
Calcium Silicate-Based Sealer Dentinal Tubule Penetration—A Systematic Review of In Vitro Studies

Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
2.3. Information Sources and Search Strategy
2.4. Study Screening and Selection Process
2.5. Data Collection Process and Data Items
2.6. Study Risk of Bias Assessment
3. Results
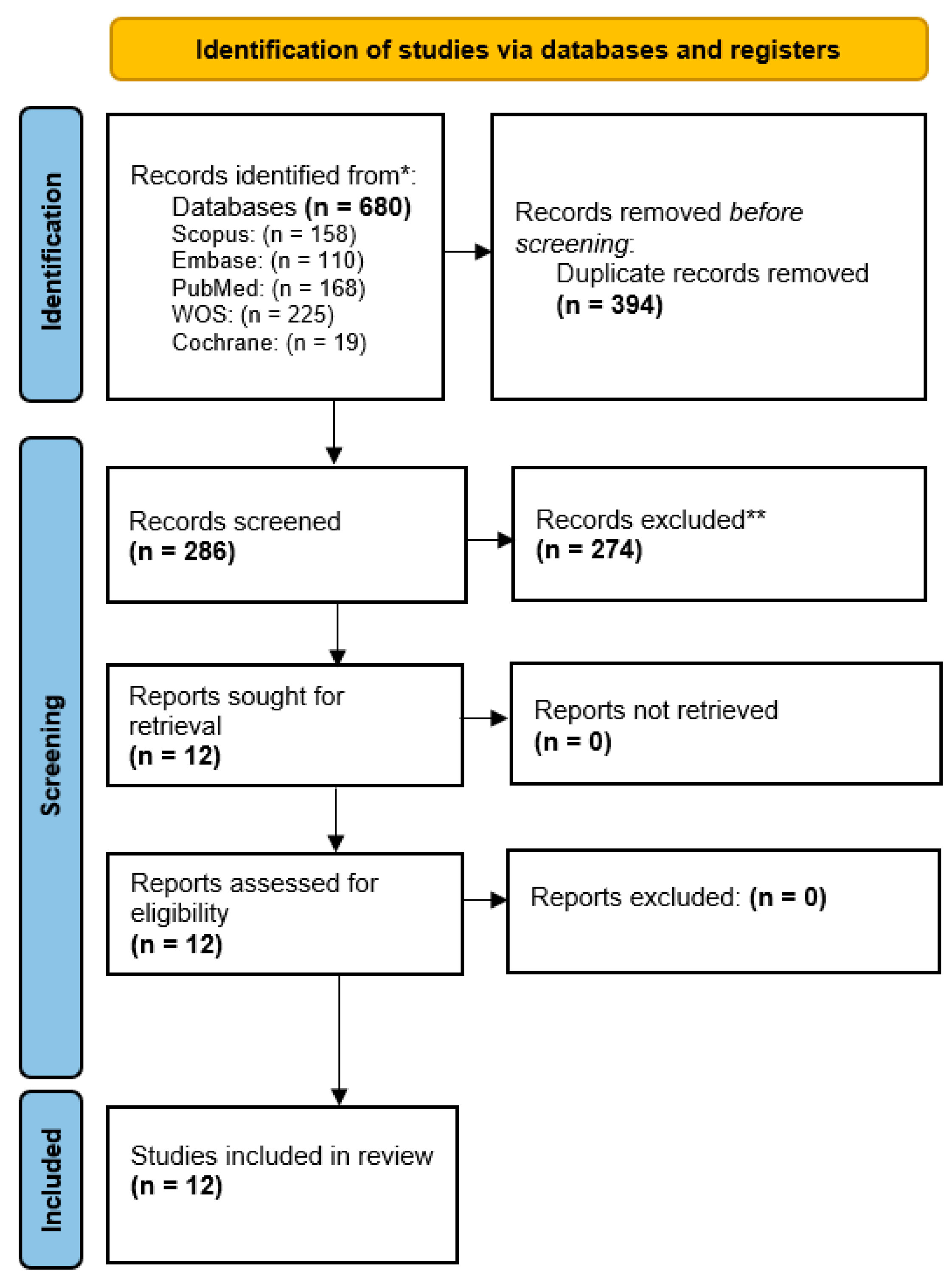
3.1. Study Selection
3.2. Study Methodology
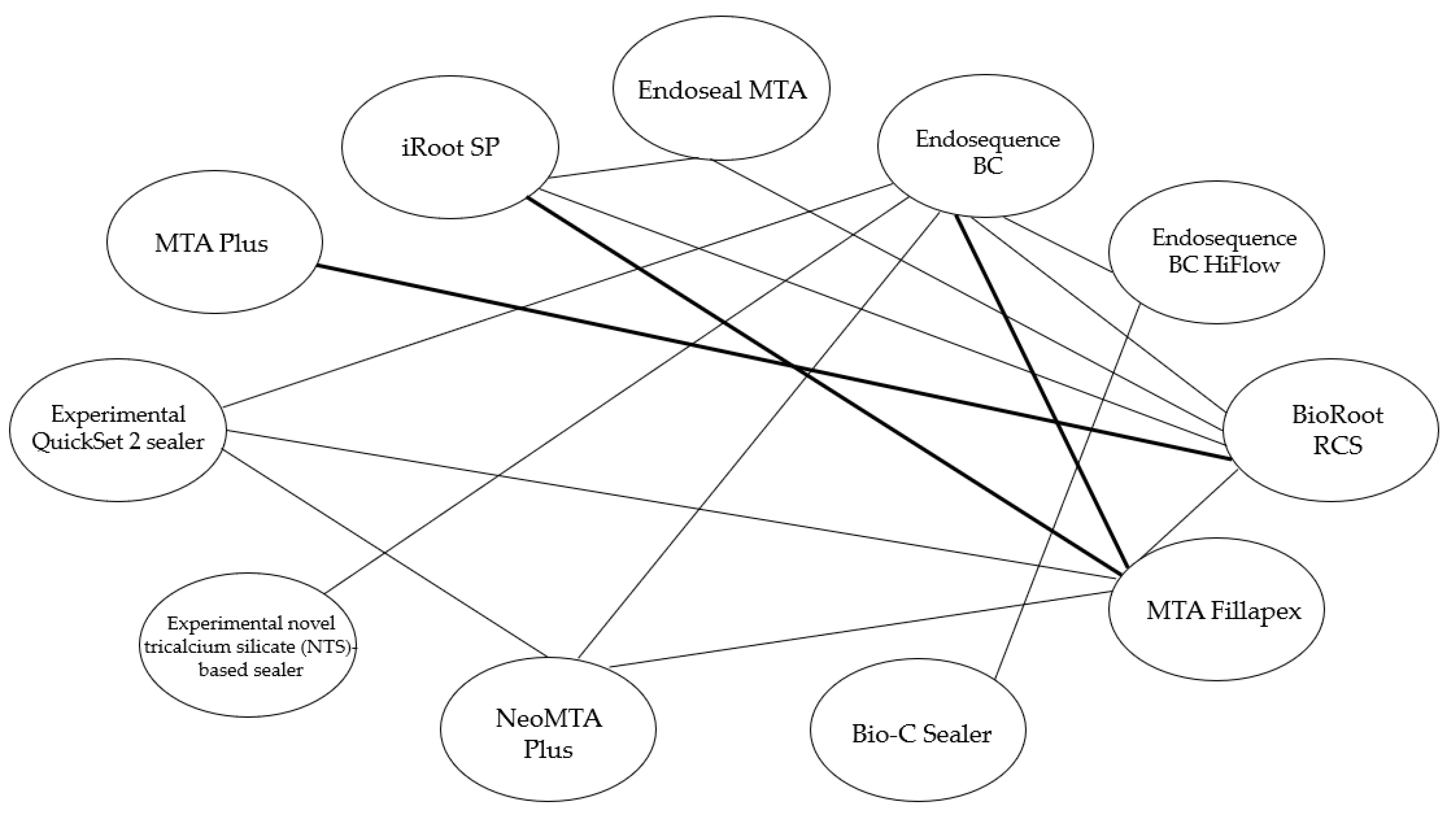
3.2.1. Studied Materials
3.2.2. Sample Characteristics, Instrumentation, and Irrigation Sequence
3.2.3. Study Groups and Outcome Measurement
3.3. Study Results
3.3.1. Sealer Tubular Penetration Depth
3.3.2. Sealer Penetration Percentage and Area
3.4. Quality Assessment
4. Discussion
4.1. On the Methodology of the Included Studies
4.2. On the Results of the Included Studies
4.3. Factors which Influence Dentinal Tubule Penetration
4.4. Strengths, Limitations, and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schilder, H.; Hargreaves, K.M. Filling Root Canals in Three Dimensions. J. Endod. 2006, 32, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Tomson, R.M.E.; Polycarpou, N.; Tomson, P.L. Contemporary Obturation of the Root Canal System. Br. Dent. J. 2014, 216, 315–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Liu, S.; Dong, Y. In Vitro Study of Dentinal Tubule Penetration and Filling Quality of Bioceramic Sealer. PLoS ONE 2018, 13, e0192248. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zhao, X.; Qiu, Y.; Xu, D.; Cui, L.; Wu, B. The Tubular Penetration Depth and Adaption of Four Sealers: A Scanning Electron Microscopic Study. Biomed. Res. Int. 2017, 2017, 2946524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ordinola-Zapata, R.; Bramante, C.M.; Graeff, M.S.Z.; del Carpio Perochena, A.; Vivan, R.R.; Camargo, E.J.; Garcia, R.B.; Bernardineli, N.; Gutmann, J.L.; de Moraes, I.G. Depth and Percentage of Penetration of Endodontic Sealers into Dentinal Tubules after Root Canal Obturation Using a Lateral Compaction Technique: A Confocal Laser Scanning Microscopy Study. Oral Surg. Oral Med. Oral. Radiol. 2009, 108, 450–457. [Google Scholar] [CrossRef] [PubMed]
- Deniz Sungur, D.; Aksel, H.; Purali, N. Effect of a Low Surface Tension Vehicle on the Dentinal Tubule Penetration of Calcium Hydroxide and Triple Antibiotic Paste. J. Endod. 2017, 43, 452–455. [Google Scholar] [CrossRef]
- Alsubait, S.; Albader, S.; Alajlan, N.; Alkhunaini, N.; Niazy, A.; Almahdy, A. Comparison of the Antibacterial Activity of Calcium Silicate- and Epoxy Resin-Based Endodontic Sealers against Enterococcus Faecalis Biofilms: A Confocal Laser-Scanning Microscopy Analysis. Odontology 2019, 107, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Kok, D.; Duarte, M.A.H.; da Rosa, R.A.; Wagner, M.H.; Pereira, J.R.; Só, M.V.R. Evaluation of Epoxy Resin Sealer after Three Root Canal Filling Techniques by Confocal Laser Scanning Microscopy. Microsc. Res. Technol. 2012, 75, 1277–1280. [Google Scholar] [CrossRef]
- Al-Haddad, A.; Aziz, Z.A.C.A. Bioceramic-Based Root Canal Sealers: A Review. Int. J. Biomater. 2016, 2016, 9753210. [Google Scholar] [CrossRef] [Green Version]
- Raghavendra, S.S.; Jadhav, G.R.; Gathani, K.M.; Kotadia, P. Bioceramics in Endodontics—A Review. J. Istanb. Univ. Fac. Dent. 2017, 51, S128. [Google Scholar] [CrossRef]
- Santos, J.M.; Diogo, P.; Dias, S.; Marques, J.A.; Palma, P.J.; Ramos, J.C. Long-Term Outcome of Nonvital Immature Permanent Teeth Treated With Apexification and Corono-Radicular Adhesive Restoration: A Case Series. J. Endod. 2022, 48, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Lee, D.Y.; Lee, S.H. Comparison of Antimicrobial Activity of Traditional and New Developed Root Sealers against Pathogens Related Root Canal. J. Dent. Sci. 2018, 13, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Palma, P.J.; Ramos, J.C.; Martins, J.B.; Diogenes, A.; Figueiredo, M.H.; Ferreira, P.; Viegas, C.; Santos, J.M. Histologic Evaluation of Regenerative Endodontic Procedures with the Use of Chitosan Scaffolds in Immature Dog Teeth with Apical Periodontitis. J. Endod. 2017, 43, 1279–1287. [Google Scholar] [CrossRef]
- Candeiro, G.T.D.M.; Correia, F.C.; Duarte, M.A.H.; Ribeiro-Siqueira, D.C.; Gavini, G. Evaluation of Radiopacity, PH, Release of Calcium Ions, and Flow of a Bioceramic Root Canal Sealer. J. Endod. 2012, 38, 842–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva Almeida, L.H.; Moraes, R.R.; Morgental, R.D.; Pappen, F.G. Are Premixed Calcium Silicate–Based Endodontic Sealers Comparable to Conventional Materials? A Systematic Review of In Vitro Studies. J. Endod. 2017, 43, 527–535. [Google Scholar] [CrossRef]
- Cavenago, B.C.; Pereira, T.C.; Duarte, M.A.H.; Ordinola-Zapata, R.; Marciano, M.A.; Bramante, C.M.; Bernardineli, N. Influence of Powder-to-Water Ratio on Radiopacity, Setting Time, PH, Calcium Ion Release and a Micro-CT Volumetric Solubility of White Mineral Trioxide Aggregate. Int. Endod. J. 2014, 47, 120–126. [Google Scholar] [CrossRef]
