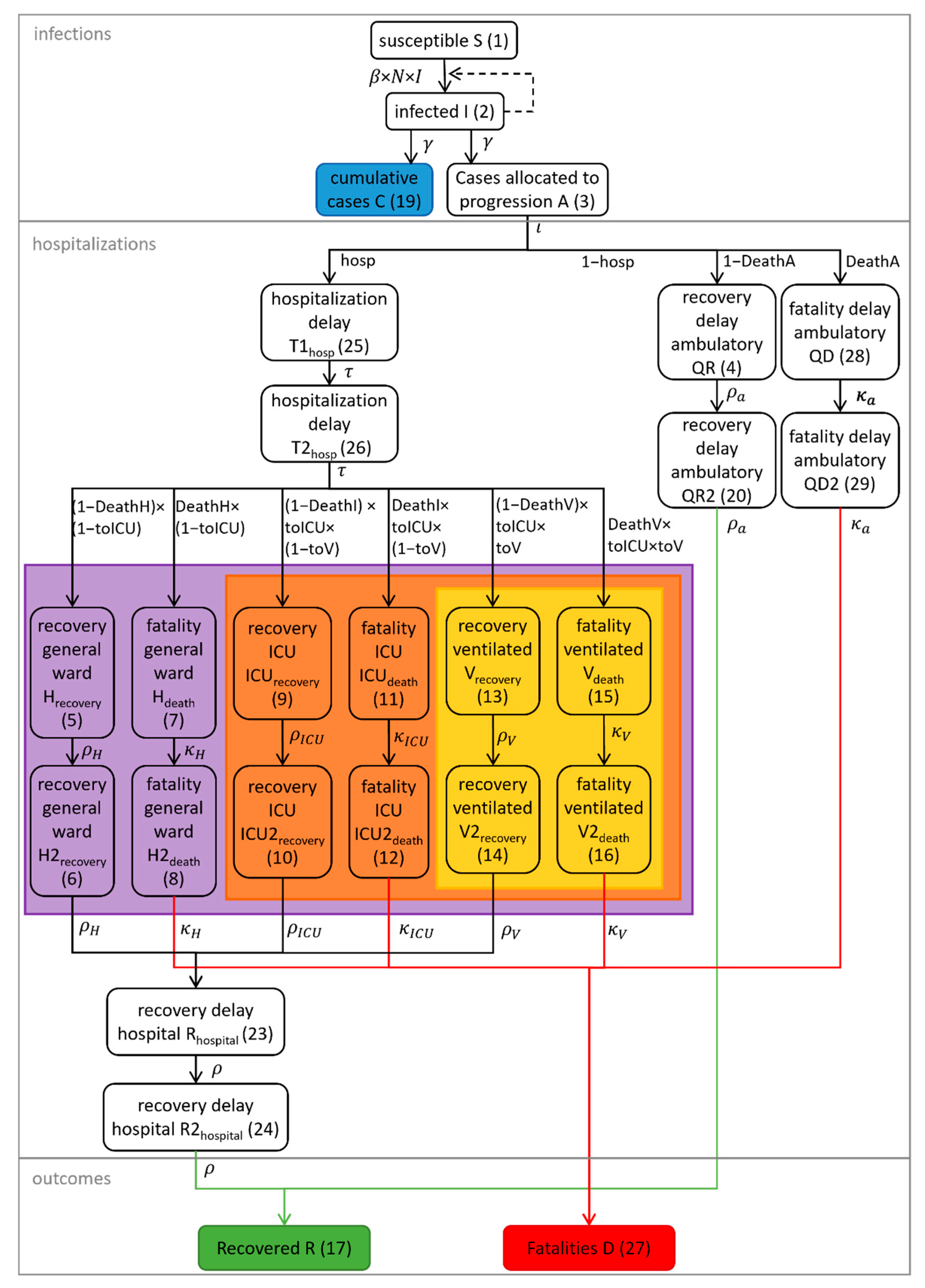
2.2. Model Development
2.3. Infections
2.4. Hospitalization and Outcome of COVID-19 Patients in Germany
2.5. Model Parametrization and Mixed-Effects Modeling
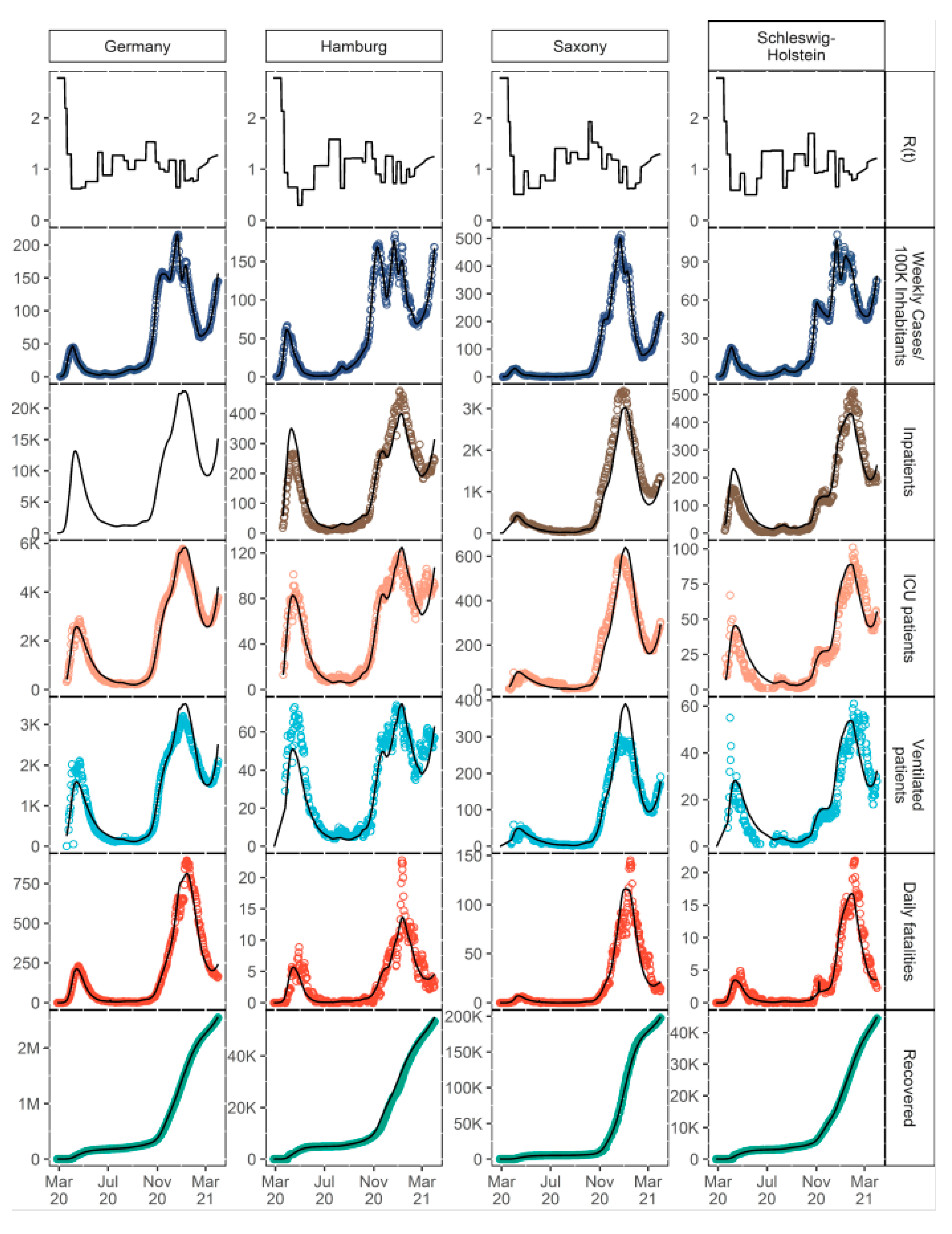
3. Results
3.1. Clinical Database
3.2. Model Structure
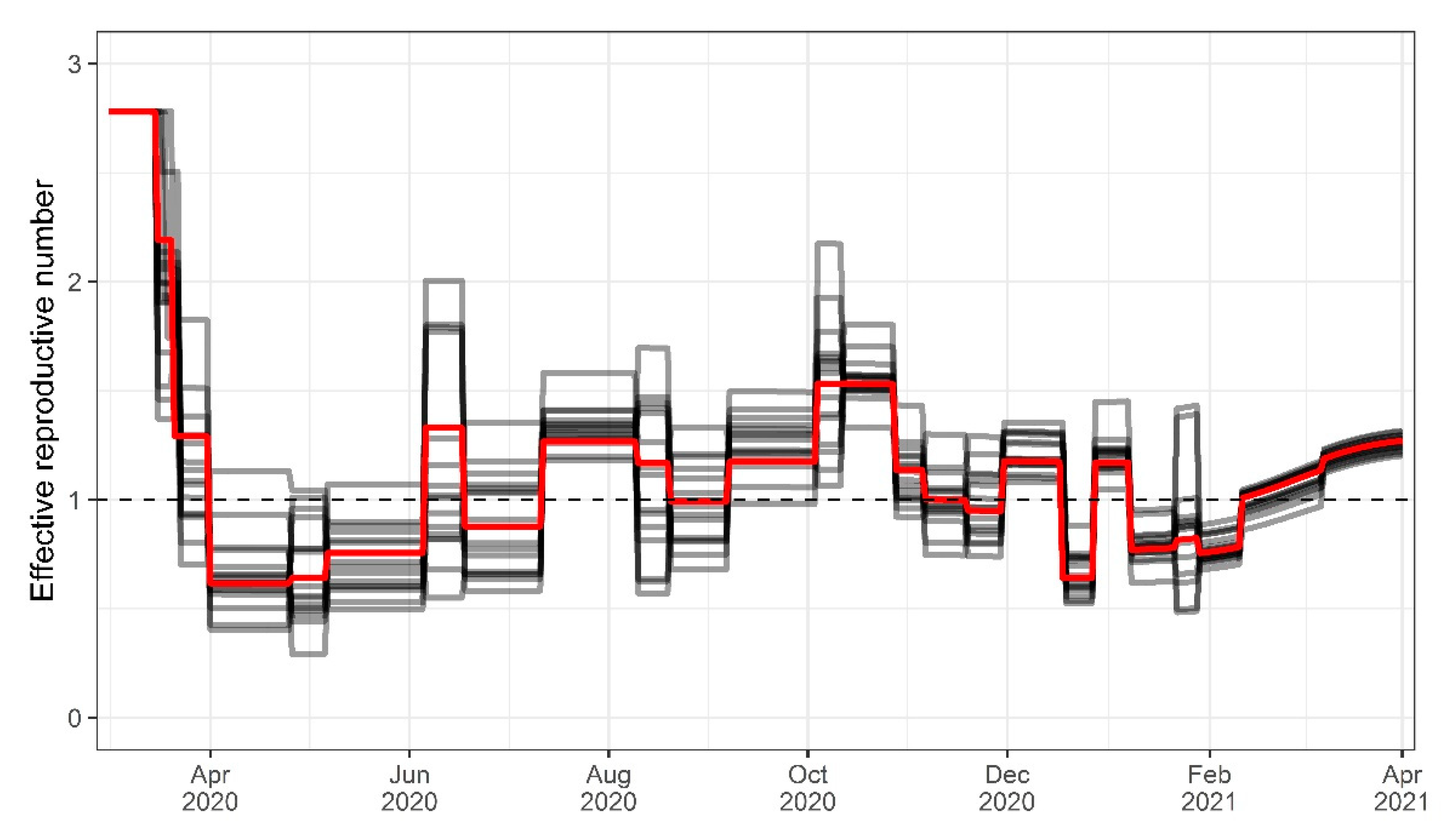
3.3. Infectiousness
3.4. Hospitalization and Outcome of COVID-19 Patients in Germany
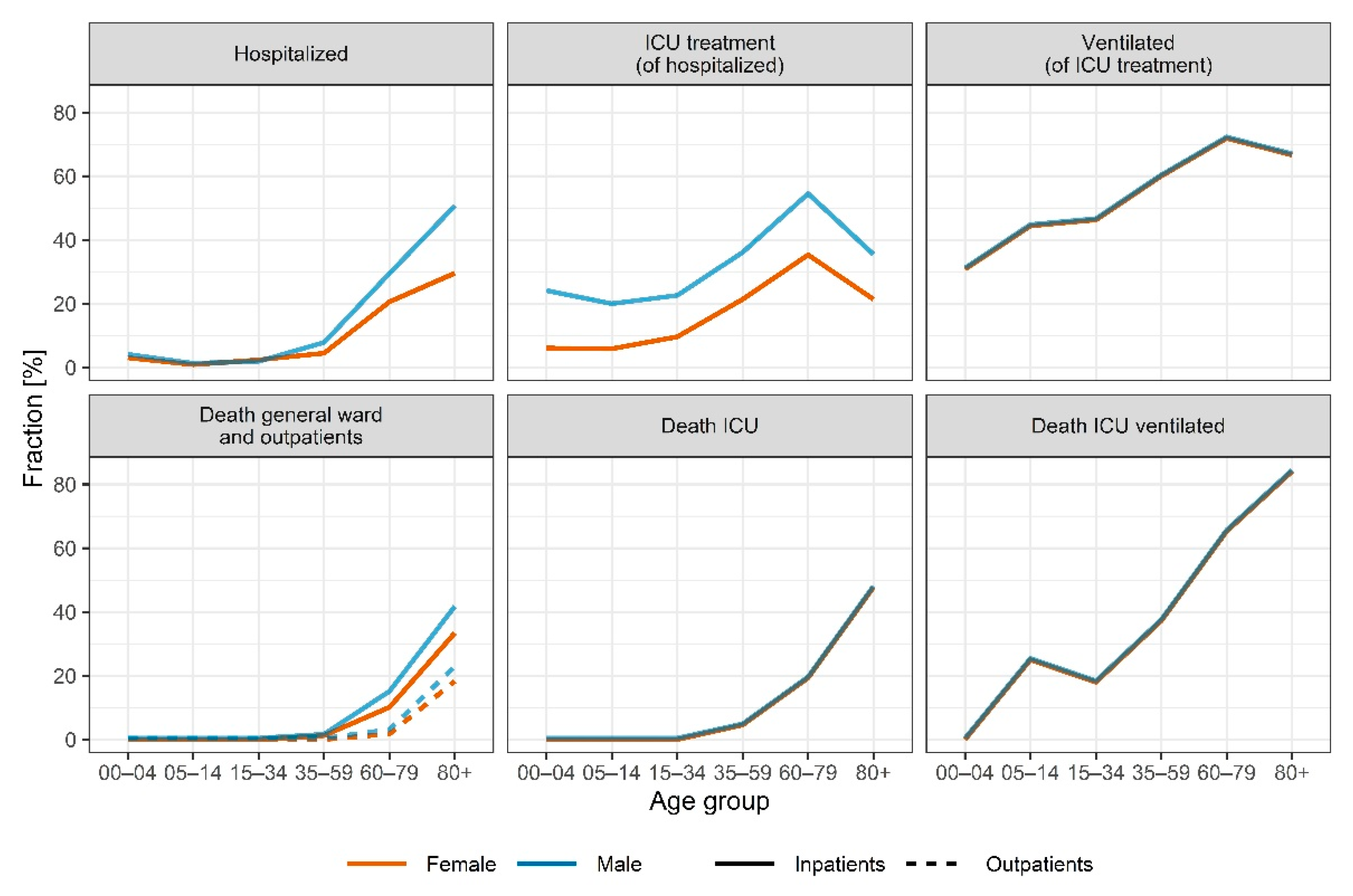
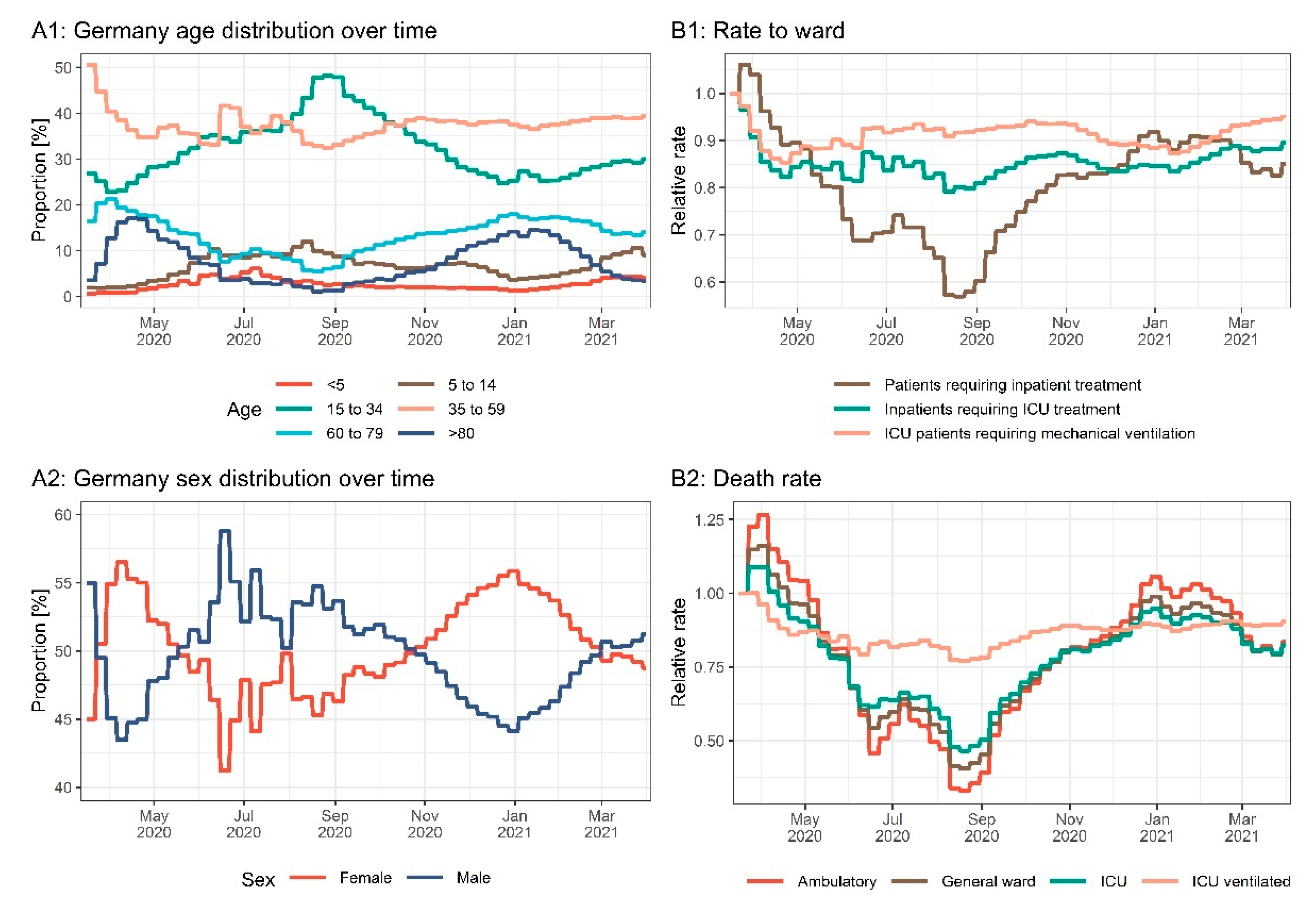
3.5. Age and Sex
3.6. Variants of Concern
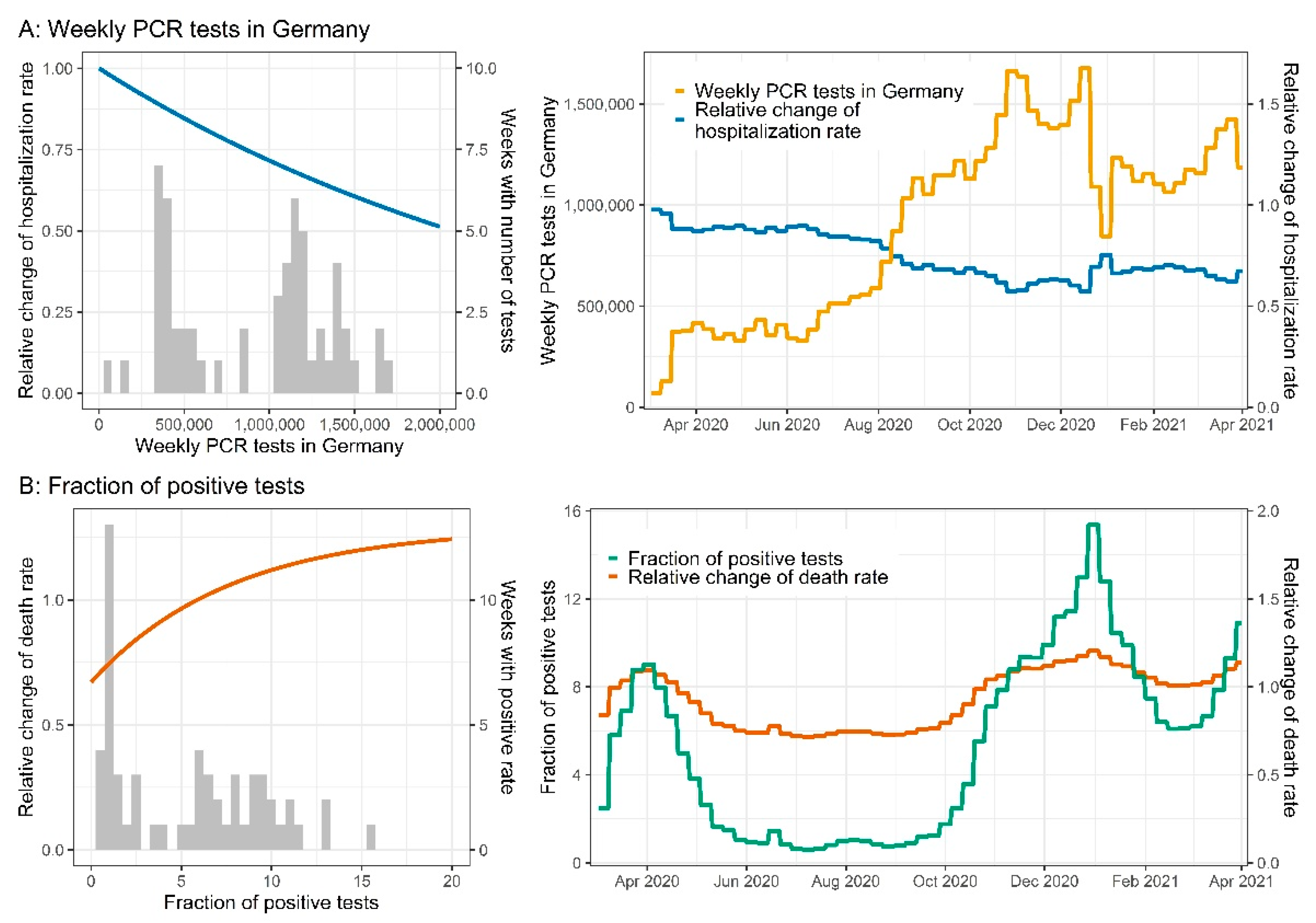
3.7. Testing Strategy
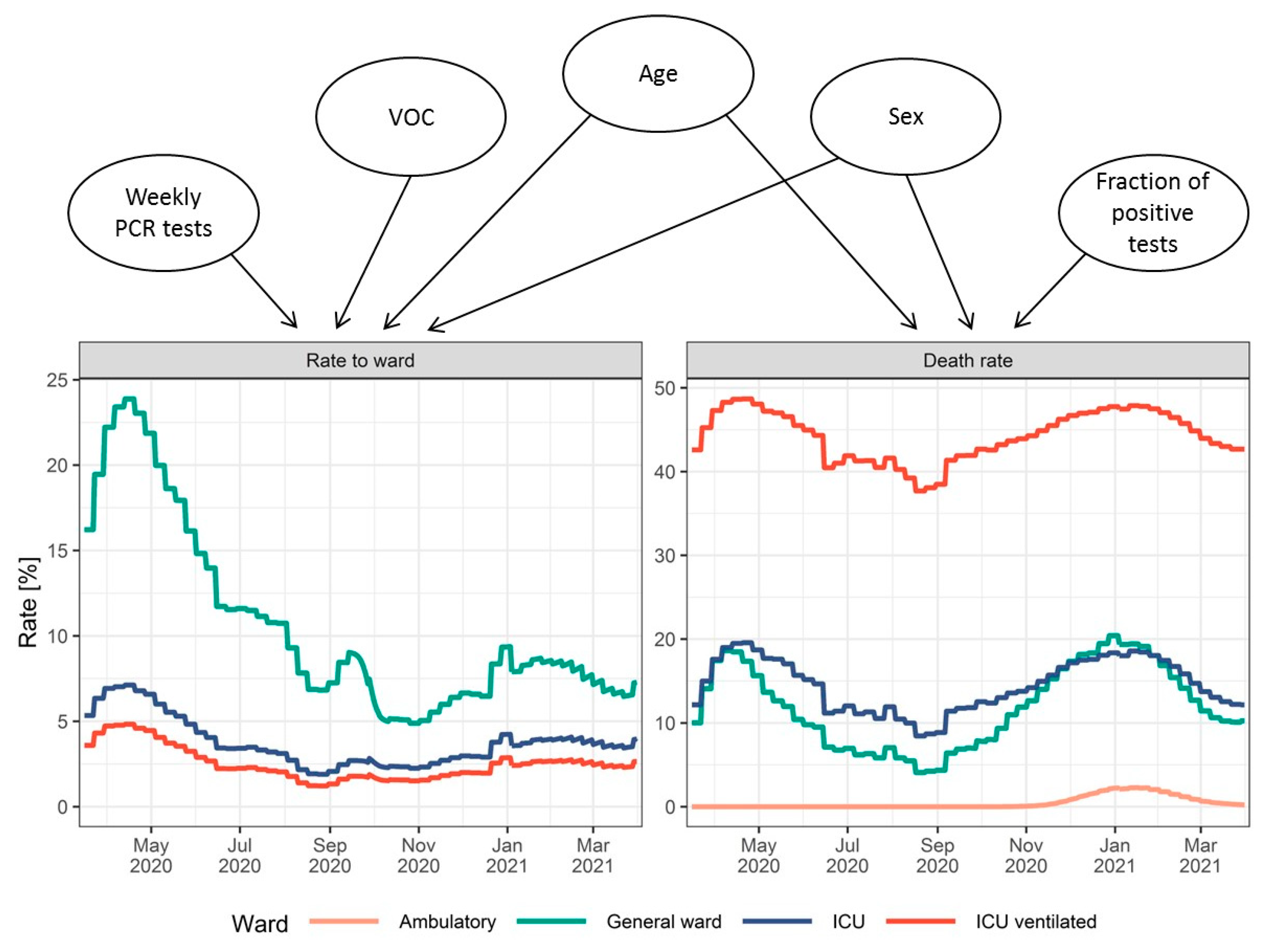
3.8. Hospitalization Rates and Time Effects
