Young Adults’ Lived Experiences with Cancer-Related Cognitive Impairment: An Exploratory Qualitative Study


Abstract
:1. Introduction
Current Study
2. Materials and Methods
2.1. Design
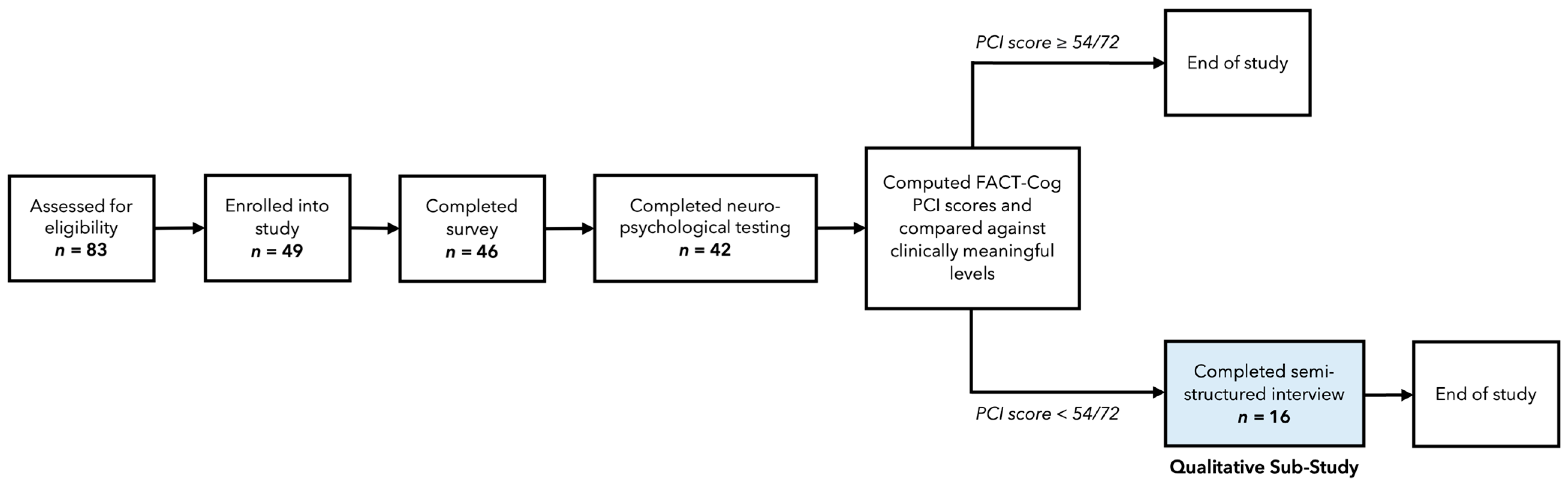
2.2. Participants and Procedures
2.3. Measures
2.3.1. Sociodemographic and Medical Characteristics
2.3.2. Self-Reported Cognitive Function
2.3.3. PA
2.3.4. Interviews
2.4. Interviewer
2.5. Sample Size
2.6. Data Analysis
2.7. Study Rigour
3. Results
3.1. Sample
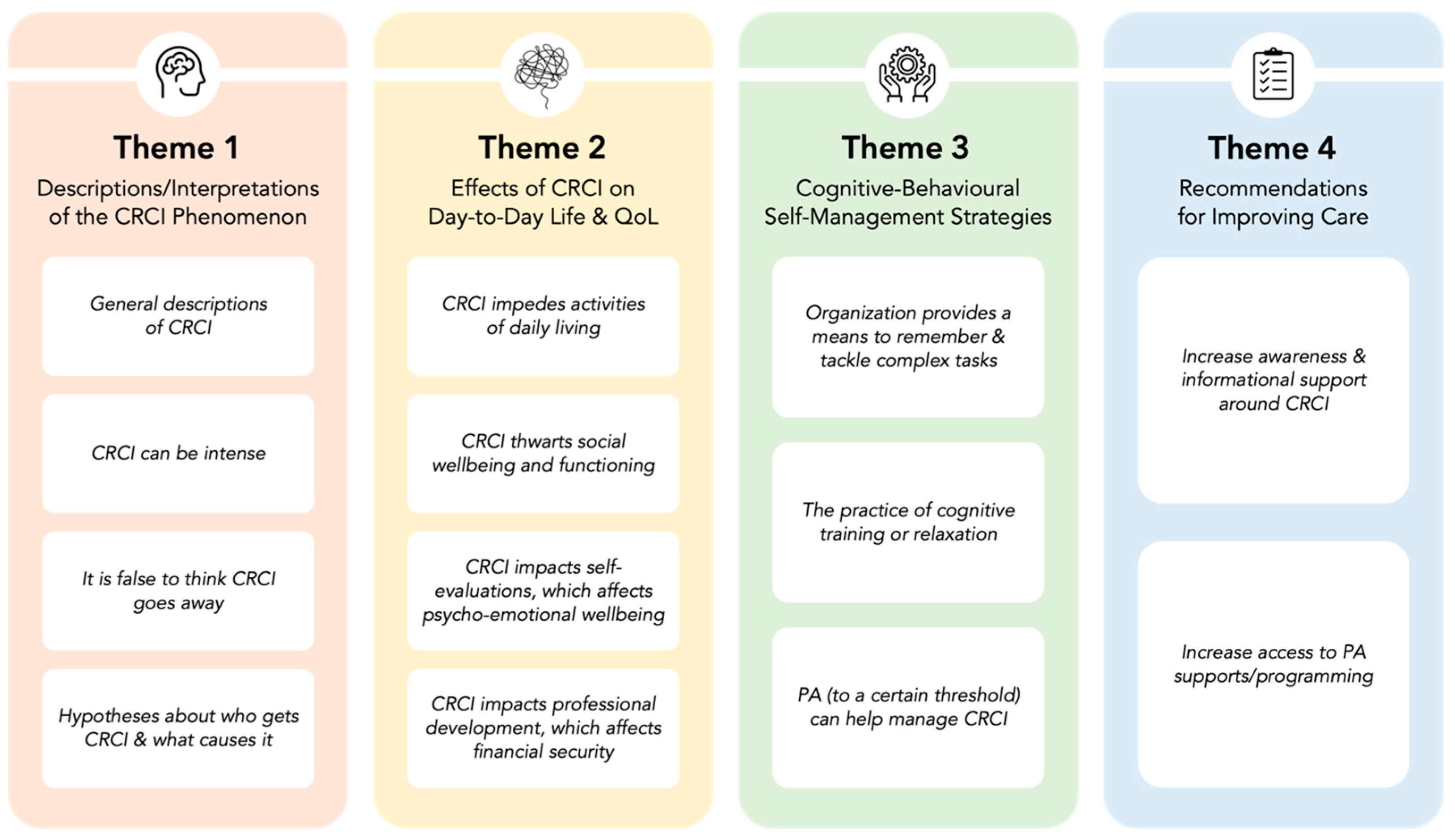
3.2. Themes
3.2.1. Theme 1: Descriptions and Interpretations of the CRCI Phenomenon
3.2.2. Theme 2: Effects of CRCI on Day-to-Day Life and QoL
3.2.3. Theme 3: Cognitive–Behavioural Self-Management Strategies
3.2.4. Theme 4: Recommendations for Improving Care
4. Discussion
4.1. CRCI Is Consequential for Young Adults
4.2. Self-Managing CRCI
4.3. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, S.; Harper, A.; Ruan, Y.; Barr, R.; Frazier, A.L.; Ferlay, J.; Steliarova-Foucher, E.; Fidler-Benaoudia, M.M. International trends in the incidence of cancer among adolescents and young adults. J. Natl. Cancer Inst. 2020, 112, 1105–1117. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A.; Ferrari, A.; Whelan, J.; Barr, R.D. Global assessment of cancer incidence and survival in adolescents and young adults. Pediatr. Blood Cancer 2017, 64. [Google Scholar] [CrossRef] [PubMed]
- Quinn, G.P.; Goncalves, V.; Sehovic, I.; Bowman, M.L.; Reed, D.R. Quality of life in adolescent and young adult cancer patients: A systematic review of the literature. Patient Relat. Outcome Meas. 2015, 6, 19–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, M.; Licaj, I.; Clarisse, B.; Humbert, X.; Grellard, J.M.; Tron, L.; Joly, F. Cognitive complaints in cancer survivors and expectations for support: Results from a web-based survey. Cancer Med. 2019, 8, 2654–2663. [Google Scholar] [CrossRef] [Green Version]
- Lange, M.; Joly, F.; Vardy, J.; Ahles, T.; Dubois, M.; Tron, L.; Winocur, G.; De Ruiter, M.B.; Castel, H. Cancer-related cognitive impairment: An update on state of the art, detection, and management strategies in cancer survivors. Ann. Oncol. 2019, 30, 1925–1940. [Google Scholar] [CrossRef] [Green Version]
- Janelsins, M.C.; Kohli, S.; Mohile, S.G.; Usuki, K.; Ahles, T.A.; Morrow, G.R. An update on cancer- and chemotherapy-related cognitive dysfunction: Current status. Semin. Oncol. 2011, 38, 431–438. [Google Scholar] [CrossRef] [Green Version]
- Collins, B.; Mackenzie, J.; Tasca, G.A.; Scherling, C.; Smith, A. Persistent cognitive changes in breast cancer patients 1 year following completion of chemotherapy. J. Int. Neuropsychol. Soc. 2014, 20, 370–379. [Google Scholar] [CrossRef]
- Janelsins, M.C.; Heckler, C.E.; Peppone, L.J.; Kamen, C.; Mustian, K.M.; Mohile, S.G.; Magnuson, A.; Kleckner, I.R.; Guido, J.J.; Young, K.L.; et al. Cognitive complaints in survivors of breast cancer after chemotherapy compared with age-matched controls: An analysis from a nationwide, multicenter, prospective longitudinal study. J. Clin. Oncol. 2017, 35, 506–514. [Google Scholar] [CrossRef]
- Dewar, E.O.; Ahn, C.; Eraj, S.; Mahal, B.A.; Sanford, N.N. Psychological distress and cognition among long-term survivors of adolescent and young adult cancer in the USA. J. Cancer Surv. 2021, 15, 776–784. [Google Scholar] [CrossRef]
- Epelman, C.L. The adolescent and young adult with cancer: State of the art—Psychosocial aspects. Curr. Oncol. Rep. 2013, 15, 325–331. [Google Scholar] [CrossRef]
