Real-Time Urethral and Ureteral Assessment during Radical Cystectomy Using Ex-Vivo Optical Imaging: A Novel Technique for the Evaluation of Fresh Unfixed Surgical Margins


 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Dataset
- -
- to estimate the level of agreement between FCM and final histological diagnosis;
- -
- to assess the reliability of this technique for evaluating cancer infiltration on surgical specimens (ureters/urethra) during ORC.
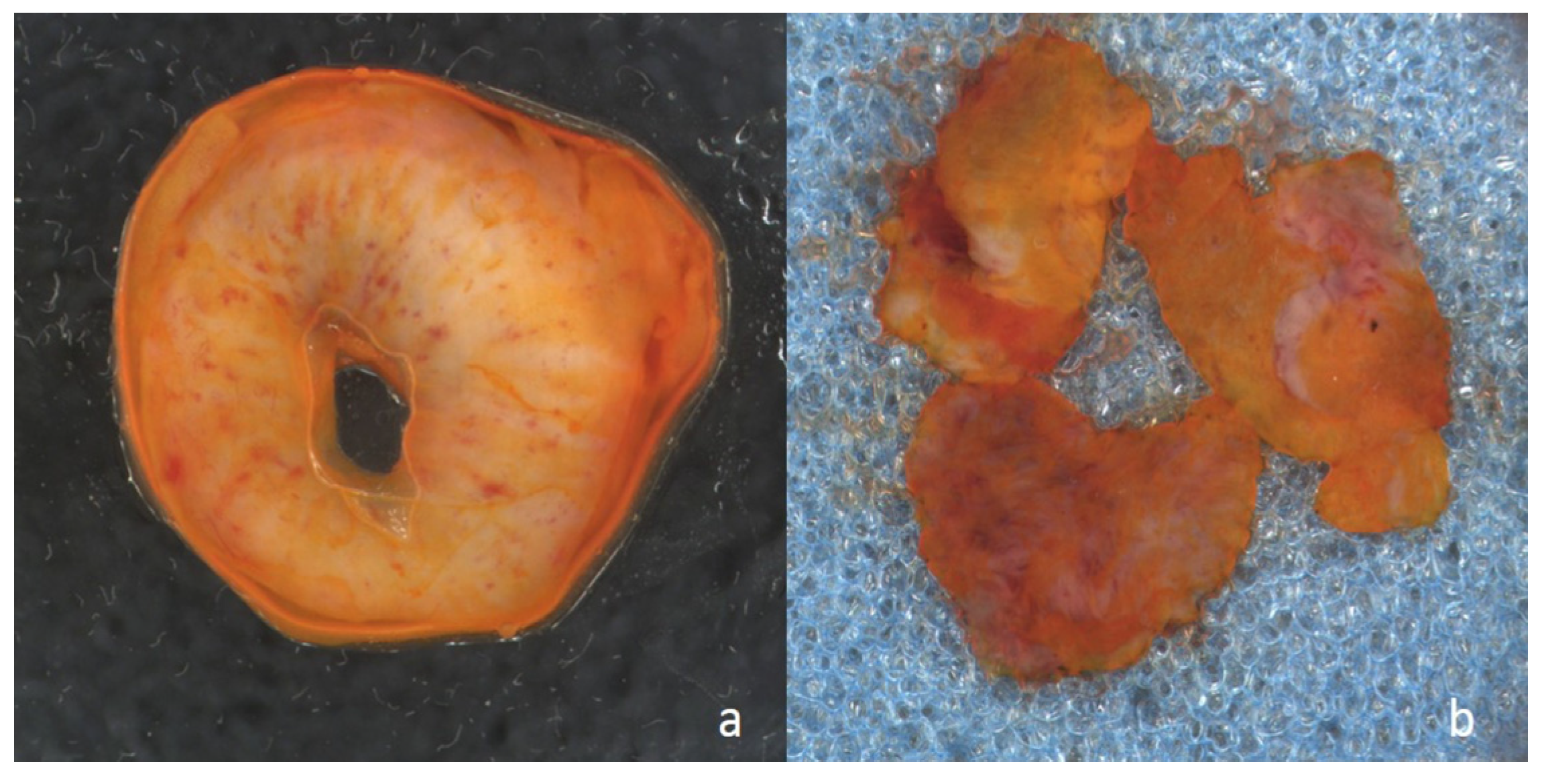
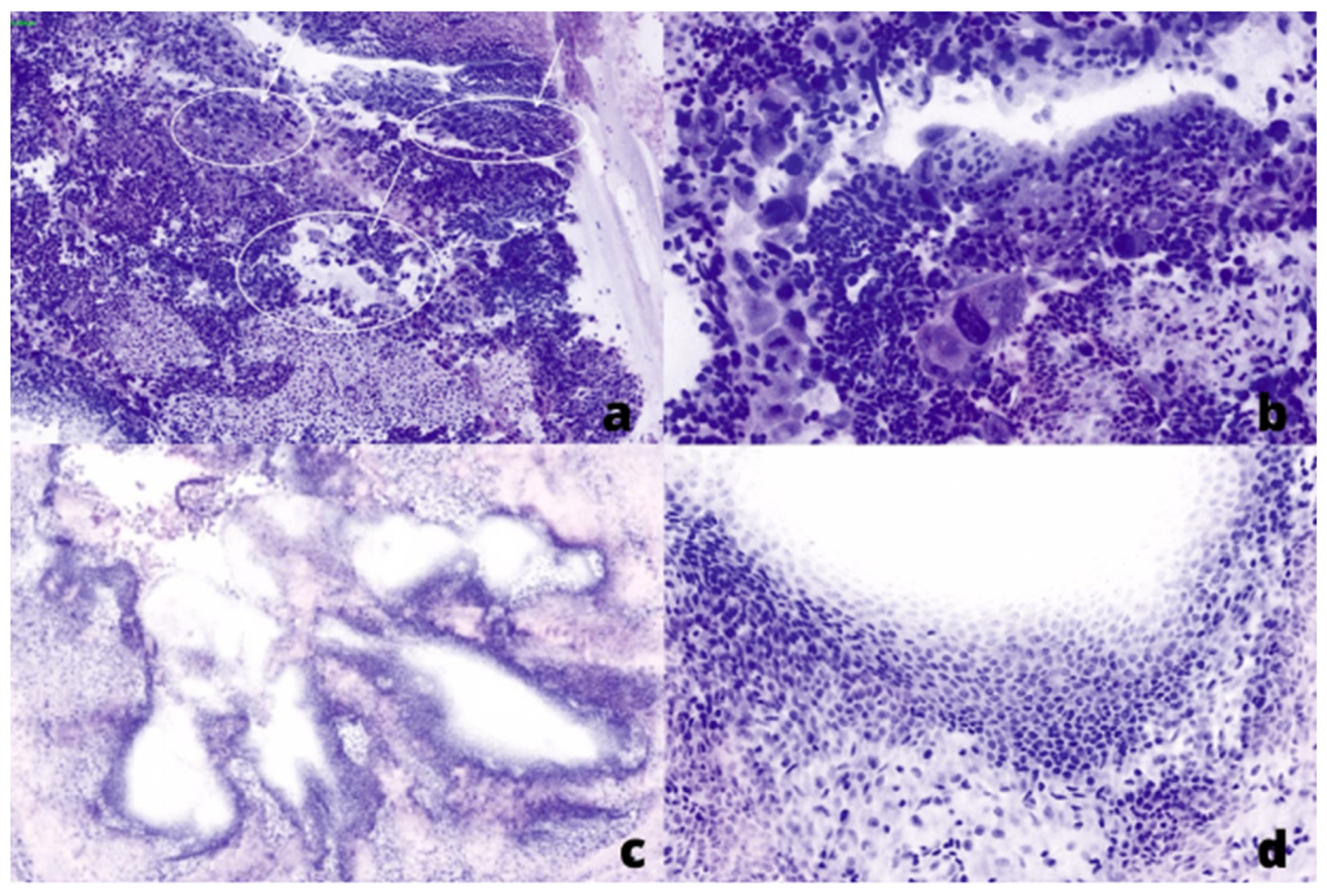
2.2. Fluorescent Confocal Microscopy
2.3. Tissue Preparation
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Linares Espinós, E.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Papalia, R.; Simone, G.; Grasso, R.; Augelli, R.; Faiella, E.; Guaglianone, S.; Cazzato, R.; Del Vescovo, R.; Ferriero, M.; Zobel, B.; et al. Diffusion-weighted magnetic resonance imaging in patients selected for radical cystectomy: Detection rate of pelvic lymph node metastases. BJU Int. 2012, 109, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)—2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef] [PubMed]
- Gakis, G.; Black, P.C.; Bochner, B.H.; Boorjian, S.A.; Stenzl, A.; Thalmann, G.N.; Kassouf, W. Systematic Review on the Fate of the Remnant Urothelium after Radical Cystectomy. Eur. Urol. 2017, 71, 545–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahmy, O.; Khairul-Asri, M.G.; Schubert, T.; Renninger, M.; Kübler, H.; Stenzl, A.; Gakis, G. Urethral recurrence after radical cystectomy for urothelial carcinoma: A systematic review and meta-analysis. Urol. Oncol. 2018, 36, 54–59. [Google Scholar] [CrossRef]
- Chan, Y.; Fisher, P.; Tilki, D.; Evans, C.P. Urethral recurrence after cystectomy: Current preventative measures, diagnosis and management. BJU Int. 2016, 117, 563–569. [Google Scholar] [CrossRef] [PubMed]
- Moschini, M.; Karnes, R.J.; Sharma, V.; Gandaglia, G.; Fossati, N.; Dell’Oglio, P.; Cucchiara, V.; Capogrosso, P.; Shariat, S.F.; Damiano, R.; et al. Patterns and prognostic significance of clinical recurrences after radical cystectomy for bladder cancer: A 20-year single center experience. Eur. J. Surg. Oncol. 2016, 42, 735–743. [Google Scholar] [CrossRef] [PubMed]
