Persisting Deficits in Health-Related Quality of Life of Colorectal Cancer Survivors 14–24 Years Post-Diagnosis: A Population-Based Study

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. CAESAR Study
2.2. LinDe Study
2.3. HRQOL Assessment
2.4. Demographics and Clinical Data
2.5. Statistical Analyses
3. Results
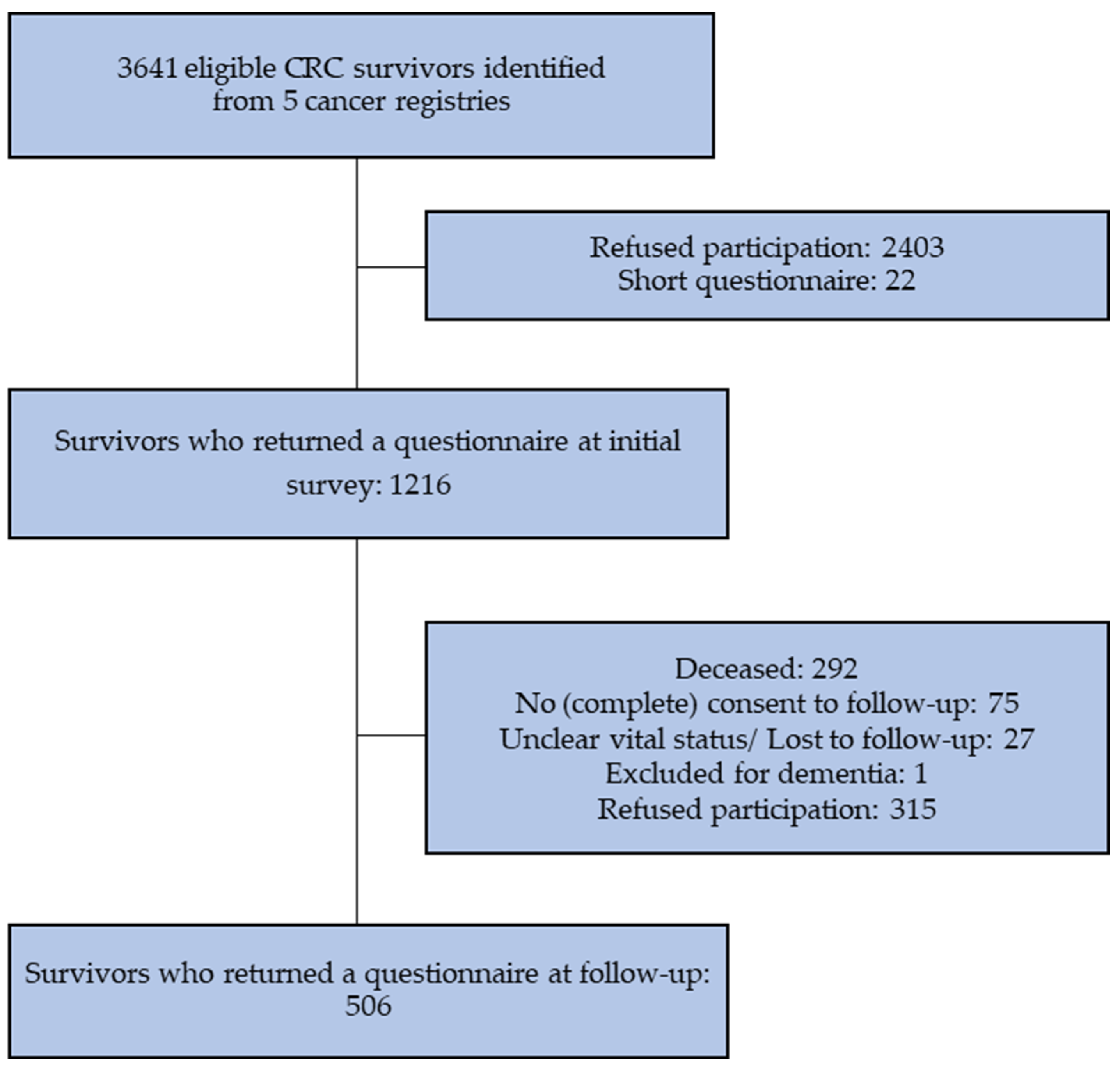
3.1. Non-Response Analysis
3.2. Characteristics of CRC Survivors and Controls
3.3. Characteristics of CRC Survivors by Cancer Type
3.4. HRQOL of CRC Survivors and Controls
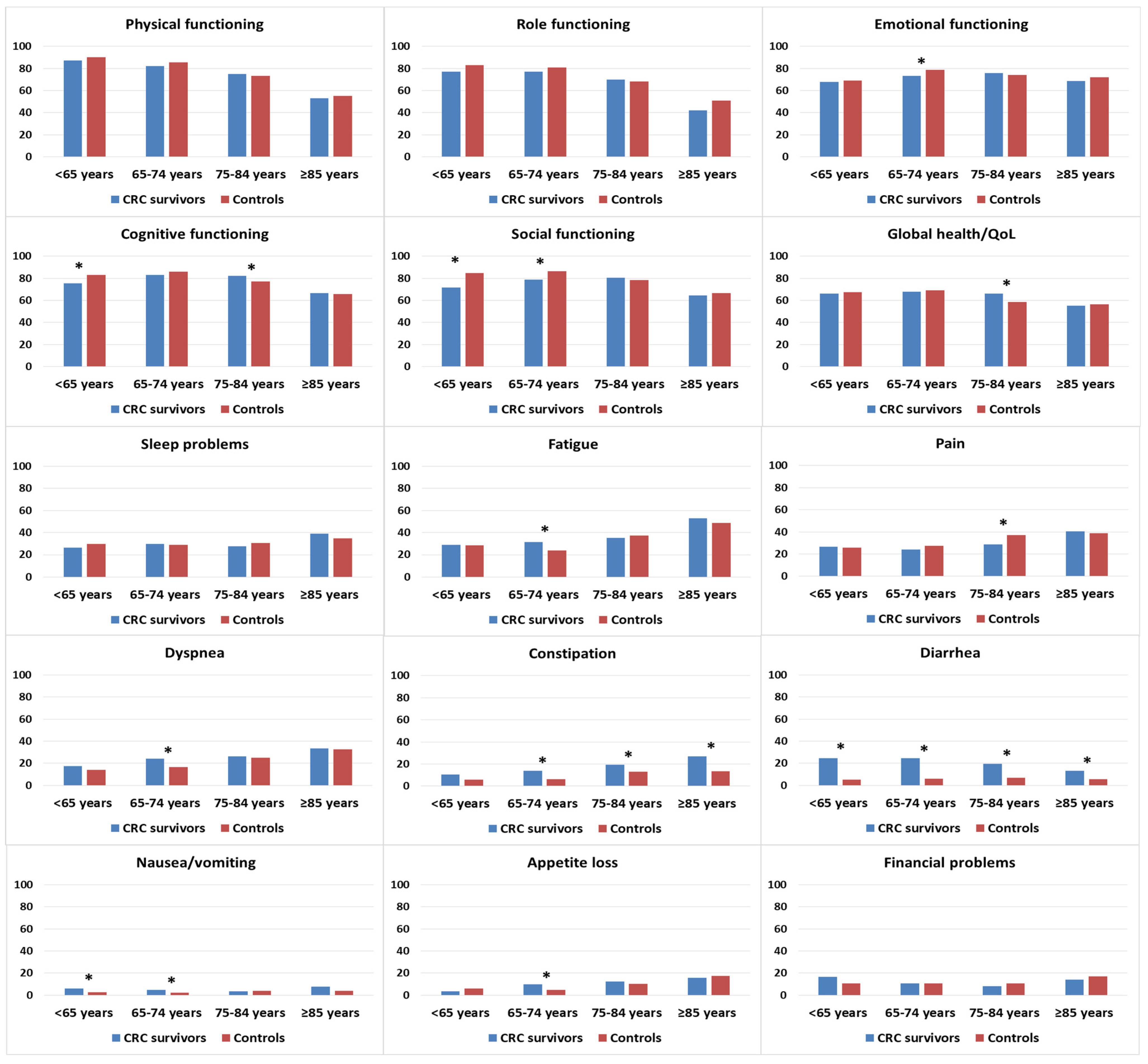
3.5. HRQOL of CRC Survivors and Controls, Stratified by Demographic Factors
3.5.1. By Age at Survey
3.5.2. By Education
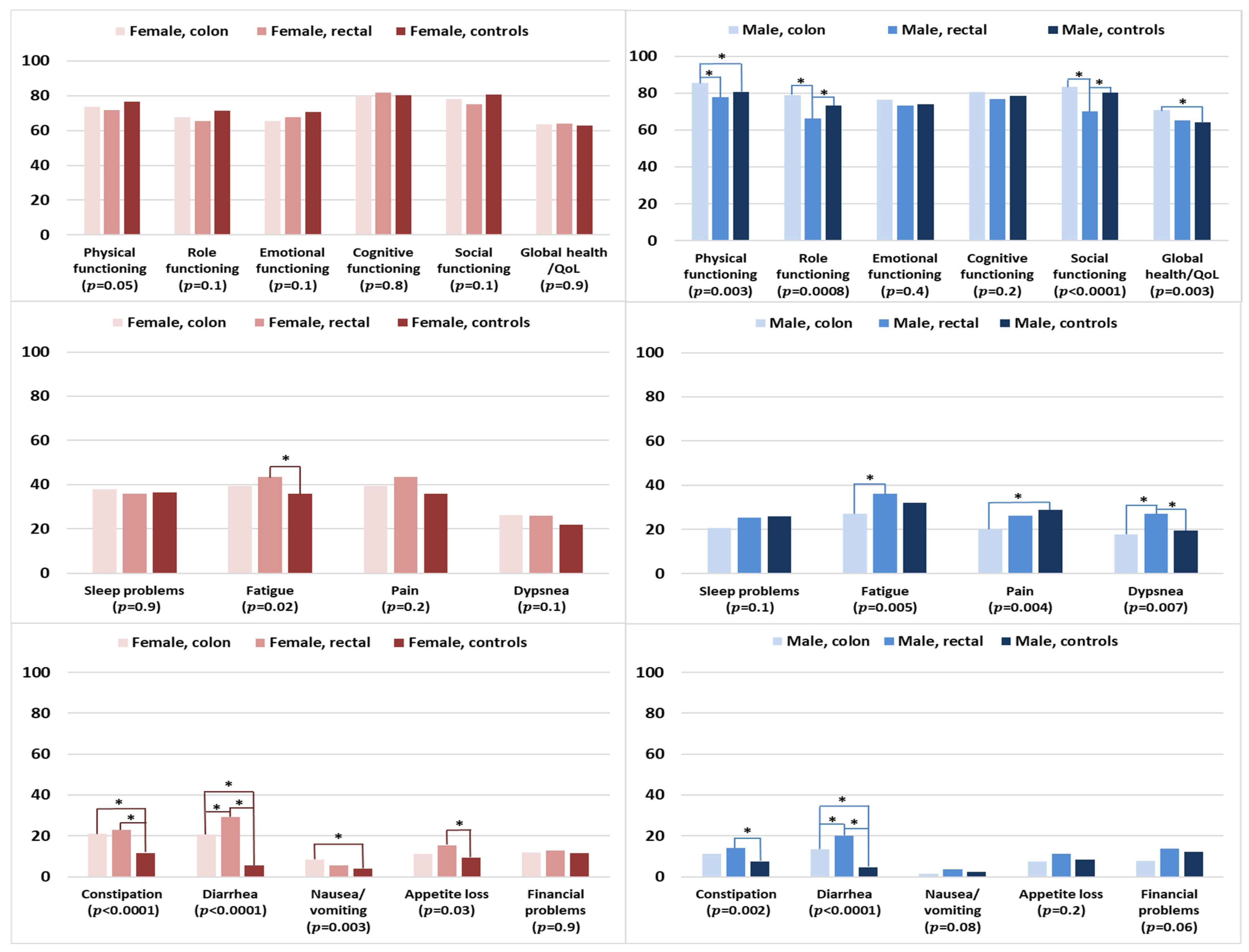
3.6. HRQOL of Survivors by Cancer Type and Controls, Stratified by Sex
3.7. HRQOL of Survivors Stratified by Clinical Factors, and Controls
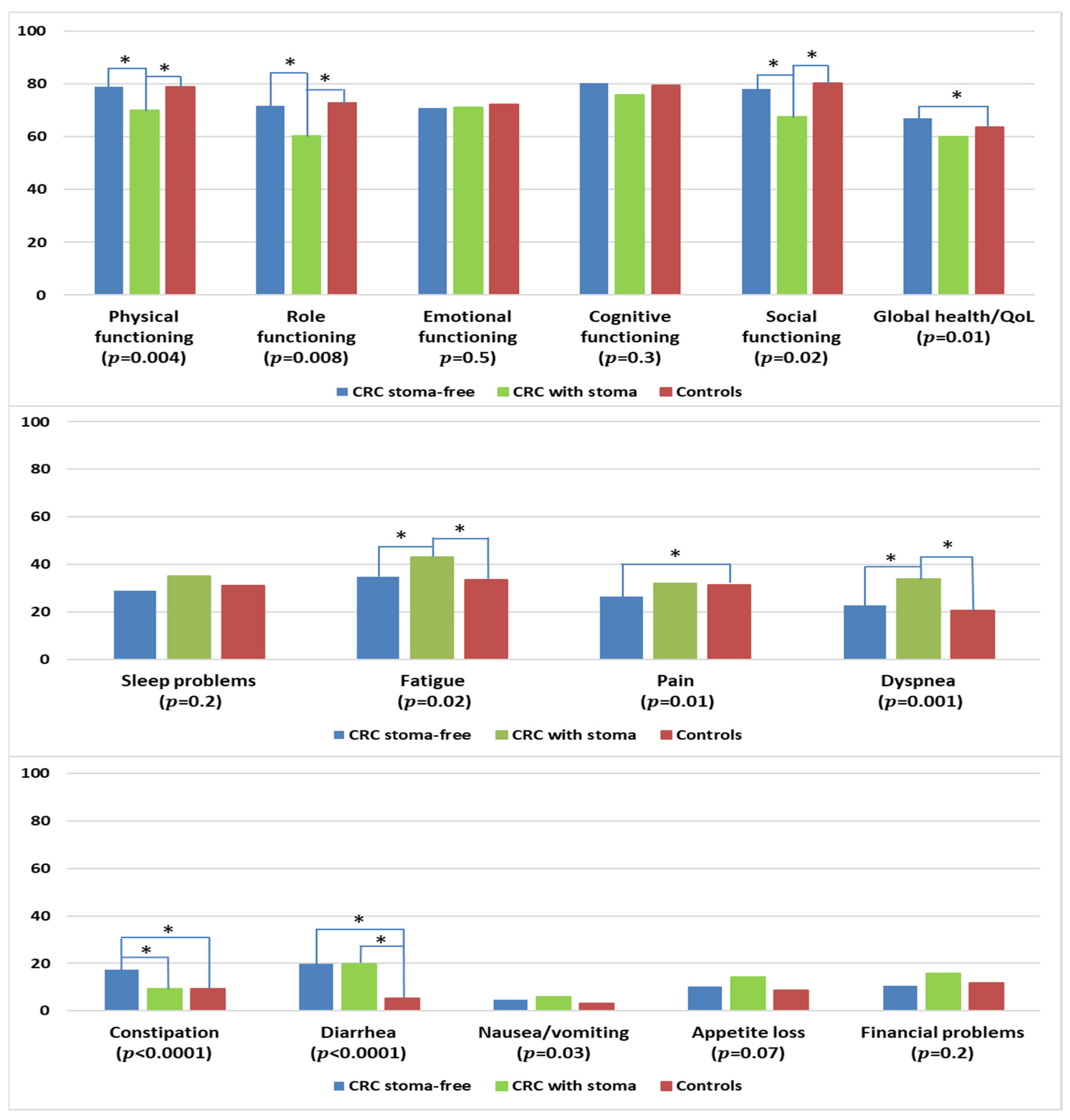
3.7.1. By Stoma Status
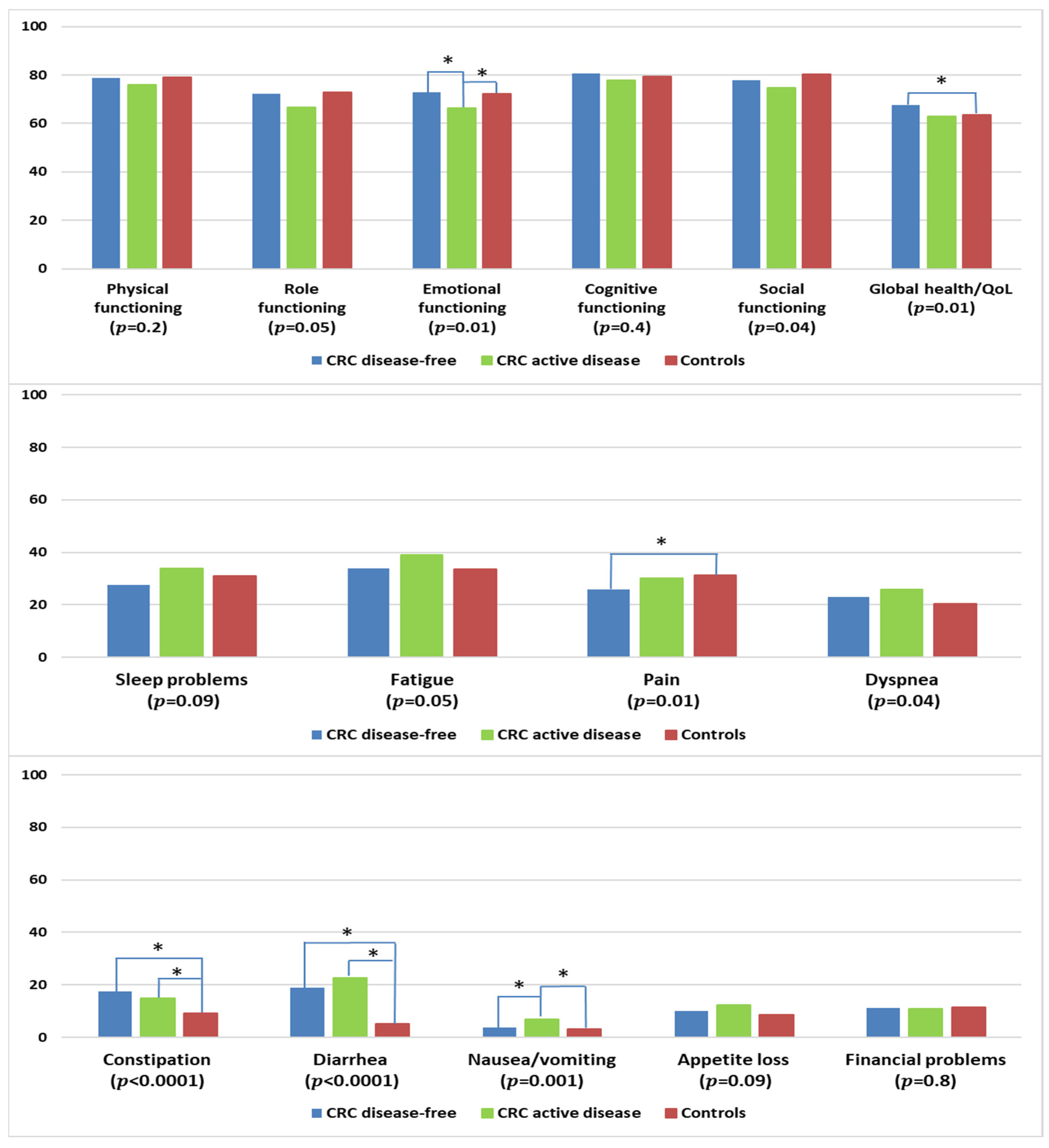
3.7.2. By Disease Status
4. Discussion
4.1. Clinical Implications
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- André, T.; Meyerhardt, J.; Iveson, T.; Sobrero, A.; Yoshino, T.; Souglakos, I.; Grothey, A.; Niedzwiecki, D.; Saunders, M.; Labianca, R.; et al. Effect of duration of adjuvant chemotherapy for patients with stage III colon cancer (IDEA collaboration): Final results from a prospective, pooled analysis of six randomised, phase 3 trials. Lancet Oncol. 2020, 21, 1620–1629. [Google Scholar] [CrossRef]
