
Can Abutment with Novel Superlattice CrN/NbN Coatings Influence Peri-Implant Tissue Health and Implant Survival Rate Compared to Machined Abutment? 6-Month Results from a Multi-Center Split-Mouth Randomized Control Trial

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients Selection
2.3. Surgical Appointments
2.4. Clinical Outcomes
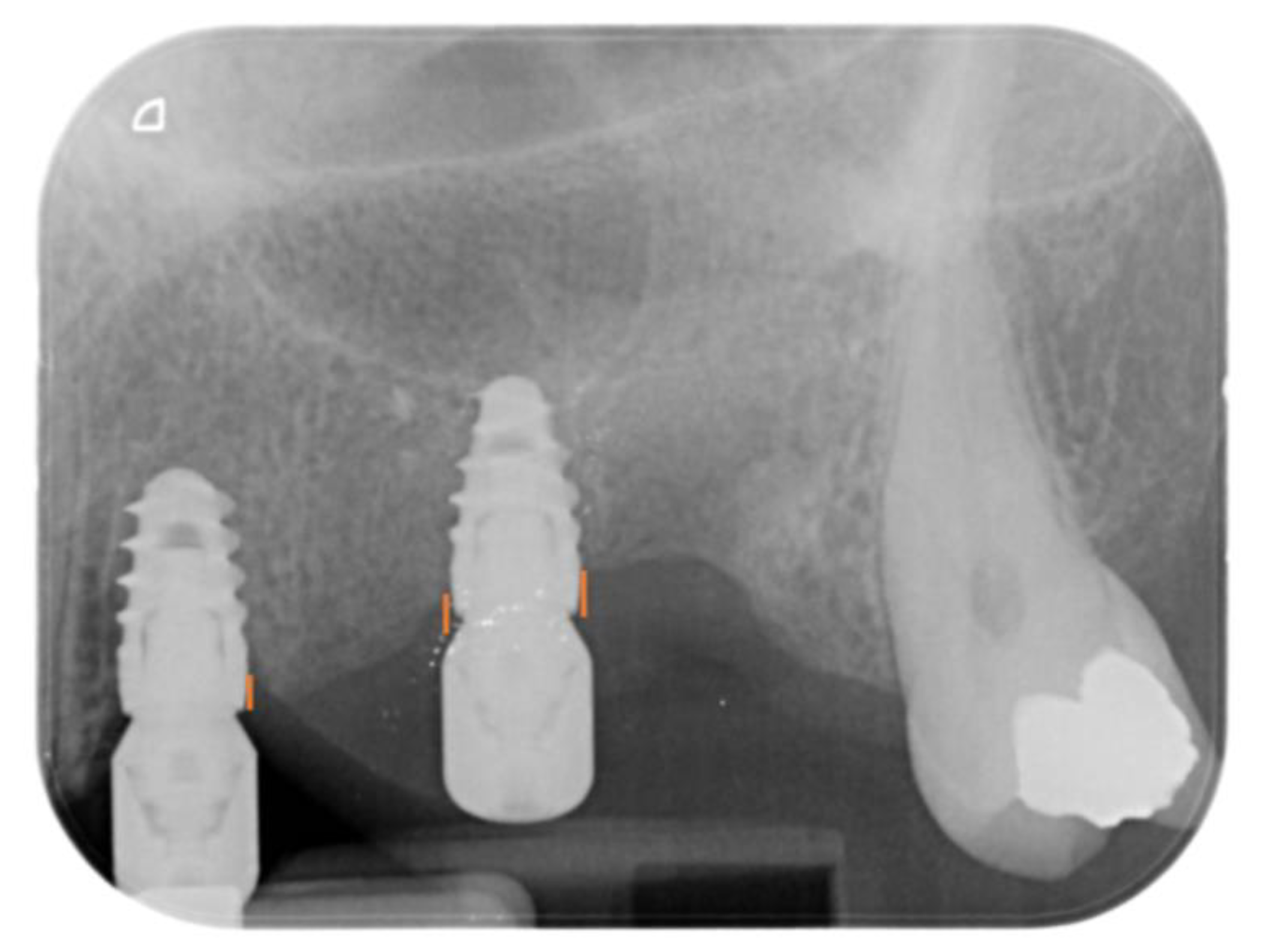
- Marginal bone loss (MBL), evaluated at both the mesial and distal aspects of the implants immediately after surgery (T0) and at 6 (T6) months after surgery. MBL was evaluated on intraoral apical X-rays by measuring the distance between the implant-abutment interface and the most coronal aspect of the bone (Figure 5) using Imagej software. The known length of the implant was used to set the mm scale. The difference between T6 and T0 resulted in the MBL.
