Prediction of Disease Progression to Upfront Pembrolizumab Monotherapy in Advanced Non-Small-Cell Lung Cancer with High PD-L1 Expression Using Baseline CT Disease Quantification and Smoking Pack Years

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. CT Scan Acquisition and Review
2.3. Statistical Analysis
3. Results
3.1. Summary of Patient’s Baseline Characteristics and Treatment Response at the 1st Follow-Up CT
3.2. Comparison of the Baseline Variables between Patients with PD vs. DC
3.3. Association between Baseline Variables and Progressive Disease (PD)
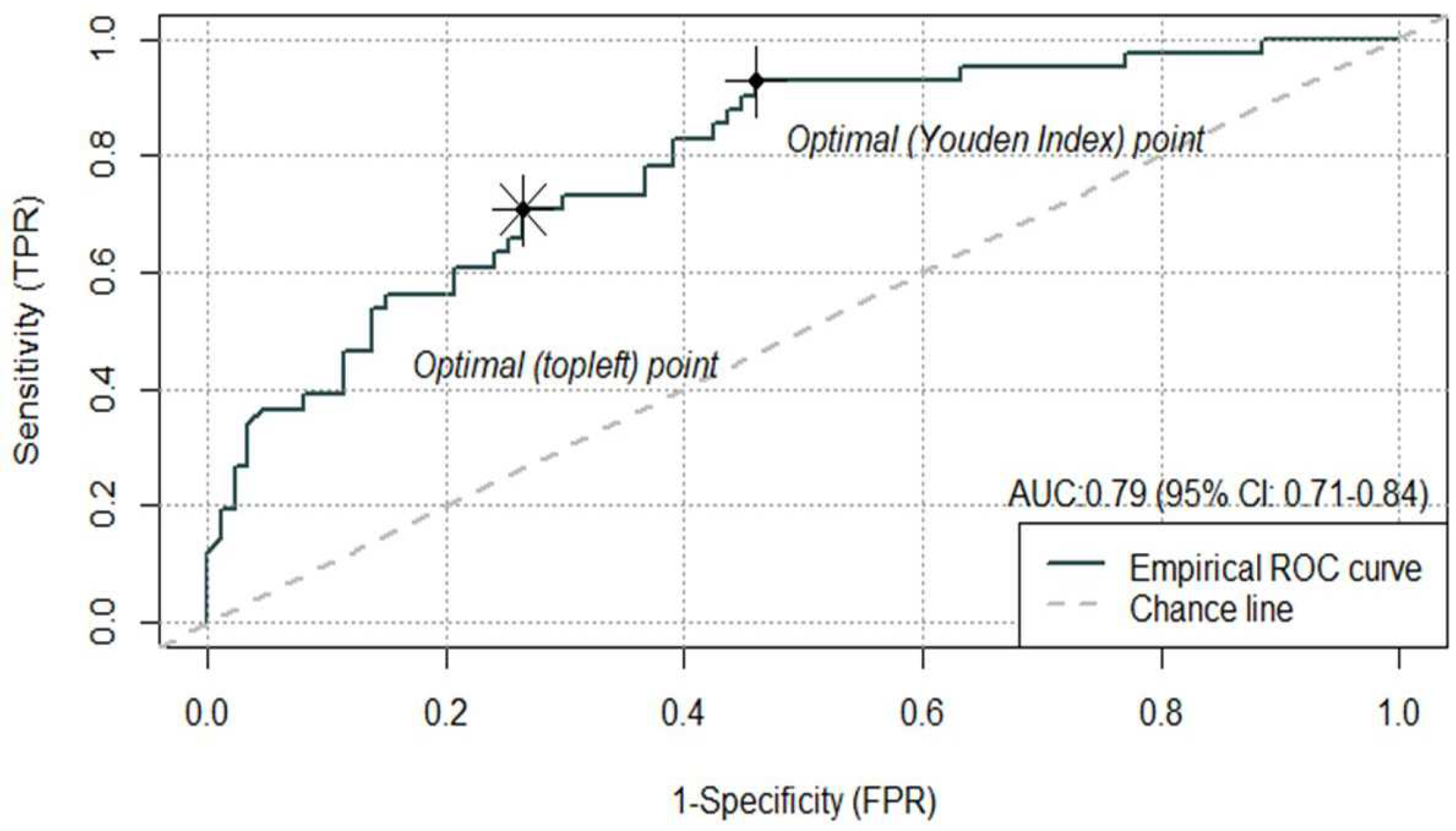
3.4. Performance of the MV Logistic Regression Model in Classifying PD or DC
3.5. Individual Predicted “Risk of Progression” and Predicted “High- vs. Low-Risk of Progression” Groups
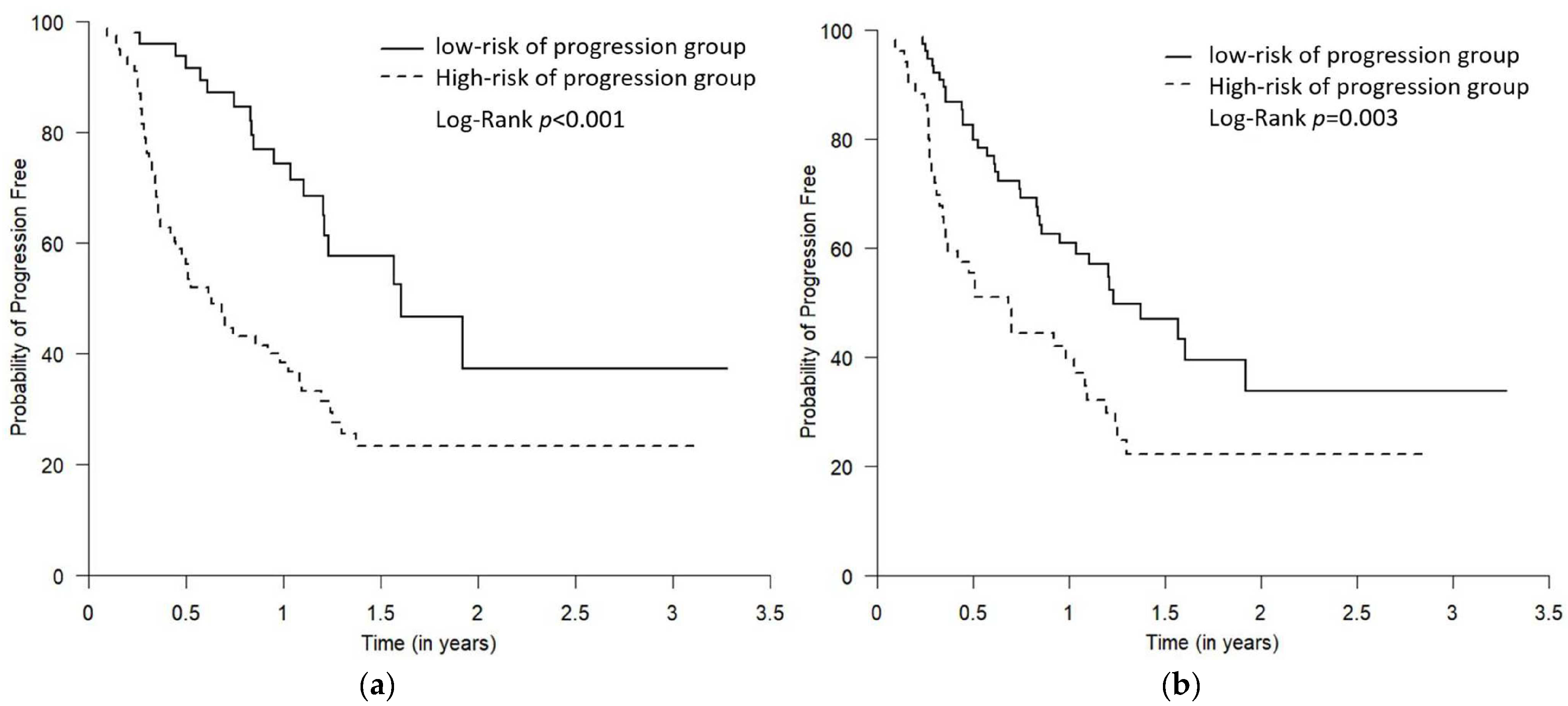
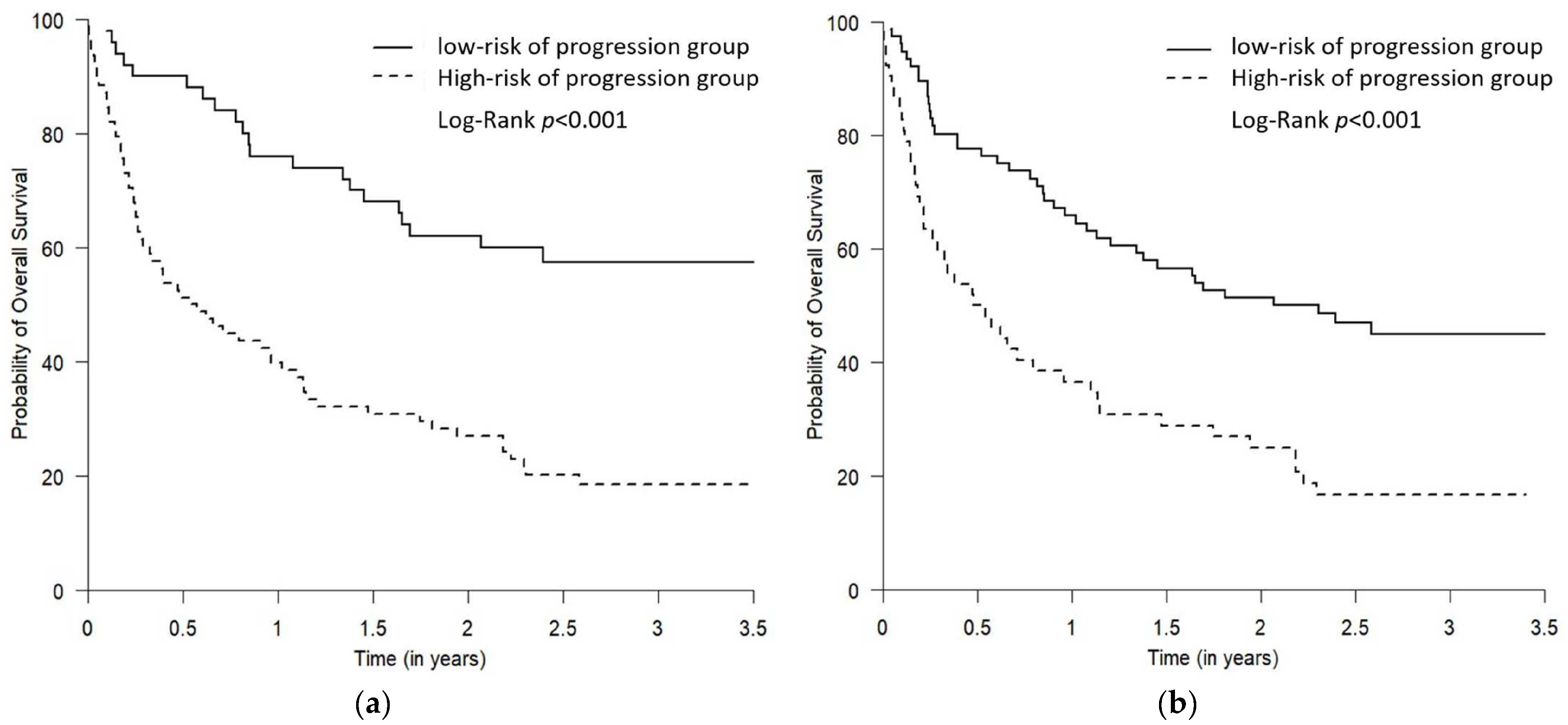
3.6. Survival (PFS and OS) of the Predicted “High- vs. Low-Risk of Progression” Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Canadian Cancer Statistics Advisory Committee in Collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian Cancer Statistics 2021. Toronto, ON: Canadian Cancer Society. 2021. Available online: https://www.cancer.ca/Canadian-Cancer-Statistics-2021-EN (accessed on 5 June 2023).
