
3D-Printed Double-Helical Biodegradable Iron Suture Anchor: A Rabbit Rotator Cuff Tear Model

 ,
,  ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
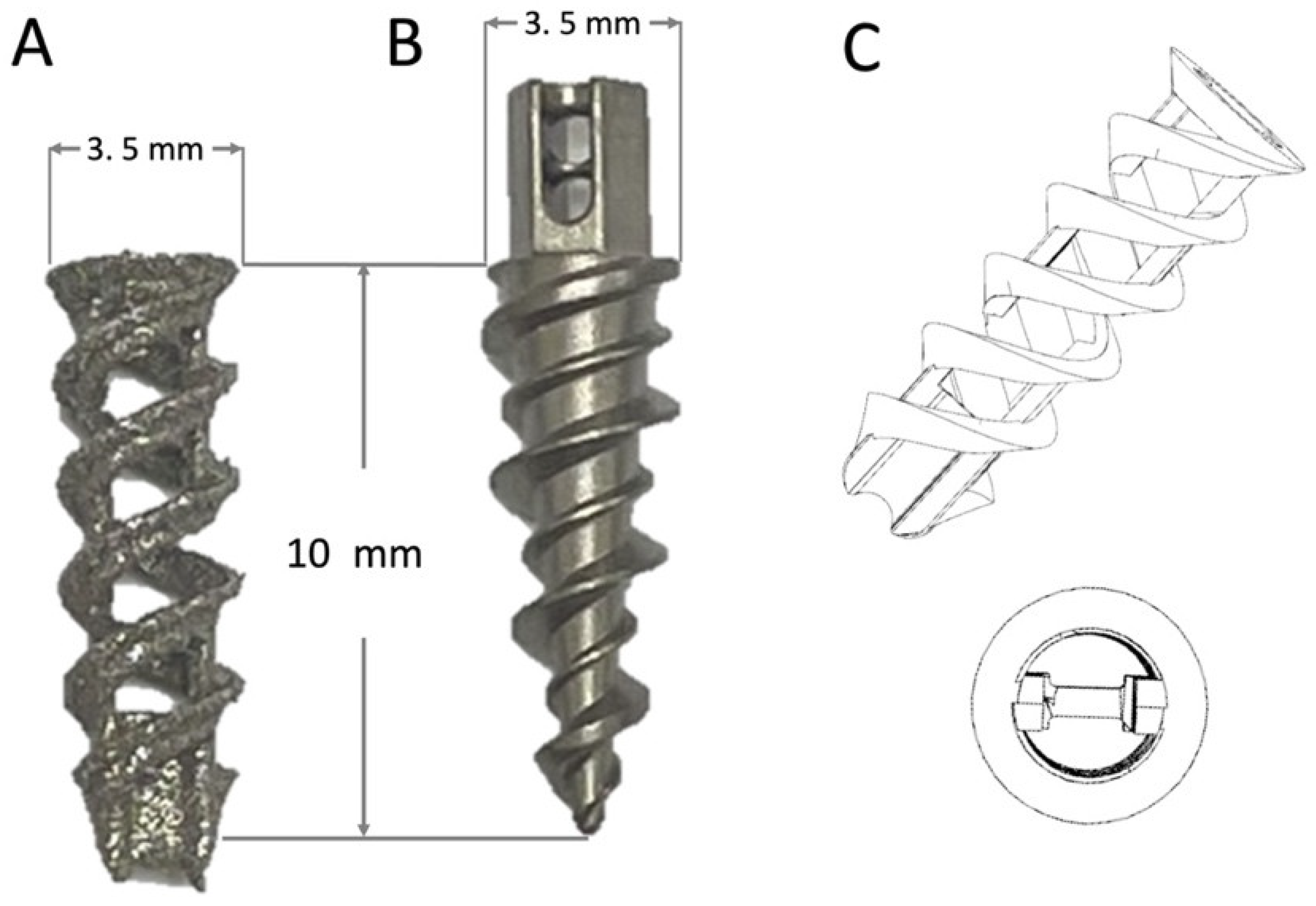
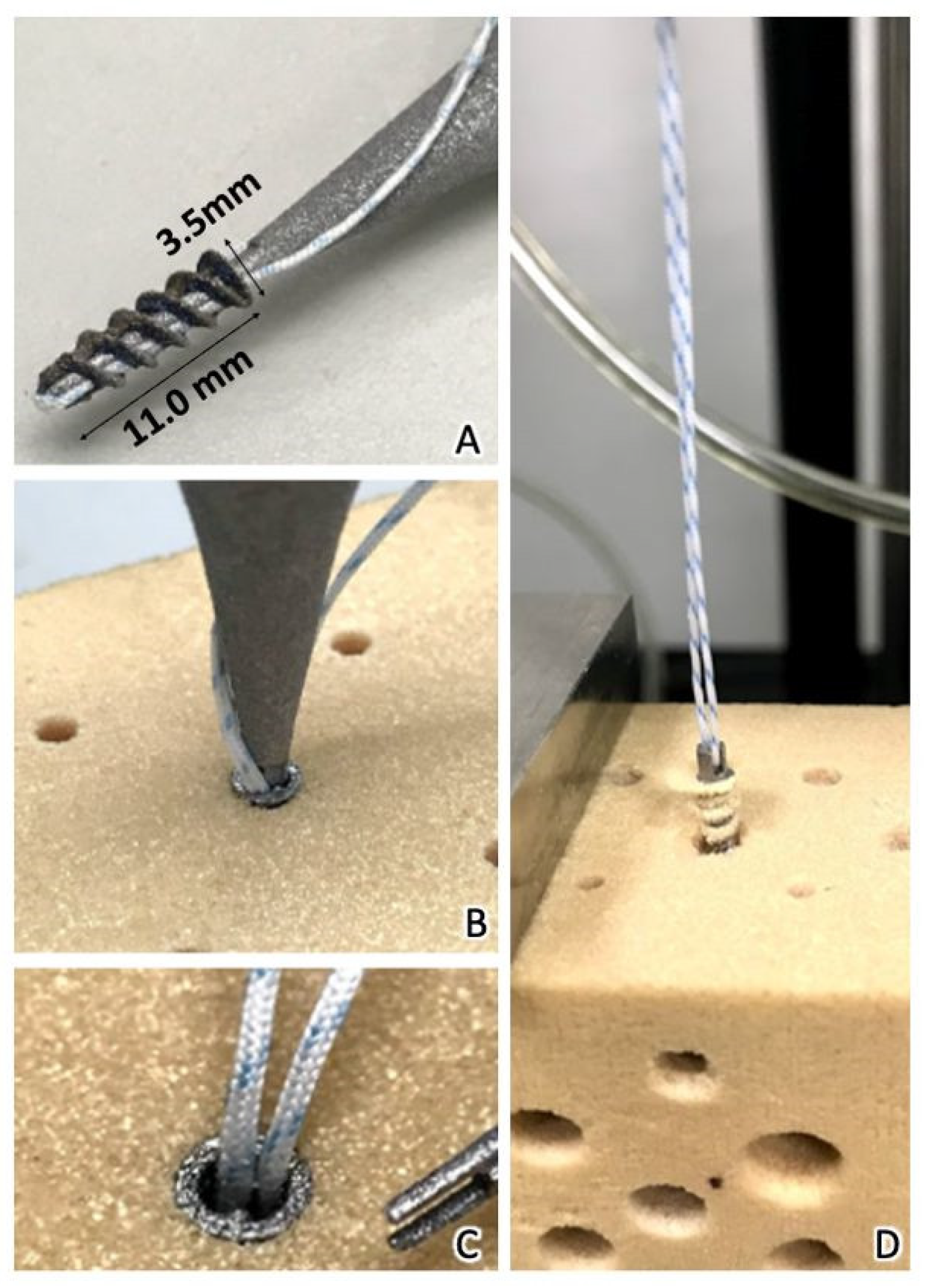
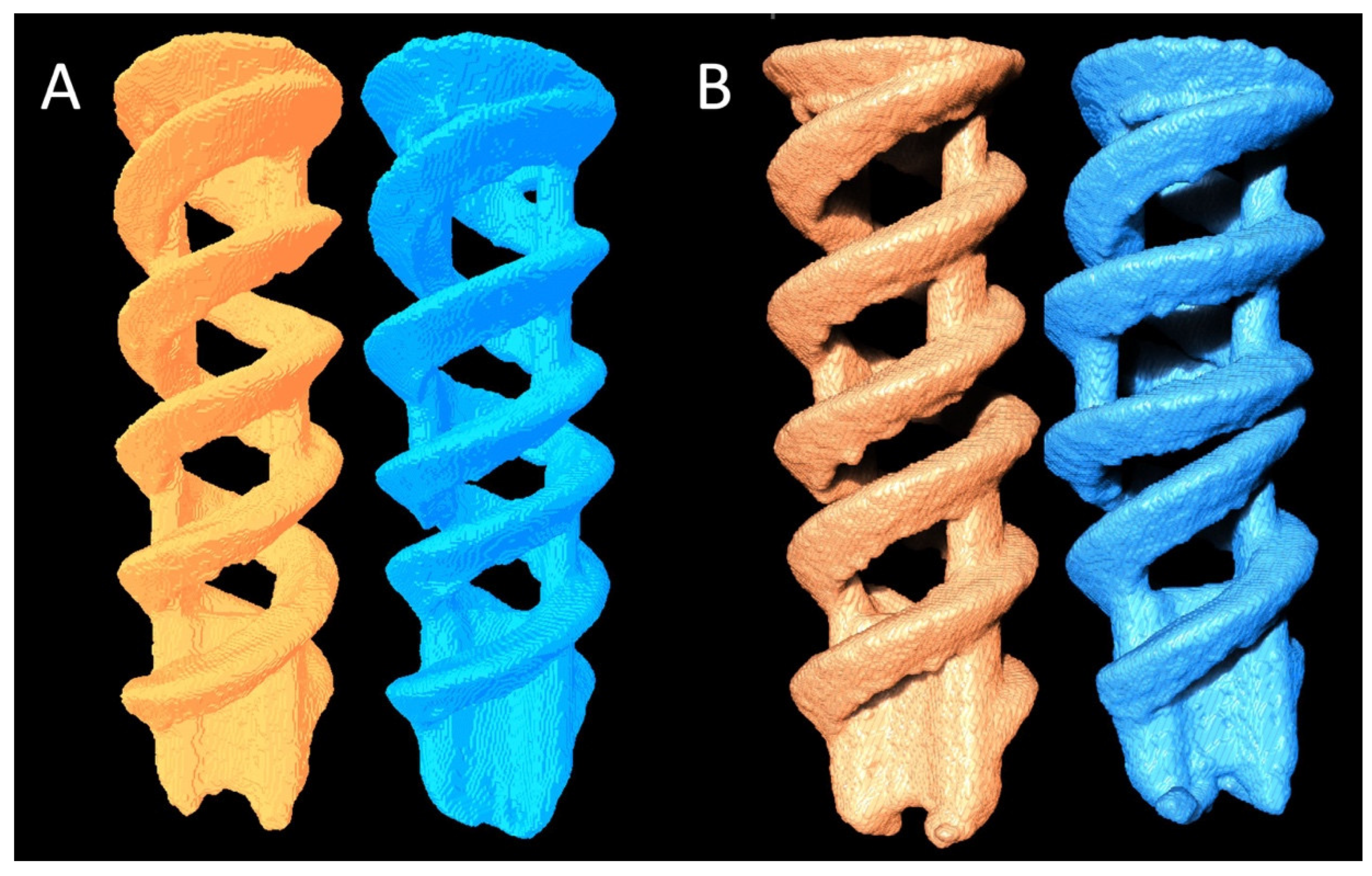
2.1. Production and In Vitro Tests of Double-Helical Biodegradable Fe SAs
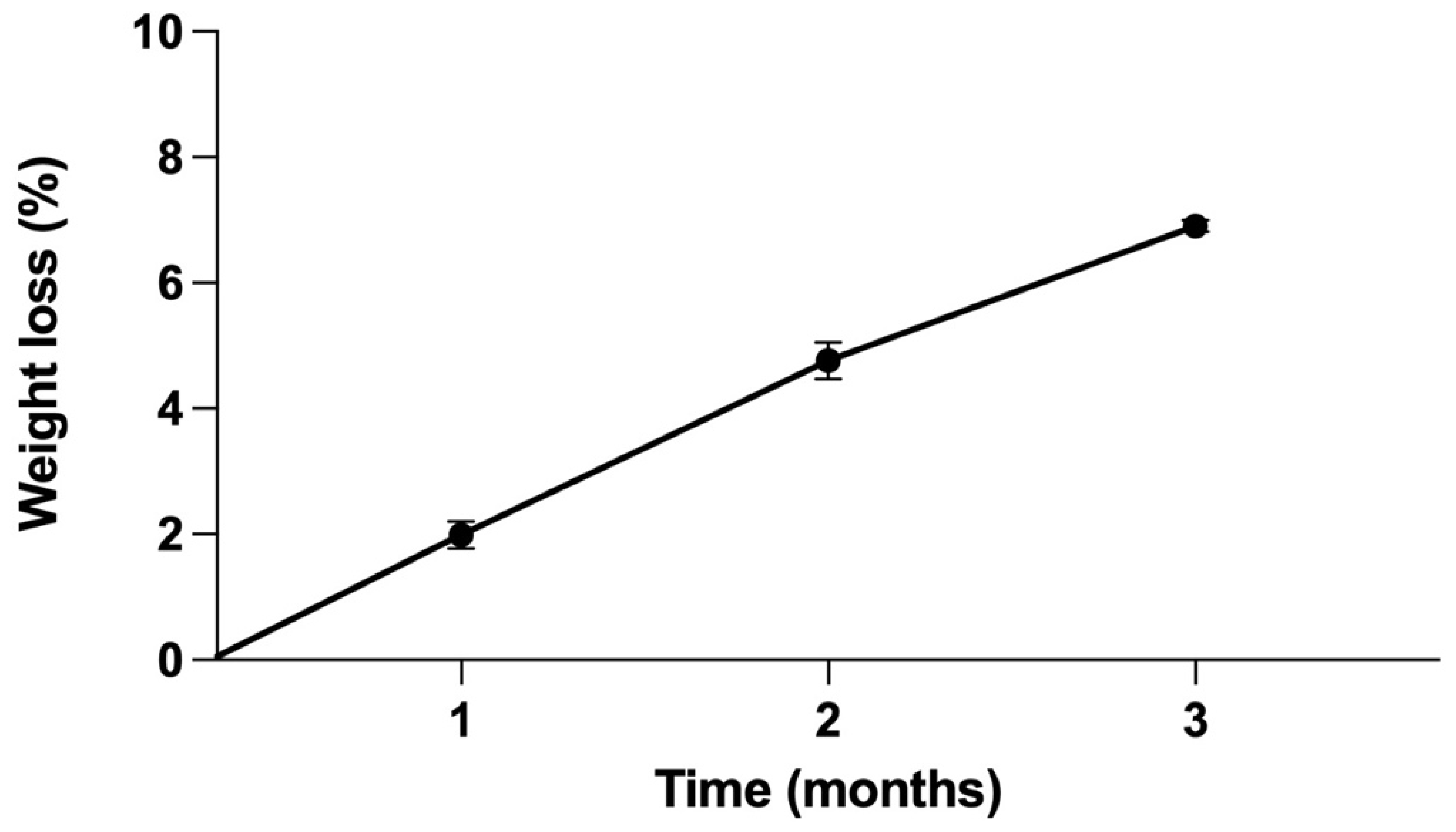
2.2. Corrosion Rate of Pure Fe SAs Using Static Immersion Tests
2.3. In Vivo Animal Study Design
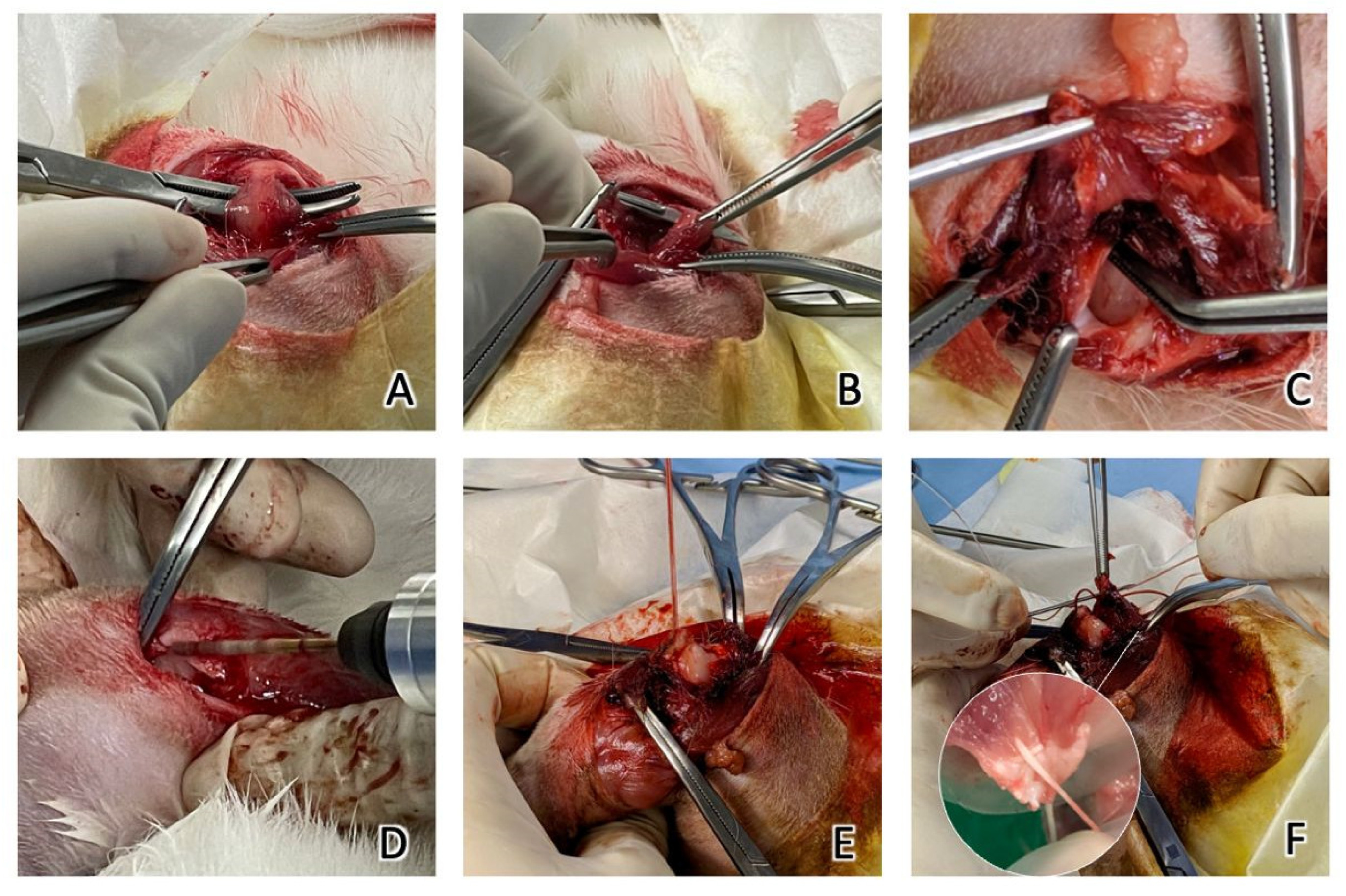
2.4. Surgical Methods
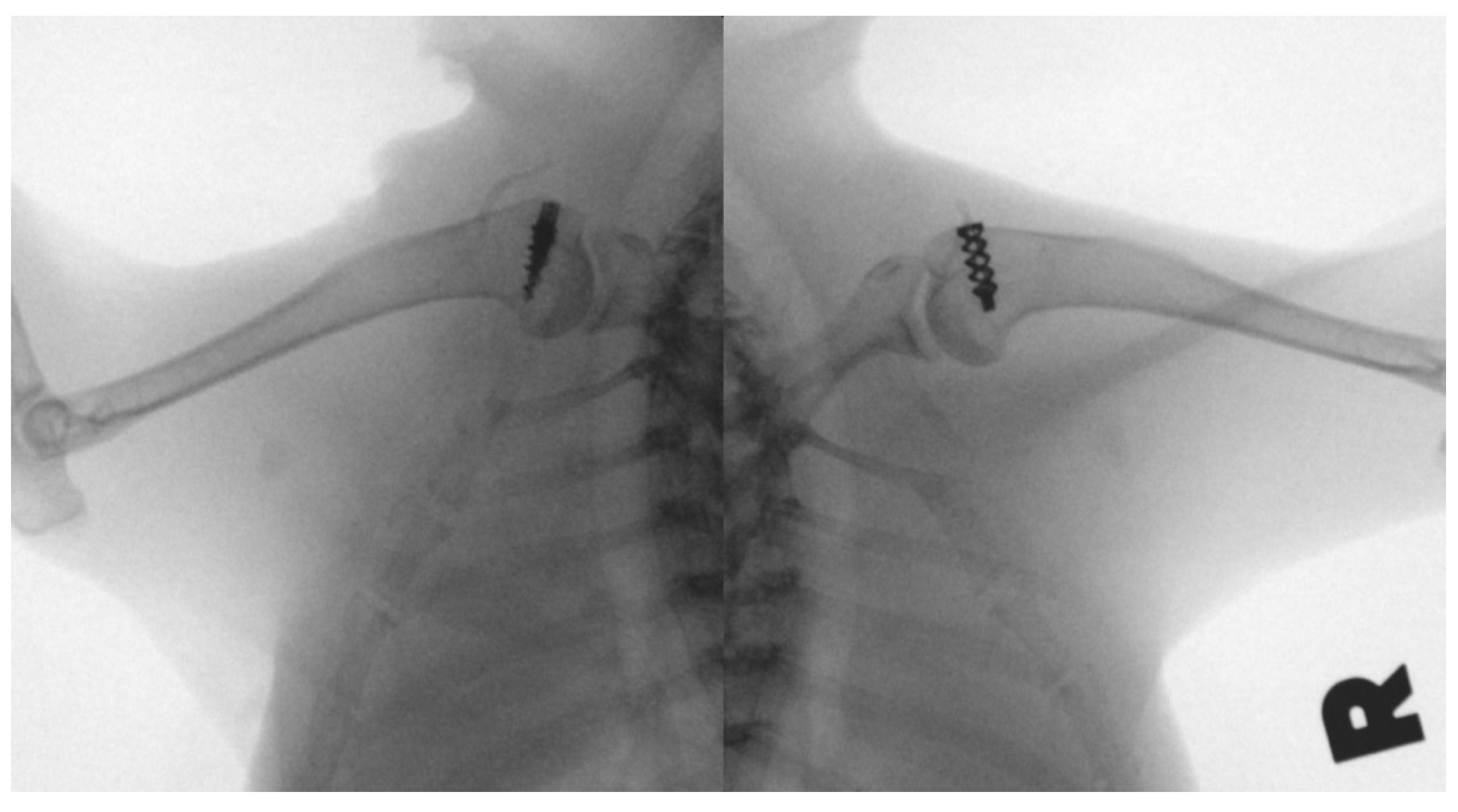
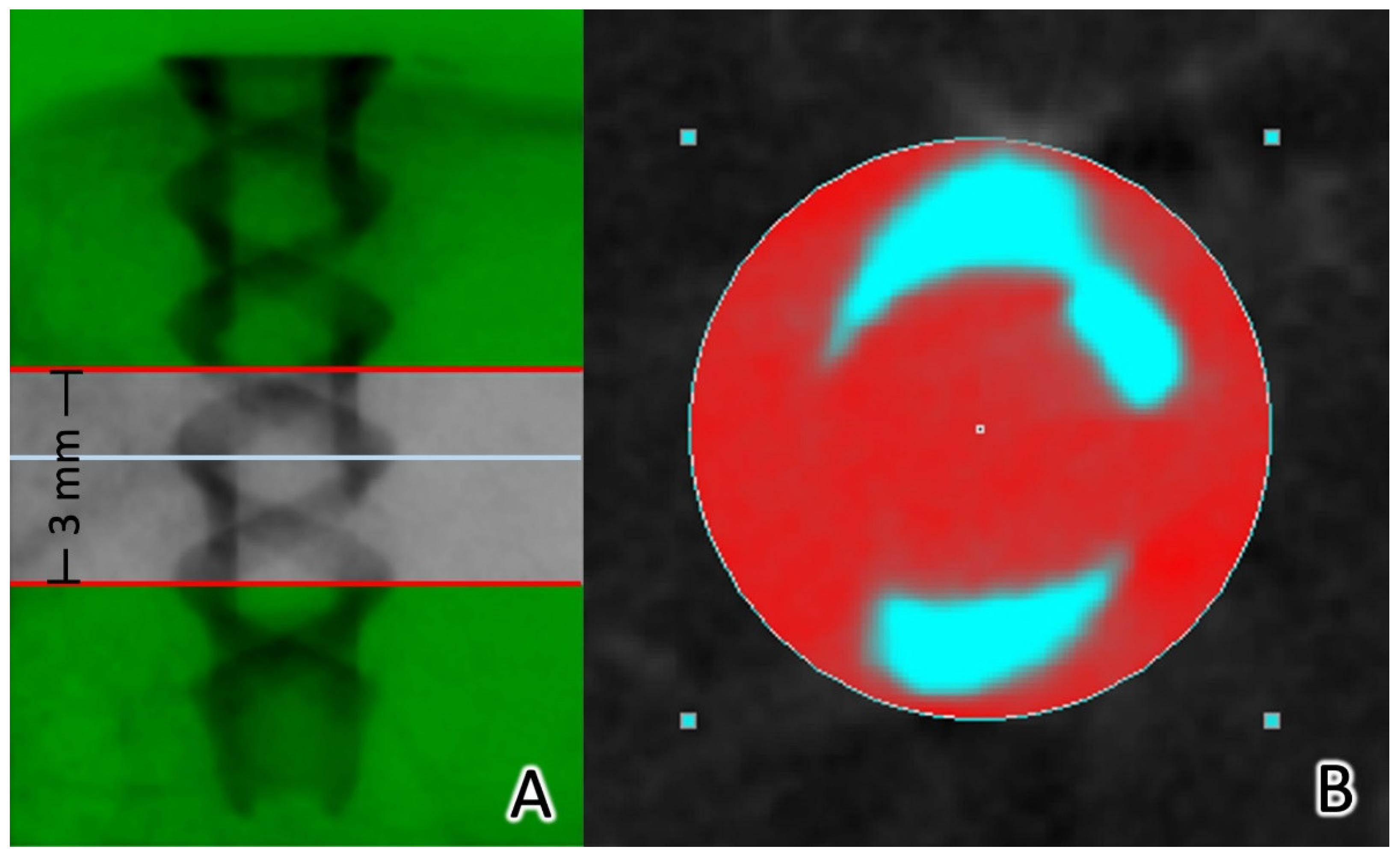
2.5. Micro-CT Analysis
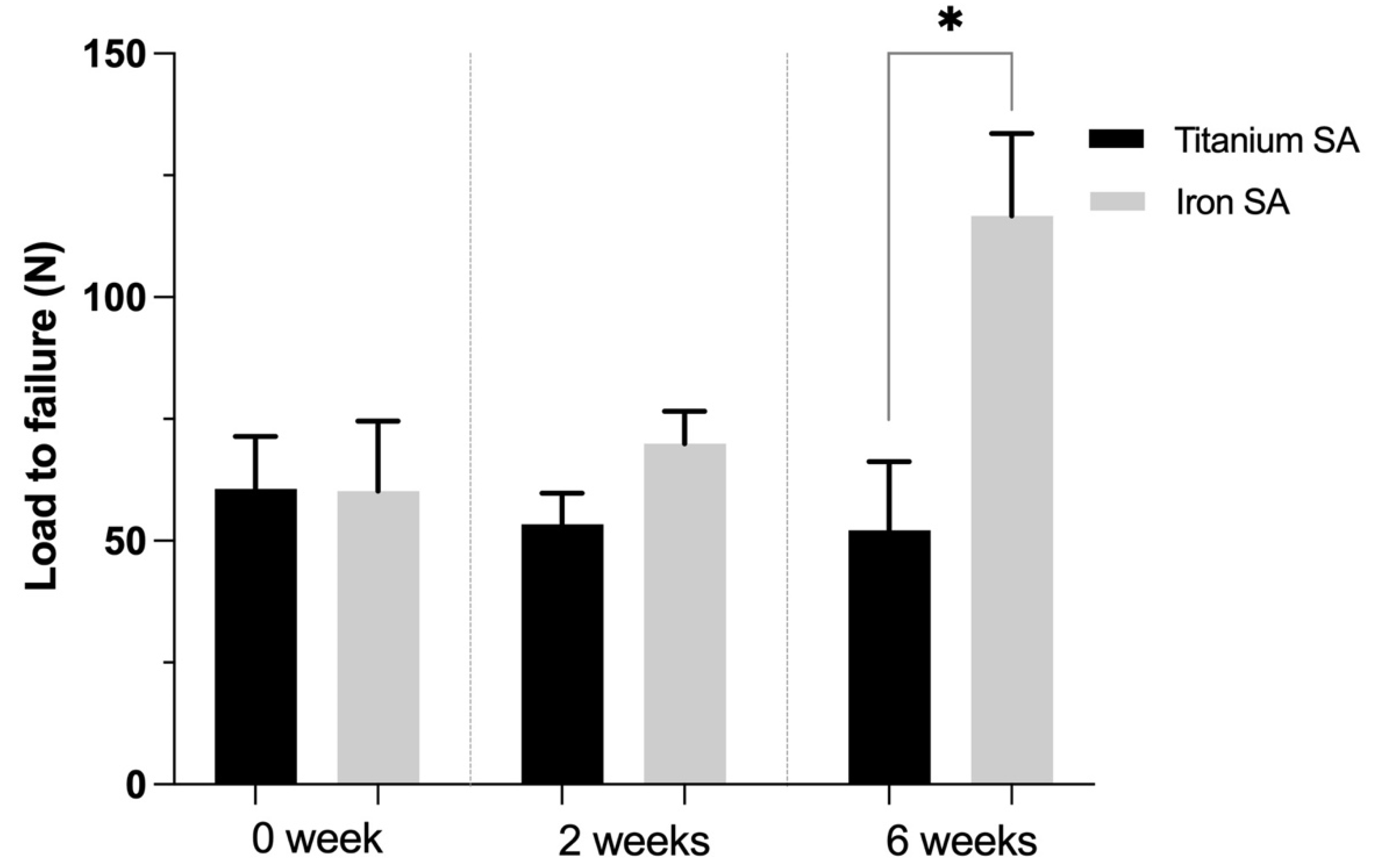
2.6. Biomechanical Analysis
2.7. Histological Analysis
2.8. Biochemical Analysis
2.9. Statistical Analysis
3. Results
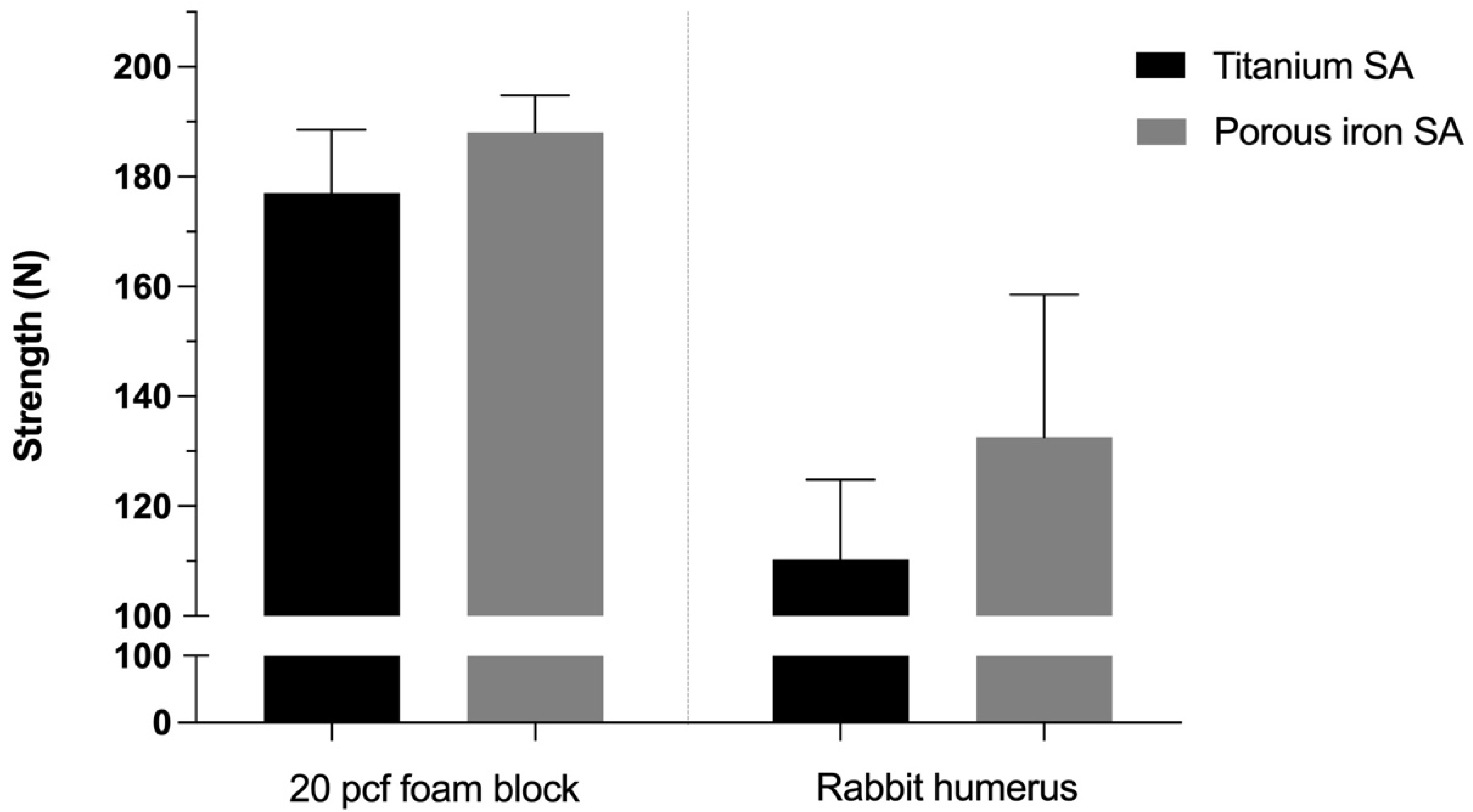
3.1. In Vitro Mechanical Analyses of the Bioabsorbable Fe SA
3.2. Static Immersion Test
3.3. In Vivo Biomechanical Analysis
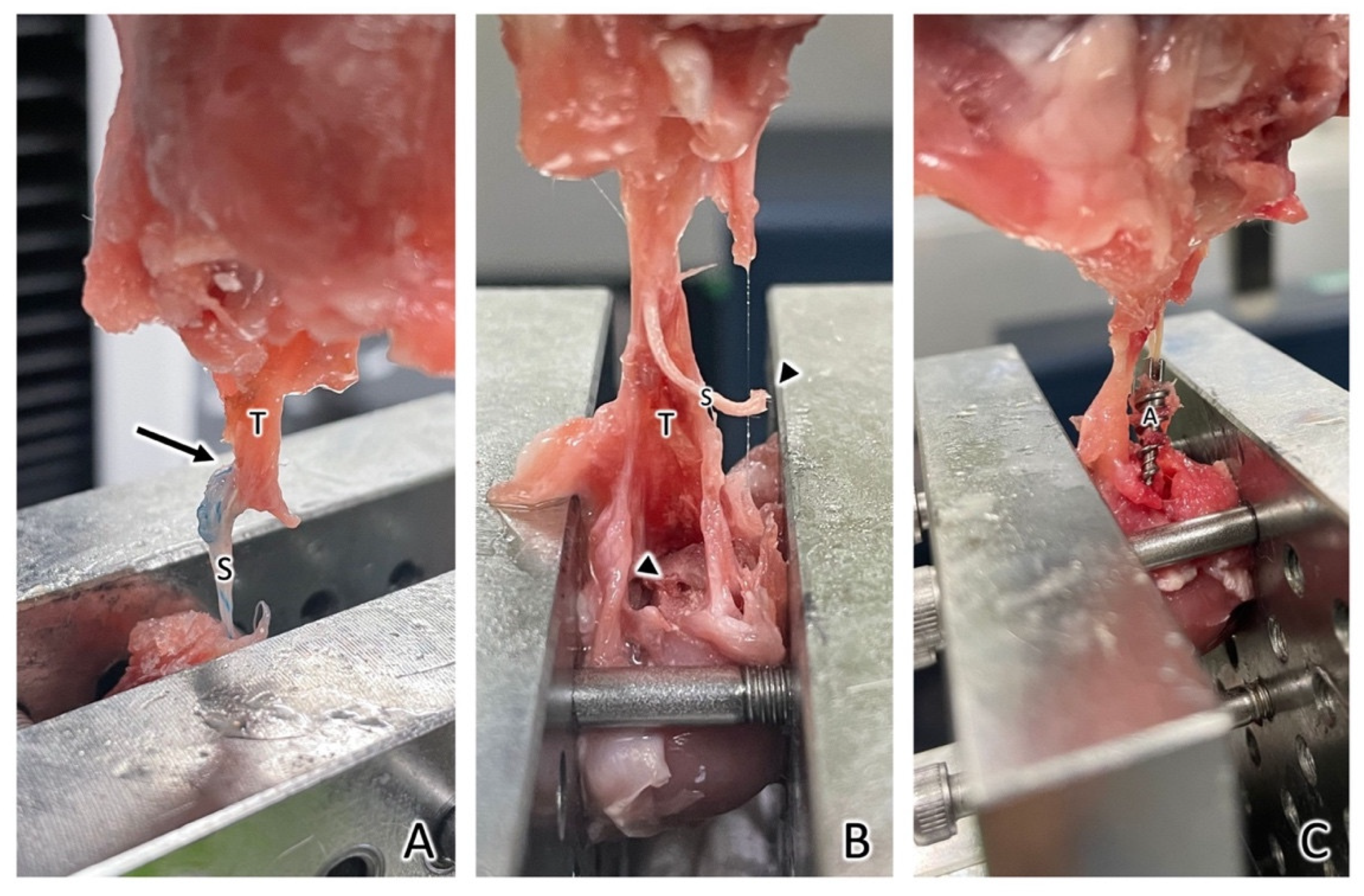
3.4. Failure Sites
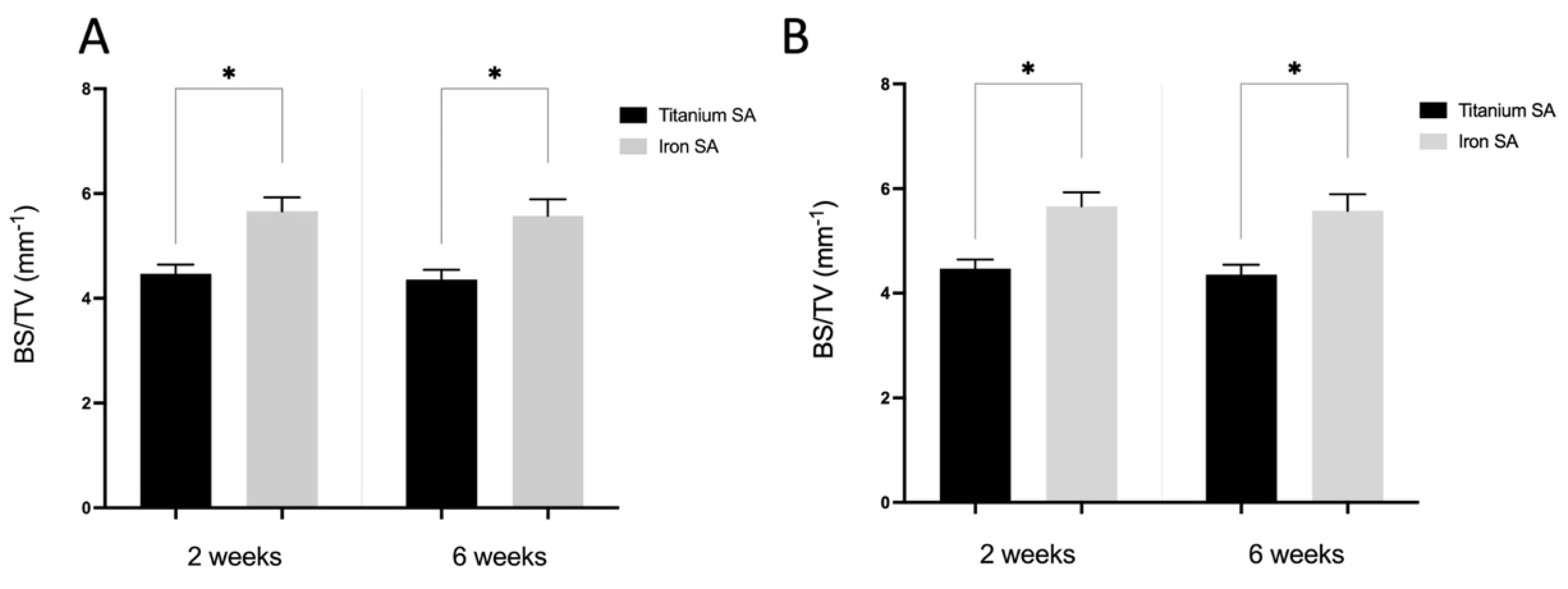
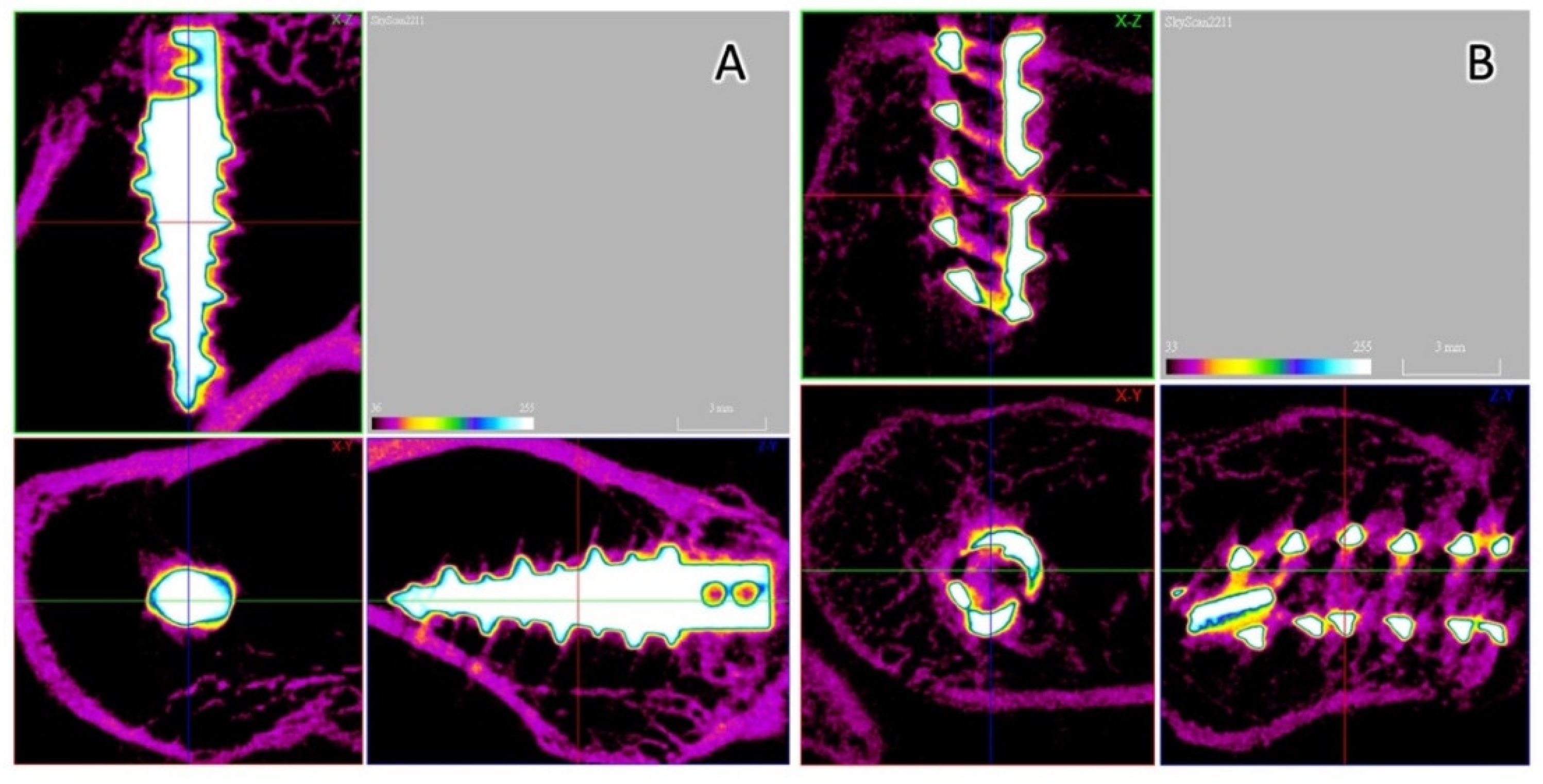
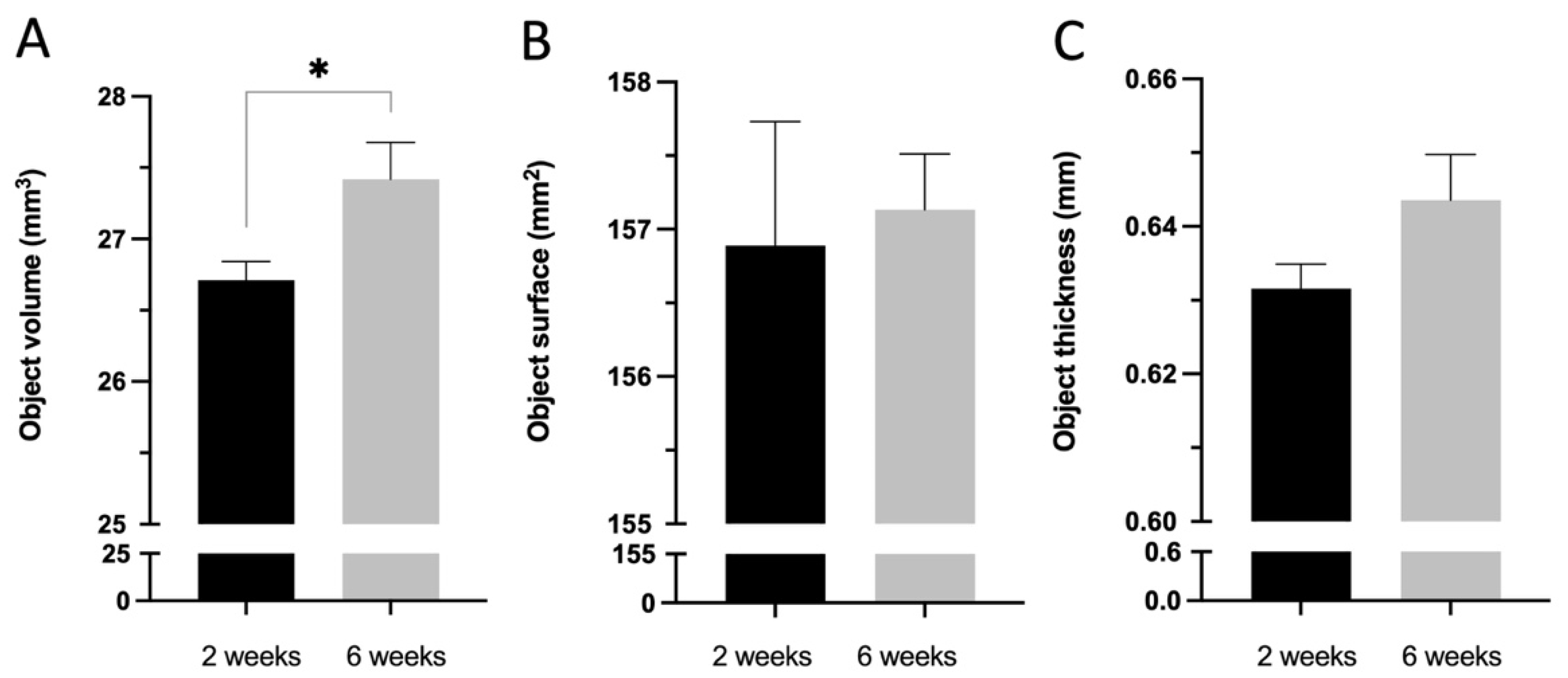
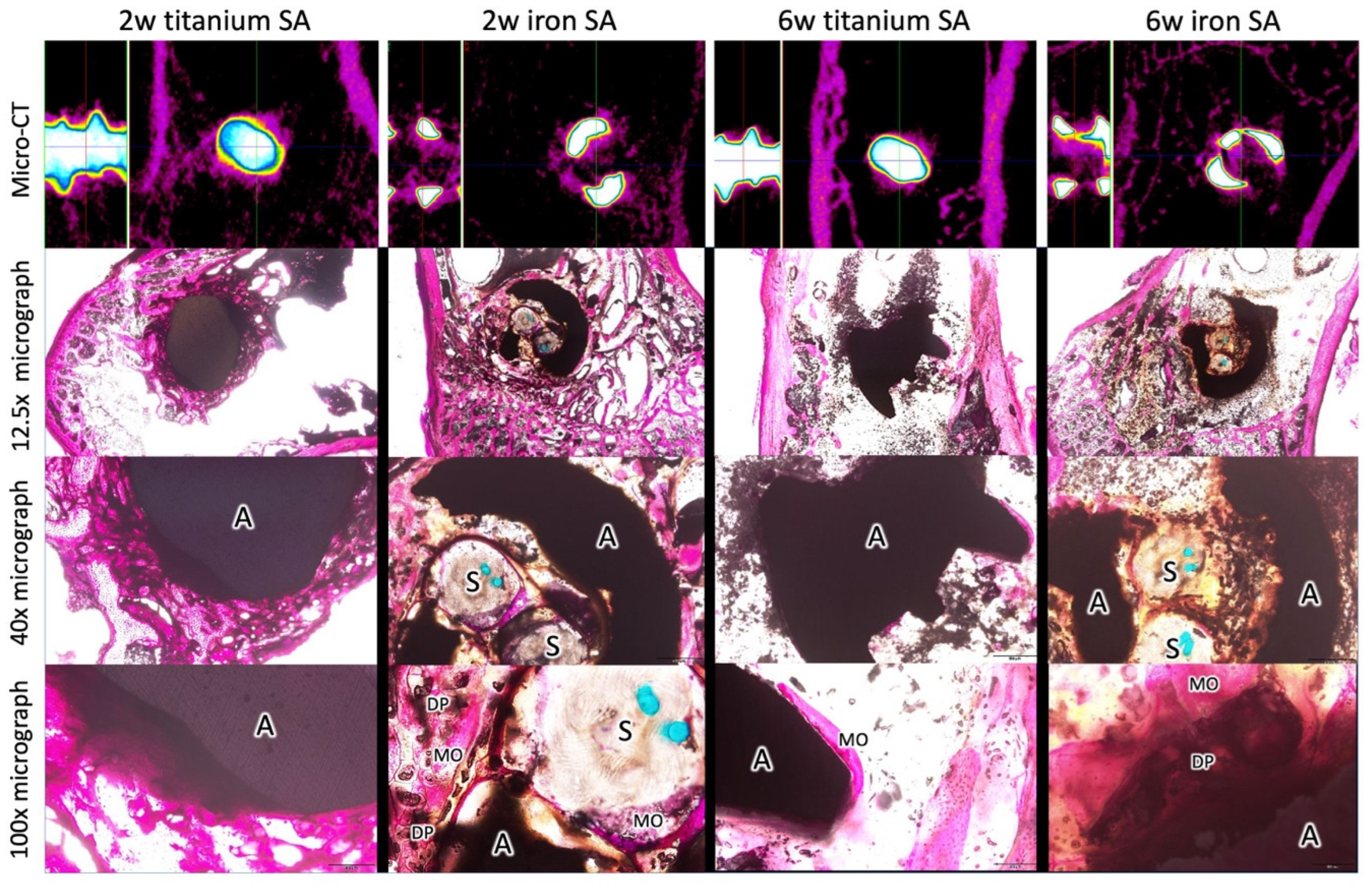
