
Additive Manufacturing of Spinal Braces: Evaluation of Production Process and Postural Stability in Patients with Scoliosis

 , , , and
, , , and
Abstract
:1. Introduction
- To quantitatively evaluate all phases of an innovative production process to produce spinal orthoses based on FDM additive manufacturing for the treatment of scoliosis in AIS and OI patients.
- To compare postural stability metrics between the unbraced and the two braced conditions (3D-printed and conventional), obtained using a wearable inertial sensor.
2. Materials and Methods
2.1. Study Design and Participants
2.2. Production of the 3D-Printed Braces
2.2.1. 3D Chest Geometry Acquisition
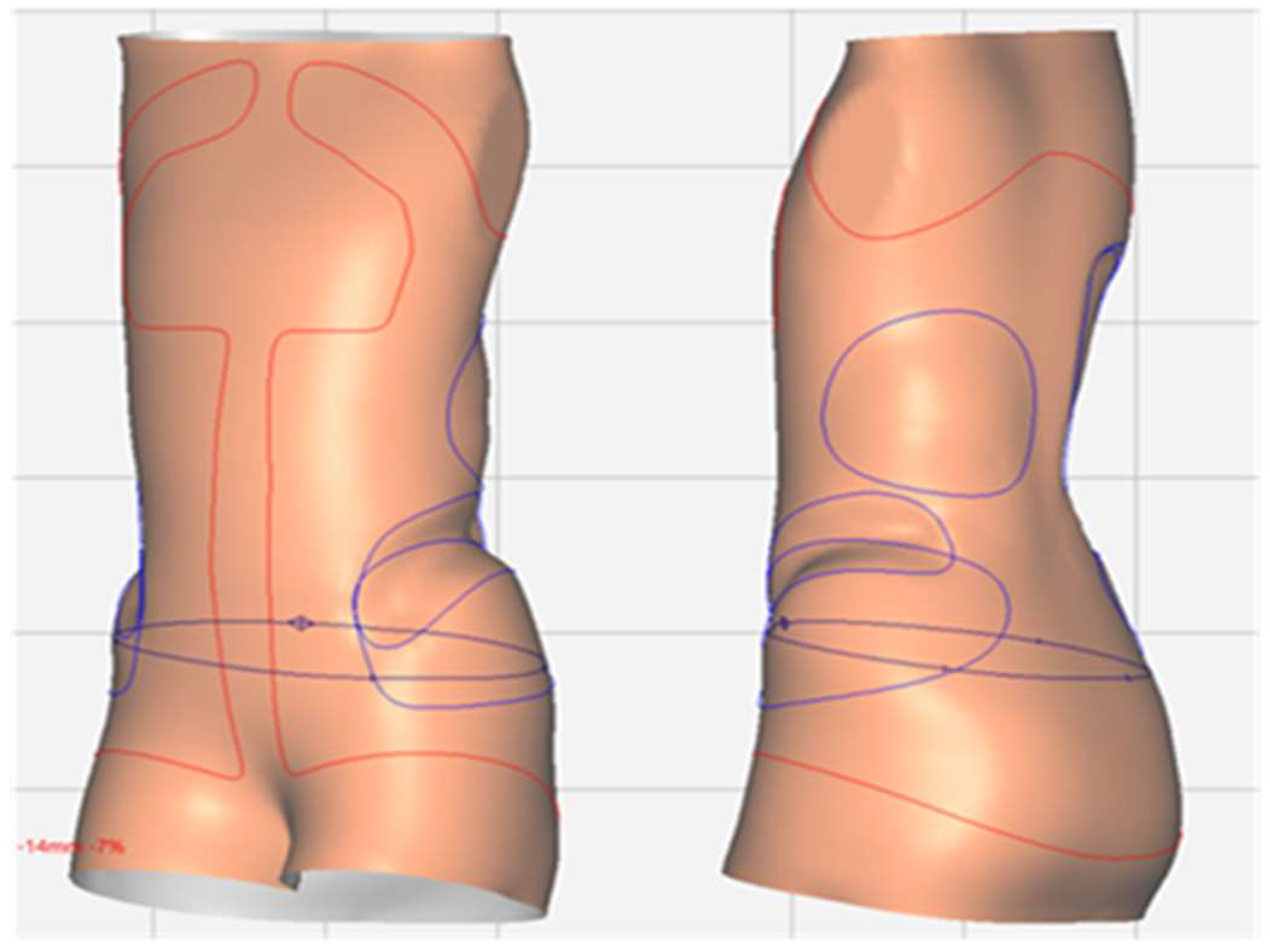
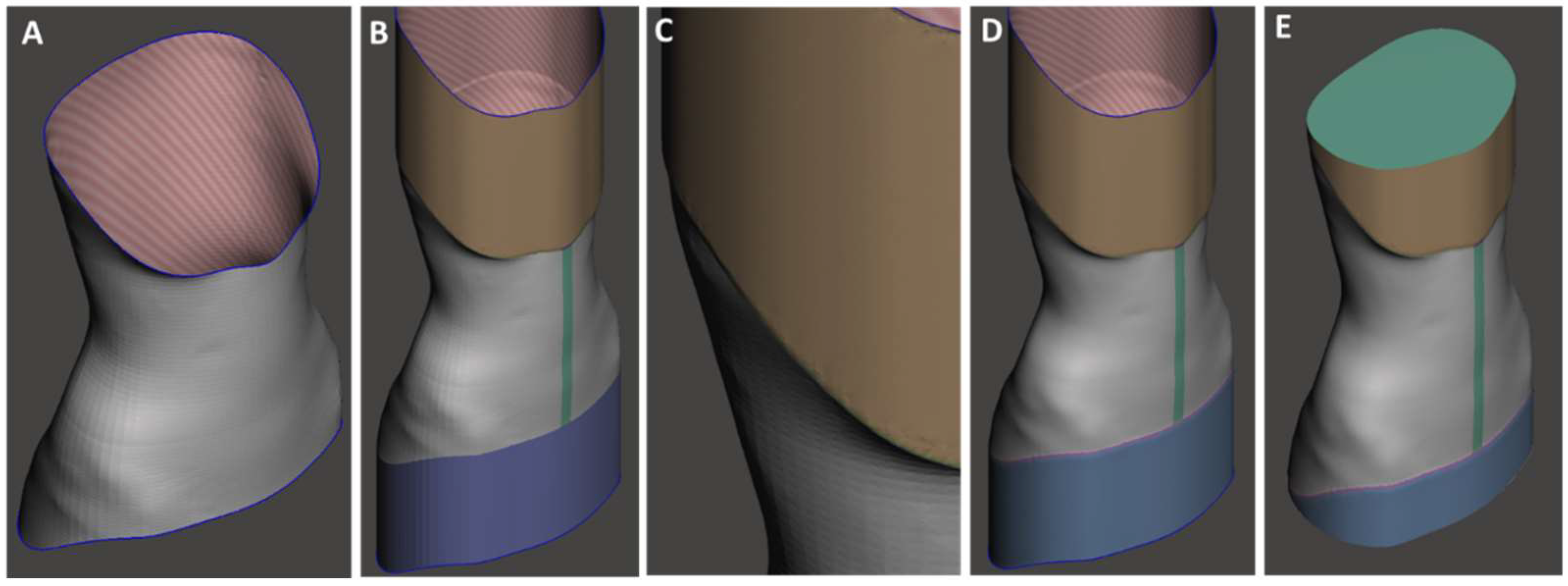
2.2.2. CAD Design Process
2.2.3. Additive Manufacturing
2.2.4. Post-Processing
2.3. Production of the Conventional Braces
2.4. Analysis of the Production Process
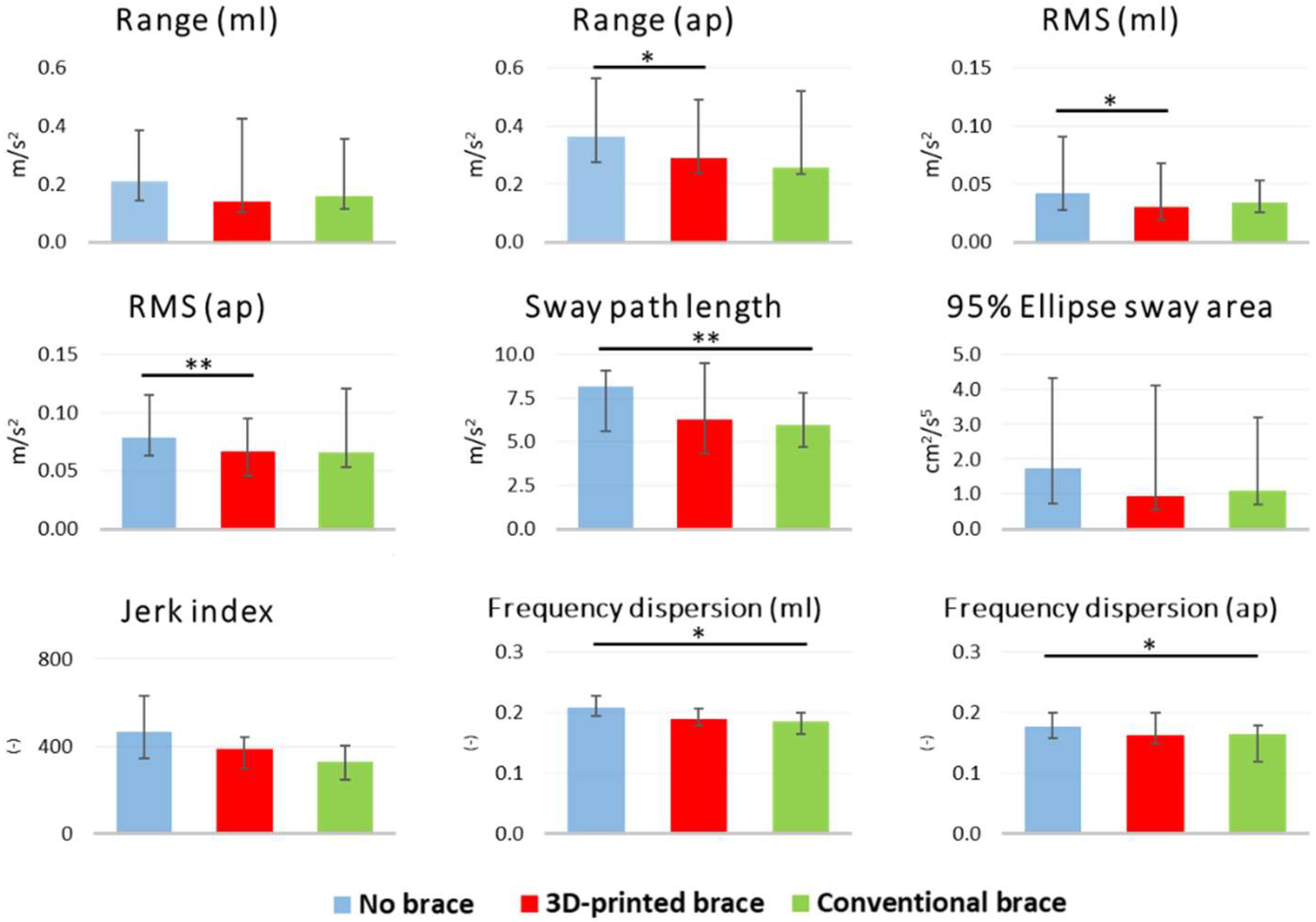
2.5. Postural Stability
3. Results
3.1. Patients
3.2. Analysis of the Production Process
3.3. Postural Stability
4. Discussion
4.1. 3D Scanning
4.2. CAD Design
4.3. Additive Manufacturing
4.4. Post-Processing
4.5. Postural Stability
4.6. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldberg, C.J.; Moore, D.P.; Fogarty, E.E.; Dowling, F.E. Scoliosis: A review. Pediatr. Surg. Int. 2008, 24, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Janicki, J.A.; Alman, B. Scoliosis: Review of diagnosis and treatment. Paediatr. Child Health 2007, 12, 771–776. [Google Scholar] [CrossRef] [PubMed]
- Yamane, A. 1-Orthotic Prescription, 5th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of Bracing in Adolescents with Idiopathic Scoliosis. N. Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef]
- Weintrob, J.C. Orthotic management for children with osteogenesis imperfecta. Connect. Tissue Res. 1995, 31, s41–s43. [Google Scholar] [CrossRef]
- Cheng, J.C.; Castelein, R.M.; Chu, W.C.; Danielsson, A.J.; Dobbs, M.B.; Grivas, T.B.; Gurnett, C.A.; Luk, K.D.; Moreau, A.; Newton, P.O.; et al. Adolescent idiopathic scoliosis. Nat. Rev. Dis. Prim. 2015, 1, 1–21. [Google Scholar] [CrossRef]
- Marini, J.C.; Forlino, A.; Bächinger, H.P.; Bishop, N.J.; Byers, P.H.; De Paepe, A.; Fassier, F.; Fratzl-Zelman, N.; Kozloff, K.M.; Krakow, D.; et al. Osteogenesis imperfecta. Nat. Rev. Dis. Prim. 2017, 3, 1–19. [Google Scholar] [CrossRef]