- Peri-implant soft tissue parameters, including peri-implant probing depth (PPD), plaque index (PI), and bleeding index (BI). PPD was evaluated using a HuFriedy PCPUNC 15 probe (HuFriedy, Chicago, IL, USA) at the mesio-buccal, buccal, disto-buccal, mesio-lingual, lingual, and disto-lingual aspect of each implant. PI and BI were evaluated as number of surfaces (the mesio-buccal, buccal, disto-buccal, mesio-lingual, lingual, and disto-lingual) presenting plaque or bleeding on probing. All the parameters were evaluated at T6.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lindquist, L.W.; Carlsson, G.E.; Jemt, T. A prospective 15-year follow-up study of mandibular fixed prostheses supported by osseointegrated implants. Clinical results and marginal bone loss. Clin. Oral. Implant. Res. 1996, 7, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Pera, P.; Menini, M.; Pesce, P.; Bevilacqua, M.; Pera, F.; Tealdo, T. Immediate Versus Delayed Loading of Dental Implants Supporting Fixed Full-Arch Maxillary Prostheses: A 10-year Follow-up Report. Int. J. Prosthodont. 2019, 32, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors Influencing Early Dental Implant Failures. J. Dent. Res. 2016, 95, 995–1002. [Google Scholar] [CrossRef]
- Menini, M.; Pesce, P.; Baldi, D.; Coronel Vargas, G.; Pera, P.; Izzotti, A. Prediction of Titanium Implant Success by Analysis of microRNA Expression in Peri-Implant Tissue. A 5-Year Follow-Up Study. J. Clin. Med. 2019, 8, 888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortensi, L.; Ortensi, M.; Minghelli, A.; Grande, F. Implant-Supported Prosthetic Therapy of an Edentulous Patient: Clinical and Technical Aspects. Prosthesis 2020, 2, 140–152. [Google Scholar] [CrossRef]
- Menini, M.; Setti, P.; Pera, P.; Pera, F.; Pesce, P. Peri-implant Tissue Health and Bone Resorption in Patients with Immediately Loaded, Implant-Supported, Full-Arch Prostheses. Int. J. Prosthodont. 2018, 31, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Conserva, E.; Menini, M.; Ravera, G.; Pera, P. The role of surface implant treatments on the biological behavior of SaOS-2 osteoblast-like cells. An in vitro comparative study. Clin. Oral. Implant. Res. 2013, 24, 880–889. [Google Scholar] [CrossRef] [PubMed]
- Mussano, F.; Genova, T.; Serra, F.G.; Carossa, M.; Munaron, L.; Carossa, S. Nano-Pore Size of Alumina Affects Osteoblastic Response. Int. J. Mol. Sci. 2018, 19, 528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wennerberg, A.; Albrektsson, T. Effects of titanium surface topography on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20, 172–184. [Google Scholar] [CrossRef]
- Alovisi, M.; Carossa, M.; Mandras, N.; Roana, J.; Costalonga, M.; Cavallo, L.; Pira, E.; Putzu, M.G.; Bosio, D.; Roato, I.; et al. Disinfection and Biocompatibility of Titanium Surfaces Treated with Glycine Powder Airflow and Triple Antibiotic Mixture: An In Vitro Study. Materials 2022, 15, 4850. [Google Scholar] [CrossRef]
