
Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics
2.2. Participants and Setting
2.3. Laboratory Tests
- -
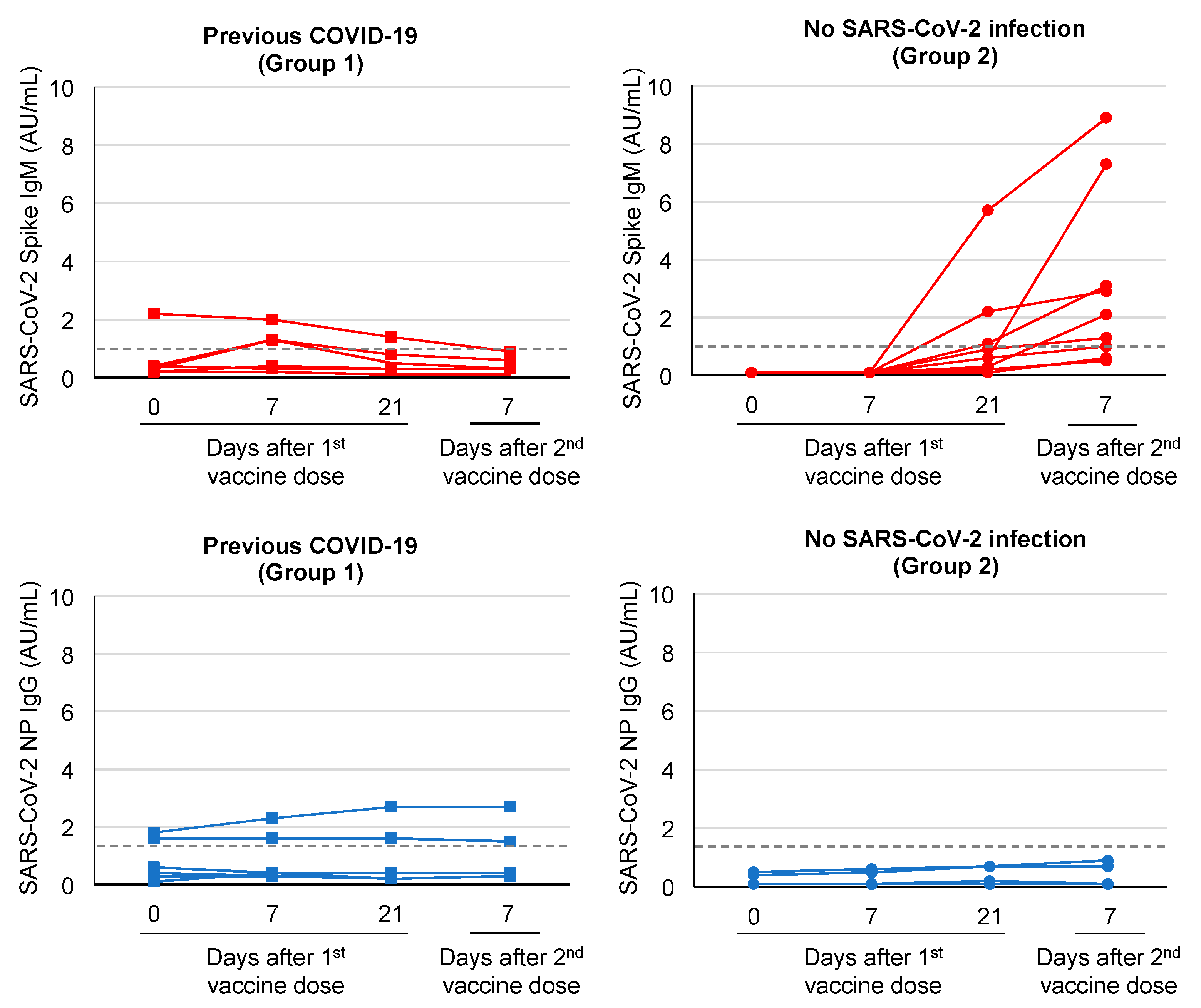
- An automated chemiluminescent microparticle immunoassay (CMIA) test for the qualitative detection of IgM antibodies to the spike protein of SARS-CoV-2 (SARS-CoV-2 IgM, Abbott Laboratories, IL, USA). According to the manufacturer’s instructions, serum samples were considered positive when the output index was ≥1.0 AU/mL.