3.5. Micro-CT Analysis
3.6. Histological Analyses
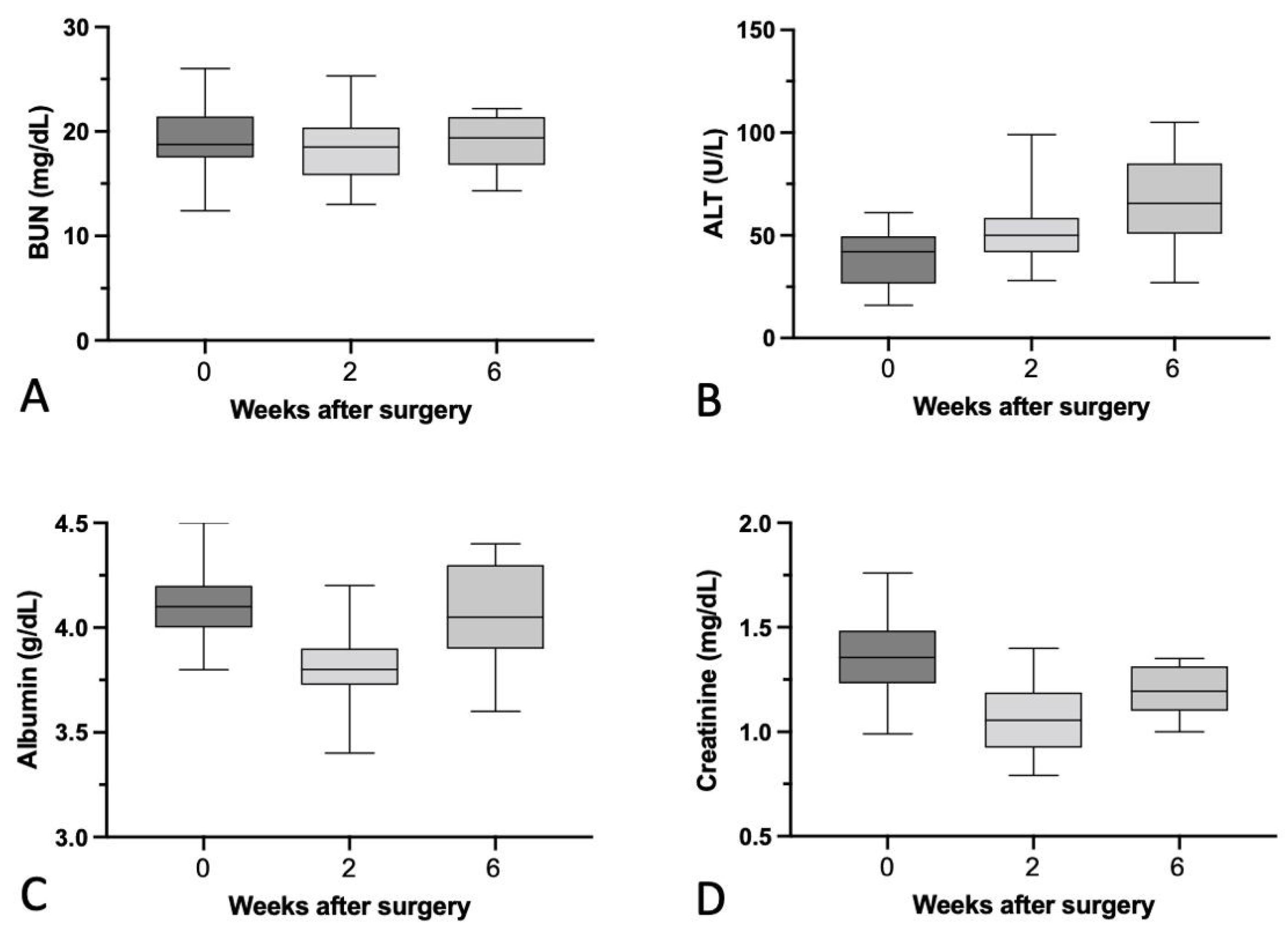
3.7. Biochemical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tashjian, R.Z. Epidemiology, natural history, and indications for treatment of rotator cuff tears. Clin. Sports Med. 2012, 31, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, Y.S.; Park, I.; Lee, H.J.; Han, S.Y.; Jung, S.; Shin, S.J. A Comparison of open-construct PEEK suture anchor and non-vented biocomposite suture anchor in arthroscopic rotator cuff repair: A prospective randomized clinical trial. Arthroscopy 2020, 36, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Petrillo, S.; Loppini, M.; Candela, V.; Rizzello, G.; Maffulli, N.; Denaro, V. Metallic versus biodegradable suture anchors for rotator cuff repair: A case control study. BMC Musculoskelet. Disord. 2019, 20, 477. [Google Scholar] [CrossRef] [PubMed]
- Suchenski, M.; McCarthy, M.B.; Chowaniec, D.; Hansen, D.; McKinnon, W.; Apostolakos, J.; Arciero, R.; Mazzocca, A.D. Material properties and composition of soft-tissue fixation. Arthroscopy 2010, 26, 821–831. [Google Scholar] [CrossRef]