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Melosky, B.; Blais, N.; Cheema, P.; Couture, C.; Juergens, R.; Kamel-Reid, S.; Tsao, M.S.; Wheatley-Price, P.; Xu, Z.; Ionescu, D.N. Standardizing biomarker testing for Canadian patients with advanced lung cancer. Curr. Oncol. 2018, 25, 73–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gumus, M.; Mazieres, J.; Hermes, B.; Cay Senler, F.; Csoszi, T.; Fulop, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Mok, T.S.K.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; Moro-Sibilot, D.; et al. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): Key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir. Med. 2019, 7, 387–401. [Google Scholar] [CrossRef] [PubMed]
- West, H.; McCleod, M.; Hussein, M.; Morabito, A.; Rittmeyer, A.; Conter, H.J.; Kopp, H.G.; Daniel, D.; McCune, S.; Mekhail, T.; et al. Atezolizumab in combination with carboplatin plus nab-paclitaxel chemotherapy compared with chemotherapy alone as first-line treatment for metastatic non-squamous non-small-cell lung cancer (IMpower130): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 924–937. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-Year Outcomes with Pembrolizumab Versus Chemotherapy for Metastatic Non-Small-Cell Lung Cancer with PD-L1 Tumor Proportion Score ≥ 50. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Perkins, N.J.; Schisterman, E.F. The inconsistency of “optimal” cutpoints obtained using two criteria based on the receiver operating characteristic curve. Am. J. Epidemiol. 2006, 163, 670–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Jiang, W.; Wang, H.; He, J.; Su, C.; Yu, Q. Impact of Smoking History on Response to Immunotherapy in Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 703143. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.T.; Ma, W.Y.; Sun, B.B.; Fan, L.W.; Xu, K.; Hall, S.R.R.; Al-Hurani, M.F.; Schmid, R.A.; Peng, R.W.; Hida, T.; et al. Smoking signature is superior to programmed death-ligand 1 expression in predicting pathological response to neoadjuvant immunotherapy in lung cancer patients. Transl. Lung Cancer Res. 2021, 10, 3807–3822. [Google Scholar] [CrossRef]
- Tinazzi, A.; Cytel Inc. PhUSE 1 Paper IS01: Efficacy Endpoints in Oncology; Cytel Inc.: Geneva, Switzerland, 2013. [Google Scholar]
- Zito Marino, F.; Ascierto, P.A.; Rossi, G.; Staibano, S.; Montella, M.; Russo, D.; Alfano, R.; Morabito, A.; Botti, G.; Franco, R. Are tumor-infiltrating lymphocytes protagonists or background actors in patient selection for cancer immunotherapy? Expert Opin. Biol. 2017, 17, 735–746. [Google Scholar] [CrossRef]
- Kerr, K.M.; Tsao, M.S.; Nicholson, A.G.; Yatabe, Y.; Wistuba, I.I.; Hirsch, F.R.; Committee, I.P. Programmed Death-Ligand 1 Immunohistochemistry in Lung Cancer: In what state is this art? J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2015, 10, 985–989. [Google Scholar] [CrossRef] [Green Version]
- Ma, W.; Gilligan, B.M.; Yuan, J.; Li, T. Current status and perspectives in translational biomarker research for PD-1/PD-L1 immune checkpoint blockade therapy. J. Hematol. Oncol. 2016, 9, 47. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.; Huang, Z.; Teng, F.; Xing, L.; Yu, J. Predictive biomarkers in PD-1/PD-L1 checkpoint blockade immunotherapy. Cancer Treat. Rev. 2015, 41, 868–876. [Google Scholar] [CrossRef]