- Natali, A.N.; Gasparetto, A.; Carniel, E.L.; Pavan, P.G.; Fabbro, S. Interaction phenomena between oral implants and bone tissue in single and multiple implant frames under occlusal loads and misfit conditions: A numerical approach. J. Biomed. Mater. Res. B Appl. Biomater. 2007, 83, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Koutouzis, T.; Koutouzis, G.; Gadella, H.; Neiva, R. The Effect of Healing Abutment Reconnection and Disconnection on Soft and Hard Peri-implant Tissues: A Short-Term Randomized Controlled Clinical Trial. Int. J. Oral Maxillofac. Implant. 2013, 28, 807–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozzan, M.C.; Grande, F.; Mochi Zamperoli, E.; Tesini, F.; Carossa, M.; Catapano, S. Assessment of Preload Loss after Cyclic Loading in the OT Bridge System in an “All-on-Four” Rehabilitation Model in the Absence of One and Two Prosthesis Screws. Materials 2022, 15, 1582. [Google Scholar] [CrossRef] [PubMed]
- Suárez-López Del Amo, F.; Lin, G.H.; Monje, A.; Galindo-Moreno, P.; Wang, H.L. Influence of Soft Tissue Thickness on Peri-Implant Marginal Bone Loss: A Systematic Review and Meta-Analysis. J. Periodontol. 2016, 87, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Welander, M.; Abrahamsson, I.; Berglundh, T. The mucosal barrier at implant abutments of different materials. Clin. Oral. Implant. Res. 2008, 19, 635–641. [Google Scholar]
- Canullo, L.; Menini, M.; Santori, G.; Rakic, M.; Sculean, A.; Pesce, P. Titanium abutment surface modifications and peri-implant tissue behavior: A systematic review and meta-analysis. Clin. Oral. Investig. 2020, 24, 1113–1124. [Google Scholar] [CrossRef]
- Menini, M.; Pera, F.; Bagnasco, F.; Delucchi, F.; Morganti, E.; Pesce, P. Morphological and chemical characterization of titanium and zirconia dental implants with different macro- and micro-structure. Appl. Sci. 2020, 10, 7520. [Google Scholar] [CrossRef]
- Conserva, E.; Lanuti, A.; Menini, M. Cell behavior related to implant surfaces with different microstructure and chemical composition: An in vitro analysis. Int. J. Oral. Maxillofac. Implant. 2010, 25, 1099–1107. [Google Scholar]
- Mussano, F.; Genova, T.; Laurenti, M.; Zicola, E.; Munaron, L.; Rivolo, P.; Mandracci, P.; Carossa, S. Early response of fibroblasts and epithelial cells to pink-shaded anodized dental implant abut- ments: An in vitro study. Int. J. Oral. Maxillofac. Implant. 2018, 33, 571–579. [Google Scholar] [CrossRef]
- Dorkhan, M.; Yücel-Lindberg, T.; Hall, J.; Svensäter, G.; Davies, J.R. Adherence of human oral keratinocytes and gingival fibroblasts to nano- structured titanium surfaces. BMC Oral. Health 2014, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Meredith, D.O.; Eschbach, L.; Wood, M.A.; Riehle, M.O.; Curtis, A.S.; Richards, R.G. Human fibroblast reactions to standard and electropolished titanium and Ti-6Al-7Nb, and electropolished stainless steel. J. Biomed. Mater. Res. 2005, 75, 541–555. [Google Scholar] [CrossRef] [PubMed]
- Duske, K.; Koban, I.; Kindel, E.; Schröder, K.; Nebe, B.; Holtfreter, B.; Jablonowski, L.; Weltmann, K.D.; Kocher, T. Atmospheric plasma enhances wettability and cell spreading on dental implant metals. J. Clin. Periodontol. 2012, 39, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Pesce, P.; Menini, M.; Santori, G.; De Giovanni, E.; Bagnasco, F.; Canullo, L. Photo and Plasma activation of dental implant titanium surfaces. A systematic review with meta-analysis of pre-clinical studies. J. Clin. Med. 2020, 9, 2817. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Genova, T.; Pesce, P.; Nakajima, Y.; Yonezawa, D.; Mussano, F. Surface bio-functionalization using plasma of Argon could alter microbiological and topographic surface analysis of dental implants? Ann. Anat. 2020, 230, 151489. [Google Scholar] [CrossRef]