- Stoetzel, S.; Malhan, D.; Wild, U.; Helbing, C.; Hassan, F.; Attia, S.; Jandt, K.D.; Heiss, C.; El Khassawna, T. Osteocytes influence on bone matrix integrity affects biomechanical competence at bone-implant interface of bioactive-coated titanium implants in rat tibiae. Int. J. Mol. Sci 2021, 23, 374. [Google Scholar] [CrossRef]
- Schroder, F.F.; Huis In’t Veld, R.; den Otter, L.A.; van Raak, S.M.; Ten Haken, B.; Vochteloo, A.J.H. Metal artefacts severely hamper magnetic resonance imaging of the rotator cuff tendons after rotator cuff repair with titanium suture anchors. Shoulder Elb. 2018, 10, 107–113. [Google Scholar] [CrossRef]
- Micic, I.; Kholinne, E.; Kwak, J.M.; Koh, K.H.; Jeon, I.H. Osteolysis is observed around both bioabsorbable and nonabsorbable anchors on serial magnetic resonance images of patients undergoing arthroscopic rotator cuff repair. Acta Orthop. Traumatol. Turc. 2019, 53, 414–419. [Google Scholar] [CrossRef]
- Scholten, D.J., 2nd; Waterman, B.R. Editorial commentary: Taking a "PEEK" at suture anchor composition following arthroscopic rotator cuff repair: Is bio really better? Arthroscopy 2020, 36, 397–399. [Google Scholar] [CrossRef]
- Cho, C.H.; Bae, K.C.; Kim, D.H. Biomaterials used for suture anchors in orthopedic surgery. Clin. Orthop. Surg. 2021, 13, 287–292. [Google Scholar] [CrossRef]