- Cardoso, R.; Guo, F.; Heisser, T.; Hackl, M.; Ihle, P.; De Schutter, H.; Van Damme, N.; Valerianova, Z.; Atanasov, T.; Májek, O.; et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: An international population-based study. Lancet Oncol. 2021, 22, 1002–1013. [Google Scholar] [CrossRef]
- van Gijn, W.; Marijnen, C.A.; Nagtegaal, I.D.; Kranenbarg, E.M.; Putter, H.; Wiggers, T.; Rutten, H.J.; Påhlman, L.; Glimelius, B.; van de Velde, C.J. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011, 12, 575–582. [Google Scholar] [CrossRef]
- Jansen, L.; Castro, F.A.; Gondos, A.; Krilaviciute, A.; Barnes, B.; Eberle, A.; Emrich, K.; Hentschel, S.; Holleczek, B.; Katalinic, A.; et al. Recent cancer survival in Germany: An analysis of common and less common cancers. Int. J. Cancer 2014, 136, 2649–2658. [Google Scholar] [CrossRef] [PubMed]
- Schlesinger-Raab, A.; Werner, J.; Friess, H.; Hölzel, D.; Engel, J. Age and Outcome in Gastrointestinal Cancers: A Population-Based Evaluation of Oesophageal, Gastric and Colorectal Cancer. Visc. Med. 2017, 33, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Qaderi, S.M.; Dickman, P.W.; De Wilt, J.H.; Verhoeven, R. Conditional Survival and Cure of Patients with Colon or Rectal Cancer: A Population-Based Study. J. Natl. Compr. Cancer Netw. 2020, 18, 1230–1237. [Google Scholar] [CrossRef]
- United States Department of Health and Human Services Food and Drug Administration. Patient-Reported Outcome Measures: Use in Medical Product Development to Support Labeling Claims; United States Department of Health and Human Services Food and Drug Administration: Silver Spring, MD, USA, 2009.