- Corvino, E.; Pesce, P.; Mura, R.; Marcano, E.; Canullo, L. Influence of Modified Titanium Abutment Surface on Peri-implant Soft Tissue Behavior: A Systematic Review of In Vitro Studies. Int. J. Oral. Maxillofac. Implant. 2020, 35, 503–519. [Google Scholar] [CrossRef]
- Carossa, M.; Cavagnetto, D.; Mancini, F.; Mosca Balma, A.; Mussano, F. Plasma of Argon Treatment of the Implant Surface, Systematic Review of In Vitro Studies. Biomolecules 2022, 12, 1219. [Google Scholar] [CrossRef]
- Pesce, P.; Menini, M.; Tommasato, G.; Patini, R.; Canullo, L. Influence of modified titanium abutment surface on peri-implant soft tissue behaviour: A systematic review of histological findings. Int. J. Oral. Implantol. 2019, 12, 419–429. [Google Scholar]
- Hovsepian, P.E.; Ehiasarian, A.P.; Purandare, Y.; Sugumaran, A.A.; Marriott, T.; Khan, I. Development of superlattice CrN/NbN coatings for joint replacements deposited by high power impulse magnetron sputtering. J. Mater. Sci. Mater. Med. 2016, 27, 147. [Google Scholar] [CrossRef]
- Skjöldebrand, C.; Tipper, J.L.; Hatto, P.; Bryant, M.; Hall, R.M.; Persson, C. Current status and future potential of wear-resistant coatings and articulating surfaces for hip and knee implants. Mater. Today Bio. 2022, 30, 100270. [Google Scholar] [CrossRef]
- Huang, W.; Zalnezhad, E.; Musharavati, F.; Jahanshahi, P. Investigation of the tribological and biomechanical properties of CrAlTiN and CrN/NbN coatings on SST 304. Ceram. Int. 2017, 43, 7992–8003. [Google Scholar] [CrossRef]
- Canullo, L.; Troiano, G.; Sbricoli, L.; Guazzo, R.; Laino, L.; Caiazzo, A.; Pesce, P. The Use of Antibiotics in Implant Therapy: A Systematic Review and Meta-Analysis with Trial Sequential Analysis on Early Implant Failure. Int. J. Oral. Maxillofac. Implant. 2020, 35, 485–494. [Google Scholar] [CrossRef] [PubMed]
- Caiazzo, A.; Canullo, L.; Consensus Meeting Group; Pesce, P. Consensus Report by the Italian Academy of Osseointegration on the Use of Antibiotics and Antiseptic Agents in Implant Surgery. Int. J. Oral. Maxillofac. Implant. 2021, 36, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Lazzara, R.J.; Porter, S.S. Platform switching: A new concept in implant dentistry for controlling postrestorative crestal bone levels. Int. J. Periodont. Restor. Dent. 2006, 26, 9–17. [Google Scholar]
- Menini, M.; Pesce, P.; Delucchi, F.; Ambrogio, G.; Canepa, C.; Carossa, M.; Pera, F. One-stage versus two-stage technique using two splinted extra-short implants: A multicentric split-mouth study with a one-year follow-up. Clin. Implant. Dent Relat Res. 2022, 24, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Abi-Aad, H.; Daher, F.; Dimassi, H.; Cordioli, G.; Majzoub, Z. Immediate vs conventional loading of variable-thread tapered implants supporting three- to four-unit fixed partial dentures in the posterior maxilla: 1-year interim results of a split-mouth randomised controlled trial. Eur. J. Oral. Implantol. 2018, 11, 337–350. [Google Scholar] [PubMed]
