Geographic Variations and the Associated Factors in Adherence to and Persistence with Adjuvant Hormonal Therapy for the Privately Insured women Aged 18–64 with Breast Cancer in Texas

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
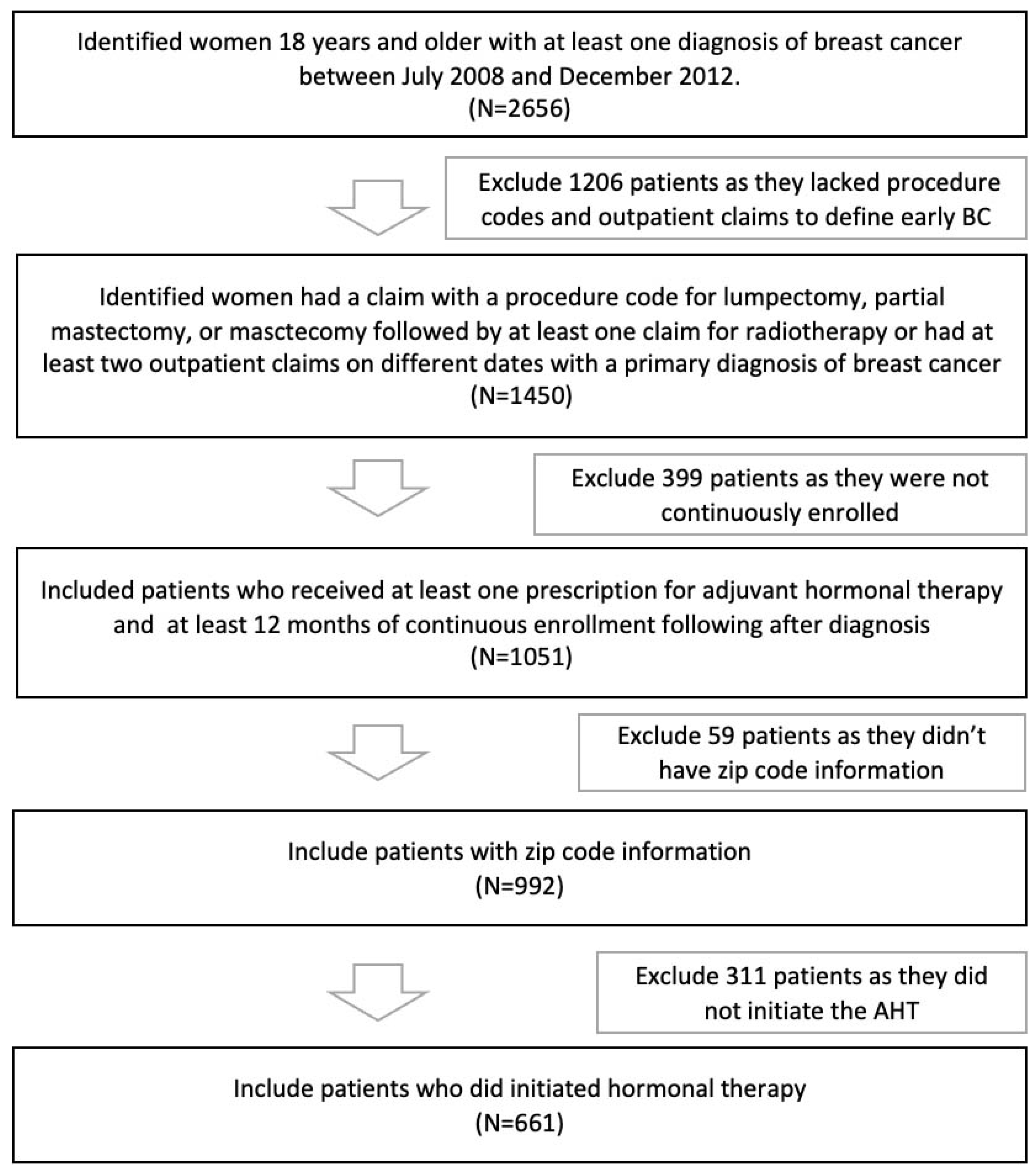
2.2. Study Cohort Description
2.3. Outcome
2.4. Patient-Level, Provider-Level, and Area-Level Characteristics
2.5. Statistical Analysis
3. Results
3.1. Predictors of Adherence
3.2. Predictors of Persistence
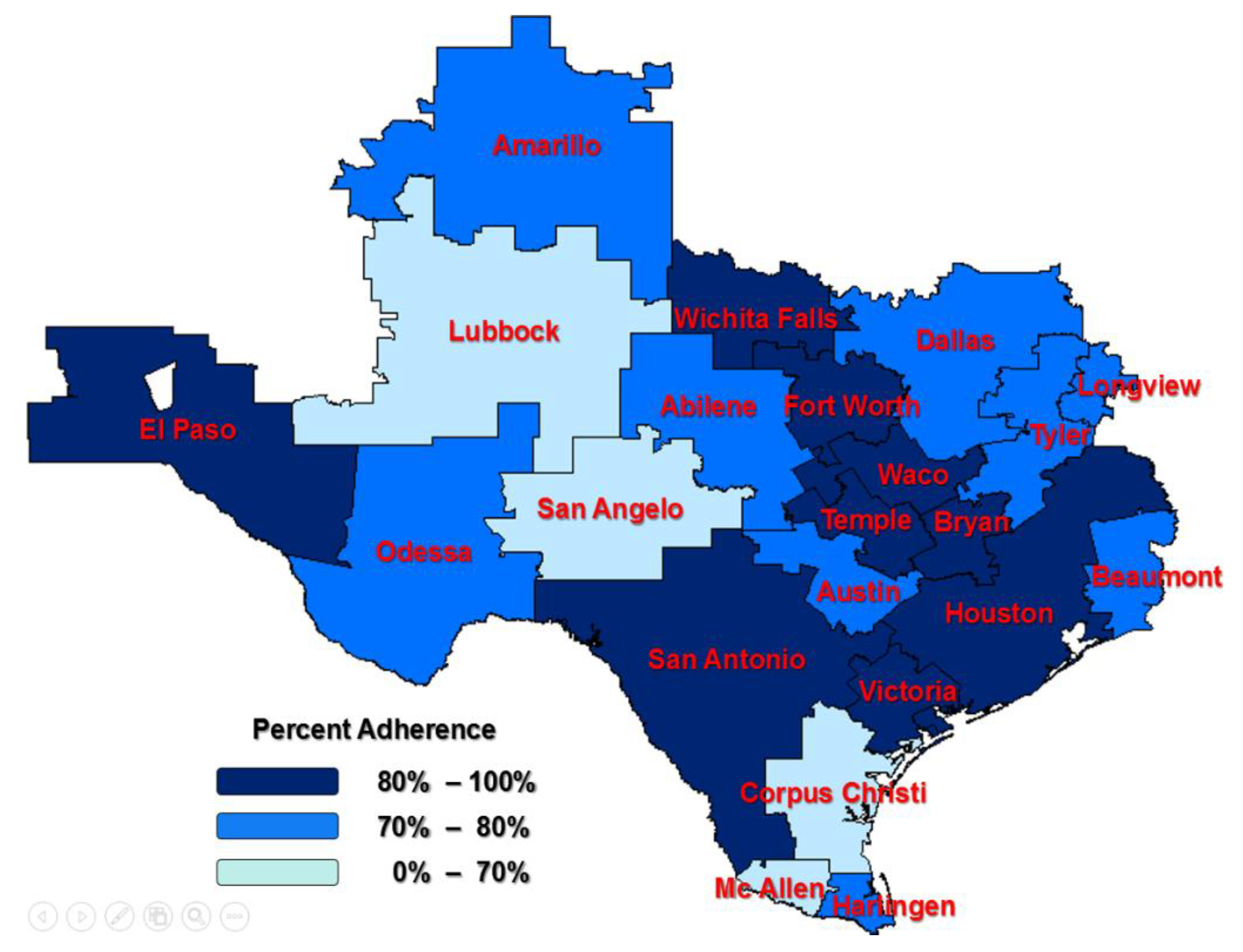
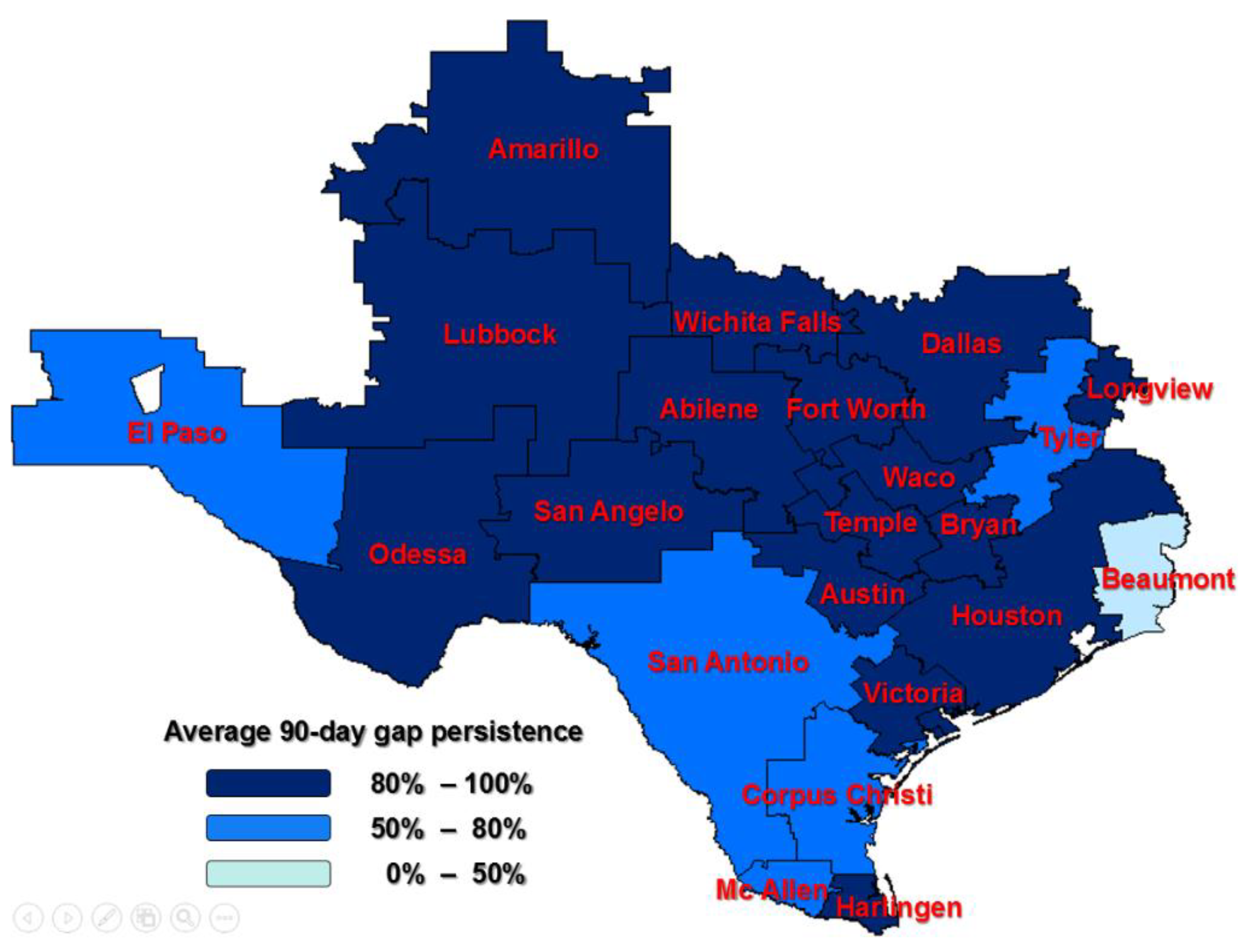
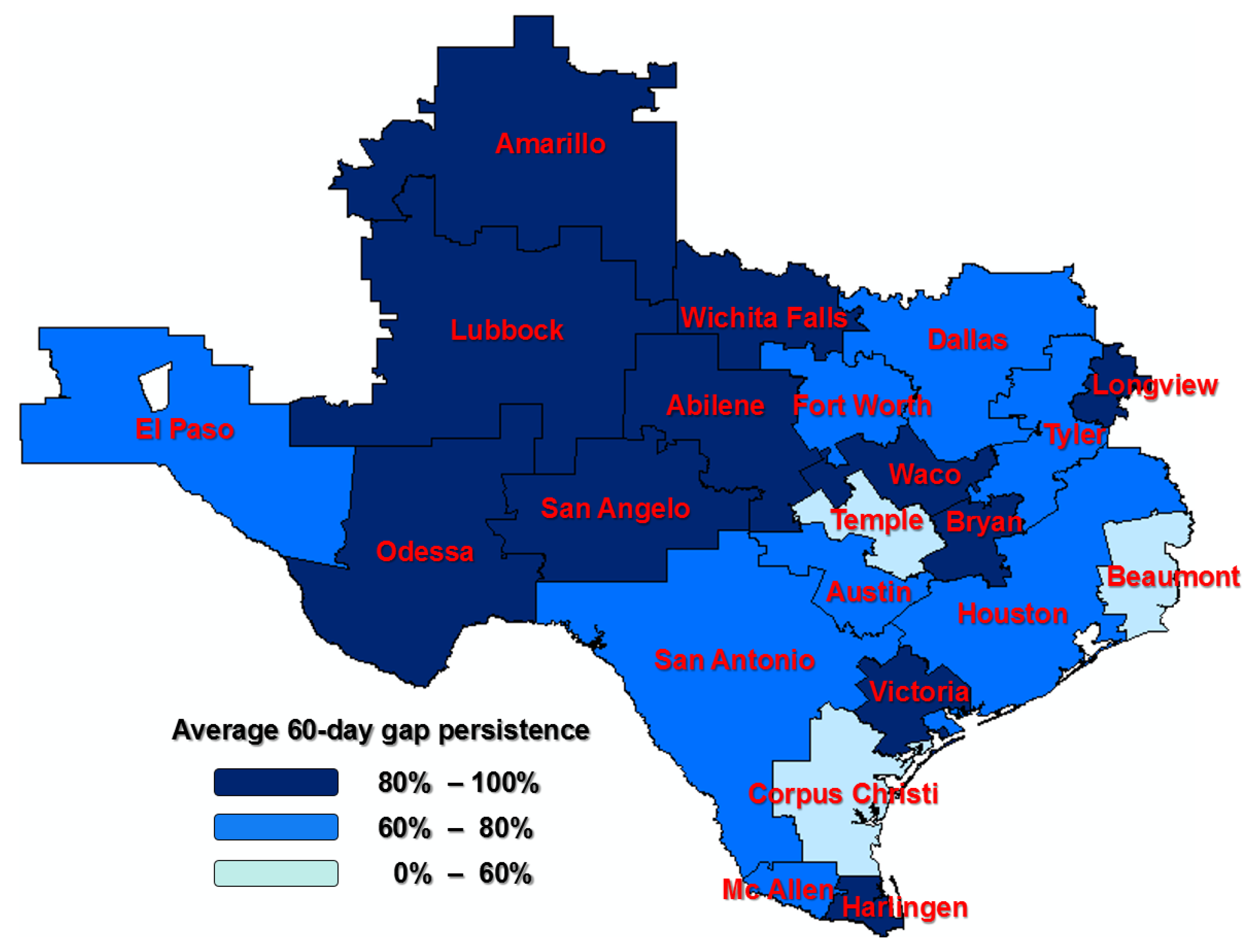
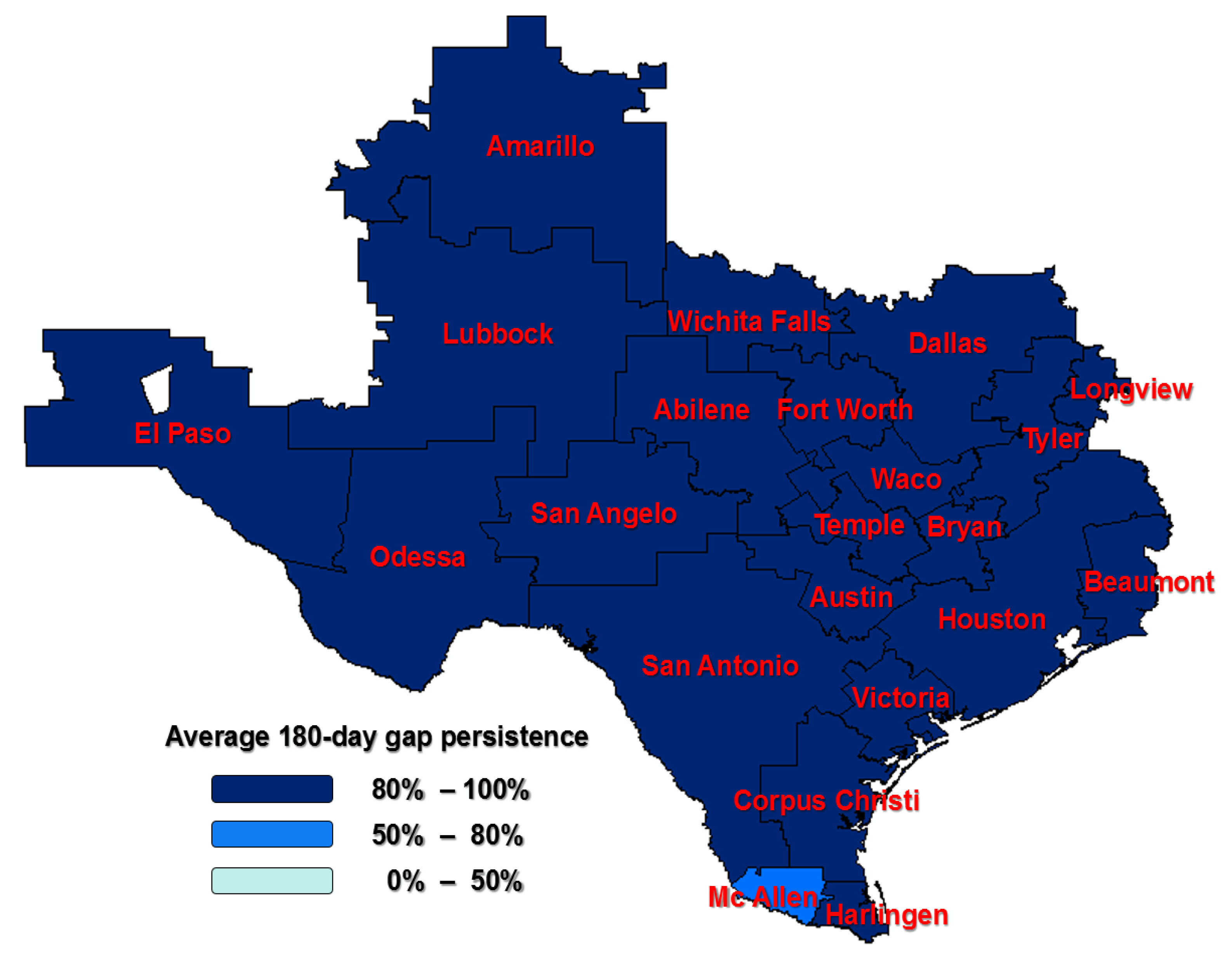
Regional Variation in Persistence
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | 60-Day Gap Persistence by HRR * | 180-Day Gap Persistence by HRR * | |
|---|---|---|---|
| Hospital Referral Region | |||
| Abilene | 9 | 0.89 | 0.89 |
| Amarillo | 15 | 0.80 | 0.80 |
| Austin | 57 | 0.75 | 0.95 |
| Beaumont | 9 | 0.56 | 0.89 |
| Bryan | 10 | 1 | 1 |
| Corpus Christi | 5 | 0.40 | 1 |
| Dallas | 169 | 0.72 | 0.89 |
| El Paso | 13 | 0.77 | 0.85 |
| Fort Worth | 55 | 0.70 | 0.89 |
| Harlingen | 8 | 0.88 | 1 |
| Houston | 165 | 0.70 | 0.91 |
| Longview | 15 | 0.87 | 1 |
| Lubbock | 18 | 0.83 | 0.94 |
| McAllen | 12 | 0.67 | 0.67 |
| Odessa | 21 | 0.81 | 1 |
| San Angelo | 2 | 1 | 1 |