- Mastroianni, R.; Ferriero, M.; Tuderti, G.; Anceschi, U.; Bove, A.M.; Brassetti, A.; Misuraca, L.; Zampa, A.; Torregiani, G.; Ghiani, E.; et al. Open Radical Cystectomy versus Robot-Assisted Radical Cystectomy with Intracorporeal Urinary Diversion: Early Outcomes of a Single-Center Randomized Controlled Trial. J. Urol. 2022, 207, 982–992. [Google Scholar] [CrossRef]
- Brassetti, A.; Tuderti, G.; Anceschi, U.; Ferriero, M.; Guaglianone, S.; Gallucci, M.; Simone, G. Combined reporting of surgical quality, cancer control and functional outcomes of robot-assisted radical cystectomy with intracorporeal orthotopic neobladder into a novel trifecta. Minerva Urol. Nefrol. 2019, 71, 590–596. [Google Scholar] [CrossRef]
- Chang, S.S.; Bochner, B.H.; Chou, R.; Dreicer, R.; Kamat, A.M.; Lerner, S.P.; Lotan, Y.; Meeks, J.J.; Michalski, J.M.; Morgan, T.M.; et al. Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline. J. Urol. 2017, 198, 552–559, Erratum in J. Urol. 2017, 198, 1175. [Google Scholar] [CrossRef]
- Laukhtina, E.; Rajwa, P.; Mori, K.; Moschini, M.; D’Andrea, D.; Abufaraj, M.; Soria, F.; Mari, A.; Krajewski, W.; Albisinni, S.; et al. Accuracy of Frozen Section Analysis of Urethral and Ureteral Margins During Radical Cystectomy for Bladder Cancer: A Systematic Review and Diagnostic Meta-Analysis. Eur. Urol. Focus 2022, 8, 752–760. [Google Scholar] [CrossRef]
- Puliatti, S.; Bertoni, L.; Pirola, G.M.; Azzoni, P.; Bevilacqua, L.; Eissa, A.; Elsherbiny, A.; Sighinolfi, M.C.; Chester, J.; Kaleci, S.; et al. Ex vivo fluorescence confocal microscopy: The first application for real-time pathological examination of prostatic tissue. BJU Int. 2019, 124, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Rocco, B.; Sighinolfi, M.C.; Bertoni, L.; Spandri, V.; Puliatti, S.; Eissa, A.; Reggiani Bonetti, L.; Azzoni, P.; Sandri, M.; De Carne, C.; et al. Real-time assessment of surgical