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soerjomataram, I.; Thong, M.S.Y.; Ezzati, M.; Lamont, E.B.; Nusselder, W.J.; Van De Poll-Franse, L.V. Most colorectal cancer survivors live a large proportion of their remaining life in good health. Cancer Causes Control 2012, 23, 1421–1428. [Google Scholar] [CrossRef] [Green Version]
- Mols, F.; Beijers, T.; Lemmens, V.; Hurk, C.J.V.D.; Vreugdenhil, G.; van de Poll-Franse, L.V. Chemotherapy-Induced Neuropathy and Its Association with Quality of Life Among 2- to 11-Year Colorectal Cancer Survivors: Results from the Population-Based PROFILES Registry. J. Clin. Oncol. 2013, 31, 2699–2707. [Google Scholar] [CrossRef]
- Chen, T.Y.-T.; Wiltink, L.M.; Nout, R.A.; Kranenbarg, E.M.-K.; Laurberg, S.; Marijnen, C.A.; van de Velde, C.J. Bowel Function 14 Years after Preoperative Short-Course Radiotherapy and Total Mesorectal Excision for Rectal Cancer: Report of a Multicenter Randomized Trial. Clin. Color. Cancer 2014, 14, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Thong, M.S.Y.; Koch-Gallenkamp, L.; Jansen, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Waldeyer-Sauerland, M.; Waldmann, A.; Zeissig, S.R.; Brenner, H.; et al. Age-specific health-related quality of life in long-term and very long-term colorectal cancer survivors versus population controls—A population-based study. Acta Oncol. 2019, 58, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bennett, J.A.; Cameron, L.D.; Brown, P.M.; Whitehead, L.C.; Porter, D.; Ottaway-Parkes, T.; Robinson, E. Time Since Diagnosis as a Predictor of Symptoms, Depression, Cognition, Social Concerns, Perceived Benefits, and Overall Health in Cancer Survivors. Oncol. Nurs. Forum 2010, 37, 331–338. [Google Scholar] [CrossRef] [Green Version]