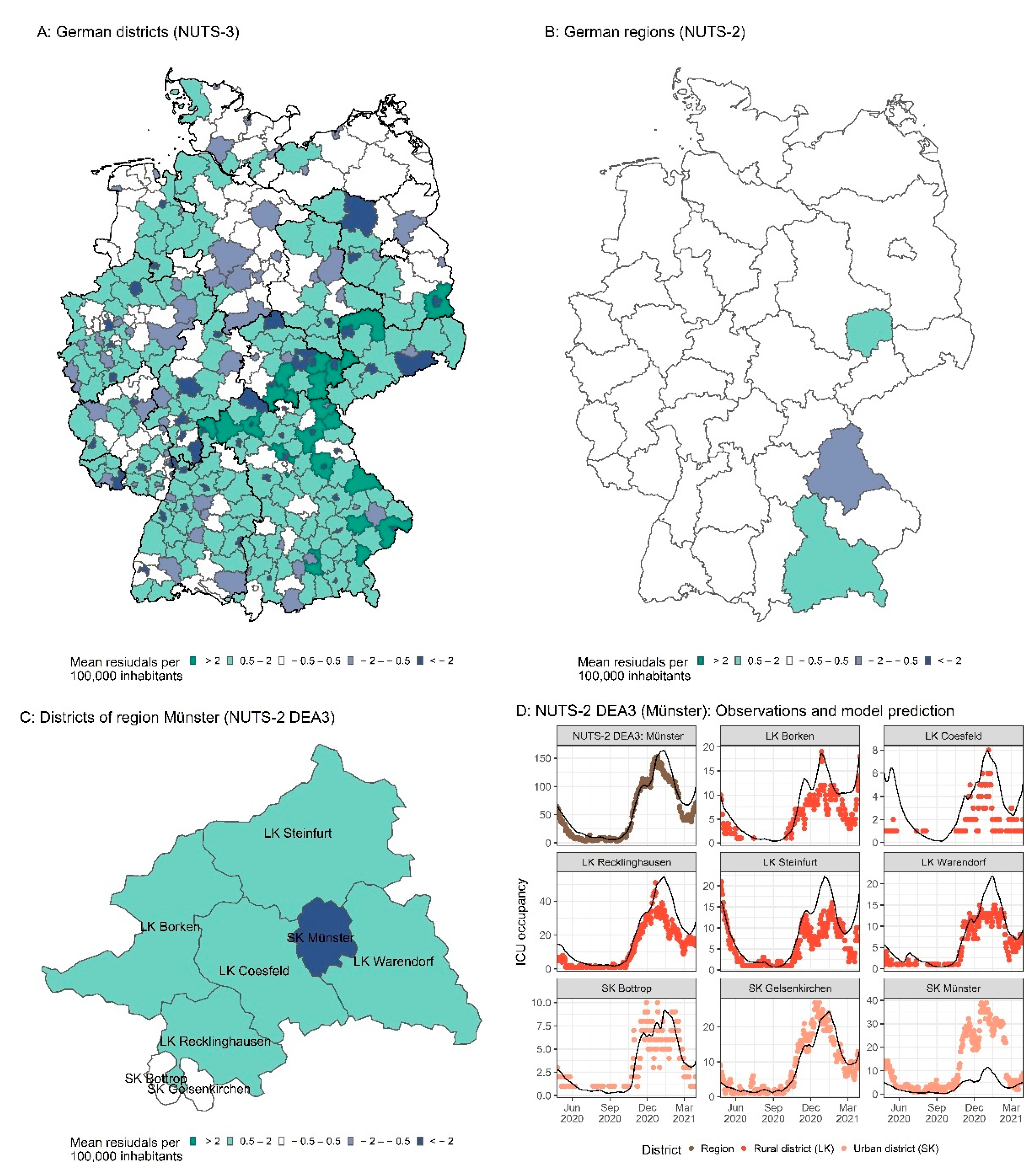
3.9. German Districts
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model Parameter | Unit | Population Estimate | RSE [%] | Parameter Description |
|---|---|---|---|---|
| Population Parameters (Fixed Effects) | ||||
| - | 0.99 | - | Factor on the age-specific hospitalization rates | |
| - | −0.496 | 1.6 | Relative change in hospitalization rate at | |
| Day * | 281 | 0.2 | Time of hospitalization rate change | |
| - | 100 | - | Hill factor of time-dependent hospitalization and ICU rate change | |
| 106/Tests | 0.344 | 3.7 | Slope of death rate change per 1,000,000 PCR tests performed | |
| - | 1.69 | 0.9 | Factor time to discharge of recovering ventilated patients | |