| San Antonio | 51 | 0.65 | 0.86 |
| Temple | 1 | 0 | 1 |
| Tyler | 18 | 0.78 | 0.83 |
| Victoria | 1 | 1 | 1 |
| Waco | 5 | 0.80 | 1 |
| Wichita Falls | 2 | 1 | 1 |
| N | 60-Day Gap Persistence | 180-Day Gap Persistence | |||
|---|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | ||
| Abilene | 9 | 1.00 | 2.07 | 0.32 | 0.20 |
| Amarillo | 15 | 0.35 | 0.34 | 0.09 a (0.006) b | 0.03 (0.0003) |
| Austin | 57 | 0.93 | 1.56 | 2.73 | 1.08 |
| Beaumont | 9 | 0.25 | 0.33 | 0.36 | 0.21 |
| Bryan | 10 | 0.01 | - | - | - |
| Corpus Christi | 5 | 0.22 | 0.79 | - | - |
| Dallas | 169 | 1.18 | 1.51 | 0.83 | 0.21 |
| El Paso | 13 | 0.96 | 3.99 | 0.55 | 0.73 |
| Fort Worth | 55 | 1.42 | 0.75 | 1.11 | 0.18 |
| Harlingen | 8 | 0.78 | 7.46 | - | - |
| Houston | 165 | 2.27 | 0.90 | 1.28 | 0.27 |
| Longview | 15 | 2.04 | 2.19 | - | - |
| Lubbock | 18 | 1.60 | 4.44 | 1 | |
| McAllen | 12 | 0.70 | 4.70 | 0.2 | 0.47 |
| Odessa | 21 | 1.17 | 3.98 | - | - |
| San Angelo | 2 | 0.01 | - | - | - |
| San Antonio | 51 | 0.44 | 1.63 | 0.56 | 0.60 |
| Temple | 1 | - | - | - | - |
| Tyler | 18 | 1 | - | 0.46 | 0.12 |
| Victoria | 1 | 0.01 | - | - | - |
| Waco | 5 | 2.62 | 0.42 | - | - |
| Wichita Falls | 2 | 0.01 | - | - | - |
| Characteristic | Duration of Gap in Therapy | |
|---|---|---|
| 60 Days | 180 Days | |
| Patient-level characteristics | ||