- Tomlinson, M.; Lyon, S.B.; Hovsepian, P.; Munz, W.D. Corrosion performance of CrN/NbN superlattice coatings deposited by the combined cathodic arc/unbalanced magnetron technique. Vacuum 1999, 53, 117–121. [Google Scholar] [CrossRef]
- Reinhard, C.; Ehiasarian, A.P.; Hovsepian, P.E. CrN/NbN superlattice structured coatings with enhanced corrosion resistance achieved by high power impulse magnetron sputtering interface pre-treatment. Thin Solid Films. 2007, 515, 3685–3692. [Google Scholar] [CrossRef]
- Purandare, Y.P.; Ehiasarian, A.P.; Stack, M.M.; Hovsepian, P.E. CrN/NbN coatings deposited by HIPIMS: A preliminary study of erosion-corrosion performance. Surf. Coat. Technol. 2010, 204, 1158–1162. [Google Scholar] [CrossRef] [Green Version]
- Stack, M.M.; Purandare, Y.; Hovsepian, P. Impact angle effects on the erosion-corrosion of superlattice CrN/NbN PVD coatings. Surf. Coat. Technol. 2004, 188–189, 556–565. [Google Scholar] [CrossRef]
- Canullo, L.; Annunziata, M.; Pesce, P.; Tommasato, G.; Nastri, L.; Guida, L. Influence of abutment material and modifications on peri-implant soft-tissue attachment: A systematic review and meta-analysis of histological animal studies. J. Prosthet. Dent. 2021, 125, 426–436. [Google Scholar] [CrossRef]
- Canullo, L.; Götz, W. Peri-implant hard tissue response to glow-discharged abutments: Prospective study. Preliminary radiological results. Ann. Anat. 2012, 194, 529–532. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Peñarrocha, D.; Clementini, M.; Iannello, G.; Micarelli, C. Impact of plasma of argon cleaning treatment on implant abutments in patients with a history of periodontal disease and thin biotype: Radiographic results at 24-month follow-up of a RCT. Clin. Oral Implant. Res. 2015, 26, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Zitzmann, N.U.; Berglundh, T.; Linder, E.; Wennerberg, A.; Lindhe, J. The mucosal attachment to titanium implants with different surface characteristics: An experimental study in dogs. J. Clin. Periodontol. 2002, 29, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Hermann, J.S.; Jones, A.A.; Bakaeen, L.G.; Buser, D.; Schoolfield, J.D.; Cochran, D.L. Influence of a machined collar on crestal bone changes around titanium implants: A histometric study in the canine mandible. J. Periodontol. 2011, 82, 1329–1338. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Mihatovic, I.; Becker, J.; Bormann, K.H.; Keeve, P.L.; Friedmann, A. Histological evaluation of different abutments in the posterior maxilla and mandible: An experimental study in humans. J. Clin. Periodontol. 2013, 40, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Martín, I.; Sanz-Sánchez, I.; Carrillo de Albornoz, A.; Figuero, E.; Sanz, M. Effects of modified abutment characteristics on peri-implant soft tissue health: A systematic review and meta-analysis. Clin. Oral. Implant. Res. 2018, 29, 118–129. [Google Scholar] [CrossRef]