- Fess, E.E.; Gettle, K.S.; Philips, C.A.; Janson, J. Hand and Upper Extremity Splinting: Principles & Methods, 3rd ed.; Elsevier Mosby: Maryland Heights, MI, USA, 2005; ISBN 9780801675225. [Google Scholar]
- Górski, F.; Wichniarek, R.; Kuczko, W.; Zukowska, M.; Lulkiewicz, M.; Zawadzki, P. Experimental studies on 3D printing of automatically designed customized wrist-hand orthoses. Materials 2020, 13, 4091. [Google Scholar] [CrossRef]
- Redaelli, D.F.; Biffi, E.; Colombo, G.; Fraschini, P.; Reni, G. Current and Future Manufacturing of Chest Orthoses, Considering the Case of Osteogenesis Imperfecta. In Proceedings of the ASME 2018 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference, Quebec City, QC, Canada, 26–29 August 2018; pp. 1–7. [Google Scholar]
- Górski, F.; Wichniarek, R.; Kuczko, W.; Żukowska, M. Study on properties of automatically designed 3d-printed customized prosthetic sockets. Materials 2021, 14, 5240. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.D.; Gallo, D.; Dallmayer, R. In-brace correction of the Cobb angle with RSC-CAD CAM compared with “hand made” from the original author. Scoliosis 2010, 5, O68. [Google Scholar] [CrossRef]
- Desbiens-Blais, F.; Clin, J.; Parent, S.; Labelle, H.; Aubin, C.E. New brace design combining CAD/CAM and biomechanical simulation for the treatment of adolescent idiopathic scoliosis. Clin. Biomech. 2012, 27, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Saleh, J.M.; Dalgarno, K.W. Cost and benefit analysis of Fused Deposition Modelling (FDM) technique and Selective Laser Sintering (SLS) for fabrication of customised foot orthoses. In Innovative Developments in Design and Manufacturing—Advanced Research in Virtual and Rapid Prototyping; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Molnár, I.; Morovič, L. Design and manufacture of orthopedic corset using 3D digitization and additive manufacturing. IOP Conf. Ser. Mater. Sci. Eng. 2018, 448, 012058. [Google Scholar] [CrossRef]
- Samdani, U.F.; Hwang, S.W. 3D printing in spine surgery: Current and future applications. J. 3D Print. Med. 2021, 5, 145–153. [Google Scholar] [CrossRef]
- Wang, Y.; Tan, Q.; Pu, F.; Boone, D.; Zhang, M. A Review of the Application of Additive Manufacturing in Prosthetic and Orthotic Clinics from a Biomechanical Perspective. Engineering 2020, 6, 1258–1266. [Google Scholar] [CrossRef]
