1. Introduction
Dengue is a vector-borne viral disease that is a major public health problem in tropical and subtropical regions of the globe. According to the World Health Organization, the incidence of dengue has grown globally, reaching up to 4.2 million cases in 2019 [
1]. Out of all these cases, 73% were reported in the Americas, and 25,000 of them were classified as severe cases and represented the main cause of mortality in children under 15 years of age in Latin American [
1,
2].
Dengue fever is caused by four distinct dengue virus serotypes (DENV1, 2, 3, and 4) that are comprised within the Flaviviridae family [
3]. Each of these serotypes causes clinical disease that can range from mild undifferentiated fever to more severe and potentially life-threatening symptoms such as dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) [
3,
4,
5]. Interestingly, almost 70% of DENV infections may present themselves as asymptomatic [
6]. Clinical characteristics of a mild infection with DENV include fever, rash, headache, and chills, and it is often indistinguishable from other infectious diseases that are also endemic in the tropics, including malaria or Zika fever [
7,
8]. Severe forms of DENV infection are characterized by an increase in vascular permeability, hypovolemia, and petechiae, which may lead to death within 24 h if not treated effectively. However, early diagnosis seems to have a significant positive impact on patient recovery when following appropriate treatment [
9].
DENV is transmitted via the infectious bite of female
Aedes mosquitoes, and mosquito surveillance as well as vector control remain as the main tools to combat this disease [
10]. In Colombia, DENV is transmitted by two species of
Aedes mosquitoes with
Ae. aegypti as the primary vector in almost 80% of the Colombian territory, and
Ae. albopictus as secondary vector in places where these species have been recently introduced [
11,
12]. Colombia is classified as hyperendemic for dengue transmission since all four serotypes are circulating throughout the country and are even within the same endemic foci [
13]. Severe dengue presentations are usually associated with secondary infections caused by a different DENV serotype than the one causing the primary infection. Therefore, people living in hyperendemic areas, such as Colombia, are at higher risk of severe disease.
In 2019, Colombia presented 127,553 dengue cases, which represents an increase of 185% from the 44,825 cases reported in 2018 [
14]. In rural areas where access to health care is precarious, health personnel rely on clinical characteristics to diagnose febrile diseases due to increased costs, limited access to diagnostic methods, or increased time to diagnosis [
15]. In the case of dengue fever, lower platelets with leukocytosis are often used to discriminate between dengue and other febrile diseases. Data from the Pan-American Health Organization (PAHO) shows that only 44.6% (1,415,658) of all dengue cases reported in 2019 in the Americas were laboratory confirmed [
16]. In addition, natural disasters and social instability provoking forced migration, both within and between countries, have an impact on transmission, moving pathogens from one side of the border to the other and weakening the already fragile health infrastructure in developing countries [
17]. Such an example is the current mass migration from Venezuela impacting almost every country in Latin America. In this case, access to health care and the availability of proper tools to identify infected people have become important issues [
18].
In this scenario, rapid, accurate and cost-efficient diagnosis of dengue fever becomes critical for clinical care since it can prevent evolution to severe clinical presentations. Furthermore, accurate and prompt detection of DENV infections can guide vector control activities and can provide important data to guide public health policy, vaccine research, and monitor the effectiveness of control measures [
15,
19]. This situation demands the need to develop and test field deployable diagnostic tools. The development of rapid diagnostic tests (RDT) in the dipstick format has allowed the timely detection of DENV infections in areas with no access to electricity [
20] although the sensitivity or specificity of these tests may be impacted by the presence of other flaviviruses in the area, among other factors [
21,
22]. Currently, DENV non-structural protein 1 (NS1) based tests have been developed into the dipstick format to offer the possibility of rapid and reliable diagnosis of dengue fever [
23]. The DENV NS1 protein is abundant in serum during the acute phase of infection with DENV, and it is mainly detected during the first five to six days after the onset of fever [
24,
25].
In the absence of a specific treatment to cure dengue fever and prevent complications, an effective vaccine is urgently needed. Dengvaxia
® is the only vaccine commercially available to prevent DENV infection [
26]. However, due to potential adverse effects in naïve populations, the vaccine is recommended for people older than nine years of age who have had previous exposure to DENV [
26,
27]. There is an important knowledge gap addressing the clinical characteristics of dengue fever that may be associated with the performance of diagnostics test. The characterization of infection status and hematological findings during DENV infection in endemic areas will not only help in the design of improved vaccines but will also help in the identification of at-risk age groups as well as provide tools for early identification of infected individuals after vaccine deployment in the field [
28]. Thus, with this study, we wanted to answer the question: what hematological parameters are characteristic of people who are diagnosed with dengue fever by clinical symptoms and how do those parameters correlate with diagnostic tests in hyperendemic areas? To answer this, we compared hemogram results among people diagnosed as a “probable dengue” case using clinical parameters and performed an NS1-based rapid diagnostic test (RDT) and reverse transcription polymerase chain reaction (RT-PCR) to detect current DENV infections.