| Cancer Treatment (referent: no mastectomy no BCS no chemo no rad) | ||
| Mastectomy | 0.91 (0.72, 1.16) | 0.89 (0.72, 1.10) |
| BCS | 1.04 (0.84, 1.3) | 1.003 (0.82, 1.22) |
| Chemotherapy | 1.3 (1.04, 1.62) | 1.19 (0.82, 1.22) |
| Year of diagnosis (referent: 2008) | ||
| 2009 | 1.39 (1.02, 1.89) | 1.37 (1.04, 1.80) |
| 2010 | 2.36 (1.71, 3.25) * | 2.46 (1.86, 3.27) * |
| 2011 | 3.95 (2.85, 5.49) * | 3.80 (2.82, 5.11) * |
| 2012 | 6.49 (4.5, 9.36) * | 6.67 (4.75, 9.35) * |
| 2009 | 1.39 (1.02, 1.89) | 1.37 (1.04, 1.80) |
| Therapy initiation (referent: did not initiate ATH within 1 year of BC diagnosis) | ||
| Initiated | 0.49 (0.31, 0.78) * | 0.29 (0.19, 0.44) * |
| Age at diagnosis, (referent: <40 years) | ||
| 40–44 | 0.58 (0.34, 0.99) | 0.69 (0.43, 1.11) |
| 45–49 | 0.69 (0.43, 1.1) | 0.75 (0.49, 1.14) |
| 50–54 | 0.74 (0.47, 1.18) | 0.69 (0.45, 1.03) |
| 55–59 | 0.77 (0.48. 1.23) | 0.77 (0.51. 1.17) |
| 60–64 | 0.8 (0.48, 1.34) | 0.76 (0.48, 1.22) |
| Neighborhood, % non-white (referent: <10%) | ||
| 10–24% | 1.38 (0.99, 1.89) | 1.37 (1.03, 1.82) |
| 25–50% | 1.31 (0.89, 1.93) | 1.30 (0.91, 1.84) |
| ≥50% | 1.71 (1.03, 2.84) | 1.35 (0.86, 2.13) |
| 10–24% | 1.38 (0.99, 1.89) | 1.37 (1.03, 1.82) |
| Percent of Hispanic and Latino populations | 0.94 (0.76, 1.16) | 1.01 (0.84, 1.22) |
| Neighborhood, % education lower than high school (referent: <25%) | ||