- Jiang, J. A novel fabrication strategy for additive manufacturing processes. J. Clean. Prod. 2020, 272, 122916. [Google Scholar] [CrossRef]
- Baronio, G.; Volonghi, P.; Signoroni, A. Concept and Design of a 3D Printed Support to Assist Hand Scanning for the Realization of Customized Orthosis. Appl. Bionics Biomech. 2017, 2017, 8171520. [Google Scholar] [CrossRef]
- Li, J.; Tanaka, H. Rapid customization system for 3D-printed splint using programmable modeling technique-a practical approach. 3D Print. Med. 2018, 4, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Mavroidis, C.; Ranky, R.G.; Sivak, M.L.; Patritti, B.L.; DiPisa, J.; Caddle, A.; Gilhooly, K.; Govoni, L.; Sivak, S.; Lancia, M.; et al. Patient specific ankle-foot orthoses using rapid prototyping. J. Neuroeng. Rehabil. 2011, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Lazzeri, S.; Talanti, E.; Basciano, S.; Barbato, R.; Fontanelli, F.; Uccheddu, F.; Servi, M.; Volpe, Y.; Vagnoli, L.; Amore, E.; et al. 3D-Printed Patient-Specific Casts for the Distal Radius in Children: Outcome and Pre-Market Survey. Materials 2022, 15, 2863. [Google Scholar] [CrossRef]
- Cheng, K.W.; Peng, Y.; Chen, T.L.W.; Zhang, G.; Cheung, J.C.W.; Lam, W.K.; Wong, D.W.C.; Zhang, M. A three-dimensional printed foot orthosis for flexible flatfoot: An exploratory biomechanical study on arch support reinforcement and undercut. Materials 2021, 14, 5297. [Google Scholar] [CrossRef] [PubMed]
- Lou, E.; Ng, K.; Hill, D. Immediate Outcomes and Benefits of 3D Printed Braces for the Treatment of Adolescent Idiopathic Scoliosis. Front. Rehabil. Sci. 2022, 3, 1–7. [Google Scholar] [CrossRef]
- Lin, Y.; Cheung, J.P.Y.; Chan, C.K.; Wong, S.W.F.; Cheung, K.M.C.; Wong, M.; Wong, W.C.; Cheung, P.W.H.; Wong, M.S. A Randomized Controlled Trial to Evaluate the Clinical Effectiveness of 3D-Printed Orthosis in the Management of Adolescent Idiopathic Scoliosis. Spine 2021, 47, 13–20. [Google Scholar] [CrossRef]
- Zhang, Y.; Liang, J.; Xu, N.; Zeng, L.; Du, C.; Du, Y.; Zeng, Y.; Yu, M.; Liu, Z. 3D-printed brace in the treatment of adolescent idiopathic scoliosis: A study protocol of a prospective randomised controlled trial. BMJ Open 2020, 10, e038373. [Google Scholar] [CrossRef]