margins during radical prostatectomy: A novel approach that uses fluorescence confocal microscopy for the evaluation of peri-prostatic soft tissue. BJU Int. 2020, 125, 487–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocco, B.; Sarchi, L.; Assumma, S.; Cimadamore, A.; Montironi, R.; Reggiani Bonetti, L.; Turri, F.; De Carne, C.; Puliatti, S.; Maiorana, A.; et al. Digital Frozen Sections with Fluorescence Confocal Microscopy During Robot-assisted Radical Prostatectomy: Surgical Technique. Eur. Urol. 2021, 80, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Kates, M.; Ball, M.W.; Chappidi, M.R.; Baras, A.S.; Gordetsky, J.; Sopko, N.A.; Brant, A.; Pierorazio, P.M.; Epstein, J.I.; Schoenberg, M.P.; et al. Accuracy of urethral frozen section during radical cystectomy for bladder cancer. Urol. Oncol. 2016, 34, e1–e532. [Google Scholar] [CrossRef]
- Loeser, A.; Katzenberger, T.; Vergho, D.C.; Kocot, A.; Burger, M.; Riedmiller, H. Frozen section analysis of ureteral margins in patients undergoing radical cystectomy for bladder cancer: Differential impact of carcinoma in situ in the bladder on reliability and impact on tumour recurrence in the upper urinary tract. Urol. Int. 2014, 92, 50–54. [Google Scholar] [CrossRef]
- Gordetsky, J.; Bivalacqua, T.; Schoenberg, M.; Epstein, J.I. Ureteral and urethral frozen sections during radical cystectomy or cystoprostatectomy: An analysis of denudation and atypia. Urology 2014, 84, 619–623. [Google Scholar] [CrossRef] [PubMed]
- Meeks, J.J.; Bellmunt, J.; Bochner, B.H.; Clarke, N.W.; Daneshmand, S.; Galsky, M.D.; Hahn, N.M.; Lerner, S.P.; Mason, M.; Powles, T.; et al. A systematic review of neoadjuvant and adjuvant chemotherapy for muscle-invasive bladder cancer. Eur. Urol. 2012, 62, 523–533. [Google Scholar] [CrossRef]
- Anceschi, U.; Brassetti, A.; Tuderti, G.; Ferriero, M.C.; Costantini, M.; Bove, A.M.; Calabrò, F.; Carlini, P.; Vari, S.; Mastroianni, R.; et al. Impact of Clinical Response to Neoadjuvant Chemotherapy in the Era of Robot Assisted Radical Cystectomy: Results of a Single-Center Experience. J. Clin. Med. 2020, 9, 2736. [Google Scholar] [CrossRef]