| ≥25% | 0.86 (0.64, 1.16) | 0.88 (0.67, 1.16) |
| Neighborhood, % below poverty level (referent: <20%) | ||
| ≥20% | 1.21 (0.90, 1.62) | 1.12 (0.86, 1.48) |
| Comorbidity | 0.95 (0.90, 1.0) | 0.96 (0.92, 1.006) |
| Outpatient visits | 0.99 (0.91, 1.09) | 1.01 (0.94, 1.09) |
| Inpatient visits | 0.98 (0.91, 1.07) | 0.93 (0.93, 1.07) |
| Distance to health service facilities (referent: less than 5 mile) | ||
| 5–10 mile | 0.67 (0.49, 0.91) | 0.71 (0.54, 0.94) |
| 10–35 mile | 0.80 (0.62, 1.04) | 0.92 (0.72, 1.16) |
| 35–100 mile | 0.78 (0.56, 1.09) | 0.89 (0.66, 1.19) |
| >100 mile | 0.82 (0.57, 1.19) | 0.93 (0.66, 1.30) |
| Provider-level characteristics | ||
| Total number of hospitals, 2012 | 1.02 (0.98, 1.06) | 1.02 (0.98, 1.06) |
| Hospital admissions, 2012 | 1.0 (.99, 1.001) | 1.0 (0.99, 1.001) |
| Hospital beds, 2012 | 1.0 (1.00, 1.001) | 1.0 (1.00, 1.001) |
| Area-level characteristics | ||
| Total Subspecialty, 2013 | 0.99 (0.996, 1.002) | 0.99 (0.998, 1.001) |
| Number of oncology providers in area | 0.99 (0.997, 1.001) | 0.99 (0.998, 1.003) |


References
- Female Breast Cancer in Texas. Texas Cancer Registry, Cancer Epidemiology and Surveillance Branch, Texas Department of State Health Services, October, 2022. Available online: dshs.texas.gov/tcr (accessed on 2 November 2022).