- Sanz-Pena, I.; Arachchi, S.; Halwala-Vithanage, D.; Mallikarachchi, S.; Kirumbara-Liyanage, J.; McGregor, A.; Silva, P.; Newell, N. Characterising the mould rectification process for designing scoliosis braces: Towards automated digital design of 3d-printed braces. Appl. Sci. 2021, 11, 4665. [Google Scholar] [CrossRef]
- Li, J.; Tanaka, H. Feasibility study applying a parametric model as the design generator for 3D–printed orthosis for fracture immobilization. 3D Print. Med. 2018, 4, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Khanal, M.; Arazpour, M.; Bahramizadeh, M.; Samadian, M.; Hutchins, S.W.; Kashani, R.V.; Mardani, M.A.; Tari, H.V.; Aboutorabi, A.; Curran, S.; et al. The influence of thermoplastic thoraco lumbo sacral orthoses on standing balance in subjects with idiopathic scoliosis. Prosthet. Orthot. Int. 2016, 40, 460–466. [Google Scholar] [CrossRef]
- Sadeghi, H.; Allard, P.; Barbier, F.; Chavet, P.; Gatto, L.; Rivard, C.H.; Hinse, S.; Simoneau, M. Bracing has no effect on standing balance in females with adolescent idiopathic scoliosis. Med. Sci. Monit. 2008, 14, CR293–CR298. [Google Scholar] [PubMed]
- Paolucci, T.; Morone, G.; Cesare, A.D.; Grasso, M.R.; Fusco, A.; Paolucci, S.; Saraceni, V.M.; Iosa, M. Effect of Chêneau brace on postural balance in adolescent idiopathic scoliosis: A pilot study. Eur. J. Phys. Rehabil. Med. 2013, 49, 649–657. [Google Scholar] [PubMed]
- Karimi, M.T.; Kavyani, M.; Kamali, M. Balance and gait performance of scoliotic subjects: A review of the literature. J. Back Musculoskelet. Rehabil. 2016, 29, 403–415. [Google Scholar] [CrossRef]
- Gaudreault, N.; Bertrand Arsenault, A.; Larivière, C.; Deserres, S.J.; Rivard, C.H. Assessment of the paraspinal muscles of subjects presenting an idiopathic scoliosis: An EMG pilot study. BMC Musculoskelet. Disord. 2005, 6, 14. [Google Scholar] [CrossRef]
- Pouliot-Laforte, A.; Lemay, M.; Rauch, F.; Veilleux, L.N. Static Postural Control in Youth With Osteogenesis Imperfecta Type I. Arch. Phys. Med. Rehabil. 2017, 98, 1948–1954. [Google Scholar] [CrossRef]
- Nault, M.-L.; Allard, P.; Hinse, S.; Le Blanc, R.; Caron, O.; Labelle, H.; Sadeghi, H. Relations between standing stability and body posture parameters in adolescent idiopathic scoliosis. Spine 2002, 27, 1911–1917. [Google Scholar] [CrossRef]