- Qin, Y.; Yang, H.; Liu, A.; Dai, J.; Wen, P.; Zheng, Y.; Tian, Y.; Li, S.; Wang, X. Processing optimization, mechanical properties, corrosion behavior and cytocompatibility of additively manufactured Zn-0.7Li biodegradable metals. Acta Biomater. 2022, 142, 388–401. [Google Scholar] [CrossRef]
- Agarwal, S.; Curtin, J.; Duffy, B.; Jaiswal, S. Biodegradable magnesium alloys for orthopaedic applications: A review on corrosion, biocompatibility and surface modifications. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 68, 948–963. [Google Scholar] [CrossRef] [PubMed]
- Su, T.-Y.; Tang, H.-Y.; Jang, J.S.-C.; Chen, C.-H.; Chen, H.-H. Design and development of magnesium-based suture anchor for rotator cuff repair using finite element analysis and in vitro testing. Appl. Sci. 2021, 11, 9602. [Google Scholar] [CrossRef]
- Putra, N.E.; Leeflang, M.A.; Minneboo, M.; Taheri, P.; Fratila-Apachitei, L.E.; Mol, J.M.C.; Zhou, J.; Zadpoor, A.A. Extrusion-based 3D printed biodegradable porous iron. Acta Biomater. 2021, 121, 741–756. [Google Scholar] [CrossRef] [PubMed]