- Texas Cancer Registry. SEER*Stat Database, Mortality—Texas, 1990–2016, Statewide, Texas Department of State Health Services. Available online: www.dshs.texas.gov/tcr (accessed on 2 November 2022).
- Yung, R.L.; Hassett, M.J.; Chen, K.; Gesten, F.C.; Roohan, P.J.; Boscoe, F.P.; Sinclair, A.H.; Schymura, M.J.; Schrag, D. Initiation of Adjuvant Hormone Therapy by Medicaid Insured Women with Nonmetastatic Breast Cancer. J. Natl. Cancer Inst. 2012, 104, 1102–1105. [Google Scholar] [CrossRef] [Green Version]
- Owusu, C.; Buist, D.S.M.; Field, T.S.; Lash, T.L.; Thwin, S.S.; Geiger, A.M.; Quinn, V.P.; Frost, F.J.; Prout, M.; Yood, M.U.; et al. Predictors of Tamoxifen Discontinuation Among Older Women With Estrogen Receptor–Positive Breast Cancer. J. Clin. Oncol. 2008, 26, 549–555. [Google Scholar] [CrossRef]
- Hershman, D.L.; Kushi, L.; Shao, T.; Buono, D.; Kershenbaum, A.; Tsai, W.-Y.; Fehrenbacher, L.; Gomez, S.L.; Miles, S.; Neugut, A.I. Early Discontinuation and Nonadherence to Adjuvant Hormonal Therapy in a Cohort of 8,769 Early-Stage Breast Cancer Patients. J. Clin. Oncol. 2010, 28, 4120–4128. [Google Scholar] [CrossRef] [PubMed]
- Lambert-Côté, L.; Bouhnik, A.-D.; Bendiane, M.-K.; Bérenger, C.; Mondor, M.; Huiart, L.; Lauzier, S. Adherence trajectories of adjuvant endocrine therapy in the five years after its initiation among women with non-metastatic breast cancer: A cohort study using administrative databases. Breast Cancer Res. Treat. 2020, 180, 777–790. [Google Scholar] [CrossRef]
- Vrijens, F.; Stordeur, S.; Beirens, K.; Devriese, S.; Van Eycken, E.; Vlayen, J. Effect of hospital volume on processes of care and 5-year survival after breast cancer: A population-based study on 25 000 women. Breast 2012, 21, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.T.; Yang, T.; Matthews, S.A.; Kern, T.; Mackley, H.B.; Kimmick, G.; Louis, C.; Lengerich, E.; Yao, N. Breast cancer screening, area deprivation, and later stage breast cancer in Appalachia: Does geography matter? Health Serv. Res. 2014, 49, 546–567. [Google Scholar] [CrossRef]
- Birkmeyer, J.D.; Reames, B.N.; McCulloch, P.; Carr, A.J.; Campbell, W.B.; Wennberg, J.E. Understanding of regional variation in the use of surgery. Lancet 2013, 382, 1121–1129. [Google Scholar] [CrossRef] [Green Version]
- Fairfield, K.M.; Lucas, F.L.; Earle, C.C.; Small, L.; Trimble, E.L.; Warren, J.L. Regional variation in cancer-directed surgery and mortality among women with epithelial ovarian cancer in the medicare population. Cancer 2010, 116, 4840–4848. [Google Scholar] [CrossRef]
- Feinstein, A.J.; Soulos, P.R.; Long, J.B.; Herrin, J.; Roberts, K.B.; Yu, J.B.; Gross, C.P. Variation in receipt of radiation therapy after breast-conserving surgery: Assessing the impact of physicians and geographic regions. Med. Care 2013, 51, 330–338. [Google Scholar] [CrossRef] [Green Version]
- Nattinger, A.B.; Gottlieb, M.S.; Veum, J.; Yahnke, D.; Goodwin, J.S. Geographic Variation in the Use of Breast-Conserving Treatment for Breast Cancer. N. Engl. J. Med. 1992, 326, 1102–1107. [Google Scholar] [CrossRef]
- Sariego, J. Regional variation in breast cancer treatment throughout the United States. Am. J. Surg. 2008, 196, 572–574. [Google Scholar] [CrossRef] [PubMed]
- Osteen, R.T.; Steele, G.D.; Menck, H.R.; Winchester, D.P. Regional differences in surgical management of breast cancer. CA A Cancer J. Clin. 1992, 42, 39–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Partridge, A.H.; Wang, P.S.; Winer, E.P.; Avorn, J. Nonadherence to Adjuvant Tamoxifen Therapy in Women With Primary Breast Cancer. J. Clin. Oncol. 2003, 21, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Nekhlyudov, L.; Li, L.; Ross-Degnan, D.; Wagner, A.K. Five-year patterns of adjuvant hormonal therapy use, persistence, and adherence among insured women with early-stage breast cancer. Breast Cancer Res. Treat. 2011, 130, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Sedjo, R.L.; Devine, S. Predictors of non-adherence to aromatase inhibitors among commercially insured women with breast cancer. Breast Cancer Res. Treat. 2010, 125, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Kimmick, G.; Anderson, R.; Camacho, F.; Bhosle, M.; Hwang, W.; Balkrishnan, R. Adjuvant Hormonal Therapy Use Among Insured, Low-Income Women With Breast Cancer. J. Clin. Oncol. 2009, 27, 3445–3451. [Google Scholar] [CrossRef] [Green Version]
- Balkrishnan, R.; Rajagopalan, R.; Camacho, F.T.; Huston, S.A.; Murray, F.T.; Anderson, R.T. Predictors of medication adherence and associated health care costs in an older population with type 2 diabetes mellitus: A longitudinal cohort study. Clin. Ther. 2003, 25, 2958–2971. [Google Scholar] [CrossRef]
- Blanchette, P.S.; Lam, M.; Richard, L.; Allen, B.; Shariff, S.Z.; Vandenberg, T.; Pritchard, K.I.; Chan, K.K.W.; Louie, A.V.; Desautels, D.; et al. Factors associated with endocrine therapy adherence among post-menopausal women treated for early-stage breast cancer in Ontario, Canada. Breast Cancer Res. Treat. 2019, 179, 217–227. [Google Scholar] [CrossRef]
- United States Census QuickFacts. Available online: https://www.census.gov/quickfacts/TX (accessed on 8 November 2022).