- Brower, K.; Schmitt-Boshnick, M.; Haener, M.; Wilks, S.; Soprovich, A. The use of patient-reported outcome measures in primary care: Applications, benefits and challenges. J. Patient-Reported Outcomes 2021, 5, 84. [Google Scholar] [CrossRef] [PubMed]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.J.M.; et al. The European Organisation for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Wagner, L.S.J.; Butt, Z.; Lai, J.; Cella, D. Measuring patient self-reported cognitive function: Development of the Functional Assessment of Cancer Therapy–Cognitive Function instrument. J. Support. Oncol. 2009, 7, 32–39. [Google Scholar]
- Broadbent, D.E.; Cooper, P.F.; FitzGerald, P.; Parkes, K.R. The Cognitive Failures Questionnaire (CFQ) and its correlates. Br. J. Clin. Psychol. 1982, 21, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Henneghan, A.M.; Van Dyk, K.; Kaufmann, T.; Harrison, R.; Gibbons, C.; Heijnen, C.; Kesler, S.R. Measuring self-reported cancer-related cognitive impairment: Recommendations from the Cancer Neuroscience Initiative Working Group. J. Natl. Cancer Inst. 2021, 113, 1625–1633. [Google Scholar] [CrossRef]
- Bray, V.J.; Dhillon, H.M.; Vardy, J.L. Systematic review of self-reported cognitive function in cancer patients following chemotherapy treatment. J. Cancer Surviv. 2018, 12, 537–559. [Google Scholar] [CrossRef]
- Brunet, J.; Sharma, S. A scoping review of studies exploring physical activity and cognition among persons with cancer. J. Cancer Surviv. 2023. manuscript submitted. [Google Scholar]
- Zeng, Y.; Cheng, A.S.; Liu, X.; Chan, C.C. Cervical cancer survivors’ perceived cognitive complaints and supportive care needs in mainland China: A qualitative study. BMJ Open 2017, 7, e014078. [Google Scholar] [CrossRef] [Green Version]
- Henderson, F.M.; Cross, A.J.; Baraniak, A.R. ‘A new normal with chemobrain’: Experiences of the impact of chemotherapy-related cognitive deficits in long-term breast cancer survivors. Health Psychol. Open 2019, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Crotty, M. The Foundations of Social Research: Meaning and Perspective in the Research Process; SAGE Publications: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Selamat, M.H.; Loh, S.Y.; Mackenzie, L.; Vardy, J. Chemobrain experienced by breast cancer survivors: A meta-ethnography study investigating research and care implications. PLoS ONE 2014, 9, e108002. [Google Scholar] [CrossRef] [Green Version]
- Erickson, K.I.; Kramer, A.F. Aerobic exercise effects on cognitive and neural plasticity in older adults. Br. J. Sports Med. 2009, 43, 22–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groot, C.; Hooghiemstra, A.M.; Raijmakers, P.G.; van Berckel, B.N.; Scheltens, P.; Scherder, E.J.; van der Flier, W.M.; Ossenkoppele, R. The effect of physical activity on cognitive function in patients with dementia: A meta-analysis of randomized control trials. Ageing Res. Rev. 2016, 25, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Jia, R.X.; Liang, J.H.; Xu, Y.; Wang, Y.Q. Effects of physical activity and exercise on the cognitive function of patients with Alzheimer disease: A meta-analysis. BMC Geriatr. 2019, 19, 181. [Google Scholar] [CrossRef]
- Zheng, G.; Xia, R.; Zhou, W.; Tao, J.; Chen, L. Aerobic exercise ameliorates cognitive function in older adults with mild cognitive impairment: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2016, 50, 1443–1450. [Google Scholar] [CrossRef]
- Den Heijer, A.E.; Groen, Y.; Tucha, L.; Fuermaier, A.B.; Koerts, J.; Lange, K.W.; Thome, J.; Tucha, O. Sweat it out? The effects of physical exercise on cognition and behavior in children and adults with ADHD: A systematic literature review. J. Neural Transm. 2017, 124, 3–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambez, B.; Harwood-Gross, A.; Golumbic, E.Z.; Rassovsky, Y. Non-pharmacological interventions for cognitive difficulties in ADHD: A systematic review and meta-analysis. J. Psychiatr. Res. 2020, 120, 40–55. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Manzano, S.; Ruiz-Ariza, A.; De La Torre-Cruz, M.; Martinez-Lopez, E.J. Acute and chronic effect of physical activity on cognition and behaviour in young people with ADHD: A systematic review of intervention studies. Res. Dev. Disabil. 2018, 77, 12–23. [Google Scholar] [CrossRef]