- Caravati-Jouvenceaux, A.; Launoy, G.; Klein, D.; Henry-Amar, M.; Abeilard, E.; Danzon, A.; Pozet, A.; Velten, M.; Mercier, M. Health-Related Quality of Life Among Long-Term Survivors of Colorectal Cancer: A Population-Based Study. Oncologist 2011, 16, 1626–1636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hart, T.L.; Charles, S.T.; Gunaratne, M.; Baxter, N.N.; Cotterchio, M.; Cohen, Z.; Gallinger, S. Symptom Severity and Quality of Life Among Long-term Colorectal Cancer Survivors Compared with Matched Control Subjects: A Population-Based Study. Dis. Colon Rectum 2018, 61, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Kunitake, H.; Russell, M.M.; Zheng, P.; Yothers, G.; Land, S.R.; Petersen, L.; Fehrenbacher, L.; Giguere, J.K.; Wickerham, D.L.; Ko, C.Y.; et al. Quality of life and symptoms in long-term survivors of colorectal cancer: Results from NSABP protocol LTS-01. J. Cancer Surviv. 2016, 11, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doege, D.; Thong, M.S.; Weisser, L.; Koch-Gallenkamp, L.; Jansen, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Nennecke, A.; Pritzkuleit, R.; et al. Health-related quality of life in cancer survivors >10 years past diagnosis compared to population controls: A population-based study. Cancers 2021, 13, 2754. [Google Scholar] [CrossRef]