- Poggio, C.; Lombardini, M.; Alessandro, C.; Simonetta, R. Solubility of Root-End-Filling Materials: A Comparative Study. J. Endod. 2007, 33, 1094–1097. [Google Scholar] [CrossRef]
- Ørstavik, D.; Nordahl, I.; Tibballs, J.E. Dimensional Change Following Setting of Root Canal Sealer Materials. Dent. Mater. 2001, 17, 512–519. [Google Scholar] [CrossRef]
- Silva, E.J.N.L.; Rosa, T.P.; Herrera, D.R.; Jacinto, R.C.; Gomes, B.P.F.A.; Zaia, A.A. Evaluation of Cytotoxicity and Physicochemical Properties of Calcium Silicate-Based Endodontic Sealer MTA Fillapex. J. Endod. 2013, 39, 274–277. [Google Scholar] [CrossRef]
- Antunes, T.B.M.; Janini, A.C.P.; Pelepenko, L.E.; Abuna, G.F.; Paiva, E.M.; Sinhoreti, M.A.C.; Raimundo, I.M.; Gomes, B.P.F.A.; de-Jesus-Soares, A.; Marciano, M.A. Heating Stability, Physical and Chemical Analysis of Calcium Silicate-Based Endodontic Sealers. Int. Endod. J. 2021, 54, 1175–1188. [Google Scholar] [CrossRef]
- Ha, W.; Kahler, B.; Walsh, L.J. Classification and Nomenclature of Commercial Hygroscopic Dental Cements. Eur. Endod. J. 2017, 2, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandolfi, M.G.; Taddei, P.; Siboni, F.; Modena, E.; Ciapetti, G.; Prati, C. Development of the Foremost Light-Curable Calcium-Silicate MTA Cement as Root-End in Oral Surgery. Chemical-Physical Properties, Bioactivity and Biological Behavior. Dent. Mater. 2011, 2, e134–e157. [Google Scholar] [CrossRef] [PubMed]
- Donnermeyer, D.; Bürklein, S.; Dammaschke, T.; Schäfer, E. Endodontic Sealers Based on Calcium Silicates: A Systematic Review. Odontology 2019, 107, 421–436. [Google Scholar] [CrossRef]
- Caceres, C.; Larrain, M.R.; Monsalve, M.; Peña-Bengoa, F. Dentinal Tubule Penetration and Adaptation of Bio-C Sealer and AH-Plus: A Comparative SEM Evaluation. Eur. Endod. J. 2021, 6, 216–220. [Google Scholar]
- Khullar, S.; Aggarwal, A.; Chhina, H.; Kaur, T.; Sharma, M.; Bala, D. Sealer Penetration in the Dentinal Tubules: A Confocal Laser Scanning Microscopy Study. Endodontology. 2021, 33, 92–96. [Google Scholar] [CrossRef]
- Kuçi, A.; Alaçam, T.; Yavaş, Ö.; Ergul-Ulger, Z.; Kayaoglu, G.; Kuci, A.; Alacam, T.; Yavas, O.; Ergul-Ulger, Z.; Kayaoglu, G. Sealer Penetration into Dentinal Tubules in the Presence or Absence of Smear Layer: A Confocal Laser Scanning Microscopic Study. J. Endod. 2014, 40, 1627–1631. [Google Scholar] [CrossRef]
- Majumdar, T.; Mukherjee, S.; Mazumdar, P. Microscopic Evaluation of Sealer Penetration and Interfacial Adaptation of Three Different Endodontic Sealers: An in Vitro Study. J. Conserv. Dent. 2021, 24, 435–439. [Google Scholar] [CrossRef]
- Najafzadeh, R.; Fazlyab, M.; Esnaashari, E. Comparison of Bioceramic and Epoxy Resin Sealers in Terms of Marginal Adaptation and Tubular Penetration Depth with Different Obturation Techniques in Premolar Teeth: A Scanning Electron Microscope and Confocal Laser Scanning Microscopy Study. J. Family Med. Prim. Care. 2022, 11, 1794. [Google Scholar]
- Candeiro, G.T.d.M.; Lavor, A.B.; Lima, I.T. de F.; Vasconcelos, B.C. de; Gomes, N.V.; Iglecias, E.F.; Gavini, G. Penetration of Bioceramic and Epoxy-Resin Endodontic Cements into Lateral Canals. Braz. Oral. Res. 2019, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, G.S.S.; Chan, D.Z.K.; Leong, J.Z.; Kan, I.Z.; Xuan, W.M.; Tee, V. Dentinal Tubule Penetration of Bioceramic-Based versus Epoxy Resin-Based Root Canal Sealers: A Systematic Review and Meta-Analysis. G. Ital. Endod. 2022, 36, 2. [Google Scholar]
- Guerrero-Gironés, J.; Forner, L.; Sanz, J.L.; Rodríguez-Lozano, F.J.; Ghilotti, J.; Llena, C.; Lozano, A.; Melo, M. Scientific Production on Silicate-Based Endodontic Materials: Evolution and Current State: A Bibliometric Analysis. Clin. Oral Investig. 2022, 26, 5611–5624. [Google Scholar] [CrossRef] [PubMed]
- De-Deus, G.; Souza, E.M.; Silva, E.J.N.L.; Belladonna, F.G.; Simões-Carvalho, M.; Cavalcante, D.M.; Versiani, M.A. A Critical Analysis of Research Methods and Experimental Models to Study Root Canal Fillings. Int. Endod. J. 2022, 55, 384–445. [Google Scholar] [CrossRef] [PubMed]
- Donnermeyer, D.; Schmidt, S.; Rohrbach, A.; Berlandi, J.; Bürklein, S.; Schäfer, E. Debunking the Concept of Dentinal Tubule Penetration of Endodontic Sealers: Sealer Staining with Rhodamine B Fluorescent Dye Is an Inadequate Method. Materials. 2021, 14, 3211. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Guidelines and Guidance Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [Green Version]
- Nagendrababu, V.; Murray, P.E.; Ordinola-Zapata, R.; Peters, O.A.; Rôças, I.N.; Siqueira, J.F.; Priya, E.; Jayaraman, J.; Siqueira, J.F., Jr.; Camilleri, J.; et al. PRILE 2021 Guidelines for Reporting Laboratory Studies in Endodontology: A Consensus-Based Development. Int. Endod. J. 2021, 54, 1482–1490. [Google Scholar] [CrossRef]