- Galiano-Castillo, N.; Arroyo-Morales, M.; Lozano-Lozano, M.; Fernandez-Lao, C.; Martin-Martin, L.; Del-Moral-Avila, R.; Cantarero-Villanueva, I. Effect of an Internet-based telehealth system on functional capacity and cognition in breast cancer survivors: A secondary analysis of a randomized controlled trial. Support. Care Cancer 2017, 25, 3551–3559. [Google Scholar] [CrossRef]
- Gokal, K.; Munir, F.; Ahmed, S.; Kancherla, K.; Wallis, D. Does walking protect against decline in cognitive functioning among breast cancer patients undergoing chemotherapy? Results from a small randomised controlled trial. PLoS ONE 2018, 13, e0206874. [Google Scholar] [CrossRef]
- Myers, J.S. Chemotherapy-related cognitive impairment: The breast cancer experience. Oncol. Nurs. Forum 2012, 39, E31–E40. [Google Scholar] [CrossRef] [Green Version]
- Campbell, K.L.; Zadravec, K.; Bland, K.A.; Chesley, E.; Wolf, F.; Janelsins, M.C. The effect of exercise on cancer-related cognitive impairment and applications for physical therapy: Systematic review of randomized controlled trials. Phys. Ther. 2020, 100, 523–542. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dyk, K.V.; Crespi, C.M.; Petersen, L.; Ganz, P.A. Identifying cancer-related cognitive impairment using the FACT-Cog perceived cognitive impairment. JNCI Cancer Spectr. 2020, 4, pkz099. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Godin, G.; Shephard, R.J. A simple method to assess exercise behavior in the community. Can. J. Appl. Sport. Sci. 1985, 10, 141–146. [Google Scholar]
- Godin, G. The Godin-Shephard leisure-time physical activity questionnaire. Health Fitness J. Can. 2011, 4, 18–22. [Google Scholar]
- Jacobs, D.R., Jr.; Ainsworth, B.E.; Hartman, T.J.; Leon, A.S. A simultaneous evaluation of 10 commonly used physical activity questionnaires. Med. Science Sports Exerc. 1993, 25, 81–91. [Google Scholar] [CrossRef]
- Amireault, S.; Godin, G.; Lacombe, J.; Sabiston, C.M. The use of the Godin-Shephard Leisure-Time Physical Activity Questionnaire in oncology research: A systematic review. BMC Med. Res. Methodol. 2015, 15, 60. [Google Scholar] [CrossRef] [Green Version]
- Fontana, A.; Frey, J.H. The interview: From neutral stance to political involvement. In The SAGE Handbook of Qualitative Research, 3rd ed.; Denzin, N.K., Lincoln, Y.S., Eds.; SAGE Publications: Thousand Oaks, CA, USA, 2005; pp. 695–727. [Google Scholar]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine Publishing: Chicago, IL, USA, 1967. [Google Scholar]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Smith, J.A.; Osborn, M. Interpretative phenomenological analysis. In Qualitative Psychology: A Practical Guide to Research Methods; Smith, J.A., Ed.; SAGE Publications: London, UK, 2003; pp. 51–80. [Google Scholar]
- Smith, B.; McGannon, K.R. Developing rigor in qualitative research: Problems and opportunities within sport and exercise psychology. Int. Rev. Sport. Exerc. Psychol. 2018, 11, 101–121. [Google Scholar] [CrossRef]
- Vizer, L.M.; Mikles, S.P.; Piepmeier, A.T. Cancer-related cognitive impairment in survivors of adolescent and young adult non-central nervous system cancer: A scoping review. Psycho-Oncology 2022, 31, 1275–1285. [Google Scholar] [CrossRef] [PubMed]