- Hutchins, D.S.; Zeber, J.E.; Roberts, C.S.; Williams, A.F.; Manias, E.; Peterson, A.M.; IPSOR Medication Adherence and Persistence Special Interest Group. Initial Medication Adherence—Review and Recommendations for Good Practices in Outcomes Research: An ISPOR Medication Adherence and Persistence Special Interest Group Report. Value Health 2015, 18, 690–699. [Google Scholar] [CrossRef] [Green Version]
- Cramer, J.A.; Roy, A.; Burrell, A.; Fairchild, C.J.; Fuldeore, M.J.; Ollendorf, D.A.; Wong, P.K. Medication Compliance and Persistence: Terminology and Definitions. Value Health 2008, 11, 44–47. [Google Scholar] [CrossRef] [Green Version]
- Neugut, A.I.; Hillyer, G.C.; Kushi, L.H.; Lamerato, L.; Leoce, N.; Nathanson, S.D.; Ambrosone, C.B.; Bovbjerg, D.H.; Mandelblatt, J.S.; Magai, C.; et al. Non-initiation of adjuvant hormonal therapy in women with hormone receptor-positive breast cancer: The Breast Cancer Quality of Care Study (BQUAL). Breast Cancer Res. Treat. 2012, 134, 419–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lash, T.L.; Fox, M.P.; Westrup, J.L.; Fink, A.K.; Silliman, R.A. Adherence to tamoxifen over the five-year course. Breast Cancer Res. Treat. 2006, 99, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Cluze, C.; Rey, D.; Huiart, L.; BenDiane, M.; Bouhnik, A.; Berenger, C.; Carrieri, M.; Giorgi, R. Adjuvant endocrine therapy with tamoxifen in young women with breast cancer: Determinants of interruptions vary over time. Ann. Oncol. 2012, 23, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Deyo, R.A.; Cherkin, D.C.; Ciol, M.A. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- D’Hoore, W.; Bouckaert, A.; Tilquin, C. Practical considerations on the use of the charlson comorbidity index with administrative data bases. J. Clin. Epidemiol. 1996, 49, 1429–1433. [Google Scholar] [CrossRef]
- The Darthmouth Atlas of Health Care. Research Methods. Available online: http://www.dartmouthatlas.org/tools/faq/researchmethods.aspx (accessed on 8 November 2022).
- Cahir, C.; Barron, T.I.; Sharp, L.; Bennett, K. Can demographic, clinical and treatment-related factors available at hormonal therapy initiation predict non-persistence in women with stage I–III breast cancer? Cancer Causes Control 2017, 28, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Emerson, M.A.; Achacoso, N.S.; Benefield, H.C.; Troester, M.A.; Habel, L.A. Initiation and adherence to adjuvant endocrine therapy among urban, insured American Indian/Alaska Native breast cancer survivors. Cancer 2021, 127, 1847–1856. [Google Scholar] [CrossRef]
- Gao, P.; You, L.; Wu, D.; Shi, A.; Miao, Q.; Rana, U.; Martin, D.P.; Du, Y.; Zhao, G.; Han, B.; et al. Adherence to endocrine therapy among Chinese patients with breast cancer: Current status and recommendations for improvement. Patient Prefer. Adherence 2018, 12, 887–897. [Google Scholar] [CrossRef] [Green Version]
- Ma, S.; Shepard, D.S.; Ritter, G.A.; Martell, R.E.; Thomas, C.P. The impact of the introduction of generic aromatase inhibitors on adherence to hormonal therapy over the full course of 5-year treatment for breast cancer. Cancer 2020, 126, 3417–3425. [Google Scholar] [CrossRef]
- Kong, A.L.; Yen, T.W.F.; Pezzin, L.E.; Miao, H.; Ms, R.A.S.; Laud, P.W.; Nattinger, A.B. Socioeconomic and Racial Differences in Treatment for Breast Cancer at a Low-Volume Hospital. Ann. Surg. Oncol. 2011, 18, 3220–3227. [Google Scholar] [CrossRef] [Green Version]
- Schootman, M.; Jeffe, D.B.; Lian, M.; Gillanders, W.E.; Aft, R. The Role of Poverty Rate and Racial Distribution in the Geographic Clustering of Breast Cancer Survival Among Older Women: A Geographic and Multilevel Analysis. Am. J. Epidemiol. 2008, 169, 554–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.; Rajan, S.S.; Du, X.L.; Franzini, L.; Giordano, S.H.; Morgan, R.O. Association between financial burden and adjuvant hormonal therapy adherence and persistent use for privately insured women aged 18–64 years in BCBS of Texas. Breast Cancer Res. Treat. 2018, 169, 573–586. [Google Scholar] [CrossRef] [PubMed]
- Cavazza, M.; Banks, H.; Ercolanoni, M.; Cukaj, G.; Bianchi, G.; Capri, G.; Longo, F. Factors influencing adherence to adjuvant endocrine therapy in breast cancer-treated women: Using real-world data to inform a switch from acute to chronic disease management. Breast Cancer Res. Treat. 2020, 183, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Bosco-Lévy, P.; Jové, J.; Robinson, P.; Moore, N.; Fourrier-Réglat, A.; Bezin, J. Persistence to 5-year hormonal breast cancer therapy: A French national population-based study. Br. J. Cancer 2016, 115, 912–919. [Google Scholar] [CrossRef] [Green Version]