- Gauchard, G.C.; Lascombes, P.; Kuhnast, M.; Perrin, P.P. Influence of different types of progressive idiopathic scoliosis on static and dynamic postural control. Spine 2001, 26, 1052–1058. [Google Scholar] [CrossRef] [PubMed]
- Moe-Nilssen, R.; Helbostad, J.L. Trunk accelerometry as a measure of balance control during quiet standing. Gait Posture 2002, 16, 60–68. [Google Scholar] [CrossRef]
- Redaelli, D.F.; Abbate, V.; Storm, F.A.; Ronca, A.; Sorrentino, A.; De Capitani, C.; Biffi, E.; Ambrosio, L.; Colombo, G.; Fraschini, P. 3D printing orthopedic scoliosis braces: A test comparing FDM with thermoforming. Int. J. Adv. Manuf. Technol. 2020, 111, 1707–1720. [Google Scholar] [CrossRef]
- Redaelli, D.F.; Barsanti, S.G.; Biffi, E.; Storm, F.A. Comparison of geometrical accuracy of active devices for 3D orthopaedic reconstructions. Int. J. Adv. Manuf. Technol. 2021, 114, 319–342. [Google Scholar] [CrossRef]
- Ronca, A.; Abbate, V.; Redaelli, D.F.; Storm, F.A.; Cesaro, G.; De Capitani, C.; Sorrentino, A.; Colombo, G.; Fraschini, P.; Ambrosio, L. A Comparative Study for Material Selection in 3D Printing of Scoliosis Back Brace. Materials 2022, 15, 5724. [Google Scholar] [CrossRef] [PubMed]
- Ghislieri, M.; Gastaldi, L.; Pastorelli, S.; Tadano, S.; Agostini, V. Wearable Inertial Sensors to Assess Standing Balance: A Systematic Review. Sensors 2019, 19, 4075. [Google Scholar] [CrossRef] [PubMed]
- Mancini, M.; Salarian, A.; Carlson-Kuhta, P.; Zampieri, C.; King, L.; Chiari, L.; Horak, F.B. ISway: A sensitive, valid and reliable measure of postural control. J. Neuroeng. Rehabil. 2012, 9, 59. [Google Scholar] [CrossRef]
- Moe-Nilssen, R. Test-retest reliability of trunk accelerometry during standing and walking. Arch. Phys. Med. Rehabil. 1998, 79, 1377–1385. [Google Scholar] [CrossRef]
- Miller, L.A.; Pickerill, T.; Kuiken, T.A. A novel, low-cost transradial socket fabrication method using mass-producible components and expanding rigid foam. Prosthet. Orthot. Int. 2020, 45, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Casavola, C.; Cazzato, A.; Moramarco, V.; Pappalettere, C. Orthotropic mechanical properties of fused deposition modelling parts described by classical laminate theory. Mater. Des. 2016, 90, 453–458. [Google Scholar] [CrossRef]