- Hakozaki, K.; Kikuchi, E.; Fukumoto, K.; Shirotake, S.; Miyazaki, Y.; Maeda, T.; Kaneko, G.; Yoshimine, S.; Tanaka, N.; Kanai, K.; et al. Significance of a frozen section analysis of the ureteral margin in bladder cancer patients treated with radical cystectomy and neoadjuvant chemotherapy. Med. Oncol. 2017, 34, 187, Published 2017 October 23. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Results |
|---|---|
| Male (n, %) | 37 (80.4%) |
| Female (n, %) | 9 (19.6%) |
| Age (yrs, median) | 74 (70–79) |
| BMI (kg/m2, median) | 25.36 (22.4–28.1) |
| ASA score (n, %) | |
| 1–2 | 20 (43.5%) |
| 3–4 | 26 (56.5%) |
| Smoking History | 35 (76.1%) |
| Current Smoker (n, %) | 16 (34.8%) |
| Former Smoker (n, %) | 19 (41.3%) |
| No smoking history (n, %) | 11 (23.9%) |
| Diabetes (n, %) | 10 (21.7%) |
| Hypertension (n, %) | 33 (71.7%) |
| BCG irrigations (n, %) | 6 (13%) |
| Neoadjuvant chemotherapy (n, %) | |
| GC (n, %) | 6 (13%) |
| Other regimens (n, %) | 0 (0%) |
| Neoadjuvant radiotherapy (n, %) | 0 (0%) |
| Preoperative Hydronephrosis (n, %) | 24 (52.2%) |
| Left | 15 (32.6%) |
| Right | 16 (34.8%) |
| Bilateral | 7 (15.2%) |
| Preoperative CKD stage (n, %) | |
| 1 | 7 (15.2%) |
| 2 | 18 (39.1%) |
| 3a | 10 (21.7%) |
| 3b | 6 (13%) |
| 4–5 | 5 (10.9%) |
| cT (n, %) | |
| 1 | 8 (17.4%) |
| 2 | 25 (54.3%) |
| 3 | 9 (19.5%) |
| 4 | 4 (8.7%) |
| Cis (n, %) | 5 (10.9%) |
| cN (n, %) | 9 (19.5%) |
| 1 | 0 (0%) |
| 2 | 7 (15.2%) |
| 3 | 2 (4.3%) |
| Incidental PCa (n, %) | 13 (351%) |
| Urinary diversion (n, %) | |
| Continent | 11 (23.9%) |
| Incontinent | 35 (76.1%) |
| pT (n, %) | |
| 0 | 4 (8.7%) |
| 1 | 11 (23.9%) |
| 2a | 2 (4.3%) |
| 2b | 7 (15.2%) |
| 3a | 14 (30.4%) |
| 3b | 1 (2.2%) |
| 4a | 6 (13%) |
| 4b | 1 (2.2%) |
| pTis (n, %) | 11 (23.9%) |
| pN (n, %) | 11 (23.9%) |
| 1 | 3 (6.5%) |
| 2 | 7 (15.2%) |
| 3 | 1 (2.2%) |
| Histology (type, n, %) | |
| Urothelial | 43 (93.5%) |
| Squamous | 1 (2.2%) |
| Cribriform | 1 (2.2%) |
| OS (n, %) | 25 (54.3%) |