- Burstein, H.J.; Prestrud, A.A.; Seidenfeld, J.; Anderson, H.; Buchholz, T.A.; Davidson, N.E.; Gelmon, K.E.; Giordano, S.H.; Hudis, C.A.; Malin, J.; et al. American Society of Clinical Oncology Clinical Practice Guideline: Update on Adjuvant Endocrine Therapy for Women With Hormone Receptor–Positive Breast Cancer. J. Clin. Oncol. 2010, 28, 3784–3796. [Google Scholar] [CrossRef] [Green Version]
- Elbeddini, A.; To, A.; Tayefehchamani, Y.; Wen, C.X. Importance of medication reconciliation in cancer patients. J. Pharm. Policy Pract. 2021, 14, 98. [Google Scholar] [CrossRef]
- Trogdon, J.G.; Amin, K.; Gupta, P.; Urick, B.Y.; Reeder-Hayes, K.E.; Farley, J.F.; Wheeler, S.B.; Spees, L.; Lund, J.L. Providers’ mediating role for medication adherence among cancer survivors. PLoS ONE 2021, 16, e0260358. [Google Scholar] [CrossRef]
- Nattinger, A.B.; Laud, P.W.; Bajorunaite, R.; Sparapani, R.A.; Freeman, J.L. An Algorithm for the Use of Medicare Claims Data to Identify Women with Incident Breast Cancer. Health Serv. Res. 2004, 39, 1733–1749. [Google Scholar] [CrossRef] [Green Version]
- Choo, P.W.; Rand, C.S.; Inui, T.S.; Lee, M.-L.T.; Cain, E.; Cordeiro-Breault, M.; Canning, C.; Platt, R. Validation of Patient Reports, Automated Pharmacy Records, and Pill Counts With Electronic Monitoring of Adherence to Antihypertensive Therapy. Med. Care 1999, 37, 846–857. [Google Scholar] [CrossRef]
- Steiner, J.F.; Koepsell, T.D.; Fihn, S.D.; Inui, T.S. A General Method of Compliance Assessment Using Centralized Pharmacy Records. Description and validation. Med. Care 1988, 26, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Lima-Dellamora, E.D.C.; de Castro, C.G.S.O.; Madruga, L.G.D.S.L.; Azeredo, T.B. Use of pharmacy records to measure treatment adherence: A critical review of the literature. Cad. Saude Publica 2017, 33, e00136216, (In Portuguese, English). [Google Scholar] [CrossRef] [PubMed] [Green Version]



| Characteristic | N (%) |
|---|---|
| Adjuvant hormonal therapy | |
| Initiated therapy | 661 (66.2) |
| Tamoxifen only | 353 (53.4) |
| Aromatase inhibitor only | 308 (44.6) |
| Did not initiate therapy | 311 (33.8) |
| Cancer Treatment | |
| Breast conserving surgery | 573 (57.8) |
| Mastectomy | 329 (33.2) |
| Chemotherapy | 593 (59.8) |
| Radiation therapy | 964 (97.2) |
| Year of diagnosis | |
| 2008 | 238 (24.0) |
| 2009 | 234 (23.6) |
| 2010 | 210 (21.2) |
| 2011 | 179 (18.0) |
| 2012 | 131 (13.2) |
| Age at diagnosis | |
| <40 | 48 (4.8) |
| 40–44 | 87 (8.8) |
| 45–49 | 186 (18.8) |
| 50–54 | 247 (24.9) |
| 55–59 | 331 (33.3) |
| 60–64 | 93 (9.4) |
| Neighborhood, % non-white population | |
| <10% | 118 (11.9) |
| 10–24% | 481 (48.5) |
| 25–50% | 289 (29.1) |
| ≥50% | 104 (10.5) |
| Percent of the population aged 25 and older, without a high school education | |
| <25% | 775 (78.1) |
| ≥25% | 217 (21.9) |
| Neighborhood, % below poverty level | |
| <20% | 748 (75.4) |
| ≥20% | 244 (24.6) |
| Distance to health service facilities | |
| less than 5 mile | 287 (28.9) |
| 5–10 mile | 173 (17.4) |
| 10–35 mile | 312 (31.5) |
| 35–100 mile | 131 (13.2) |
| >100 mile | 89 (9.0) |
| Comorbidity at diagnosis, mean (SD) | 1.27 (2.0) |
| Health care utilization at diagnosis | |
| Outpatient visits in prior 6 months, mean (SD) | 1.74 (2.7) |
| Inpatient days in prior 6 months, mean (SD) | 1.47 (1.4) |
| N | Adherence by HRR * | 90-Day Gap Persistence by HRR ** | |||
|---|---|---|---|---|---|
| Austin | 57 | 0.77 | 0.86 | ||
| Bryan | 10 | 0.94 | 1 | Maximum region | |
| El Paso | 13 | 0.82 | 0.78 | ||
| Houston | 165 | 0.81 | 0.80 | ||
| Beaumont | 9 | 0.73 | 0.50 | Minimum region | |
| Dallas | 169 | 0.79 | Median region | 0.81 | Median region |
| Fort Worth | 55 | 0.83 | 0.80 | ||
| Harlingen | 8 | 0.71 | 0.88 | ||
| McAllen | 12 | 0.66 | 0.67 | ||
| Odessa | 21 | 0.71 | 0.90 | ||
| San Antonio | 51 | 0.84 | 0.73 | ||
| Temple | 1 | 0.8 | 1 | Maximum region | |
| Victoria | 1 | 1 | Maximum region | 1 | Maximum region |
| San Angelo | 2 | 0.54 | Minimum region | 1 | Maximum region |
| Waco | 5 | 0.96 | 0.80 | ||
| Wichita Falls | 2 | 0.93 | 1 | Maximum region | |
| Abilene | 9 | 0.7 | 0.89 | ||
| Corpus Christi | 5 | 0.61 | 0.6 | ||
| Amarillo | 15 | 0.78 | 0.80 | ||
| Longview | 15 | 0.77 | 0.87 | ||
| Lubbock | 18 | 0.68 | 0.89 | ||
| Tyler | 18 | 0.76 | 0.78 | ||
| Adherence | Persistence of 90-Day Gap in Therapy | |
|---|---|---|
| OR (CI) | HR (CI) | |
| Patient-level characteristics | ||
| Cancer treatment Surgery (referent: no cancer-directed surgery) | ||
| Breast-conserving surgery | 2.04 (1.18, 3.54) | 1.69 (0.94, 3.04) |