- Arndt, V.; Koch-Gallenkamp, L.; Jansen, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Schmid-Höpfner, S.; Waldmann, A.; Zeissig, S.R.; Brenner, H. Quality of life in long-term and very long-term cancer survivors versus population controls in Germany. Acta Oncol. 2017, 56, 190–197. [Google Scholar] [CrossRef] [Green Version]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; De Haes, J.C.J.M.; et al. The European Organization for Research and Treatment of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. JNCI J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef]
- Fayers, P.M.; Aaronson, N.K.; Bjordal, K.; Sullivan, M. EORTC QLQ-C30 Scoring Manual; EORTC: Brussels, Belgium, 1995. [Google Scholar]
- Jansen, L.; Koch, L.; Brenner, H.; Arndt, V. Quality of life among long-term (≥5 years) colorectal cancer survivors—Systematic review. Eur. J. Cancer 2010, 46, 2879–2888. [Google Scholar] [CrossRef]
- Reyes, M.E.; Ye, Y.; Zhou, Y.; Liang, A.; Kopetz, S.; Rodriquez, M.A.; Wu, X.; Hildebrandt, M.A.T. Predictors of health-related quality of life and association with survival may identify colorectal cancer patients at high risk of poor prognosis. Qual. Life Res. 2016, 26, 319–330. [Google Scholar] [CrossRef] [Green Version]
- van Heinsbergen, M.; Janssen-Heijnen, M.L.; Leijtens, J.W.; Slooter, G.D.; Konsten, J.L. Bowel dysfunction after sigmoid resection underestimated: Multicentre study on quality of life after surgery for carcinoma of the rectum and sigmoid. Eur. J. Surg. Oncol. 2018, 44, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Al Rashid, F.; Liberman, A.S.; Charlebois, P.; Stein, B.; Feldman, L.S.; Fiore, J.F., Jr.; Lee, L. The impact of bowel dysfunction on health-related quality of life after rectal cancer surgery: A systematic review. Tech. Coloproctol. 