- Tallarico, M.; Canullo, L.; Caneva, M.; Ozcam, M. Microbial colonization of the implant-abutment interface and its possible influence on the development of peri-implantitis: A systematic review with meta-analysis. J. Prosthodont. Res. 2017, 61, 233–241. [Google Scholar] [CrossRef] [Green Version]
- Carossa, M.; Alovisi, M.; Crupi, A.; Ambrogio, G.; Pera, F. Full-Arch Rehabilitation Using Trans-Mucosal Tissue-Level Implants with and without Implant-Abutment Units: A Case Report. Dent. J. 2022, 10, 116. [Google Scholar] [CrossRef]
- Canullo, L.; Masucci, L.; Quaranta, G.; Patini, R.; Caponio, V.C.A.; Pesce, P.; Ravidà, A.; Penarrocha-Oltra, D.; Penarrocha-Diago, M. Culturomic and quantitative real-time-polymerase chain reaction analyses for early contamination of abutments with different surfaces: A randomized clinical trial. Clin. Implant. Dent. Relat Res. 2021, 23, 568–578. [Google Scholar] [CrossRef]
- Canullo, L.; Penarrocha, D.; Pesce, P.; Zarauz, C.; Lattanzio, R.; Penarrocha, M.; Iezzi, G. Soft tissue integration of different abutment surfaces: An experimental study with histological analysis. Clin. Oral. Implant. Res. 2021, 32, 928–940. [Google Scholar] [CrossRef]
- Catapano, S.; Ferrari, M.; Mobilio, N.; Montanari, M.; Corsalini, M.; Grande, F. Comparative Analysis of the Stability of Prosthetic Screws under Cyclic Loading in Implant Prosthodontics: An In Vitro Study. Appl. Sci. 2021, 11, 622. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Patients (n = 20) |
|---|---|
| Age (mean ± SD) | 40 ± 13 |
| Male | 35% (n = 7) |
| Female | 65% (n = 13) |
| Implants (n = 40) | |
| Length 13 mm | 7.5% (n =3) |
| Length 10 mm | 72.5% (n = 29) |
| Length 8.5 mm | 15% (n = 6) |
| Length (mm, mean ± SD) | 10 ± 0.45 |
| Diameter 4.3 mm | 100% (n = 40) |
| Variable | Coefficients | p Value |
|---|---|---|
| Mesial MBL | −0.133 | 0.419 |
| Distal MBL | −0.092 | 0.579 |
| PPD | 0.036 | 0.826 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pera, F.; Menini, M.; Alovisi, M.; Crupi, A.; Ambrogio, G.; Asero, S.; Marchetti, C.; Canepa, C.; Merlini, L.; Pesce, P.; et al. Can Abutment with Novel Superlattice CrN/NbN Coatings Influence Peri-Implant Tissue Health and Implant Survival Rate Compared to Machined Abutment? 6-Month Results from a Multi-Center Split-Mouth Randomized Control Trial. Materials 2023, 16, 246. https://doi.org/10.3390/ma16010246
Pera F, Menini M, Alovisi M, Crupi A, Ambrogio G, Asero S, Marchetti C, Canepa C, Merlini L, Pesce P, et al. Can Abutment with Novel Superlattice CrN/NbN Coatings Influence Peri-Implant Tissue Health and Implant Survival Rate Compared to Machined Abutment? 6-Month Results from a Multi-Center Split-Mouth Randomized Control Trial. Materials. 2023; 16(1):246. https://doi.org/10.3390/ma16010246
Chicago/Turabian StylePera, Francesco, Maria Menini, Mario Alovisi, Armando Crupi, Giulia Ambrogio, Sofia Asero, Carlotta Marchetti, Camilla Canepa, Laura Merlini, Paolo Pesce, and et al. 2023. "Can Abutment with Novel Superlattice CrN/NbN Coatings Influence Peri-Implant Tissue Health and Implant Survival Rate Compared to Machined Abutment? 6-Month Results from a Multi-Center Split-Mouth Randomized Control Trial" Materials 16, no. 1: 246. https://doi.org/10.3390/ma16010246