- -
- An automated CMIA test for the qualitative detection of IgG antibodies to the nucleocapsid protein of SARS-CoV-2 (SARS-CoV-2 IgG, Abbott Laboratories). Serum samples were considered positive when the output index was ≥1.4 AU/mL.
- -
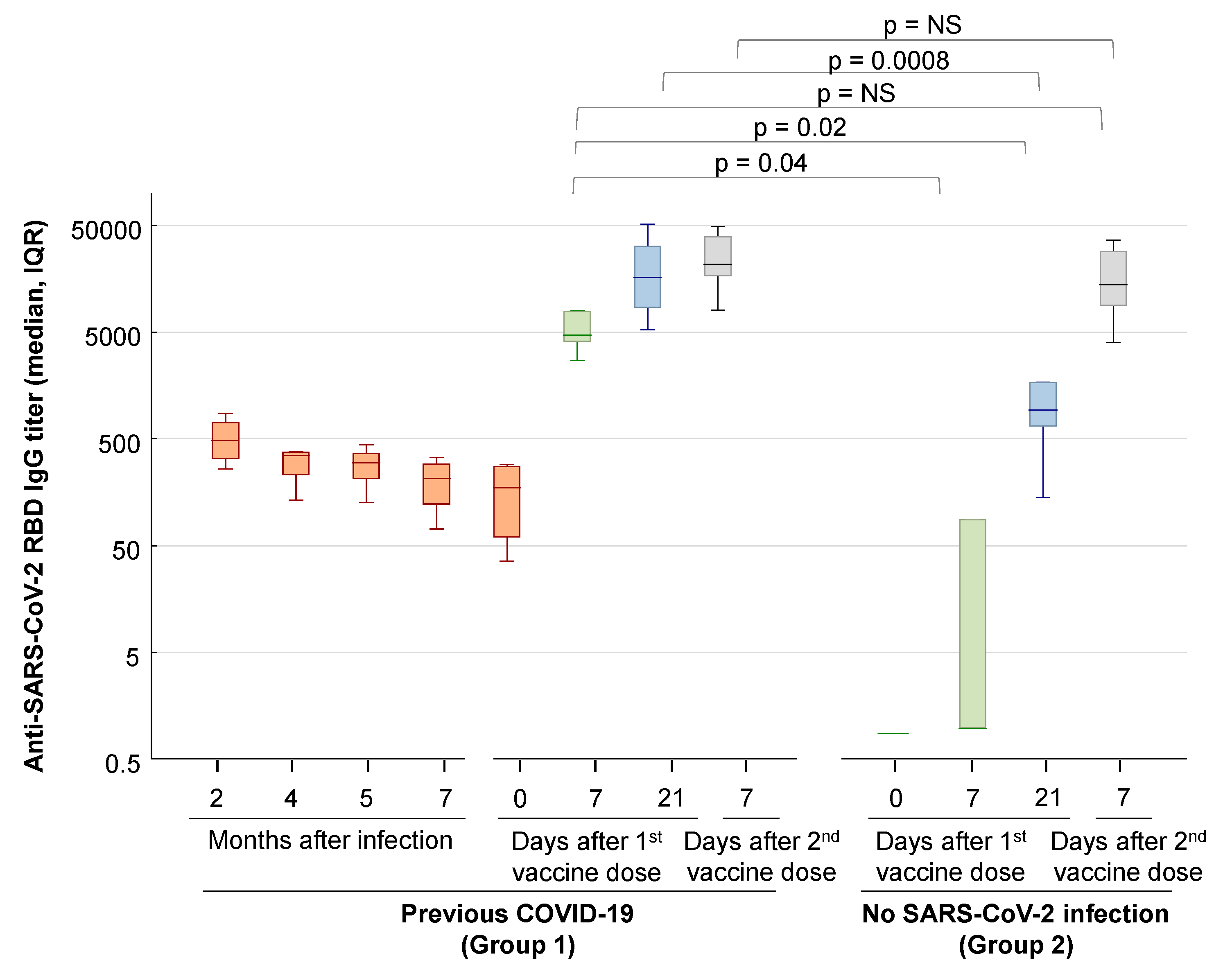
- An automated CMIA test for the qualitative and quantitative detection of IgG antibodies to the spike receptor-binding domain (RBD) of SARS-CoV-2 (SARS-CoV-2 IgG II Quant assay, Abbott Laboratories). The LOD of the assay was 6.9 AU/mL; the upper limit of quantification was 80,000 AU/mL.