4. Discussion
Dengue is still a major arboviral disease of the tropics and subtropical areas and Latin America is no exception [
27] Thus, it was is not surprising to find infections caused by each of the four DENV serotypes from the PCR analysis. Importantly, ~3% of infected individuals presented an infection with more than one serotype, consistent with previous reports showing Norte de Santander as a hyperendemic region for DENV transmission [
30,
31]. Although no other arboviruses were tested in our current study, our study area is well known for the transmission of other Aedes-borne viruses such as Zika virus (ZIKV) and Chikungunya virus (CHIKV). All of these viruses cause febrile disease, which are clinically indistinguishable during the first days of symptoms most of the time. Although no specific treatment is available against any of these diseases, accurate diagnosis is pivotal to prevent the progression of severity in all of them.
In Colombia, dengue fever is generally diagnosed using IgM-ELISA, however, not all health centers are properly equipped to offer this service to the public due to a lack of electricity or other necessary infrastructure, making it obligatory for physicians to learn how to differentiate these entities using clinical characteristics [
32]. In this study we wanted to provide a list of hematological parameters found in people classified as a “probable” dengue infected patient using clinical and hematological parameters in wait of a confirmatory test. Our objective with this was to help guide decisions based on hematological parameters that are associated with a positive diagnostic test result. Our results suggest that, besides platelet count, total white blood cell count and monocyte cell count are important parameters differentiating the “probable dengue” cases with a positive confirmatory test from those with negative tests. In this context, other studies have described significant leukopenia in dengue patients [
29,
33], and although peripheral blood parameters change over the course of infection with DENV, in this study, we included volunteers seeking medical care 3 to 7 days after presenting symptoms compatible with DENV infection such as fever and rash. Once the physician sends the hematological tests, a patient is diagnosed as a “probable” dengue fever case based on the platelet and leucocyte counts as well as the hematocrit level.
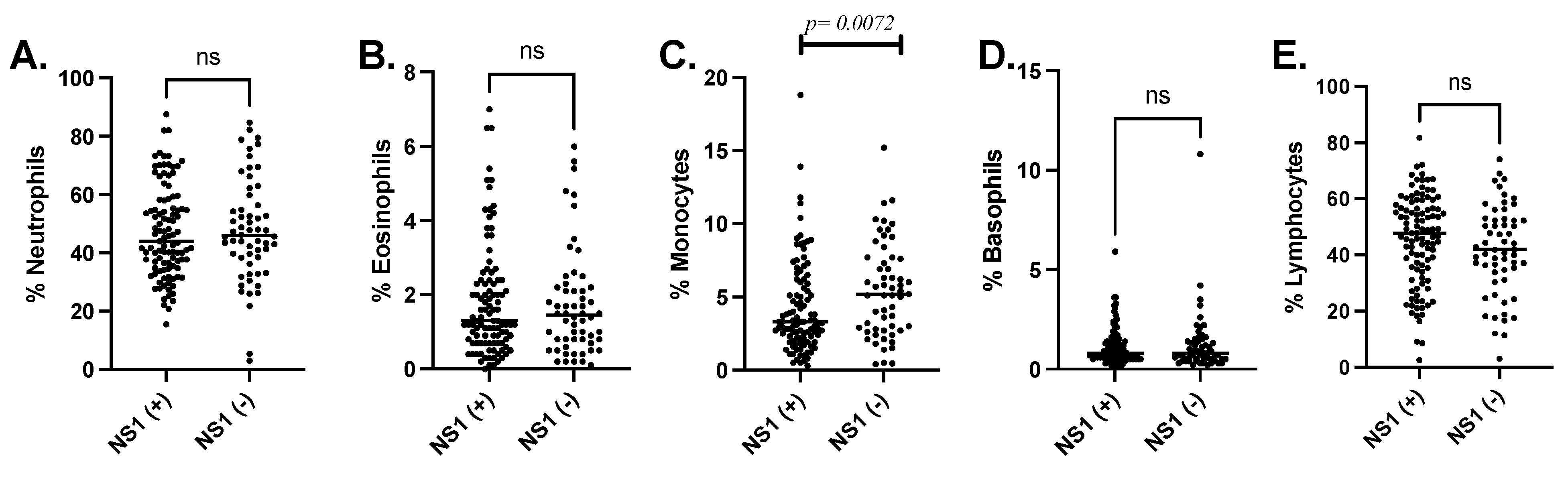
In the case of leukocyte count, we found that volunteers with a positive DENV-NS1-Ag test presented a significantly lower leukocyte count than those with probable dengue fever but with a negative RDT. Further analyzing the type of white blood cells that are more affected by DENV infection, we found that monocytes were significantly lower in people with a positive DENV-NS1-Ag test. However, monocytes are among the main targets of DENV infection and have been implicated in both protection and pathogenesis [
34] because they produce inflammatory cytokines often involved with endothelial disruption and plasma leakage [
35]. Previous studies suggest that monocytes are also the subject of apoptosis induced by DENV in several ways [
36,
37]. First, DENV infection in monocytes may induce pyroptosis, known as the induction of cell death, mediated by the concomitant activation of caspase 1 and interleukin 1 (IL1) production [
37]. In addition, the production of tumor necrosis factor alpha (TNF-α) in DENV infected monocytes also induces apoptosis in such cells [
36,
37]. These mechanisms may explain the significant decrease in monocytes in people where the NS1 antigen can be detected by the RDT. Interestingly, a retrospective study in Taiwan with more than 1000 patients diagnosed with DENV 2 and 3 infections, reported lower absolute monocyte counts five days after fever onset in patients with mild disease when compared to patients with severe DENV infection [