- He, Y.; Rozeboom, L.; Rivard, C.J.; Ellison, K.; Dziadziuszko, R.; Yu, H.; Zhou, C.; Hirsch, F.R. PD-1, PD-L1 Protein Expression in Non-Small Cell Lung Cancer and Their Relationship with Tumor-Infiltrating Lymphocytes. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2017, 23, 1208–1216. [Google Scholar]
- Hellmann, M.D.; Ciuleanu, T.E.; Pluzanski, A.; Lee, J.S.; Otterson, G.A.; Audigier-Valette, C.; Minenza, E.; Linardou, H.; Burgers, S.; Salman, P.; et al. Nivolumab plus Ipilimumab in Lung Cancer with a High Tumor Mutational Burden. N. Engl. J. Med. 2018, 378, 2093–2104. [Google Scholar] [CrossRef]
- McGranahan, N.; Furness, A.J.; Rosenthal, R.; Ramskov, S.; Lyngaa, R.; Saini, S.K.; Jamal-Hanjani, M.; Wilson, G.A.; Birkbak, N.J.; Hiley, C.T.; et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 2016, 351, 1463–1469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizvi, N.A.; Hellmann, M.D.; Snyder, A.; Kvistborg, P.; Makarov, V.; Havel, J.J.; Lee, W.; Yuan, J.; Wong, P.; Ho, T.S.; et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 2015, 348, 124–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayers, M.; Lunceford, J.; Nebozhyn, M.; Murphy, E.; Loboda, A.; Kaufman, D.R.; Albright, A.; Cheng, J.D.; Kang, S.P.; Shankaran, V.; et al. IFN-gamma-related mRNA profile predicts clinical response to PD-1 blockade. J. Clin. Investig. 2017, 127, 2930–2940. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A.M.; Piccioni, D.; Kato, S.; Boichard, A.; Wang, H.Y.; Frampton, G.; Lippman, S.M.; Connelly, C.; Fabrizio, D.; Miller, V.; et al. Prevalence of PDL1 Amplification and Preliminary Response to Immune Checkpoint Blockade in Solid Tumors. JAMA Oncol. 2018, 4, 1237–1244. [Google Scholar] [CrossRef] [Green Version]
- Offin, M.; Rizvi, H.; Tenet, M.; Ni, A.; Sanchez-Vega, F.; Li, B.T.; Drilon, A.; Kris, M.G.; Rudin, C.M.; Schultz, N.; et al. Tumor Mutation Burden and Efficacy of EGFR-Tyrosine Kinase Inhibitors in Patients with EGFR-Mutant Lung Cancers. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 1063–1069. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, H.; Sanchez-Vega, F.; La, K.; Chatila, W.; Jonsson, P.; Halpenny, D.; Plodkowski, A.; Long, N.; Sauter, J.L.; Rekhtman, N.; et al. Molecular Determinants of Response to Anti-Programmed Cell Death (PD)-1 and Anti-Programmed Death-Ligand 1 (PD-L1) Blockade in Patients with Non-Small-Cell Lung Cancer Profiled with Targeted Next-Generation Sequencing. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 633–641. [Google Scholar] [CrossRef]
- Memmott, R.M.; Wolfe, A.R.; Carbone, D.P.; Williams, T.M. Predictors of Response, Progression-Free Survival and Overall Survival in Patients with Lung Cancer Treated with Immune Checkpoint Inhibitors. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2021, 16, 1086–1098. [Google Scholar] [CrossRef]
- Owada-Ozaki, Y.; Muto, S.; Takagi, H.; Inoue, T.; Watanabe, Y.; Fukuhara, M.; Yamaura, T.; Okabe, N.; Matsumura, Y.; Hasegawa, T.; et al. Prognostic Impact of Tumor Mutation Burden in Patients with Completely Resected Non-Small Cell Lung Cancer: Brief Report. J. Thorac. Oncol. Off. Publ. Int. Assoc. Study Lung Cancer 2018, 13, 1217–1221. [Google Scholar] [CrossRef] [Green Version]