2.4. Statistical Analysis
3. Results
3.1. Case Description
3.2. Reactogenicity of BNT162b2 mRNA COVID-19 Vaccine
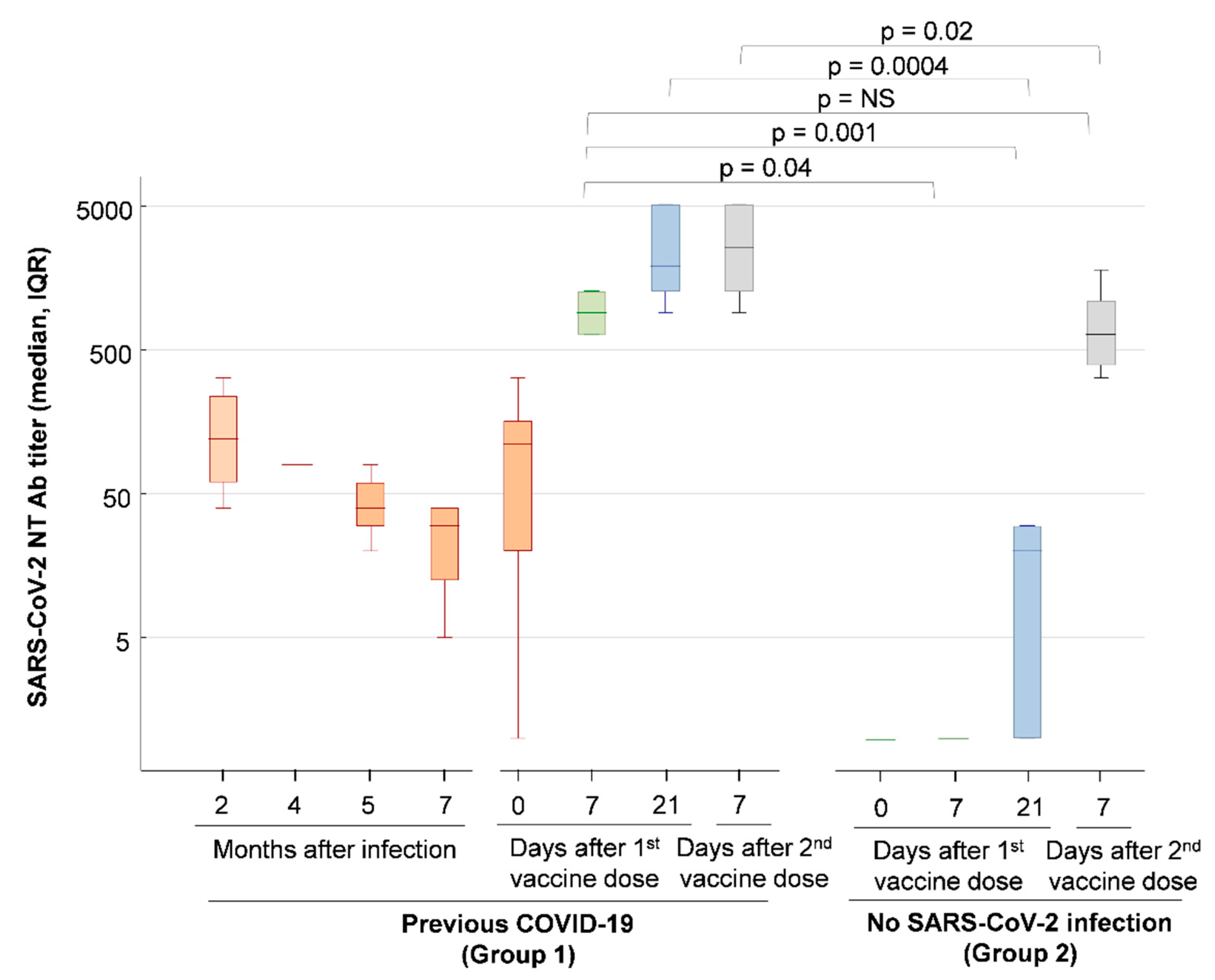
3.3. Antibody Responses after Natural SARS-CoV-2 Infection and Vaccination with BNT162b2 mRNA Vaccine
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://covid19.who.int/ (accessed on 16 February 2021).