- Maharani, N.; Ricardo, S.; Ayu, D.; Putri, N. Differences in Penetration of Two Types of Calcium Silicate-Based Sealers with Ultrasonic Activation into Dentinal Tubules. Int. J. Pharm. Res. 2021, 9, 3339–3344. [Google Scholar]
- Alim Uysal, B.A.; Kotan, G.; Guneser, M.B.; Dincer, A.N.; Senturk, H.; Rafiqi, A.M. Investigation of the Effect of Different Chelation Solutions on Penetration of Resin-Based and Bioceramic Sealers with a Novel Method. Microsc. Res. Technol. 2021, 84, 1571–1576. [Google Scholar] [CrossRef]
- Eid, D.; Medioni, E.; De-Deus, G.; Khalil, I.; Naaman, A.; Zogheib, C. Impact of Warm Vertical Compaction on the Sealing Ability of Calcium Silicate-Based Sealers: A Confocal Microscopic Evaluation. Materials 2021, 14, 372. [Google Scholar] [CrossRef]
- Muedra, P.; Forner, L.; Lozano, A.; Sanz, J.L.; Rodríguez-Lozano, F.J.; Guerrero-Gironés, J.; Riccitiello, F.; Spagnuolo, G.; Llena, C. Could the Calcium Silicate-Based Sealer Presentation Form Influence Dentinal Sealing? An in Vitro Confocal Laser Study on Tubular Penetration. Materials 2021, 14, 659. [Google Scholar] [CrossRef]
- Reynolds, J.Z.; Augsburger, R.A.; Svoboda, K.K.H.; Jalali, P. Comparing Dentinal Tubule Penetration of Conventional and “HiFlow” Bioceramic Sealers with Resin-Based Sealer: An in Vitro Study. Aust. Endod. J. 2020, 46, 387–393. [Google Scholar] [CrossRef]
- Marissa, C.; Usman, M.; Suprastiwi, E.; Erdiani, A.; Meidyawati, R. Comparison of Dentinal Tubular Penetration of Three Bioceramic Sealers. Int. J. Appl. Pharm. 2020, 12, 23–26. [Google Scholar] [CrossRef]
- El Hachem, R.; Khalil, I.; Le Brun, G.; Pellen, F.; Le Jeune, B.; Daou, M.; El Osta, N.; Naaman, A.; Abboud, M. Dentinal Tubule Penetration of AH Plus, BC Sealer and a Novel Tricalcium Silicate Sealer: A Confocal Laser Scanning Microscopy Study. Clin. Oral. Investig. 2019, 23, 1871–1876. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Kim, B.-S.; Kim, Y.-M.; Lee, D.; Kim, S.-Y. The Penetration Ability of Calcium Silicate Root Canal Sealers into Dentinal Tubules Compared to Conventional Resin-Based Sealer: A Confocal Laser Scanning Microscopy Study. Materials 2019, 12, 531. [Google Scholar] [CrossRef] [Green Version]
- Aktemur Turker, S.; Uzunoglu, E.; Purali, N.; Aktemur Türker, S.; Uzunoğlu, E.; Purali, N. Evaluation of Dentinal Tubule Penetration Depth and Push-out Bond Strength of AH 26, BioRoot RCS, and MTA Plus Root Canal Sealers in Presence or Absence of Smear Layer. J. Dent. Res. Dent. Clin. Dent. Prospect. 2018, 12, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arikatla, S.K.; Chalasani, U.; Mandava, J.; Yelisela, R.K. Interfacial Adaptation and Penetration Depth of Bioceramic Endodontic Sealers. J. Conserv. Dent. 2018, 21, 373. [Google Scholar]
- McMichael, G.E.; Primus, C.M.; Opperman, L.A. Dentinal Tubule Penetration of Tricalcium Silicate Sealers. J. Endod. 2016, 42, 632–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akcay, M.; Arslan, H.; Durmus, N.; Mese, M.; Capar, I.D. Dentinal Tubule Penetration of AH Plus, IRoot SP, MTA Fillapex, and Guttaflow Bioseal Root Canal Sealers after Different Final Irrigation Procedures: A Confocal Microscopic Study. Lasers Surg. Med. 2016, 48, 70–76. [Google Scholar] [CrossRef]
- Reszka, P.; Nowicka, A.; Lipski, M.; Dura, W.; Droździk, A.; Woźniak, K. A Comparative Chemical Study of Calcium Silicate-Containing and Epoxy Resin-Based Root Canal Sealers. Biomed. Res. Int. 2016, 2016, 9808432. [Google Scholar] [CrossRef]
- Ha, J.-H.; Kim, H.-C.; Kyung Kim, Y.; Kwon, T.-Y. Materials An evaluation of wetting and adhesion of three bioceramic root canal sealers to intraradicular human dentin. Materials. 2018, 11, 1286. [Google Scholar] [CrossRef] [Green Version]
- Bidar, M.; Sadeghalhoseini, N.; Forghani, M.; Attaran, N. Effect of the Smear Layer on Apical Seals Produced by Two Calcium Silicate-Based Endodontic Sealers. J. Oral Sci. 2014, 56, 215–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoshino, R.A.; Delfino, M.M.; Silva, G.F.d.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Sasso-Cerri, E.; Cerri, P.S. Biocompatibility and Bioactive Potential of the NeoMTA Plus Endodontic Bioceramic-Based Sealer. Restor. Dent. Endod. 2021, 46, e4. [Google Scholar] [CrossRef] [PubMed]
- Zordan-Bronzel, C.L.; Esteves Torres, F.F.; Tanomaru-Filho, M.; Chávez-Andrade, G.M.; Bosso-Martelo, R.; Guerreiro-Tanomaru, J.M. Evaluation of Physicochemical Properties of a New Calcium Silicate-Based Sealer, Bio-C Sealer. J. Endod. 2019, 45, 1248–1252. [Google Scholar] [CrossRef] [PubMed]
- Guven, Y.; Tuna, E.B.; Dincol, M.E.; Aktoren, O. X-ray Diffraction Analysis of MTA-Plus, MTA-Angelus and DiaRoot BioAggregate. Eur. J. Dent. 2014, 8, 211–215. [Google Scholar] [CrossRef]