- Venezuela, J.; Dargusch, M.S. The influence of alloying and fabrication techniques on the mechanical properties, biodegradability and biocompatibility of zinc: A comprehensive review. Acta Biomater. 2019, 87, 1–40. [Google Scholar] [CrossRef]
- Hermawan, H. Updates on the research and development of absorbable metals for biomedical applications. Prog. Biomater. 2018, 7, 93–110. [Google Scholar] [CrossRef]
- Zhang, J.; Hiromoto, S.; Yamazaki, T.; Huang, H.; Jia, G.Z.; Li, H.Y.; Yuan, G.Y. Macrophage phagocytosis of biomedical Mg alloy degradation products prepared by electrochemical method. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 75, 1178–1183. [Google Scholar] [CrossRef]
- Sanchez, A.H.M.; Luthringer, B.J.C.; Feyerabend, F.; Willumeit, R. Mg and Mg alloys: How comparable are in vitro and in vivo corrosion rates? A review. Acta Biomater. 2015, 13, 16–31. [Google Scholar] [CrossRef]
- Johnston, S.; Dargusch, M.; Atrens, A. Building towards a standardised approach to biocorrosion studies: A review of factors influencing Mg corrosion in vitro pertinent to in vivo corrosion. Sci. China Mater. 2018, 61, 475–500. [Google Scholar] [CrossRef]
- Shuai, C.J.; Li, S.; Peng, S.P.; Feng, P.; Lai, Y.X.; Gao, C.D. Biodegradable metallic bone implants. Mat. Chem. Front. 2019, 3, 544–562. [Google Scholar] [CrossRef]