- Yu, Y.; Zeng, D.; Ou, Q.; Liu, S.; Li, A.; Chen, Y.; Lin, D.; Gao, Q.; Zhou, H.; Liao, W.; et al. Association of Survival and Immune-Related Biomarkers with Immunotherapy in Patients with Non-Small Cell Lung Cancer: A Meta-analysis and Individual Patient-Level Analysis. JAMA Netw. Open 2019, 2, e196879. [Google Scholar] [CrossRef] [Green Version]
- Mazieres, J.; Drilon, A.; Lusque, A.; Mhanna, L.; Cortot, A.B.; Mezquita, L.; Thai, A.A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- He, B.X.; Dong, D.; She, Y.L.; Zhou, C.C.; Fang, M.J.; Zhu, Y.B.; Zhang, H.H.; Huang, Z.P.; Jiang, T.; Tian, J.; et al. Predicting response to immunotherapy in advanced non-small-cell lung cancer using tumor mutational burden radiomic biomarker. J. Immunother. Cancer 2020, 8, e000550. [Google Scholar] [CrossRef] [PubMed]
- Ricciuti, B.; Alessi, J.V.; Alden, S.; Lamberti, G.; Vaz, V.; Barrichello, A.; Sholl, L.; Awad, M. 312—Three-year outcomes with first-line pembrolizumab for metastatic non–small-cell lung cancer (NSCLC) with a very high PD-L1 tumor proportion score (TPS) ≥90%. J. Immunother. Cancer 2021, 9 (Suppl. 2), A336. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Variables | Overall, n = 138 | Progressive Disease (PD), n = 46 | Disease Control (DC), n = 92 | p-Value | |||
|---|---|---|---|---|---|---|---|
| Age [median, Q1–Q3] | |||||||
| 73 | 67–78 | 72 | 65–77 | 73 | 69–78 | 0.2129 | |
| Sex (n, col%) | |||||||
| Female | 73 | 52.90 | 21 | 45.65 | 52 | 56.52 | 0.2785 |
| Male | 65 | 47.10 | 25 | 54.35 | 40 | 43.48 | |
| Smoking status (n, col%) | |||||||
| Light and non-smoker | 7 | 5.07 | 5 | 10.87 | 2 | 2.17 | 0.0345 * |
| Smoker (current/ex) | 127 | 92.03 | 38 | 82.61 | 89 | 96.74 | |
| Unknown | 4 | 2.90 | 3 | 6.52 | 1 | 1.09 | |
| Pack years 1 [median, Q1–Q3] | |||||||
| 40 | 28–50 | 30 | 22–43 | 45 | 30–50 | 0.0226 * | |
| Smoking and pack years (n, col%) | |||||||
| Light and non-smoker | 7 | 5.07 | 5 | 10.87 | 2 | 2.17 | 0.0031 * |
| Smoker with pack years ≤40 | 65 | 47.10 | 26 | 56.52 | 39 | 42.39 | |
| Smokers with pack years >40 | 57 | 41.30 | 11 | 23.91 | 46 | 50.00 | |
| Unknown 2 | 9 | 6.52 | 4 | 8.70 | 5 | 5.43 | |
| Eastern Cooperative Oncology Group performance status (ECOG) (n, col%) | |||||||
| ≤1 | 81 | 58.70 | 20 | 43.48 | 61 | 66.30 | 0.0153 * |
| ≥2 | 53 | 38.41 | 24 | 52.17 | 29 | 31.52 | |
| Unknown | 4 | 2.90 | 2 | 4.35 | 2 | 2.17 | |
| Tumor histology (n, col%) | |||||||
| Non-SCC | 116 | 84.06 | 36 | 78.26 | 80 | 86.96 | 0.1923 |
| SCC | 19 | 13.77 | 9 | 19.57 | 10 | 10.87 | |
| Not Otherwise Specified | 3 | 2.17 | 1 | 2.17 | 2 | 2.17 | |
| On baseline CT: Number of patients with metastatic involvement in organs (n, col%) | |||||||
| Lung | 72 | 52.17 | 27 | 58.70 | 45 | 48.91 | 0.3662 |
| Lymph node | 114 | 82.61 | 42 | 91.30 | 72 | 78.26 | 0.0612 |
| Adrenal | 33 | 23.91 | 16 | 34.78 | 17 | 18.48 | 0.0554 |
| Liver | 16 | 11.59 | 10 | 21.74 | 6 | 6.52 | 0.0119 * |
| Bone | 48 | 34.78 | 26 | 56.52 | 22 | 23.91 | 0.0003 * |