| CCS (n, %) | 45 (97.8%) |
| MFS (n, %) | 33 (71.7%) |
| Recurrence | |
| Upper urinary tract | 1 (2.2%) |
| Urethral | 0 (0%) |
| Local | 0 (0%) |
| Follow-up (months) (median, IQR) | 11.5 (5–15) |
| Variable | FSA | Final Histology |
|---|---|---|
| Prevalence | 5/5 (100%) | 5/6 (83.3%) |
| Sensitivity | 80% | 66.7% |
| Specificity | 97.8% | 97.5% |
| Positive Predictive Value (PPV) | 80% | 80% |
| Negative Predictive Value (NPV) | 97.6% | 95.1% |
| K Cohen | 0.776 (p < 0.001) | 0.691 (p < 0.001) |
| Variable | FSA | Final Histology |
|---|---|---|
| Prevalence | 7/9 (77.8%) | 7/9 (77.8%) |
| Sensitivity | 69.2% | 53.8% |
| Specificity | 97% | 90.9% |
| Positive Predictive Value (PPV) | 90% | 70% |
| Negative Predictive Value (NPV) | 88.9% | 83.3% |
| K Cohen | 0.712 (p < 0.001) | 0.481 (p < 0.001) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prata, F.; Anceschi, U.; Taffon, C.; Rossi, S.M.; Verri, M.; Iannuzzi, A.; Ragusa, A.; Esperto, F.; Prata, S.M.; Crescenzi, A.; et al. Real-Time Urethral and Ureteral Assessment during Radical Cystectomy Using Ex-Vivo Optical Imaging: A Novel Technique for the Evaluation of Fresh Unfixed Surgical Margins. Curr. Oncol. 2023, 30, 3421-3431. https://doi.org/10.3390/curroncol30030259
Prata F, Anceschi U, Taffon C, Rossi SM, Verri M, Iannuzzi A, Ragusa A, Esperto F, Prata SM, Crescenzi A, et al. Real-Time Urethral and Ureteral Assessment during Radical Cystectomy Using Ex-Vivo Optical Imaging: A Novel Technique for the Evaluation of Fresh Unfixed Surgical Margins. Current Oncology. 2023; 30(3):3421-3431. https://doi.org/10.3390/curroncol30030259
Chicago/Turabian StylePrata, Francesco, Umberto Anceschi, Chiara Taffon, Silvia Maria Rossi, Martina Verri, Andrea Iannuzzi, Alberto Ragusa, Francesco Esperto, Salvatore Mario Prata, Anna Crescenzi, and et al. 2023. "Real-Time Urethral and Ureteral Assessment during Radical Cystectomy Using Ex-Vivo Optical Imaging: A Novel Technique for the Evaluation of Fresh Unfixed Surgical Margins" Current Oncology 30, no. 3: 3421-3431. https://doi.org/10.3390/curroncol30030259