- Gorejova, R.; Orinakova, R.; Kralova, Z.O.; Balaz, M.; Kupkova, M.; Hrubovcakova, M.; Haverova, L.; Dzupon, M.; Orinak, A.; Kal’avsky, F.; et al. In vitro corrosion behavior of biodegradable iron foams with polymeric coating. Materials 2020, 13, 184. [Google Scholar] [CrossRef]
- Bowen, P.K.; Drelich, J.; Goldman, J. Zinc exhibits ideal physiological corrosion behavior for bioabsorbable stents. Adv. Mater. 2013, 25, 2577–2582. [Google Scholar] [CrossRef] [PubMed]
- Hagelstein, S.; Zankovic, S.; Kovacs, A.; Barkhoff, R.; Seidenstuecker, M. Mechanical analysis and corrosion analysis of zinc alloys for bioabsorbable implants for osteosynthesis. Materials 2022, 15, 421. [Google Scholar] [CrossRef] [PubMed]
- Kraus, T.; Moszner, F.; Fischerauer, S.; Fiedler, M.; Martinelli, E.; Eichler, J.; Witte, F.; Willbold, E.; Schinhammer, M.; Meischel, M.; et al. Biodegradable Fe-based alloys for use in osteosynthesis: Outcome of an in vivo study after 52 weeks. Acta Biomater. 2014, 10, 3346–3353. [Google Scholar] [CrossRef]
- Hong, D.H.; Chou, D.T.; Velikokhatnyi, O.I.; Roy, A.; Lee, B.; Swink, I.; Issaev, I.; Kuhn, H.A.; Kumta, P.N. Binder-jetting 3D printing and alloy development of new biodegradable Fe-Mn-Ca/Mg alloys. Acta Biomater. 2016, 45, 375–386. [Google Scholar] [CrossRef] [PubMed]