| - | −0.648 | 1.6 | Relative change in fBEAT1 at | |
| Day * | 228 | 0.5 | Time of change in fVent1 | |
| - | 0.476 | 0.9 | Factor on the age-specific ICU rates | |
| - | 0.29 | 4.2 | Relative change of for some states ** at | |
| - | 0.0904 | 10.2 | Relative change of for the states other than ** at | |
| - | 0.153 | 0.0 | Relative change of Germany at | |
| - | 1.05 | 2.1 | Maximum death rate change depending on the test positivity rate | |
| - | 0.48 | 2.7 | Minimum death rate change depending on the test positivity rate | |
| 1/% | 0.129 | 9.9 | Slope of death rate change depending on the test positivity rate | |
| day−1 | 0.226 | 5.4 | Death rate of outpatients between and | |
| Day * | 348 | 0.6 | Time of change in | |
| Day * | 446 | 0.8 | Time of change in | |
| - | 27 | 10.6 | Hill factor of time-dependent death rate changes | |
| - | 0.395 | 14.1 | Relative hospitalization rate change for VOC B.1.1.7 | |
| - | 0.162 | 33.1 | Relative rate change to ICU for VOC B.1.1.7 | |
| - | 100 | - | Transit rate from confirmed case to inpatient | |
| Residual Errors | ||||
| %CV | 0.55 | 3 | Exponential error cases | |
| SD | 32.6 | 4.6 | Additive error cases | |
| %CV | 23.3 | 2.8 | Proportional error ICU | |
| SD | 4.56 | 5 | Additive error ICU | |
| %CV | 9.78 | 2.9 | Proportional error fatalities | |
| SD | 11.8 | 6.8 | Additive error fatalities | |
| %CV | 35.2 | 3.5 | Proportional error hospitalizations | |
| SD | 11.8 | 13 | Additive error hospitalizations | |
| %CV | 29.7 | 2.6 | Proportional error ventilated patients | |
| SD | 1.48 | 9.3 | Additive error ventilated patients | |
| %CV | 80.4 | 2.7 | Proportional error daily fatalities | |
| SD | 0.36 | 6.4 | Additive error daily fatalities | |
| %CV | 261 | 3.5 | Proportional error daily fatalities and hospitalizations | |
| SD | 1.46 | 17 | Additive error daily fatalities and hospitalizations | |
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.M.; Wang, W.; Song, Z.G.; Hu, Y.; Tao, Z.W.; Tian, J.H.; Pei, Y.Y.; et al. A New Coronavirus Associated with Human Respiratory Disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 21 July 2022).