- Dahl, A.A.; Fossa, S.D.; Lie, H.C.; Loge, J.H.; Reinertsen, K.V.; Ruud, E.; Kiserud, C.E. Employment status and work ability in long-term young adult cancer survivors. J. Adolesc. Young Adult Oncol. 2019, 8, 304–311. [Google Scholar] [CrossRef]
- Brock, H.; Friedrich, M.; Sender, A.; Richter, D.; Geue, K.; Mehnert-Theuerkauf, A.; Leuteritz, K. Work ability and cognitive impairments in young adult cancer patients: Associated factors and changes over time-results from the AYA-Leipzig study. J. Cancer Surviv. 2022, 16, 771–780. [Google Scholar] [CrossRef] [PubMed]
- Ketterl, T.G.; Syrjala, K.L.; Casillas, J.; Jacobs, L.A.; Palmer, S.C.; McCabe, M.S.; Ganz, P.A.; Overholser, L.; Partridge, A.; Rajotte, E.J.; et al. Lasting effects of cancer and its treatment on employment and finances in adolescent and young adult cancer survivors. Cancer 2019, 125, 1908–1917. [Google Scholar] [CrossRef] [Green Version]
- Boykoff, N.; Moieni, M.; Subramanian, S.K. Confronting chemobrain: An in-depth look at survivors’ reports of impact on work, social networks, and health care response. J. Cancer Surviv. 2009, 3, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Cheung, Y.T.; Shwe, M.; Tan, Y.P.; Fan, G.; Ng, R.; Chan, A. Cognitive changes in multiethnic Asian breast cancer patients: A focus group study. Ann. Oncol. 2012, 23, 2547–2552. [Google Scholar] [CrossRef]
- Munir, F.; Burrows, J.; Yarker, J.; Kalawsky, K.; Bains, M. Women’s perceptions of chemotherapy-induced cognitive side affects on work ability: A focus group study. J. Clin. Nurs. 2010, 19, 1362–1370. [Google Scholar] [CrossRef] [Green Version]
- Von Ah, D.; Habermann, B.; Carpenter, J.S.; Schneider, B.L. Impact of perceived cognitive impairment in breast cancer survivors. Eur. J. Oncol. Nurs. 2013, 17, 236–241. [Google Scholar] [CrossRef]
- Dhillon, H.M.; Tannock, I.F.; Pond, G.R.; Renton, C.; Rourke, S.B.; Vardy, J.L. Perceived cognitive impairment in people with colorectal cancer who do and do not receive chemotherapy. J. Cancer Surviv. 2018, 12, 178–185. [Google Scholar] [CrossRef]
- Pullens, M.J.; De Vries, J.; Van Warmerdam, L.J.; Van De Wal, M.A.; Roukema, J.A. Chemotherapy and cognitive complaints in women with breast cancer. Psycho-Oncology 2013, 22, 1783–1789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ganz, P.A.; Kwan, L.; Castellon, S.A.; Oppenheim, A.; Bower, J.E.; Silverman, D.H.; Cole, S.W.; Irwin, M.R.; Ancoli-Israel, S.; Belin, T.R. Cognitive complaints after breast cancer treatments: Examining the relationship with neuropsychological test performance. J. Natl. Cancer Inst. 2013, 105, 791–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schilder, C.M.; Seynaeve, C.; Linn, S.C.; Boogerd, W.; Beex, L.V.; Gundy, C.M.; Nortier, J.W.; van de Velde, C.J.; van Dam, F.S.; Schagen, S.B. Self-reported cognitive functioning in postmenopausal breast cancer patients before and during endocrine treatment: Findings from the neuropsychological TEAM side-study. Psycho-Oncology 2012, 21, 479–487. [Google Scholar] [CrossRef]
- Yang, Y.; Hendrix, C.C. Cancer-related cognitive impairment in breast cancer patients: Influences of psychological variables. Asia-Pac. J. Oncol. Nurs. 2018, 5, 296–306. [Google Scholar] [CrossRef]
- Pearce, S.; Whelan, J.; Kelly, D.; Gibson, F. Renegotiation of identity in young adults with cancer: A longitudinal narrative study. Int. J. Nurs. Stud. 2020, 102, 103465. [Google Scholar] [CrossRef]
- Huysse-Gaytandjieva, A.; Groot, W.; Pavlova, M.; Joling, C. Low self-esteem predicts future unemployment. J. Appl. Econ. 2015, 18, 325–346. [Google Scholar] [CrossRef]
- Statistics Canada. A Generational Portrait of Canada’s Aging Population from the 2021 Census. Available online: https://www12.statcan.gc.ca/census-recensement/2021/as-sa/98-200-X/2021003/98-200-X2021003-eng.cfm (accessed on 2 April 2023).