- Tai, C.-C.; Lo, H.-L.; Liaw, C.-K.; Huang, Y.-M.; Huang, Y.-H.; Yang, K.-Y.; Huang, C.-C.; Huang, S.-I.; Shen, H.-H.; Lin, T.-H.; et al. Biocompatibility and Biological performance evaluation of additive-manufactured bioabsorbable iron-based porous suture anchor in a rabbit model. Int. J. Mol. Sci. 2021, 22, 7368. [Google Scholar] [CrossRef]
- Md Yusop, A.H.; Ulum, M.F.; Al Sakkaf, A.; Hartanto, D.; Nur, H. Insight into the bioabsorption of Fe-based materials and their current developments in bone applications. Biotechnol. J. 2021, 16, e2100255. [Google Scholar] [CrossRef] [PubMed]
- Mathewson, M.A.; Kwan, A.; Eng, C.M.; Lieber, R.L.; Ward, S.R. Comparison of rotator cuff muscle architecture between humans and other selected vertebrate species. J. Exp. Biol. 2014, 217, 261–273. [Google Scholar] [CrossRef]
- Barber, F.A.; Herbert, M.A.; Richards, D.P. Sutures and suture anchors: Update 2003. Arthroscopy 2003, 19, 985–990. [Google Scholar] [CrossRef]
- ASTM G 31-72; Standard Practice for Laboratory Immersion Corrosion Testing of Metals. American Society for Testing and Materials: West Conshohocken, PA, USA, 2004.