- Kok, D.; da Rosa, R.A.; Barreto, M.S.; Busanello, F.H.; Santini, M.F.; Pereira, J.R.; Só, M.V.R. Penetrability of AH plus and MTA Fillapex after Endodontic Treatment and Retreatment: A Confocal Laser Scanning Microscopy Study. Microsc. Res. Technol. 2014, 77, 467–471. [Google Scholar] [CrossRef]
- Versiani, M.A.; Carvalho, J.R.; Padilha, M.I.A.F.; Lacey, S.; Pascon, E.A.; Sousa-Neto, M.D. A Comparative Study of Physicochemical Properties of AH PlusTM and EpiphanyTM Root Canal Sealants. Int. Endod. J. 2006, 39, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Collado-González, M.; García-Bernal, D.; Oñate-Sánchez, R.E.; Ortolani-Seltenerich, P.S.; Lozano, A.; Forner, L.; Llena, C.; Rodríguez-Lozano, F.J. Biocompatibility of Three New Calcium Silicate-Based Endodontic Sealers on Human Periodontal Ligament Stem Cells. Int. Endod. J. 2017, 50, 875–884. [Google Scholar] [CrossRef]
- Bukhari, S.; Karabucak, B. The Antimicrobial Effect of Bioceramic Sealer on an 8-Week Matured Enterococcus Faecalis Biofilm Attached to Root Canal Dentinal Surface. J. Endod. 2019, 45, 1047–1052. [Google Scholar] [CrossRef]
- Camps, J.; Jeanneau, C.; el Ayachi, I.; Laurent, P.; About, I. Bioactivity of a Calcium Silicate-Based Endodontic Cement (BioRoot RCS): Interactions with Human Periodontal Ligament Cells In Vitro. J. Endod. 2015, 41, 1469–1473. [Google Scholar] [CrossRef]
- Ginebra, M.P.; Fernández, E.; de Maeyer, E.A.P.; Verbeeck, R.M.H.; Boltong, M.G.; Ginebra, J.; Driessens, F.C.M.; Planell, J.A. Setting Reaction and Hardening of an Apatitic Calcium Phosphate Cement. J. Dent. Res. 2016, 76, 905–912. [Google Scholar] [CrossRef]
- Balguerie, E.; van der Sluis, L.; Vallaeys, K.; Gurgel-Georgelin, M.; Diemer, F. Sealer Penetration and Adaptation in the Dentinal Tubules: A Scanning Electron Microscopic Study. J. Endod. 2011, 37, 1576–1579. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, M.; Felippe, M.C.S.; Felippe, W.; Alves, A.M.H.; Bortoluzzi, E.; Teixeira, C. Adhesive Interface and Bond Strength of Endodontic Sealers to Root Canal Dentine after Immersion in Phosphate-Buffered Saline. Microsc. Res. Technol. 2014, 77, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Hammad, M.; Qualtrough, A.; Silikas, N. Three-Dimensional Evaluation of Effectiveness of Hand and Rotary Instrumentation for Retreatment of Canals Filled with Different Materials. J. Endod. 2008, 34, 1370–1373. [Google Scholar] [CrossRef]
- Kokkas, A.B.; Boutsioukis, A.C.; Vassiliadis, L.P.; Stavrianos, C.K. The Influence of the Smear Layer on Dentinal Tubule Penetration Depth by Three Different Root Canal Sealers: An in vitro Study. J. Endod. 2004, 30, 100–102. [Google Scholar] [CrossRef]
- Tedesco, M.; Chain, M.C.; Bortoluzzi, E.A.; Garcia, L.d.F.R.; Alves, A.M.H.; Teixeira, C.S. Comparison of Two Observational Methods, Scanning Electron and Confocal Laser Scanning Microscopies, in the Adhesive Interface Analysis of Endodontic Sealers to Root Dentine. Clin. Oral Investig. 2018, 22, 2353–2361. [Google Scholar] [CrossRef] [PubMed]
- Jardine, A.P.; Rosa, R.A.d.; Santini, M.F.; Wagner, M.; Só, M.V.R.; Kuga, M.C.; Pereira, J.R.; Kopper, P.M.P. The Effect of Final Irrigation on the Penetrability of an Epoxy Resin-Based Sealer into Dentinal Tubules: A Confocal Microscopy Study. Clin. Oral Investig. 2016, 20, 117–123. [Google Scholar] [CrossRef]
- Teixeira, C.S.; Alfredo, E.; de Camargo Thomé, L.H.; Gariba-Silva, R.; Silva-Sousa, Y.T.C.; Sousa-Neto, M.D. Adhesion of an Endodontic Sealer to Dentin and Gutta-Percha: Shear and Push-out Bond Strength Measurements and SEM Analysis. J. Appl. Oral Sci. 2009, 17, 129–135. [Google Scholar] [CrossRef] [Green Version]
- Bitter, K.; Paris, S.; Mueller, J.; Neumann, K.; Kielbassa, A.M. Correlation of Scanning Electron and Confocal Laser Scanning Microscopic Analyses for Visualization of Dentin/Adhesive Interfaces in the Root Canal. J. Adhes. Dent. 2009, 11, 7–14. [Google Scholar]
- Jeong, J.W.; DeGraft-Johnson, A.; Dorn, S.O.; Di Fiore, P.M. Dentinal Tubule Penetration of a Calcium Silicate-Based Root Canal Sealer with Different Obturation Methods. J. Endod. 2017, 43, 633–637. [Google Scholar] [CrossRef]
- Patel, D.V.; Sherriff, M.; Ford, T.R.P.; Watson, T.F.; Mannocci, F. The Penetration of RealSeal Primer and Tubliseal into Root Canal Dentinal Tubules: A Confocal Microscopic Study. Int. Endod. J. 2007, 40, 67–71. [Google Scholar] [CrossRef]