38]. Another study found that dengue fever patients presented significantly lower white blood cell and monocyte count when compared to patients with other febrile illness [
39]. These studies highlight the importance of more research describing hematological findings in people infected with arboviruses in hyperendemic areas.
As explained above, a lack of testing for arbovirus infection in several primary health facilities results in these diseases often being diagnosed by clinical findings, including a decreased platelet count, leukopenia, and an increase in hematocrit among the main parameters [
40,
41]. Rapid diagnostic tests (RDT) can overcome some of the limitations posed by restricted access to electricity and highly trained personnel. Thus, we decided to test the efficacy of a DENV NS1-based RDT to identify DENV infection in these settings. Previous studies have determined that the presence of NS1 Ag overlays with the viremic phase of DENV infection during the first 4 to 5 days of clinical symptoms [
42], but test performance may be affected by the time the person seeks medical attention. In this study, the NS1-Ag test presented a lower specificity than was previously reported in other studies; however, we found that the sensitivity of the DENV-NS1-Ag test in comparison to the RT-PCR decreased from 87% when the test was performed within the first 5 days of presenting symptoms to 81% if the test was performed afterwards. These results are consistent with previous studies showing the sensitivity and the specificity of the DENV-NS1-Ag test ranging between 27.8 and 93.4%, respectively [
43,
44,
45].
Differences in the incidence of DENV infections between males and females have been previously reported. In this study, the majority of probable and confirmed dengue cases determined by the RDT were found among female volunteers. Additionally, a significant number of cases with a positive dengue diagnostic test were 15 years of age and younger, consistent with previous studies in the country [
46]. Although previous studies have shown gender-associated differences in dengue fever incidence, the geographical area appears to strongly influence the associations and occurrence of dengue infections [
47,
48,
49]. For instance, a study including dengue fever cases from at least six Asian countries showed a higher incidence of dengue in males [
47], while other studies in Central and South America demonstrated a higher incidence of dengue in females [
48,
49].
A significant limitation in our current study is that we could not follow the patient’s clinical development or hematological findings on the days after the diagnosis so, it is impossible for us to correlate these parameters with progression to severe forms of infection. Another limitation is the lack of access to the previous dengue history of the patients or asymptomatic infections to compare hematological parameters, which would help to narrow down key factors associated with current infections.
In summary, our findings suggest a significant leukopenia in those with a positive DENV-NS1-Ag test and that monocytes may be the main white blood cells affected in this group of patients. Due to the presence of all four DENV serotypes and the probability of multiple infections in the area, it is important to evaluate diagnostic tools that can be implemented in areas where infrastructure does not allow the implementation of molecular tools such as RT-PCR. A vaccine against DENV in this area should be able to prevent infection against the four serotypes, especially in younger populations representing the majority of cases in this hyperendemic area of Colombia.







{kind=link}
{kind=link}