| Mastectomy | 1.30 (0.73, 2.33) | 1.42 (0.76, 2.67) |
| Chemotherapy (referent: no chemotherapy) | ||
| Yes | 1.61 (1.04, 2.48) | 1.17 (0.95, 1.45) |
| Radiation therapy (referent: no radiation therapy) | ||
| Yes | 1.10 (0.20, 6.17) | 0.39 (0.15, 0.97) |
| Year of diagnosis (referent: 2008) | ||
| 2009 | 1.53 (0.87, 2.71) | 0.48 (0.27, 0.85) |
| 2010 | 1.18 (0.66, 2.09) | 1.11 (0.60, 2.05) |
| 2011 | 1.54 (0.86, 2.75) | 1.29 (0.67, 2.48) |
| 2012 | 1.54 (0.80, 2.98) | 2.54 (1.13, 5.74) |
| Therapy initiation (referent: did not initiated ATH within 1 year of BC diagnosis) | ||
| Not-Initiated | 0.02 (0.009, 0.04) * | 0.87 (0.53, 0.98) |
| Age at diagnosis, (referent: <40 years) | ||
| 40–44 | 2.28 (0.81, 6.37) | 1.25 (0.46, 3.46) |
| 45–49 | 1.54 (0.60, 3.98) | 1.43 (0.56, 3.67) |
| 50–54 | 2.07 (0.82, 5.23) | 2.57 (0.99, 6.60) |
| 55–59 | 2.49 (0.99, 6.30) | 1.98 (0.78. 5.01) |
| 60–64 | 1.12 (0.39, 3.21) | 3.44 (1.13, 10.52) |
| Neighborhood, % non-white (referent: <10%) | ||
| 10–24% | 0.56 (0.30, 1.02) | 0.79 (0.39, 1.62) |
| 25–50% | 2.47 (1.27, 4.81) | 1.41 (0.64, 3.11) |
| ≥50% | 1.16 (0.57, 2.38) | 1.87 (0.80, 4.35) |
| Percent of Hispanic and Latino population | 0.57 (0.39, 0.84) | 1.03 (0.84, 1.25) |
| Neighborhood, % education lower than high school (referent: first quartile) | ||
| Second quartile | 1.64 (0.79, 3.39) | 0.54 (0.22, 1.34) |
| Third quartile | 1.55 (0.67, 3.67) | 0.23 (0.08, 0.72) |
| Fourth quartile | 1.48 (0.57, 3.86) | 0.21 (0.06, 0.72) |
| Neighborhood, % below poverty level (referent: first quartile) | ||
| Second quartile | 0.34 (0.16, 0.70) | 2.12 (0.85, 5.30) |
| Third quartile | 0.32 (0.13, 0.78) | 3.06 (1.02, 9.14) |
| Fourth quartile | 0.55 (0.21, 1.43) | 3.27 (0.91, 11.75) |
| Comorbidity | 0.92 (0.83, 1.02) | 0.98 (0.88, 1.09) |
| Outpatient visits | 1.13 (1.00, 1.26) | 0.84 (0.72, 0.98) |
| Inpatient visits | 0.85 (0.72, 0.997) | 0.88 (0.75, 1.03) |
| Distance to health service facilities (referent: less than 5 miles) | ||
| 5–10 mile | 0.92 (0.83, 1.02) | 0.98 (0.88, 1.09) |
| 10–35 mile | 1.13 (1.00, 1.26) | 0.84 (0.72, 0.98) |
| 35–100 mile | 0.85 (0.72, 0.997) | 0.88 (0.75, 1.03) |
| >100 mile | 0.92 (0.83, 1.02) | 0.98 (0.88, 1.09) |
| Provider-level characteristics | ||
| Total number of hospitals, 2012 | 1.02 (0.98, 1.06) | 0.93 (0.82, 1.05) |
| Hospital admissions, 2012 | 1.00 (0.99, 1.001) | 1.00 (.99, 1.001) |
| Hospital beds, 2012 | 1.00 (1.00, 1.001) | 0.998 (0.995, 1.001) |
| Area-level characteristics | ||
| Total Subspecialty, 2013 | 0.99 (0.996, 1.002) | 0.99 (0.998, 1.001) |
| Number of oncology providers in the area | 0.99 (0.984, 0.991) * | 0.99 (0.992, 0.999) |
| N | 90-Day Gap Persistence | ||
|---|---|---|---|
| Unadjusted | Adjusted | ||
| Abilene | 9 | 0.96 | 0.91 |
| Amarillo | 15 | 0.22 a (0.003) b | 0.14 (0.02) |
| Austin | 57 | 1.70 | 0.99 |
| Beaumont | 9 | 0.33 | 0.57 |
| Bryan | 10 | - | - |
| Corpus Christi | 5 | 0.33 | 0.55 |
| Dallas | 169 | Ref | Ref |
| El Paso | 13 | 0.80 | 0.87 |
| Fort Worth | 55 | 0.98 | 0.48 |
| Harlingen | 8 | 1.21 | 3.03 (0.005) |
| Houston | 165 | 0.50 (0.003) | 1.05 |
| Longview | 15 | 1.74 | 1.43 |
| Lubbock | 18 | 1.52 | 2.04 |
| McAllen | 12 | 0.48 | 1.15 |
| Odessa | 21 | 2.82 | 10.29 (0.02) |
| San Angelo | 2 | - | - |
| San Antonio | 51 | 0.56 | 1.02 |
| Temple | 1 | - | - |
| Tyler | 18 | 0.76 | 0.33 |
| Victoria | 1 | - | - |
| Waco | 5 | 0.29 | 0.46 |
| Wichita Falls | 2 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.; Kim, M.S.; Rajan, S.S.; Du, X.L.; Franzini, L.; Kim, T.G.; Giordano, S.H.; Morgan, R.O. Geographic Variations and the Associated Factors in Adherence to and Persistence with Adjuvant Hormonal Therapy for the Privately Insured women Aged 18–64 with Breast Cancer in Texas. Curr. Oncol. 2023, 30, 3800-3816. https://doi.org/10.3390/curroncol30040288
Kim J, Kim MS, Rajan SS, Du XL, Franzini L, Kim TG, Giordano SH, Morgan RO. Geographic Variations and the Associated Factors in Adherence to and Persistence with Adjuvant Hormonal Therapy for the Privately Insured women Aged 18–64 with Breast Cancer in Texas. Current Oncology. 2023; 30(4):3800-3816. https://doi.org/10.3390/curroncol30040288
Chicago/Turabian StyleKim, Junghyun, Man S. Kim, Suja S. Rajan, Xianglin L. Du, Luisa Franzini, Tae Gi Kim, Sharon H. Giordano, and Robert O. Morgan. 2023. "Geographic Variations and the Associated Factors in Adherence to and Persistence with Adjuvant Hormonal Therapy for the Privately Insured women Aged 18–64 with Breast Cancer in Texas" Current Oncology 30, no. 4: 3800-3816. https://doi.org/10.3390/curroncol30040288