- Stone, D.S.; Ganz, P.A.; Pavlish, C.; Robbins, W.A. Young adult cancer survivors and work: A systematic review. J. Cancer Surviv. 2017, 11, 765–781. [Google Scholar] [CrossRef] [Green Version]
- Hampstead, B.M.; Gillis, M.M.; Stringer, A.Y. Cognitive rehabilitation of memory for mild cognitive impairment: A methodological review and model for future research. J. Int. Neuropsychol. Soc. 2014, 20, 135–151. [Google Scholar] [CrossRef] [Green Version]
- Mayo, S.J.; Rourke, S.B.; Atenafu, E.G.; Vitorino, R.; Chen, C.; Kuruvilla, J. Computerized cognitive training in post-treatment hematological cancer survivors: A feasibility study. Pilot. Feasibility Stud. 2021, 7, 36. [Google Scholar] [CrossRef]
- Conklin, H.M.; Ogg, R.J.; Ashford, J.M.; Scoggins, M.A.; Zou, P.; Clark, K.N.; Martin-Elbahesh, K.; Hardy, K.K.; Merchant, T.E.; Jeha, S.; et al. Computerized cognitive training for amelioration of cognitive late effects among childhood cancer survivors: A randomized controlled trial. J. Clin. Oncol. 2015, 33, 3894–3902. [Google Scholar] [CrossRef] [Green Version]
- Simons, D.J.; Boot, W.R.; Charness, N.; Gathercole, S.E.; Chabris, C.F.; Hambrick, D.Z.; Stine-Morrow, E.A. Do “brain-training” programs work? Psychol. Sci. Public. Interest. 2016, 17, 103–186. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, L.; Marshall, K. Effective non-pharmacological interventions for cancer related cognitive impairment in adults (excluding central nervous system or head and neck cancer): Systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2022, 58, 258–270. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Wei, S.; Liu, Q. Effect of cognitive training on patients with breast cancer reporting cognitive changes: A systematic review and meta-analysis. BMJ Open. 2023, 13, e058088. [Google Scholar] [CrossRef] [PubMed]
- Gooch, M.; Mehta, A.; John, T.; Lomeli, N.; Naeem, E.; Mucci, G.; Toh, Y.L.; Chan, A.; Bota, D.A.; Torno, L. Feasibility of cognitive training to promote recovery in cancer-related cognitive impairment in adolescent and young adult patients. J. Adolesc. Young Adult Oncol. 2022, 11, 290–296. [Google Scholar] [CrossRef]
- Milbury, K.; Chaoul, A.; Biegler, K.; Wangyal, T.; Spelman, A.; Meyers, C.A.; Arun, B.; Palmer, J.L.; Taylor, J.; Cohen, L. Tibetan sound meditation for cognitive dysfunction: Results of a randomized controlled pilot trial. Psycho-Oncology 2013, 22, 2354–2363. [Google Scholar] [CrossRef]
- Johns, S.A.; Von Ah, D.; Brown, L.F.; Beck-Coon, K.; Talib, T.L.; Alyea, J.M.; Monahan, P.O.; Tong, Y.; Wilhelm, L.; Giesler, R.B. Randomized controlled pilot trial of mindfulness-based stress reduction for breast and colorectal cancer survivors: Effects on cancer-related cognitive impairment. J. Cancer Surviv. 2016, 10, 437–448. [Google Scholar] [CrossRef] [Green Version]
- Duval, A.; Davis, C.G.; Khoo, E.L.; Romanow, H.; Shergill, Y.; Rice, D.; Smith, A.M.; Poulin, P.A.; Collins, B. Mindfulness-based stress reduction and cognitive function among breast cancer survivors: A randomized controlled trial. Cancer 2022, 128, 2520–2528. [Google Scholar] [CrossRef]
- Alvarez, J.; Meyer, F.L.; Granoff, D.L.; Lundy, A. The effect of EEG biofeedback on reducing postcancer cognitive impairment. Integr. Cancer Ther. 2013, 12, 475–487. [Google Scholar] [CrossRef] [Green Version]
- Freeman, L.W.; White, R.; Ratcliff, C.G.; Sutton, S.; Stewart, M.; Palmer, J.L.; Link, J.; Cohen, L. A randomized trial comparing live and telemedicine deliveries of an imagery-based behavioral intervention for breast cancer survivors: Reducing symptoms and barriers to care. Psycho-Oncology 2015, 24, 910–918. [Google Scholar] [CrossRef] [Green Version]
- Lambert, M.; Wurz, A.; Smith, A.M.; Fang, Z.; Brunet, J. Preliminary evidence of improvement in adolescent and young adult cancer survivors’ brain health following physical activity: A proof-of-concept sub-study. Brain Plast. 2021, 7, 97–109. [Google Scholar] [CrossRef]
- Wurz, A.; Ayson, G.; Smith, A.M.; Brunet, J. A proof-of-concept sub-study exploring feasibility and preliminary evidence for the role of physical activity on neural activity during executive functioning tasks among young adults after cancer treatment. BMC Neurol. 2021, 21, 300. [Google Scholar] [CrossRef] [PubMed]