- Pollak, M.; Torok, J.; Zajac, J.; Kocisko, M.; Teliskova, M. The structural design of 3D print head and execution of printing via the robotic arm ABB IRB 140. In Proceedings of the 2018 5th International Conference on Industrial Engineering and Applications (ICIEA), Singapore, 26–28 April 2018; pp. 194–198. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Typical Value | Range |
|---|---|---|
| Layer height | 0.6 mm with a 1.2 mm nozzle | 0.4–0.6 mm |
| Line width | 1.1 mm | 1.0–1.25 mm |
| Wall thickness | 2.2 mm | 2.0–2.5 mm |
| Z-seam alignment | Close to the brace aperture | NA |
| Infill density | No infill (only wall lines) | NA |
| Printing temperature | 240 °C | 230–250 °C |
| Build plate temperature | 90 °C | NA |
| Flow | 110% | 103–110% |
| Speed | 35 mm/s | 25–35 mm/s |
| Build plate adhesion type | Brim (5 lines)—150 mm | NA |
| Production Phase | Level | Criteria Description |
|---|---|---|
| 3D chest acquisition | Not acceptable | More than five attempts were needed for a successful scan |
| Acceptable | Four or five attempts were needed for a successful scan | |
| Good | Two or three attempts were needed for a successful scan | |
| Optimal | The scan was performed successfully at the first attempt | |
| CAD design | Not acceptable | The CAD design was successful after more than 3 h |
| Acceptable | The CAD design process lasted 2 to 3 h | |
| Good | The CAD design process lasted 1 to 2 h | |
| Optimal | The CAD design process lasted less than 1 h | |
| Additive manufacturing | Not acceptable | Production was successful after more than three attempts |
| Acceptable | Production was successful at the third attempt | |
| Good | Production was successful at the second attempt | |
| Optimal | Production was successful at the first attempt | |
| Post-processing | Not acceptable | Post-processing lasted more than 1.5 h |
| Acceptable | Post-processing lasted 1 to 1.5 h | |
| Good | Post-processing lasted 0.5 to 1 h | |
| Optimal | Post-processing lasted less than 0.5 h |
| Balance Metric | Definition of Metric |
|---|---|
| Range | Range in the mediolateral (mL) and anteroposterior (ap) directions (m/s2) |
| Root mean square | Acceleration root mean square in the mediolateral (mL) and anteroposterior (ap) directions (m/s2) |
| Sway path length | Accelerometer trajectory length in the horizontal plane (m/s2) |