| Brain 3 | 21 | 15.22 | 7 | 15.22 | 14 | 15.22 | 1.0000 |
| Pleura 4 | 43 | 31.16 | 18 | 39.13 | 25 | 27.17 | 0.1775 |
| On baseline CT: Target lung lesion size in mm5 [median, Q1–Q3] | |||||||
| 35.5 | 24–50 | 38 | 24.5–51.5 | 35 | 24–47 | 0.4821 | |
| On baseline CT: Number of involved organs with metastasis per patient [median, Q1–Q3] | |||||||
| 3 | 2–4 | 3 | 2–4 | 2 | 2–3 | 0.0015 * | |
| Univariate (Unadjusted) | Multivariate (Adjusted) 1 | |||||||
|---|---|---|---|---|---|---|---|---|
| Odds Ratio | [95% CI for OR] | p-Value | Odds Ratio | [95% CI for OR] | p-Value | |||
| Sex | ||||||||
| Female [ref] | 1.00 | 1.00 | ||||||
| Male | 1.74 | [0.82 | 3.73] | 0.1495 | 1.92 | [0.81 | 4.64] | 0.1415 |
| Smoking history (smoking status and pack years) | ||||||||
| 0 (light and non-smoker) [ref] | 1.00 | 1.00 | ||||||
| Current/ex-smoker, ≤40 pack years | 0.26 | [0.03 | 1.29] | 0.1199 | 0.12 | [0.01 | 0.82] | 0.0412 |
| Current/ex-smoker, >40 pack years | 0.10 | [0.01 | 0.51] | 0.0092 | 0.04 | [0.0040 | 0.30] | 0.0033 |
| Eastern Cooperative Oncology Group performance status (ECOG) | ||||||||
| ≤1 [ref] | 1.00 | 1.00 | ||||||
| ≥2 | 2.44 | [1.14 | 5.28] | 0.0216 | 1.95 | [0.81 | 4.76] | 0.1357 |
| Age (10 years) | ||||||||
| 0.70 | [0.39 | 1.20] | 0.2000 | 0.55 | [0.28 | 1.07] | 0.0853 | |
| No. of involved organs on baseline CT | ||||||||
| 1.67 | [1.27 | 2.27] | 0.0004 | 1.59 | [1.19 | 2.20] | 0.0027 | |
| Youden | Topleft | ||||
|---|---|---|---|---|---|
| cut-offs on ROC to defined “high-” vs. “low-risk” of progression group | 0.20 | 0.33 | |||
| Comparison between “true response” and “predicted risk of progression” | |||||
| True Response (PD vs. DC) | PD (n = 41) | DC (n = 87) | PD (n = 41) | DC (n = 87) | |
| Predicted risk of progression 1 | |||||
| High-risk of progression 2 | 38 | 40 | 29 | 23 | |
| Low-risk of progression 3 | 3 | 47 | 12 | 64 | |
| Sensitivity:0.93 | Specificity: 0.54 | Sensitivity: 0.71 | Specificity: 0.74 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silver, A.; Ho, C.; Ye, Q.; Zhang, J.; Janzen, I.; Li, J.; Martin, M.; Wu, L.; Wang, Y.; Lam, S.; et al. Prediction of Disease Progression to Upfront Pembrolizumab Monotherapy in Advanced Non-Small-Cell Lung Cancer with High PD-L1 Expression Using Baseline CT Disease Quantification and Smoking Pack Years. Curr. Oncol. 2023, 30, 5546-5559. https://doi.org/10.3390/curroncol30060419
Silver A, Ho C, Ye Q, Zhang J, Janzen I, Li J, Martin M, Wu L, Wang Y, Lam S, et al. Prediction of Disease Progression to Upfront Pembrolizumab Monotherapy in Advanced Non-Small-Cell Lung Cancer with High PD-L1 Expression Using Baseline CT Disease Quantification and Smoking Pack Years. Current Oncology. 2023; 30(6):5546-5559. https://doi.org/10.3390/curroncol30060419
Chicago/Turabian StyleSilver, Ali, Cheryl Ho, Qian Ye, Jianjun Zhang, Ian Janzen, Jessica Li, Montgomery Martin, Lang Wu, Ying Wang, Stephen Lam, and et al. 2023. "Prediction of Disease Progression to Upfront Pembrolizumab Monotherapy in Advanced Non-Small-Cell Lung Cancer with High PD-L1 Expression Using Baseline CT Disease Quantification and Smoking Pack Years" Current Oncology 30, no. 6: 5546-5559. https://doi.org/10.3390/curroncol30060419