2022, 26, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.Y.S.; Laidsaar-Powell, R.C.; Young, J.M.; Kao, S.C.; Zhang, Y.; Butow, P. Colorectal cancer survivorship: A systematic review and thematic synthesis of qualitative research. Eur. J. Cancer Care 2021, 30, e13421. [Google Scholar] [CrossRef] [PubMed]
- Drury, A.; Payne, S.; Brady, A.-M. Prevalence vs impact: A mixed methods study of survivorship issues in colorectal cancer. Qual. Life Res. 2021, 31, 1117–1134. [Google Scholar] [CrossRef]
- Sun, V.; Grant, M.; Wendel, C.S.; McMullen, C.K.; Bulkley, J.E.; Altschuler, A.; Ramirez, M.; Baldwin, C.M.; Herrinton, L.J.; Hornbrook, M.C.; et al. Dietary and Behavioral Adjustments to Manage Bowel Dysfunction After Surgery in Long-Term Colorectal Cancer Survivors. Ann. Surg. Oncol. 2015, 22, 4317–4324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jansen, F.; Van Uden-Kraan, C.F.; Braakman, J.A.; Van Keizerswaard, P.M.; Witte, B.I.; Leeuw, I.M.V.-D. A mixed-method study on the generic and ostomy-specific quality of life of cancer and non-cancer ostomy patients. Support. Care Cancer 2014, 23, 1689–1697. [Google Scholar] [CrossRef]
- Mols, F.; Lemmens, V.; Bosscha, K.; Broek, W.V.D.; Thong, M.S. Living with the physical and mental consequences of an ostomy: A study among 1-10-year rectal cancer survivors from the population-based PROFILES registry. Psycho-Oncology 2014, 23, 998–1004. [Google Scholar] [CrossRef]