- Louati, H.; Uhthoff, H.K.; Culliton, K.; Laneuville, O.; Lapner, P.; Trudel, G. Supraspinatus tendon repair using anchors: A biomechanical evaluation in the rabbit. J. Orthop Surg. Res. 2018, 13, 64. [Google Scholar] [CrossRef]
- Chiu, Y.R.; Hsu, Y.T.; Wu, C.Y.; Lin, T.H.; Yang, Y.Z.; Chen, H.Y. Fabrication of asymmetrical and gradient hierarchy structures of poly-p-xylylenes on multiscale regimes based on a vapor-phase sublimation and deposition process. Chem. Mat. 2020, 32, 1120–1130. [Google Scholar] [CrossRef]
- Pyka, G.; Kerckhofs, G.; Schrooten, J.; Wevers, M. The effect of spatial micro-CT image resolution and surface complexity on the morphological 3D analysis of open porous structures. Mater. Charact. 2014, 87, 104–115. [Google Scholar] [CrossRef]
- Dalen, G.; Koster, M. 2D & 3D particle size analysis of micro-CT images. In Proceedings of the Bruker micro-CT User Meeting, Brussels, Belgium, 13 November 2012; pp. 3–5. [Google Scholar]
- Diekmann, J.; Bauer, S.; Weizbauer, A.; Willbold, E.; Windhagen, H.; Helmecke, P.; Lucas, A.; Reifenrath, J.; Nolte, I.; Ezechieli, M. Examination of a biodegradable magnesium screw for the reconstruction of the anterior cruciate ligament: A pilot in vivo study in rabbits. Mater. Sci. Eng. C Mater. Biol. Appl. 2016, 59, 1100–1109. [Google Scholar] [CrossRef] [PubMed]
- Wen, C.Y.; Qin, L.; Lee, K.M.; Chan, K.M. Peri-graft bone mass and connectivity as predictors for the strength of tendon-to-bone attachment after anterior cruciate ligament reconstruction. Bone 2009, 45, 545–552. [Google Scholar] [CrossRef] [PubMed]
- Brooks, B.D.; Sinclair, K.D.; Grainger, D.W.; Brooks, A.E. A resorbable antibiotic-eluting polymer composite bone void filler for perioperative infection prevention in a rabbit radial defect model. PLoS ONE 2015, 10, e0118696. [Google Scholar] [CrossRef] [PubMed]
- ISO. 15189 Medical Laboratories-Requirements for Quality and Competence, 3rd ed.; International Organization for Standardization, Ed.; European Committee for Standardization: Geneva, The Switzerland, 2012. [Google Scholar]
- Moravej, M.; Purnama, A.; Fiset, M.; Couet, J.; Mantovani, D. Electroformed pure iron as a new biomaterial for degradable stents: In vitro degradation and preliminary cell viability studies. Acta Biomater. 2010, 6, 1843–1851. [Google Scholar] [CrossRef]
- Obayi, C.S.; Tolouei, R.; Paternoster, C.; Turgeon, S.; Okorie, B.A.; Obikwelu, D.O.; Cassar, G.; Buhagiar, J.; Mantovani, D. Influence of cross-rolling on the micro-texture and biodegradation of pure iron as biodegradable material for medical implants. Acta Biomater. 2015, 17, 68–77. [Google Scholar] [CrossRef]
- Shuai, C.; Li, S.; Wang, G.; Yang, Y.; Peng, S.; Gao, C. Strong corrosion induced by carbon nanotubes to accelerate Fe biodegradation. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 104, 109935. [Google Scholar] [CrossRef]
- Walker, J.; Shadanbaz, S.; Kirkland, N.T.; Stace, E.; Woodfield, T.; Staiger, M.P.; Dias, G.J. Magnesium alloys: Predicting in vivo corrosion with in vitro immersion testing. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 1134–1141. [Google Scholar] [CrossRef]
- Zainal Abidin, N.I.; Rolfe, B.; Owen, H.; Malisano, J.; Martin, D.; Hofstetter, J.; Uggowitzer, P.J.; Atrens, A. The in vivo and in vitro corrosion of high-purity magnesium and magnesium alloys WZ21 and AZ91. Corros. Sci. 2013, 75, 354–366. [Google Scholar] [CrossRef]
- Yang, H.; Jia, B.; Zhang, Z.; Qu, X.; Li, G.; Lin, W.; Zhu, D.; Dai, K.; Zheng, Y. Alloying design of biodegradable zinc as promising bone implants for load-bearing applications. Nat. Commun. 2020, 11, 401. [Google Scholar] [CrossRef]
- Mostaed, E.; Sikora-Jasinska, M.; Mostaed, A.; Loffredo, S.; Demir, A.G.; Previtali, B.; Mantovani, D.; Beanland, R.; Vedani, M. Novel Zn-based alloys for biodegradable stent applications: Design, development and in vitro degradation. J. Mech. Behav. Biomed. Mater. 2016, 60, 581–602. [Google Scholar] [CrossRef] [PubMed]
- Vojtěch, D.; Kubásek, J.; Šerák, J.; Novák, P. Mechanical and corrosion properties of newly developed biodegradable Zn-based alloys for bone fixation. Acta Biomater. 2011, 7, 3515–3522. [Google Scholar] [CrossRef] [PubMed]
- Chaler, J.; Louati, H.; Uhthoff, H.K.; Trudel, G. Supraspinatus tendon transosseous vs anchor repair surgery: A comparative study of mechanical recovery in the rabbit. J. Orthop. Surg. Res. 2020, 15, 585. [Google Scholar] [CrossRef] [PubMed]
- Bouxsein, M.L.; Boyd, S.K.; Christiansen, B.A.; Guldberg, R.E.; Jepsen, K.J.; Muller, R. Guidelines for assessment of bone microstructure in rodents using micro-computed tomography. J. Bone Miner. Res. 2010, 25, 1468–1486. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, J.; Yamamoto, N.; Nagamoto, H.; Itoi, E. Minimum distance of suture anchors used for rotator cuff repair without decreasing the pullout strength: A biomechanical study. Arthroscopy 2018, 34, 377–385. [Google Scholar] [CrossRef]
- Hsieh, Y.-Y.; Wu, L.-C.; Tsuang, F.-Y.; Chen, C.-H.; Chiang, C.-J. Pull-Out capability of a 3D printed threadless suture anchor with rectangular cross-section: A biomechanical study. Appl. Sci. 2021, 11, 12128. [Google Scholar] [CrossRef]
- Anandhapadman, A.; Venkateswaran, A.; Jayaraman, H.; Ghone, N.V. Advances in 3D printing of composite scaffolds for the repairment of bone tissue associated defects. Biotechnol. Prog. 2022; online ahead of print. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Week 0 | Week 2 | Week 6 | |
|---|---|---|---|
| BUN (mg/dL) | 19.8 ± 3.19 | 18.43 ± 3.06 | 18.98 ± 2.83 |
| ALT (U/L) | 39.35 ± 13.33 | 51.95 ± 16.39 | 65.50 ± 23.19 |
| Alb (g/dL) | 4.12 ± 0.19 | 3.81 ± 0.21 | 4.07 ± 0.25 |
| Cr (mg/dL) | 1.35 ± 0.18 | 1.06 ± 0.17 | 1.19 ± 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.-C.; Chang, C.-H.; Chen, C.-H.; Lu, C.-K.; Ma, C.-H.; Huang, S.-I.; Fan, W.-L.; Shen, H.-H.; Tsai, P.-I.; Yang, K.-Y.; et al. 3D-Printed Double-Helical Biodegradable Iron Suture Anchor: A Rabbit Rotator Cuff Tear Model. Materials 2022, 15, 2801. https://doi.org/10.3390/ma15082801
Liu W-C, Chang C-H, Chen C-H, Lu C-K, Ma C-H, Huang S-I, Fan W-L, Shen H-H, Tsai P-I, Yang K-Y, et al. 3D-Printed Double-Helical Biodegradable Iron Suture Anchor: A Rabbit Rotator Cuff Tear Model. Materials. 2022; 15(8):2801. https://doi.org/10.3390/ma15082801
Chicago/Turabian StyleLiu, Wen-Chih, Chih-Hau Chang, Chung-Hwan Chen, Chun-Kuan Lu, Chun-Hsien Ma, Shin-I Huang, Wei-Lun Fan, Hsin-Hsin Shen, Pei-I Tsai, Kuo-Yi Yang, and et al. 2022. "3D-Printed Double-Helical Biodegradable Iron Suture Anchor: A Rabbit Rotator Cuff Tear Model" Materials 15, no. 8: 2801. https://doi.org/10.3390/ma15082801