- Taylor, L. COVID-19: Brazil’s Hospitals Close to Collapse as Cases Reach Record High. BMJ 2021, 372, n800. [Google Scholar] [CrossRef] [PubMed]
- Ellen Ehni, C.M. ARD-DeutschlandTREND Januar 2021. Available online: https://www.tagesschau.de/inland/deutschlandtrend-2471.pdf (accessed on 19 January 2021).
- Cousins, S. New Zealand Eliminates COVID-19. Lancet 2020, 395, 1474. [Google Scholar] [CrossRef]
- Ferguson, N.; Laydon, D.; Nedjati Gilani, G.; Imai, N.; Ainslie, K.; Baguelin, M.; Bhatia, S.; Boonyasiri, A.; Cucunuba Perez, Z.; Cuomo-Dannenburg, G.; et al. Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID19 Mortality and Healthcare Demand; Imperial College London: London, UK, 2020. [Google Scholar] [CrossRef]
- Graham, M.S.; Sudre, C.H.; May, A.; Antonelli, M.; Murray, B.; Varsavsky, T.; Kläser, K.; Canas, L.S.; Molteni, E.; Modat, M.; et al. Changes in Symptomatology, Reinfection, and Transmissibility Associated with the SARS-CoV-2 Variant B.1.1.7: An Ecological Study. Lancet Public Health 2021, 6, e335–e345. [Google Scholar] [CrossRef]
- Martina Patone, A.; Thomas, K.; Hatch, R.; San Tan, P.; Coupland, C.; Liao, W.; Mouncey, P.; Harrison, D.; Rowan, K.; Horby, P.; et al. Analysis of Severe Outcomes Associated with the SARS-CoV-2 Variant of Concern 202012/01 in England Using ICNARC Case Mix Programme and QResearch Databases. medRxiv 2021. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors Associated with Hospitalization and Critical Illness among 4,103 Patients with COVID-19 Disease in New York City. medRxiv 2020. [Google Scholar] [CrossRef]
- Killerby, M.E.; Link-gelles, R.; Haight, S.C.; Schrodt, C.A.; England, L. Characteristics Associated with Hospitalization among Patients. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 790–794. [Google Scholar] [CrossRef]
- Gallo Marin, B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 Severity: A Literature Review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef]
- Garg, S.; Kim, L.; Whitaker, M.; O’Halloran, A.; Cummings, C.; Holstein, R.; Prill, M.; Chai, S.; Kirley, P.; Alden, N.; et al. Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019—COVID-NET, 14 States, March 1–30, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 458–464. [Google Scholar] [CrossRef]
- Bundesministerium für Gesundheit. Robert Koch-Institut Aktualisierung Der Nationalen Teststrategie Und Neuverkündung Der Verordnung Zum Anspruch Auf Testung in Bezug Auf Einen Direkten Erreger- Nachweis Des Coronavirus SARS-CoV-2 (Coronavirus- Testverordnung–TestV). Epidemiol. Bull. 2020, 43, 3–6. [Google Scholar] [CrossRef]
- Bentout, S.; Tridane, A.; Djilali, S.; Touaoula, T.M. Age-Structured Modeling of COVID-19 Epidemic in the USA, UAE and Algeria. Alex. Eng. J. 2020, 60, 401–411. [Google Scholar] [CrossRef]
- Balabdaoui, F.; Mohr, D. Age-Stratified Discrete Compartment Model of the COVID-19 Epidemic with Application to Switzerland. Sci. Rep. 2020, 10, 21306. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, E. Data-Driven Modeling of COVID-19—Lessons Learned. Extrem. Mech. Lett. 2020, 40, 100921. [Google Scholar] [CrossRef] [PubMed]
- Wells, C.R.; Townsend, J.P.; Pandey, A.; Moghadas, S.M.; Krieger, G.; Singer, B.; McDonald, R.H.; Fitzpatrick, M.C.; Galvani, A.P. Optimal COVID-19 Quarantine and Testing Strategies. Nat. Commun. 2021, 12, 356. [Google Scholar] [CrossRef]
- Corona Zahlen Aktuell: Karte Für Deutschland + Weltweit. Available online: https://interaktiv.morgenpost.de/corona-virus-karte-infektionen-deutschland-weltweit/ (accessed on 4 August 2022).
- SurvStat@RKI 2.0. Available online: https://survstat.rki.de/Content/Query/Create.aspx (accessed on 4 August 2022).
- Informationen Zu Corona: Häufige Fragen-Bayerisches Staatsministerium Des Innern, Für Sport Und Integration. Available online: https://www.stmi.bayern.de/miniwebs/coronavirus/lage/index.php (accessed on 4 August 2022).
- COVID-19 Berlin. Available online: https://www.berlin.de/corona/lagebericht/desktop/corona.html#stationäre-behandlung (accessed on 4 August 2022).