- Näsvall, P.; Dahlstrand, U.; Löwenmark, T.; Rutegård, J.; Gunnarsson, U.; Strigård, K. Quality of life in patients with a permanent stoma after rectal cancer surgery. Qual. Life Res. 2016, 26, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Vonk-Klaassen, S.M.; De Vocht, H.M.; den Ouden, M.E.M.; Eddes, E.H.; Schuurmans, M.J. Ostomy-related problems and their impact on quality of life of colorectal cancer ostomates: A systematic review. Qual. Life Res. 2016, 25, 125–133. [Google Scholar] [CrossRef] [Green Version]
- Dunn, J.; Ng, S.K.; Breitbart, W.; Aitken, J.; Youl, P.; Baade, P.D.; Chambers, S.K. Health-related quality of life and life satisfaction in colorectal cancer survivors: Trajectories of adjustment. Health Qual. Life Outcomes 2013, 11, 46. [Google Scholar] [CrossRef] [Green Version]
- Wong, M.C.; Huang, J.; Lok, V.; Wang, J.; Fung, F.; Ding, H.; Zheng, Z.-J. Differences in Incidence and Mortality Trends of Colorectal Cancer Worldwide Based on Sex, Age, and Anatomic Location. Clin. Gastroenterol. Hepatol. 2020, 19, 955–966.e61. [Google Scholar] [CrossRef]
- Wiltink, L.M.; White, K.; King, M.T.; Rutherford, C. Systematic review of clinical practice guidelines for colorectal and anal cancer: The extent of recommendations for managing long-term symptoms and functional impairments. Support. Care Cancer 2020, 28, 2523–2532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- German Cancer Society GCA, AWMF. German Guideline Program in Oncology; S3-Guideline Colorectal Cancer, Long Version 2.1, 2019 AWMF Registration Number: 021-007OL; German Cancer Society GCA, AWMF: Berlin, Germany, 2019. [Google Scholar]