- Marot, S.; Malet, I.; Leducq, V.; Zafilaza, K.; Sterlin, D.; Planas, D.; Gothland, A.; Jary, A.; Dorgham, K.; Bruel, T.; et al. Rapid decline of neutralizing antibodies against SARS-CoV-2 among infected healthcare workers. Nat. Commun. 2021, 12, 844. [Google Scholar] [CrossRef] [PubMed]
- Dimeglio, C.; Herin, F.; Miedougé, M.; Martin-Blondel, G.; Soulat, J.M.; Izopet, J. Protection of healthcare workers against SARS-CoV-2 reinfection. Clin. Infect. Dis. 2021, ciab069. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.; Foulkes, S.; Charlett, A.; Atti, A.; Monk, E.J.M.; Simmons, R.; Wellington, E.; Cole, M.J.; Saei, A.; Oguti, B.; et al. Do antibody positive healthcare workers have lower SARS-CoV-2 infection rates than antibody negative healthcare workers? Large multi-centre prospective cohort study (the SIREN study), England: June to November. medRxiv 2020. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Diagnostic Testing for SARS-CoV-2. Available online: https://www.who.int/publications/i/item/diagnostic-testing-for-sars-cov-2 (accessed on 16 February 2021).
- Centers for Disease Control and Prevention. COVID-19. Research Use Only 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Primers and Probes. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/rt-pcr-panel-primer-probes.html (accessed on 16 February 2021).
- Krammer, F.; Srivastava, K.; the PARIS team; Simon, V. Robust spike antibody responses and increased reactogenicity in seropositive individuals after a single dose of SARS-CoV-2 mRNA vaccine. medRxiv 2021. [Google Scholar] [CrossRef]
- Prendecki, M.; Clarke, C.; Brown, J.; Cox, A.; Gleeson, S.; Guckian, M.; Randell, P.; Dalla Pria, A.; Lightstone, L.; Xu, X.-N.; et al. Effect of previous SARS-CoV-2 infection on humoral and T-cell responses to single-dose BNT162b2 vaccine. Lancet 2021. [Google Scholar] [CrossRef]
- Manisty, C.; Otter, A.D.; Treibel, T.A.; McKnight, Á.; Altmann, D.M.; Brooks, T.; Noursadeghi, M.; Boyton, R.J.; Semper, A.; Moon, J.C. Antibody response to first BNT162b2 dose in previously SARS-CoV-2-infected individuals. Lancet 2021. [Google Scholar] [CrossRef]
- Saadat, S.; Rikhtegaran Tehrani, Z.; Logue, J.; Newman, M.; Frieman, M.B.; Harris, A.D.; Sajadi, M.M. Single dose vaccination in healthcare workers previously infected with SARS-CoV-2. medRxiv 2021. [Google Scholar] [CrossRef]
- Stamatatos, L.; Czartoski, J.; Wan, Y.-H.; Homad, L.J.; Rubin, V.; Glantz, H.; Neradilek, M.; Seydoux, E.; Jennewein, M.F.; MacCamy, A.J.; et al. Antibodies elicited by SARS-CoV-2 infection and boosted by vaccination neutralize an emerging variant and SARS-CoV-1. medRxiv 2021. [Google Scholar] [CrossRef]
- Levi, R.; Azzolini, E.; Pozzi, C.; Ubaldi, L.; Lagioia, M.; Mantovani, A.; Rescigno, M. A cautionary note on recall vaccination in ex-COVID-19 subjects. medRxiv 2021. [Google Scholar] [CrossRef]
- Tada, T.; Dcosta, B.M.; Samanovic-Golden, M.; Herati, R.S.; Cornelius, A.; Mulligan, M.J.; Landau, N.R. Neutralization of viruses with European, South African, and United States SARS-CoV-2 variant spike proteins by convalescent sera and BNT162b2 mRNA vaccine-elicited antibodies. bioRxiv 2021. [Google Scholar] [CrossRef]