| 95% Ellipse sway normalized area | Elliptical area that encapsulates 95% of the accelerometer sway path in the horizontal plane, normalized to the duration of the test (m2/s5) |
| Normalized jerk index | First time derivative of the acceleration signal, normalized to the duration of the test (-) |
| Frequency dispersion | Measure of the variability of the frequency content (occupied bandwidth) of the power spectral density, in the mediolateral and anteroposterior directions, zero for pure sinusoid, increases with spectral bandwidth to one (-) |
| ID | 3D Chest Acquisition | CAD Design Process | Additive Manufacturing | Post-Processing |
|---|---|---|---|---|
| 1 | Optimal (#1) | Not acceptable (1 h 40 min) | Not acceptable (#5) | Acceptable (1 h 40 min) |
| 2 | Optimal (#1) | Good (1 h 40 min) | Optimal (#1) | Good (40 min) |
| 3 | Optimal (#1) | Acceptable (2 h) | Good (#2) | Good (45 min) |
| 4 | Optimal (#1) | Good (1 h 40 min) | Optimal (#1) | Acceptable (1 h 20 min) |
| 5 | Acceptable (#5) | Good (1 h) | Optimal (#1) | Acceptable (1 h 40 min) |
| 6 | Optimal (#1) | Good (1 h 20 min) | Optimal (#1) | Acceptable (1 h 20 min) |
| 7 | Optimal (#1) | Good (1 h 20 min) | Optimal (#1) | Acceptable (1 h 20 min) |
| 8 | Optimal (#1) | Good (1 h 20 min) | Optimal (#1) | Good (1 h) |
| 9 | Optimal (#1) | Good (1 h 20 min) | Optimal (#1) | Good (50 min) |
| 10 | Optimal (#1) | Optimal (40 min) | Optimal (#1) | Good (1 h) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Storm, F.A.; Redaelli, D.F.; Biffi, E.; Reni, G.; Fraschini, P. Additive Manufacturing of Spinal Braces: Evaluation of Production Process and Postural Stability in Patients with Scoliosis. Materials 2022, 15, 6221. https://doi.org/10.3390/ma15186221
Storm FA, Redaelli DF, Biffi E, Reni G, Fraschini P. Additive Manufacturing of Spinal Braces: Evaluation of Production Process and Postural Stability in Patients with Scoliosis. Materials. 2022; 15(18):6221. https://doi.org/10.3390/ma15186221
Chicago/Turabian StyleStorm, Fabio Alexander, Davide Felice Redaelli, Emilia Biffi, Gianluigi Reni, and Paolo Fraschini. 2022. "Additive Manufacturing of Spinal Braces: Evaluation of Production Process and Postural Stability in Patients with Scoliosis" Materials 15, no. 18: 6221. https://doi.org/10.3390/ma15186221