- Thota, M.M.; Sudha, K.; Malini, D.L.; Madhavi, S.B. Effect of Different Irrigating Solutions on Depth of Penetration of Sealer into Dentinal Tubules: A Confocal Microscopic Study. Contemp. Clin. Dent. 2017, 8, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Al-Haddad, A.; Abu Kasim, N.H.; Che Ab Aziz, Z.A. Interfacial Adaptation and Thickness of Bioceramic-Based Root Canal Sealers. Dent. Mater. J. 2015, 34, 516–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coronas, V.S.; Villa, N.; Nascimento, A.L.d.; Duarte, P.H.M.; Rosa, R.A.d.; Só, M.V.R. Dentinal Tubule Penetration of a Calcium Silicate-Based Root Canal Sealer Using a Specific Calcium Fluorophore. Braz. Dent. J. 2020, 31, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, B.A.; Frota, L.M.A.; Taguatinga, D.T.; Vivan, R.R.; Camilleri, J.; Duarte, M.A.H.; Carvalho De Vasconcelos, B. Influence of Ultrasonic Agitation on Bond Strength, Marginal Adaptation, and Tooth Discoloration Provided by Three Coronary Barrier Endodontic Materials. Clin. Oral. Investig. 2019, 23, 4113–4122. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.M.; Shen, Y.; Zheng, W.; Li, L.; Zheng, Y.F.; Haapasalo, M. Physical Properties of 5 Root Canal Sealers. J. Endod. 2013, 39, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Abada, H.M.; Farag, A.M.; Alhadainy, H.A.; Darrag, A.M. Push-out Bond Strength of Different Root Canal Obturation Systems to Root Canal Dentin. Tanta Dent. J. 2015, 12, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Shokouhinejad, N.; Gorjestani, H.; Nasseh, A.A.; Hoseini, A.; Mohammadi, M.; Shamshiri, A.R. Push-out Bond Strength of Gutta-Percha with a New Bioceramic Sealer in the Presence or Absence of Smear Layer. Aust. Endod. J. 2013, 39, 102–106. [Google Scholar] [CrossRef]
- Ersahan, S.; Aydin, C. Dislocation Resistance of IRoot SP, a Calcium Silicate-Based Sealer, from Radicular Dentine. J. Endod. 2010, 36, 2000–2002. [Google Scholar] [CrossRef]
- Kossev, D.; Stefanov, V. Ceramics-based sealers as new alternative to currently used endodontic sealers. Roots. 2009, 1, 42–48. [Google Scholar]
- Qu, W.; Bai, W.; Liang, Y.H.; Gao, X.J. Influence of Warm Vertical Compaction Technique on Physical Properties of Root Canal Sealers. J. Endod. 2016, 42, 1829–1833. [Google Scholar] [CrossRef]
- Heran, J.; Khalid, S.; Albaaj, F.; Tomson, P.L.; Camilleri, J. The Single Cone Obturation Technique with a Modified Warm Filler. J. Dent. 2019, 89, 103181. [Google Scholar] [CrossRef]
- Fernández, R.; Restrepo, J.S.; Aristizábal, D.C.; Álvarez, L.G. Evaluation of the Filling Ability of Artificial Lateral Canals Using Calcium Silicate-Based and Epoxy Resin-Based Endodontic Sealers and Two Gutta-Percha Filling Techniques. Int. Endod. J. 2016, 49, 365–373. [Google Scholar] [CrossRef]
- DiVito, E.; Peters, O.A.; Olivi, G. Effectiveness of the Erbium:YAG Laser and New Design Radial and Stripped Tips in Removing the Smear Layer after Root Canal Instrumentation. Lasers Med. Sci. 2012, 27, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.; Pitt Ford, T.R.; Crum, L.A. Ultrasonic Debridement of Root Canals: Acoustic Streaming and Its Possible Role. J. Endod. 1987, 13, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, J.; Formosa, L.; Damidot, D. The Setting Characteristics of MTA Plus in Different Environmental Conditions. Int. Endod. J. 2013, 46, 831–840. [Google Scholar] [CrossRef]
- Duque, J.A.; Fernandes, S.L.; Bubola, J.P.; Duarte, M.A.H.; Camilleri, J.; Marciano, M.A. The Effect of Mixing Method on Tricalcium Silicate-Based Cement. Int. Endod. J. 2018, 51, 69–78. [Google Scholar] [CrossRef]
- Alcalde, M.P.; Bramante, C.M.; Vivan, R.R.; Amorso-Silva, P.A.; de Andrade, F.B.; Duarte, M.A.H. Intradentinal Antimicrobial Action and Filling Quality Promoted by Ultrasonic Agitation of Epoxy Resin-Based Sealer in Endodontic Obturation. J. Appl. Oral. Sci. 2017, 25, 641–649. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.K.; R’oris, A.; Barkis, D.; Wesselink, P.R. Prevalence and Extent of Long Oval Canals in the Apical Third. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 89, 739–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, M.P.J.; Love, R.M.; Chandler, N.P. An Evaluation of .06 Tapered Gutta-Percha Cones for Filling of .06 Taper Prepared Curved Root Canals. Int. Endod. J. 2005, 38, 87–96. [Google Scholar] [CrossRef]
- Bergmans, L.; Moisiadis, P.; de Munck, J.; Meerbeek, B.V.; Lambrechts, P. Effect of Polymerization Shrinkage on the Sealing Capacity of Resin Fillers for Endodontic Use. J. Adhes. Dent. 2005, 7, 321–329. [Google Scholar]
- Weis, M.V.; Parashos, P.; Messer, H.H. Effect of Obturation Technique on Sealer Cement Thickness and Dentinal Tubule Penetration. Int. Endod. J. 2004, 37, 653–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, A.A.; Chandler, N.P.; Hauman, C.; Siddiqui, A.Y.; Tompkins, G.R. The Butterfly Effect: An Investigation of Sectioned Roots. J. Endod. 2013, 39, 208–210. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.; Friedlander, L.; Chandler, N. Sealer Penetration and Adaptation in Root Canals with the Butterfly Effect. Aust. Endod. J. 2018, 44, 225–234. [Google Scholar] [CrossRef]
- Kara Tuncer, A.; Tuncer, S. Effect of Different Final Irrigation Solutions on Dentinal Tubule Penetration Depth and Percentage of Root Canal Sealer. J. Endod. 2012, 38, 860–863. [Google Scholar] [CrossRef] [PubMed]