- Bradley, T.; Grundberg, E.; Selvarangan, R. Antibody responses boosted in seropositive healthcare workers after single dose of SARS-CoV-2 mRNA vaccine. medRxiv 2021. [Google Scholar] [CrossRef]
- Abu Jabal, K.; Ben-Amram, H.; Beiruti, K.; Batheesh, Y.; Sussan, C.; Zarka, S.; Edelstein, M. Impact of age, ethnicity, sex and prior infection status on immunogenicity following a single dose of the BNT162b2 mRNA COVID-19 vaccine: Real-world evidence from healthcare workers, Israel, December 2020 to January 2021. Euro Surveill. 2021, 26. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, F.; Sarasini, A.; Zierold, C.; Calleri, M.; Bonetti, A.; Vismara, C.; Blocki, F.A.; Pallavicini, L.; Chinali, A.; Campisi, D.; et al. Clinical and analytical performance of an automated serological test that identifies S1/S2-neutralizing IgG in COVID-19 patients semiquantitatively. J. Clin. Microbiol. 2020, 58, e01224-20. [Google Scholar] [CrossRef]
- Meyer, B.; Reimerink, J.; Torriani, G.; Brouwer, F.; Godeke, G.J.; Yerly, S.; Hoogerwerf, M.; Vuilleumier, N.; Kaiser, L.; Eckerle, I.; et al. Validation and clinical evaluation of a SARS-CoV-2 surrogate virus neutralisation test (sVNT). Emerg. Microbes Infect. 2020, 9, 2394–2403. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ID | Age Range, Sex | Symptoms | Quarantine Duration (Days) |
|---|---|---|---|
| 1 | 30s, female | Fever (max 38.5 °C) for 4 days, asthenia, mild cough, diarrhea (1 day), ageusia, anosmia | 25 |
| 2 | 40s, male | Fever (max 38 °C) for 1 day, asthenia, arthralgias, anosmia | 24 |
| 3 | 40s, male | Asthenia, oral ulcers, ageusia, anosmia | 29 |
| 4 | 40s, female | Fever (max 38 °C) for 3 days, asthenia, ageusia | 41 |
| 5 | 30s, female | Fever (max 38.5 °C), asthenia, ageusia, anosmia | 32 |
| 6 | 40s, male | Asthenia, anosmia | 35 |
| Vaccine-Associated Side Effects | Group 1 (n = 6) | Group 2 (n = 9) | ||
|---|---|---|---|---|
| First Dose | Second Dose | First Dose | Second Dose | |
| Local pain | 6 (100%) | 5 (83%) | 3 (33%) | 4 (44%) |
| Asthenia | 0 | 3 (50%) | 2 (22%) | 4 (44%) |
| Fever > 37.5 °C | 0 | 1 (17%) | 0 | 2 (22%) |
| Headache | 0 | 0 | 1 (11%) | 3 (33%) |
| Myalgia | 0 | 1 (17%) | 0 | 2 (22%) |
| Adenopathy | 1 (17%) | 0 | 0 | 0 |
| Lymphangitis | 0 | 0 | 0 | 1 (11%) |
| Nausea | 0 | 0 | 0 | 1 (11%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gobbi, F.; Buonfrate, D.; Moro, L.; Rodari, P.; Piubelli, C.; Caldrer, S.; Riccetti, S.; Sinigaglia, A.; Barzon, L. Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses 2021, 13, 422. https://doi.org/10.3390/v13030422
Gobbi F, Buonfrate D, Moro L, Rodari P, Piubelli C, Caldrer S, Riccetti S, Sinigaglia A, Barzon L. Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection. Viruses. 2021; 13(3):422. https://doi.org/10.3390/v13030422
Chicago/Turabian StyleGobbi, Federico, Dora Buonfrate, Lucia Moro, Paola Rodari, Chiara Piubelli, Sara Caldrer, Silvia Riccetti, Alessandro Sinigaglia, and Luisa Barzon. 2021. "Antibody Response to the BNT162b2 mRNA COVID-19 Vaccine in Subjects with Prior SARS-CoV-2 Infection" Viruses 13, no. 3: 422. https://doi.org/10.3390/v13030422