- Pressemitteilungen|Ministerium Für Soziales, Gesundheit, Integration Und Verbraucherschutz. Available online: https://msgiv.brandenburg.de/msgiv/de/presse/pressemitteilungen/ (accessed on 4 August 2022).
- Corona-Fallzahlen-Die Senatorin Für Gesundheit, Frauen Und Verbraucherschutz. Available online: https://www.gesundheit.bremen.de/corona/zahlen/corona-fallzahlen-37649 (accessed on 4 August 2022).
- Corona: Zahlen, Fälle, Statistik von COVID-19-Hamburg.De. Available online: https://www.hamburg.de/corona-zahlen/ (accessed on 4 August 2022).
- Presseinformationen|Nds. Ministerium Für Soziales, Gesundheit Und Gleichstellung. Available online: https://www.ms.niedersachsen.de/startseite/service_kontakt/presseinformationen/ (accessed on 4 August 2022).
- Daten Zur Corona-Pandemie-LAGuS. Available online: https://www.lagus.mv-regierung.de/Gesundheit/InfektionsschutzPraevention/Daten-Corona-Pandemie (accessed on 4 August 2022).
- NRW-Dashboard Zur Corona-Pandemie. Available online: https://www.giscloud.nrw.de/corona-dashboard.html (accessed on 4 August 2022).
- Coronavirus SARS-CoV-2: Aktuelle Fallzahlen Für Rheinland-Pfalz. Available online: https://lua.rlp.de/de/presse/detail/news/News/detail/coronavirus-sars-cov-2-aktuelle-fallzahlen-fuer-rheinland-pfalz/ (accessed on 4 August 2022).
- Infektionsfälle in Sachsen-Coronavirus in Sachsen-Sachsen.De. Available online: https://www.coronavirus.sachsen.de/infektionsfaelle-in-sachsen-4151.html (accessed on 4 August 2022).
- Pressemitteilungen. Available online: https://ms.sachsen-anhalt.de/presse/pressemitteilungen/ (accessed on 4 August 2022).
- COVID-19—Institut Für Infektionsmedizin. Available online: https://www.infmed.uni-kiel.de/de/epidemiologie/covid-19 (accessed on 4 August 2022).
- TMASGFF: Infektionslage. Available online: https://www.tmasgff.de/covid-19/fallzahlen (accessed on 4 August 2022).
- DIVI Intensivregister. Available online: https://www.intensivregister.de/#/aktuelle-lage/laendertabelle (accessed on 4 August 2022).
- Tagesdaten-CSV Aus Dem DIVI-Intensivregister. Available online: https://edoc.rki.de/ (accessed on 4 August 2022).
- Hethcote, H.W. The Mathematics of Infectious Diseases. SIAM Rev. 2000, 42, 599–653. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus disease 2019 (COVID-19): Situation report, 73. World Health Organization. 2020. Available online: https://apps.who.int/iris/handle/10665/331686 (accessed on 5 January 2021).
- Savic, R.M.; Jonker, D.M.; Kerbusch, T.; Karlsson, M.O. Implementation of a Transit Compartment Model for Describing Drug Absorption in Pharmacokinetic Studies. J. Pharmacokinet. Pharmacodyn. 2007, 34, 711–726. [Google Scholar] [CrossRef]
- Upton, R.N.; Mould, D.R. Basic Concepts in Population Modeling, Simulation, and Model-Based Drug Development: Part 3-Introduction to Pharmacodynamic Modeling Methods. CPT Pharmacomet. Syst. Pharmacol. 2014, 3, e88. [Google Scholar] [CrossRef]
- Wang, Y. Derivation of Various NONMEM Estimation Methods. J. Pharmacokinet. Pharmacodyn. 2007, 34, 575–593. [Google Scholar] [CrossRef]
- Karlsson, M.O.; Savic, R.M. Diagnosing Model Diagnostics. Clin. Pharmacol. Ther. 2007, 82, 17–20. [Google Scholar] [CrossRef]
- Helfand, M.; Fiordalisi, C.; Wiedrick, J.; Ramsey, K.L.; Armstrong, C.; Gean, E.; Winchell, K.; Arkhipova-Jenkins, I. Risk for Reinfection After SARS-CoV-2: A Living, Rapid Review for American College of Physicians Practice Points on the Role of the Antibody Response in Conferring Immunity Following SARS-CoV-2 Infection. Ann. Intern. Med. 2022, 175, 547–555. [Google Scholar] [CrossRef]
- Volz, E.; Mishra, S.; Chand, M.; Barrett, J.C.; Johnson, R.; Hopkins, S.; Gandy, A.; Rambaut, A.; Ferguson, N.M. Transmission of SARS-CoV-2 Lineage B.1.1.7 in England: Insights from Linking Epidemiological and Genetic Data. medRxiv 2021. [Google Scholar] [CrossRef]
- Robert Koch-Institut. 2. Bericht Zu Virusvarianten von SARS-CoV-2 in Deutschland, Insbesondere Zur Variant of Concern (VOC) B.1.1.7. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/DESH/Bericht_VOC_2021-02-17.pdf?__blob=publicationFile (accessed on 18 February 2021).
- RKI-Navigation-Besorgniserregende SARS-CoV-2-Virusvarianten (VOC). Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Virusvariante.html;jsessionid=47C4433E4DE091FA86315701A0870406.internet081?nn=2444038 (accessed on 4 August 2022).
- Eurostat; European Commission. Statistical Regions in the European Union and Partner Countries: NUTS and Statistical Regions 2021: 2020 Edition; Publications Office of the European Union: Luxembourg, 2020. [Google Scholar]
- an der Heiden, M. SARS-CoV-2-Nowcasting Und -R-Schaetzung; Zenodo: Berlin, Germany, 2022. [Google Scholar]
- Videokonferenz Der Bundeskanzlerin Mit Den Regierungschefinnen Und Regierungschefs Der Länder Am 28. Oktober 2020. Available online: https://www.bundesregierung.de/breg-de/suche/videokonferenz-der-bundeskanzlerin-mit-den-regierungschefinnen-und-regierungschefs-der-laender-am-28-oktober-2020-1805248 (accessed on 4 August 2022).