- Mjör, I.A.; Smith, M.R.; Ferrari, M.; Mannocci, F. The Structure of Dentine in the Apical Region of Human Teeth. Int. Endod. J. 2001, 34, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Khaord, P.; Amin, A.; Shah, M.; Uthappa, R.; Raj, N.; Kachalia, T.; Kharod, H. Effectiveness of Different Irrigation Techniques on Smear Layer Removal in Apical Thirds of Mesial Root Canals of Permanent Mandibular First Molar: A Scanning Electron Microscopic Study. J. Conserv. Dent. 2015, 18, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abedi-Amin, A.; Luzi, A.; Giovarruscio, M.; Paolone, G.; Darvizeh, A.; Agulló, V.V.; Sauro, S. Innovative Root-End Filling Materials Based on Calcium-Silicates and Calcium-Phosphates. J. Mater. Sci. Mater. Med. 2017, 28, 31. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Database | Search Strategy | Findings |
|---|---|---|
| Scopus | #1 TITLE-ABS-KEY (bioceramic OR silicate) | 195,865 |
| #2 TITLE-ABS-KEY (sealer) | 6299 | |
| #3 TITLE-ABS-KEY (endod* OR “root canal”) | 89,699 | |
| #4 TITLE-ABS-KEY (penetrat* OR adhesion) | 1,089,172 | |
| #1 AND #2 AND #3 AND #4 | 158 | |
| Embase | #1 (bioceramic OR silicate) | 27,933 |
| #2 (sealer) | 4092 | |
| #3 (endod* OR “root canal”) | 91,791 | |
| #4 (penetrat* OR adhesion) | 670,462 | |
| #1 AND #2 AND #3 AND #4 | 110 | |
| PubMed | #1 All fields (bioceramic OR silicate) | 53,252 |
| #2 All fields (sealer) | 4287 | |
| #3 All fields (endod* OR “root canal”) | 89,526 | |
| #4 All fields (penetrat* OR adhesion) | 542,247 | |
| #1 AND #2 AND #3 AND #4 | 168 | |
| WOS | #1 Topic (bioceramic OR silicate) | 207,528 |
| #2 Topic (sealer) | 11,993 | |
| #3 Topic (endod* OR “root canal”) | 93,644 | |
| #4 Topic (penetrat* OR adhesion) | 1,456,666 | |
| #1 AND #2 AND #3 AND #4 | 225 | |
| Cochrane | #1 All text: (bioceramic OR silicate) | 452 |
| #2 All text: (sealer) | 578 | |
| #3 All text: (endod* OR “root canal”) | 5387 | |
| #4 All text: (penetrat* OR adhesion) | 13,938 | |
| #1 AND #2 AND #3 AND #4 | 19 |
| Sealer | Manufacturer | Composition | Studies in Which it Was Assessed |
|---|---|---|---|
| BioRoot RCS | Septodont, Saint Maur-des-Fosses, France | Powder: tricalcium silicate, zirconium dioxide, and povidone. Liquid: water, calcium chloride, and polycarboxylate [49] | (Muedra et al., 2021) [40], (Marissa et al., 2020) [42], (Kim et al., 2019) [44], (Aktemur Türker et al., 2018) [45] (Arikatla et al., 2018) [46]. |
| EndoSequence BC Sealer | Brasseler USA, Savannah, GA, USA | Zirconium oxide, calcium silicates, calcium phosphate monobasic, calcium hydroxide, filler, and thickening agents [50] | (Alim Uysal et al., 2021) [38], (Muedra et al., 2021) [40], (Reynolds et al., 2020) [41], (el Hachem et al., 2019) [43], (McMichael et al., 2016) [47]. |
| Endoseal MTA | Maruchi, Wonju, Korea | Calcium silicates, calcium aluminates, calcium aluminoferrite, calcium sulfates, radiopacifier, and thickening agents [50] | (Maharani et al., 2021) [37], (Kim et al., 2019) [44]. |
| iRoot SP | Innovative BioCeramix, Vancouver, Canada | zirconium oxide, calcium silicates, calcium phosphate monobasic, calcium hydroxide, filler, thickening agents [51] | (Maharani et al., 2021) [37], (Marissa et al., 2020) [42], (Akcay et al., 2016) [48]. |
| MTA Fillapex | Angelus, Londrina, Brazil | Paste A: salicylate resin, bismuth trioxide, fumed silica, Paste B: fumed silica, titanium dioxide, mineral trioxide aggregate, and base resin. [51] | (Alim Uysal et al., 2021) [38], (Marissa et al., 2020) [42], (McMichael et al., 2016) [47], (Akcay et al., 2016) [48]. |
| NeoMTA Plus | Avalon Biomed Inc., Bradenton, FL, USA | fine powdered tricalcium and dicalcium silicate, tantalite, calcium sulfate and silica [52] | (McMichael et al., 2016) [47]. |
| Bio-C Sealer | Angelus, Londrina, PR, Brazil | Calcium silicates, calcium aluminate, calcium oxide, zirconium oxide, iron oxide, silicon dioxide, dispersing agent [53] | (Eid et al., 2021) [39] |
| MTA plus | Avalon Biomed Inc. Bradenton, FL, USA | Bismuth oxide, portlandite, dicalcium silicate and tricalcium silicate, provided with either water or a gel for mixing [54] | (Aktemur Türker et al., 2018) [45], (Arikatla et al., 2018) [46]. |
| Endosequence HiFlow | Brasseler USA, Savannah, GA, USA | Zirconium oxide, calcium silicates, calcium phosphate monobasic, calcium hydroxide, filler, and thickening agents [50] | (Eid et al., 2021) [39], (Reynolds et al., 2020) [41]. |
| Author, Year | Sample Size | Sample Storage after Extraction, until Use | Distance from the Tip of K-File to the Apical Foramen | Instrumentation System/Last File Used | Irrigation Sequence |
|---|---|---|---|---|---|
| Maharani et al., 2021 [37] | 32 premolars | Not reported | 1 mm | ProTaper Next (Dentsply Maillefer, Ballaigues, Switzerland) /×4 (40.06) | 2.5% NaOCl, 5 mL 17% EDTA. |