- Bryant, A.L.; Deal, A.M.; Battaglini, C.L.; Phillips, B.; Pergolotti, M.; Coffman, E.; Foster, M.C.; Wood, W.A.; Bailey, C.; Hackney, A.C.; et al. The effects of exercise on patient-reported outcomes and performance-based physical function in adults with acute leukemia undergoing induction therapy: Exercise and QUality of life in Acute Leukemia (EQUAL). Integr. Cancer Ther. 2018, 17, 263–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morielli, A.R.; Boule, N.G.; Usmani, N.; Tankel, K.; Joseph, K.; Severin, D.; Fairchild, A.; Nijjar, T.; Courneya, K.S. Effects of exercise during and after neoadjuvant chemoradiation on symptom burden and quality of life in rectal cancer patients: A phase II randomized controlled trial. J. Cancer Surviv. 2021. [Google Scholar] [CrossRef]
- Salerno, E.A.; Rowland, K.; Kramer, A.F.; McAuley, E. Acute aerobic exercise effects on cognitive function in breast cancer survivors: A randomized crossover trial. BMC Cancer 2019, 19, 371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological momentary assessment. Ann. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef]
- Diamond, A.; Ling, D.S. Conclusions about interventions, programs, and approaches for improving executive functions that appear justified and those that, despite much hype, do not. Dev. Cogn. Neurosci. 2016, 18, 34–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillman, C.H.; McAuley, E.; Erickson, K.I.; Liu-Ambrose, T.; Kramer, A.F. On mindful and mindless physical activity and executive function: A response to Diamond and Ling (2016). Dev. Cogn. Neurosci. 2019, 37, 100529. [Google Scholar] [CrossRef] [PubMed]
- Gheysen, F.; Poppe, L.; DeSmet, A.; Swinnen, S.; Cardon, G.; De Bourdeaudhuij, I.; Chastin, S.; Fias, W. Physical activity to improve cognition in older adults: Can physical activity programs enriched with cognitive challenges enhance the effects? A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 63. [Google Scholar] [CrossRef] [Green Version]
- Waddington, E.E.; Heisz, J.J. Orienteering experts report more proficient spatial processing and memory across adulthood. PLoS ONE 2023, 18, e0280435. [Google Scholar] [CrossRef]
- Bo, W.; Lei, M.; Tao, S.; Jie, L.T.; Qian, L.; Lin, F.Q.; Ping, W.X. Effects of combined intervention of physical exercise and cognitive training on cognitive function in stroke survivors with vascular cognitive impairment: A randomized controlled trial. Clin. Rehabil. 2019, 33, 54–63. [Google Scholar] [CrossRef]
- Melis, M.; Schroyen, G.; Leenaerts, N.; Smeets, A.; Sunaert, S.; Van der Gucht, K.; Deprez, S. The impact of mindfulness on cancer-related cognitive impairment in breast cancer survivors with cognitive complaints. Cancer 2023, 129, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Cantarero-Villanueva, I.; Fernandez-Lao, C.; Cuesta-Vargas, A.I.; Del Moral-Avila, R.; Fernandez-de-Las-Penas, C.; Arroyo-Morales, M. The effectiveness of a deep water aquatic exercise program in cancer-related fatigue in breast cancer survivors: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Cox, E.; Bells, S.; Timmons, B.W.; Laughlin, S.; Bouffet, E.; de Medeiros, C.; Beera, K.; Harasym, D.; Mabbott, D.J. A controlled clinical crossover trial of exercise training to improve cognition and neural communication in pediatric brain tumor survivors. Clin. Neurophysiol. 2020, 131, 1533–1547. [Google Scholar] [CrossRef] [PubMed]
- Galiano-Castillo, N.; Cantarero-Villanueva, I.; Fernandez-Lao, C.; Ariza-Garcia, A.; Diaz-Rodriguez, L.; Del-Moral-Avila, R.; Arroyo-Morales, M. Telehealth system: A randomized controlled trial evaluating the impact of an internet-based exercise intervention on quality of life, pain, muscle strength, and fatigue in breast cancer survivors. Cancer 2016, 122, 3166–3174. [Google Scholar] [CrossRef]
- Galvao, D.A.; Taaffe, D.R.; Spry, N.; Joseph, D.; Newton, R.U. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: A randomized controlled trial. J. Clin. Oncol. 2010, 28, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Henke, C.C.; Cabri, J.; Fricke, L.; Pankow, W.; Kandilakis, G.; Feyer, P.C.; de Wit, M. Strength and endurance training in the treatment of lung cancer patients in stages IIIA/IIIB/IV. Support. Care Cancer 2014, 22, 95–101. [Google Scholar] [CrossRef]
- Howell, C.R.; Krull, K.R.; Partin, R.E.; Kadan-Lottick, N.S.; Robison, L.L.; Hudson, M.M.; Ness, K.K. Randomized web-based physical activity intervention in adolescent survivors of childhood cancer. Pediatr. Blood Cancer 2018, 65, e27216. [Google Scholar] [CrossRef]
- Janelsins, M.C.; Peppone, L.J.; Heckler, C.E.; Kesler, S.R.; Sprod, L.K.; Atkins, J.; Melnik, M.; Kamen, C.; Giguere, J.; Messino, M.J.; et al. YOCAS(c)(R) yoga reduces self-reported memory difficulty in cancer survivors in a nationwide randomized clinical trial: Investigating relationships between memory and sleep. Integr. Cancer Ther. 2016, 15, 263–271. [Google Scholar] [CrossRef] [Green Version]