- Walsh, S.; Chowdhury, A.; Braithwaite, V.; Russell, S.; Birch, J.M.; Ward, J.L.; Waddington, C.; Brayne, C.; Bonell, C.; Viner, R.M.; et al. Do School Closures and School Reopenings Affect Community Transmission of COVID-19? A Systematic Review of Observational Studies. BMJ Open 2021, 11, e053371. [Google Scholar] [CrossRef] [PubMed]
- Elke, B.; Juliane, W.; Helene, E.; Ulrike, N.; Dimitra, P.; Christoph, R.; Tanja, R.; Reinhard, B. A Country-Level Analysis Comparing Hospital Capacity and Utilisation during the First COVID-19 Wave across Europe. Health Policy 2022, 126, 373–381. [Google Scholar] [CrossRef]
- Jun, T.; Nirenberg, S.; Weinberger, T.; Sharma, N.; Pujadas, E.; Cordon-Cardo, C.; Kovatch, P.; Huang, K. Analysis of Sex-Specific Risk Factors and Clinical Outcomes in COVID-19. Commun. Med. 2021 11 2021, 1, 3. [Google Scholar] [CrossRef] [PubMed]
- Starke, K.R.; Petereit-Haack, G.; Schubert, M.; Kämpf, D.; Schliebner, A.; Hegewald, J.; Seidler, A. The Age-Related Risk of Severe Outcomes Due to COVID-19 Infection: A Rapid Review, Meta-Analysis, and Meta-Regression. Int. J. Environ. Res. Public Health 2020, 17, 5974. [Google Scholar] [CrossRef]
- Ciarambino, T.; Para, O.; Giordano, M. Immune System and COVID-19 by Sex Differences and Age. Women’s Health 2021, 17, 1–6. [Google Scholar] [CrossRef]
- Ohsfeldt, R.L.; Choong, C.K.C.; Mc Collam, P.L.; Abedtash, H.; Kelton, K.A.; Burge, R. Inpatient Hospital Costs for COVID-19 Patients in the United States. Adv. Ther. 2021, 38, 5557–5595. [Google Scholar] [CrossRef]
- Bager, P.; Wohlfahrt, J.; Fonager, J.; Rasmussen, M.; Albertsen, M.; Michaelsen, T.Y.; Møller, C.H.; Ethelberg, S.; Legarth, R.; Button, M.S.F.; et al. Risk of Hospitalisation Associated with Infection with SARS-CoV-2 Lineage B.1.1.7 in Denmark: An Observational Cohort Study. Lancet Infect. Dis. 2021, 21, 1507–1517. [Google Scholar] [CrossRef]
- Challen, R.; Brooks-Pollock, E.; Read, J.M.; Dyson, L.; Tsaneva-Atanasova, K.; Danon, L. Risk of Mortality in Patients Infected with SARS-CoV-2 Variant of Concern 202012/1: Matched Cohort Study. BMJ 2021, 372, n579. [Google Scholar] [CrossRef]
- Modi, C.; Böhm, V.; Ferraro, S.; Stein, G.; Seljak, U. Estimating COVID-19 Mortality in Italy Early in the COVID-19 Pandemic. Nat. Commun. 2021, 12, 2729. [Google Scholar] [CrossRef]
- Liang, L.L.; Tseng, C.H.; Ho, H.J.; Wu, C.Y. COVID-19 Mortality Is Negatively Associated with Test Number and Government Effectiveness. Sci. Rep. 2020, 10, 12567. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.M.; Vinetz, J.M. Dexamethasone in the Management of COVID-19. BMJ 2020, 370, m2648. [Google Scholar] [CrossRef] [PubMed]
- Tomazini, B.M.; Maia, I.S.; Cavalcanti, A.B.; Berwanger, O.; Rosa, R.G.; Veiga, V.C.; Avezum, A.; Lopes, R.D.; Bueno, F.R.; Silva, M.V.A.O.; et al. Effect of Dexamethasone on Days Alive and Ventilator-Free in Patients With Moderate or Severe Acute Respiratory Distress Syndrome and COVID-19: The CoDEX Randomized Clinical Trial. JAMA 2020, 324, 1307–1316. [Google Scholar] [CrossRef] [PubMed]
- Versteckte Triage?: Das Sterben Der Alten Menschen-ZDFheute. Available online: https://www.zdf.de/nachrichten/panorama/corona-triage-pflegeheime-100.html (accessed on 4 August 2022).
- Booton, R.D.; MacGregor, L.; Vass, L.; Looker, K.J.; Hyams, C.; Bright, P.D.; Harding, I.; Lazarus, R.; Hamilton, F.; Lawson, D.; et al. Estimating the COVID-19 Epidemic Trajectory and Hospital Capacity Requirements in South West England: A Mathematical Modelling Framework. BMJ Open 2021, 11, 41536. [Google Scholar] [CrossRef]










| Ward (Fraction of Patients) | Outcome (Fraction of Patients by Ward) | Total Duration until Discharge [Days] (sd) | Proportion of Time in ICU [%] (sd) | Proportion of Time Ventilated [%] (sd) |
|---|---|---|---|---|
| General ward only (81.8%) | Recovery (82.2%) | 11.5 (11.4) | ||
| Death (17.8%) | 10.6 (11.2) | |||
| ICU without ventilation (6.0%) | Recovery (76.1%) | 20.4 (17.1) | 29 (96) | |
| Death (23.9%) | 20.0 (20.5) | 44 (33) | ||
| ICU with ventilation (12.2%) | Recovery (34.5%) | 28.6 (18.3) | 43 (39) | 28 (21) |
| Death (65.5%) | 15.5 (12.6) | 68 (31) | 63 (34) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dings, C.; Götz, K.M.; Och, K.; Sihinevich, I.; Werthner, Q.; Smola, S.; Bliem, M.; Mahfoud, F.; Volk, T.; Kreuer, S.; et al. Model-Based Analysis of SARS-CoV-2 Infections, Hospitalization and Outcome in Germany, the Federal States and Districts. Viruses 2022, 14, 2114. https://doi.org/10.3390/v14102114
Dings C, Götz KM, Och K, Sihinevich I, Werthner Q, Smola S, Bliem M, Mahfoud F, Volk T, Kreuer S, et al. Model-Based Analysis of SARS-CoV-2 Infections, Hospitalization and Outcome in Germany, the Federal States and Districts. Viruses. 2022; 14(10):2114. https://doi.org/10.3390/v14102114
Chicago/Turabian StyleDings, Christiane, Katharina Martha Götz, Katharina Och, Iryna Sihinevich, Quirin Werthner, Sigrun Smola, Marc Bliem, Felix Mahfoud, Thomas Volk, Sascha Kreuer, and et al. 2022. "Model-Based Analysis of SARS-CoV-2 Infections, Hospitalization and Outcome in Germany, the Federal States and Districts" Viruses 14, no. 10: 2114. https://doi.org/10.3390/v14102114