| Alim Uysal et al., 2021 [38] | 84 mandibular premolars | Distilled water | 1 mm | Protaper Next (Dentsply Maillefer, Ballaigues, Switzerland) /×3 (30.07) | Four groups according to the final irrigation: A. 2 mL of 2.5% NaOCl after each file, with saline as the final irrigation solution. (Control group) B. 2 mL of 2.5% NaOCl after each file, with 17% EDTA for 1 min as the final irrigation solution. C. 2 mL of 2.5% NaOCl after each file, with 7% MA (maleic acid)for 1 min as the final irrigation solution. D. 2 mL of 2.5% NaOCl and 9% HEBP (etidronic acid) after each file, with 2.5% NaOCl and 9% HEBP for 1 min as the final irrigation solution. |
| Eid et al., 2021 [39] | 44 mandibular premolars | Not reported | 0.5 mm | ProTaper System (Dentsply Maillefer, Ballaigues, Switzerland)/f3 (30.09) | 10 mL 5.25% NaOCl, 10 mL of 17% EDTA, 3 mL of 5.25% NaOCl for 1 min, 10 mL of deionized water as a final flush. irrigants were sonically activated for 1 min using the Endoactivator system (Dentsply Maillefer, Ballaigues, Switzerland) with a 25/04 tip. |
| Muedra et al., 2021 [40] | 60 maxillary and mandibular premolars. | 100% humidity environment | 1 mm | Mtwo rotary system (VDW, Munich, Germany)/35.04 | 5.25% NaOCl 17% EDTA during 1 min 5 mL saline |
| Reynolds et al., 2020 [41] | 50 Incisors, canines, and premolars | Formalin | 1 mm. | EndoSequence (Brasseler, Sanannah, GA, USA) rotary files/40.06 | 1 mL of 6% NaOCl prior to instrumentation, 1 mL 6%NaOCl, 3 mL 17% EDTA for 1 min, 3 mL 6% NaOCl for 1 min, 5 mL saline for 1 min. |
| Marissa et al., 2020 [42] | 27 mandibular premolars | 0.9% NaCl solution | ±0.5 mm | ProTaper Next files (Dentsply, Ballaigues, Switzerland) /×3 (30.07) | 17% EDTA gel as a lubricant when changing instruments, 2 mL 2.5% NaOCl and activated with sonic instruments, 2 mL distilled water solution, 17% EDTA for 1 min, 2 mL distilled water. |
| el Hachem et al., 2019 [43] | 96 maxillary central incisors | distilled water | 0.5 mm | ProTaper (Dentsply Maillefer, Ballaigues, Switzerland)/F4 (40.06) | 10 mL 5.25% NaOCl 10 mL 17% EDTA, 3 mL 5.25% NaOCl for 3 min, 10 mL deionised water. |
| Kim et al. 2019 [44] | 60 premolars | Not reported | 0 mm | ProFile rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland)/ 40.06 | 2 mL of 2.5% NaOCl, 2 mL of 17% EDTA for 1 min, 10 mL of distilled water. |
| Aktemur Türker et al., 2018 [45] | 90 mandibular premolars | Not reported | 1 mm | ProTaper Universal file system (Dentsply, Maillefer, Ballaigues, Switzerland)/40.06 | 2.5% NaOCl during instrumentation specimens were randomly assigned to two groups according to the final irrigation: (n = 45): NaOCl (n = 45) = 3 mL of 17% EDTA for one minute, then 3 mL NaOCl followed by a final flush with 5 mL distilled water. |
| Arikatla et al., 2018 [46] | 60 mandibular premolars | saline, after disinfection with 0.5% chloramine-T solution | ProTaper rotary files (DenTsply Maillefer, Switzerland)/F3 (30.09) | 3% NaOCl, 2 mL of 17% EDTA for 1 min, 5 mL of distilled water. | |
| McMichael et al., 2016 [47] | 80 bicuspids, canines, and incisors | distilled water Roots were also stored in distilled water at room temperature after instrumentation until filling | 1 mm | (EndoSequence, Brasseler USA)/40.06 | 1 mL NaOCl, 3 mL 17% EDTA for 1 min, 3 mL 6% NaOCl for 1 min, 5 mL saline for 1 min. |
| Akcay et al., 2016 [48] | 156 mandibular premolars | Thymol solution for 48 h for disinfection, then stored in 48 C distilled water. | 1 mm | ProTaper Universal rotary instruments (Dentsply, Maillefer)/F4 (40.06) | 2 mL of 5% NaOCl 5 mL of 17% EDTA for 1 min 5 mL of 5% NaOCl for 1 min Specimens were randomly subdivided into three groups according to the final irrigation protocol (n=13): CI (Conventional needle irrigation), PIPS (Phophoton-induced-photoacoustic streaming activation), and PUI (passive ultrasonic irrigation). |
| Author, Date | Groups | Dye Used and Mixing Method | Sample Sectioning * | Observation Method | Outcome Measure | ||
|---|---|---|---|---|---|---|---|
| Sealer | Filling Method | n | |||||
| Maharani et al., 2021 [37] | iRoot SP without Ultrasonic activation | SC | 8 | 0.1% rhodamine B dye (Sigma-Aldrich, St. Louis, MO, USA) | 5 | CLSM | Mean maximum sealer penetration depth (μm) |
| iRoot SP with Ultrasonic activation | SC | 8 | |||||
| Endoseal MTA Without ultrasonic activation | SC | 8 | |||||
| Endoseal MTA with Ultrasonic activation | SC | 8 | |||||
| Alim Uysal et al., 2021 [38] | MTA Fillapex | SC | 28 | 0.01% rhodamine B (Bereket Kimya, Istanbul, Turkey) | 2, 6 and 10 | Cytation 5 Cell Imaging Multimode Reader and Gen5 software | Maximum sealer penetration depths (μm). mean sealer penetration depths (μm). |
| EndoSequence BC Sealer | SC | 28 | |||||
| Eid et al., 2021 [39] | Bio-C sealer | SC | 10 | 0.1% Rhodamine B dye (Sigma-Aldrich, St. Louis, MO, USA) | 1 and 5 | CLSM. | Mean maximum sealer penetration depth (μm). |
| Bio-C sealer | WVC | 10 | |||||
| HiFlow | SC | 10 | |||||
| HiFlow | WVC | 10 | |||||
| Control group—filled with either HiFlow sealer or Bio-C without the fluorescent agent | 2 | ||||||