- Larkey, L.K.; Roe, D.J.; Smith, L.; Millstine, D. Exploratory outcome assessment of Qigong/Tai Chi Easy on breast cancer survivors. Complement. Ther. Med. 2016, 29, 196–203. [Google Scholar] [CrossRef] [Green Version]
- Miki, E.; Kataoka, T.; Okamura, H. Feasibility and efficacy of speed-feedback therapy with a bicycle ergometer on cognitive function in elderly cancer patients in Japan. Psycho-Oncology 2014, 23, 906–913. [Google Scholar] [CrossRef]
- Oh, B.; Butow, P.N.; Mullan, B.A.; Clarke, S.J.; Beale, P.J.; Pavlakis, N.; Lee, M.S.; Rosenthal, D.S.; Larkey, L.; Vardy, J. Effect of medical Qigong on cognitive function, quality of life, and a biomarker of inflammation in cancer patients: A randomized controlled trial. Support. Care Cancer 2012, 20, 1235–1242. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Park, K.D.; Kim, J.H.; Kim, Y.S.; Kim, E.Y.; Ahn, H.K.; Park, I.; Sym, S.J. Resistance and aerobic exercise intervention during chemotherapy in patients with metastatic cancer: A pilot study in South Korea. Ann. Palliat. Med. 2021, 10, 10236–10243. [Google Scholar] [CrossRef] [PubMed]
- Poier, D.; Bussing, A.; Rodrigues Recchia, D.; Beerenbrock, Y.; Reif, M.; Nikolaou, A.; Zerm, R.; Gutenbrunner, C.; Kroz, M. Influence of a multimodal and multimodal-aerobic therapy concept on health-related quality of life in breast cancer survivors. Integr. Cancer Ther. 2019, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Saarto, T.; Penttinen, H.M.; Sievanen, H.; Kellokumpu-Lehtinen, P.L.; Hakamies-Blomqvist, L.; Nikander, R.; Huovinen, R.; Luoto, R.; Kautiainen, H.; Jarvenpaa, S.; et al. Effectiveness of a 12-month exercise program on physical performance and quality of life of breast cancer survivors. Anticancer. Res. 2012, 32, 3875–3884. [Google Scholar] [PubMed]
- Vadiraja, H.S.; Rao, M.R.; Nagarathna, R.; Nagendra, H.R.; Rekha, M.; Vanitha, N.; Gopinath, K.S.; Srinath, B.S.; Vishweshwara, M.S.; Madhavi, Y.S.; et al. Effects of yoga program on quality of life and affect in early breast cancer patients undergoing adjuvant radiotherapy: A randomized controlled trial. Complement. Ther. Med. 2009, 17, 274–280. [Google Scholar] [CrossRef]
- Van Weert, E.; May, A.M.; Korstjens, I.; Post, W.J.; van der Schans, C.P.; van den Borne, B.; Mesters, I.; Ros, W.J.; Hoekstra-Weebers, J.E. Cancer-related fatigue and rehabilitation: A randomized controlled multicenter trial comparing physical training combined with cognitive-behavioral therapy with physical training only and with no intervention. Phys. Ther. 2010, 90, 1413–1425. [Google Scholar] [CrossRef] [Green Version]
- Zimmer, P.; Baumann, F.T.; Oberste, M.; Schmitt, J.; Joisten, N.; Hartig, P.; Schenk, A.; Kuhn, R.; Bloch, W.; Reuss-Borst, M. Influence of personalized exercise recommendations during rehabilitation on the sustainability of objectively measured physical activity levels, fatigue, and fatigue-related biomarkers in patients with breast cancer. Integr. Cancer Ther. 2018, 17, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Rosenstock, I.M. Why people use health services. Milbank Q. 1966, 44, 94–127. [Google Scholar] [CrossRef] [Green Version]
- Hanin, Y.L. Emotions and Athletic Performance: Individual Zones of Optimal Functioning Model. In European Yearbook of Sport Psychology; FEPSAC: Brussels, Belgium, 1997; pp. 29–72. [Google Scholar]
- Hanin, Y.L. Individual zones of optimal functioning (IZOF) model: Emotions-performance relationships in sport. In Emotions in Sport; Hanin, Y.L., Ed.; Human Kinetics: Champaign, IL, USA, 2000. [Google Scholar]
- Cutter, G.R.; Liu, Y. Personalized medicine: The return of the house call? Neurol. Clin. Pract. 2012, 2, 343–351. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Question Categories | Example Questions and Probes |
|---|---|
| How participants viewed their cognitive function and/or difficulties. | Can you describe your current cognitive function? [Probe] What specific cognitive difficulties or impairments (e.g., impaired memory, attention, ability to process information, etc.) do you experience? Compared to before you were diagnosed, how do you think your cognitive function has changed over the course of your cancer journey? [Probes] After diagnosis? During treatment? Immediately after treatment? What about as time went on after treatment? |