| Control group— Not obturated | 2 | ||||||
| Muedra et al., 2021 [40] | EndoSequence BC Sealer | SC | 20 | 0.1% Rhodamine B, C28H31ClN2O3, (Panreac Químicas S.A.U. Casteller del Vallès, BCN, Spain). | 3, 5, and 8 (Samples were stored in a light-free environment to avoid a previous exposure of the fluorochrome to light before it was viewed under CLSM.) | CLSM | Median Tubular Penetration Depth. Median Percentage of Perimeter Penetrated. |
| BioRoot RCS | SC | 20 | |||||
| Control Group: AH Plus | SC | 20 | |||||
| Reynolds et al., 2020 [41] | Control group: 2Seal easymiX, | WVC | 10 | rhodamine B fluorescent dye (Sigma-Aldrich, St. Louis, MO, USA) | 3 and 6 | CLSM To evaluate the maximum depth of sealer penetration, the distance between the deepest point of sealer penetration to the root canal wall was measured using imageJ software. | Median maximum sealer penetration depth. Median percentage of sealer penetration. |
| EndoSequence BC | SC | 10 | |||||
| EndoSequence BC | WVC | 10 | |||||
| EndoSequence BC hiflow | SC | 10 | |||||
| EndoSequence BC hiflow | WVC | 10 | |||||
| Marissa et al., 2020 [42] | IRoot® SP | SC | 9 | 5 | SEM | Mean maximum sealer penetration depth (μm) | |
| MTA® Fillapex | SC | 9 | |||||
| BioRoot™ RCS | SC | 9 | |||||
| el Hachem et al., 2019 [43] | EndoSequence BC Sealer | SC | 32 | 0.1% rhodamine B (Sigma-Aldrich, St. Louis, MO, USA) | 1 and 5 | CLSM | Maximum sealer penetration depth (μm). Mean sealer penetration depth (μm). |
| new experimental novel tricalcium silicate (NTS)-based sealer | SC | 32 | |||||
| Kim et al., 2019 [44] | BioRoot RCS | SC | 20 | 0.1% rhodamine B dye (Sigma-Aldrich, St. Louis, MO, USA) | 3, 5 and7 | CLSM | maximum sealer penetration depth (μm). mean fluorescence intensity. sum fluorescence intensity |
| Endoseal MTA | SC | 20 | |||||
| Aktemur Türker et al., 2018 [45] | BioRoot RCS | SC | 30 | 0.1% rhodamine B dye (Sigma Aldrich Co., St Louis, MO, USA) | Mid third | CLSM | Mean of Push-out bond strength values. Sealer mean penetration depth (mm) Penetration mean percentage % |
| MTA Plus | SC | 30 | |||||
| Arikatla et al., 2018 [46] | MTA plus | LC | 10 | isothiocyanate fluorescent 0.1% Rhodamine dye (Macsen Labs Pvt Ltd., Rajasthan) | 3 and 6 | CLSM. | sealer mean penetration depth (μm). dentin sealer interfacial gaps (μm). |
| BioRoot RCS | LC | 10 | |||||
| McMichael et al., 2016 [47] | EndoSequence BC sealer | SC | 10 | Rhodamine dye (n/s) | 1 and 5 | CLSM | Maximum sealer penetration depth (μm). Percentage of sealer penetration % |
| WVC | 10 | ||||||
| MTA Fillapex | SC | 10 | |||||
| WVC | 10 | ||||||
| NeoMTA Plus | SC | 10 | |||||
| WVC | 10 | ||||||
| QuickSet2 | SC | 10 | |||||
| WVC | 10 | ||||||
| Akcay et al., 2016 [48] | iRoot SP | SC | 39 | 0.1% fluorescent rhodamine B isothiocyanate (n/s) | 2, 5, and 8 | CLSM | Mean total dentinal tubule penetration area values (mm2). |
| MTA Fillapex | SC | 39 | |||||
| Author, Year | Distance from Apex (mm) | Sealer Penetration Depth | p Value |
|---|---|---|---|
| Alim Uysal et al., 2021 [38] | 2 mm | Maleic acid for final irrigation > EDTA and HEBP for final irrigation (in all sealers: MTA Fillapex, EndoSequence BC) | 0.013 |
| 6 mm | |||
| 10 mm | |||
| Eid et al., 2021 [39] | 1 mm | (endosequence BC HiFlow, Bio-C sealer): WVC > SCO | 0.011 |
| 5 mm | (endosequence BC HiFlow, Bio-C sealer): WVC > SCO | 0.034 | |
| Muedra et al., 2021 [40] | 3 mm | ||
| 5 mm | EndoSequence > BioRoot RCS | <0.05 | |
| 8 mm | EndoSequence > BioRoot RCS | <0.05 | |
| Marissa et al., 2020 [42] | 5 mm | MTA Fillapex ˃ IRoot® SP ˃ BioRoot™ RCS | <0.001 |
| Kim et al., 2019 [44] | 3 mm | ||
| 5 mm | BioRoot RCS > Endoseal MTA. | <0.017 | |
| 7 mm | BioRoot RCS > Endoseal MTA. | <0.017 | |
| Aktemur Türker et al., 2018 [45] | Mid third | Smear layer preserved: MTA Plus > BioRoot RCS. Smear layer removed: MTA Plus > BioRoot RCS. | <0.05 |
| McMichael et al., 2016 [47] | 1 mm | MTA Fillapex with WVC technique > MTA Fillapex with SC technique. EndoSequence with WVC technique > EndoSequence with SC technique. | <0.0125 |
| 5 mm | Endodecuence Sealer, MTA Fillapex > QuickSet2 (when used with the WVC technique compared with the SC technique). | <0.0125 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashkar, I.; Sanz, J.L.; Forner, L.; Melo, M. Calcium Silicate-Based Sealer Dentinal Tubule Penetration—A Systematic Review of In Vitro Studies. Materials 2023, 16, 2734. https://doi.org/10.3390/ma16072734
Ashkar I, Sanz JL, Forner L, Melo M. Calcium Silicate-Based Sealer Dentinal Tubule Penetration—A Systematic Review of In Vitro Studies. Materials. 2023; 16(7):2734. https://doi.org/10.3390/ma16072734
Chicago/Turabian StyleAshkar, Israa, José Luis Sanz, Leopoldo Forner, and María Melo. 2023. "Calcium Silicate-Based Sealer Dentinal Tubule Penetration—A Systematic Review of In Vitro Studies" Materials 16, no. 7: 2734. https://doi.org/10.3390/ma16072734