| What they perceived as predisposing factors to their CRCI. | Do you think that being diagnosed when you were ___ years old and now being where you are in life influence how you experience your cognitive difficulties or impairments? How so? Do you think the cognitive difficulties or impairments you are experiencing are due to your specific cancer (i.e., ____) and/or the medications you have received, namely _____? Why/why not? |
| How they felt these impairments have impacted their QoL. | Can you tell me how the cognitive difficulties or impairments you mentioned have affected your emotional and/or psychological wellbeing? [Probe] Has this affected the way you see yourself? How? |
| How they cope with CRCI. | What strategies do you use to manage your cognitive difficulties or impairments? Why these? [Probe] Was/is physical activity one of such strategies? Why so? Why not? |
| Participants’ thoughts on PA as a self-management strategy. | Do you believe PA can improve your cognitive function? Why/why not? [Probes] Do you feel that PA helps improve your memory? Attention? Processing speed? Any other specific cognitive domains? Why or why not? Has anyone ever recommended that you engage in physical activity to improve your cognitive function? If so, who? What did they say? |
| Variables | Values |
|---|---|
| Sociodemographic Characteristics | |
| Current Age (M Years ± SD; Range) | 30.8 ± 6.0; 23–39 |
| Sex, n (% Female) | 14 (87.5) |
| Gender Identity, n (% Woman) | 14 (87.5) |
| Ethnicity, n (% White) | 12 (75.0) |
| Civil Status, n (% Single) | 8 (50) |
| Highest Level of Completed Education, n (% Post-secondary) | 15 (93.8) |
| Vocational Status, n (% Working/Transitioning to Work) | 10 (62.5) |
| Annual Household Income, n (% < CAD $100,000) | 12 (75.0) |
| Medical Characteristics | |
| Age at Diagnosis (M years ± SD; range) | 27.6 ± 7.9; 15–38 |
| Time Since Diagnosis (M years ± SD; range) | 3.2 ± 3.0; 0–10 |
| Cancer Stage, n (%) | |
| I | 1 (6.3) |
| II | 7 (43.8) |
| III | 3 (18.8) |
| N/A or “Do Not Know” | 5 (31.3) |
| Cancer Type, n (%) | |
| Hematological | 4 (25) |
| Breast | 3 (18.8) |
| Sarcoma | 3 (18.8) |
| Brain | 2 (12.5) |
| Carcinoma | 1 (6.3) |
| Gynecologic | 2 (12.5) |
| Colorectal | 0 (0) |
| Melanoma | 1 (6.3) |
| Testicular | 0 (0) |
| Treatments Received, n (%) | |
| Surgery | 13 (81.3) |
| Chemotherapy | 11 (68.8) |
| Radiation | 9 (56.3) |
| Hormonal | 3 (18.8) |
| Other | 3 (18.8) |
| Perceived Overall Health, n (%) | |
| Poor to Fair | 6 (37.5) |
| Good to Very Good | 10 (62.5) |
| Excellent | 0 (0) |
| Previous Concussion(s), n (%) | 2 (12.5) |
| Cannabis Use in the Past Month, n (%) | 7 (43.8) |
| Participant Pseudonym | Sex | Age | Cancer Stage | Cancer Type | Cancer Treatment | PCI Score | MVPA LSI Score/ Classification |
|---|---|---|---|---|---|---|---|
| Cole | M | 25 | II | Hematological | C + R | 8 | 10/Insufficiently active |
| Emma | F | 39 | - a | Breast | S + C + R | 17 | 10/Insufficiently active |
| Erica | F | 28 | II | Brain | S + C + R | 48 | 25/Active |
| Eva | F | 26 | - a | Sarcoma | S + C + R | 38 | 0/Insufficiently active |
| Ivy | F | 32 | - a | Brain | S | 39 | 35/Active |
| Jack | M | 26 | II | Sarcoma | C + R | 54 b | 24/Active |
| Jaime | F | 25 | - a | Hematological | S + C | 31 | 15/Insufficiently active |
| Lauren | F | 25 | - a | Sarcoma | S + C | 51 | 33/Active |
| Layla | F | 29 | II | Hematological | C + R | 41 | 24/Active |
| Mia | F | 38 | II | Carcinoma | S | 35 | 25/Insufficiently active |
| Nina | F | 36 | I | Gynecologic | S | 37 | 5/Insufficiently active |
| Peyton | F | 27 | III | Melanoma | S | 29 | 12.5/Insufficiently active |
| Priya | F | 38 | III | Gynecologic | S + C | 44 | 10/Active |
| Sarah | F | 39 | III | Breast | S + C + R | 33 | NR |
| Sydney | F | 37 | II | Breast | S + C + R | 34 | 46/Active |
| Taylor | F | 23 | II | Hematological | S + C | 37 | 10/Insufficiently active |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharma, S.; Brunet, J. Young Adults’ Lived Experiences with Cancer-Related Cognitive Impairment: An Exploratory Qualitative Study. Curr. Oncol. 2023, 30, 5593-5614. https://doi.org/10.3390/curroncol30060422
Sharma S, Brunet J. Young Adults’ Lived Experiences with Cancer-Related Cognitive Impairment: An Exploratory Qualitative Study. Current Oncology. 2023; 30(6):5593-5614. https://doi.org/10.3390/curroncol30060422
Chicago/Turabian StyleSharma, Sitara, and Jennifer Brunet. 2023. "Young Adults’ Lived Experiences with Cancer-Related Cognitive Impairment: An Exploratory Qualitative Study" Current Oncology 30, no. 6: 5593-5614. https://doi.org/10.3390/curroncol30060422