- Yde, J.; Larsen, H.M.; Laurberg, S.; Krogh, K.; Moeller, H.B. Chronic diarrhoea following surgery for colon cancer—Frequency, causes and treatment options. Int. J. Colorectal. Dis. 2018, 33, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Larsen, H.M.; Borre, M.; Christensen, P.; Drewes, A.; Laurberg, S.; Krogh, K.; Fassov, J. Clinical evaluation and treatment of chronic bowel symptoms following cancer in the colon and pelvic organs. Acta Oncol. 2019, 58, 776–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.; Song, M. Chapter Four—Personalized nutrition for colorectal cancer. In Advances in Cancer Research; Berger, F.G., Boland, C.R., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 109–136. [Google Scholar]
- Borre, M.; Fassov, J.; Juul, T.; Laurberg, S.; Christensen, P.; Bräuner, A.B.; Ussing, O.T.; Lauritzen, M.B.; Drewes, A.M.; Faaborg, P.M.; et al. Diet and bowel symptoms among colon cancer survivors. Acta Oncol. 2022, 61, 1192–1199. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Aziz, N.M.; Rowland, J.H.; Pinto, B.M. Riding the Crest of the Teachable Moment: Promoting Long-Term Health After the Diagnosis of Cancer. J. Clin. Oncol. 2005, 23, 5814–5830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, S.Y.; Turner, J.; Kerin-Ayres, K.; Butler, S.; Deguchi, C.; Khatri, S.; Mo, C.; Warby, A.; Cunningham, I.; Malalasekera, A.; et al. Health concerns of cancer survivors after primary anti-cancer treatment. Support. Care Cancer 2019, 27, 3739–3747. [Google Scholar] [CrossRef] [PubMed]
- Akhtar-Danesh, N.; Logie, K.; Akhtar-Danesh, G.-G.; Finley, C. Uptake of minimally invasive surgery for early stage colorectal cancer and its effect on survival: A population-based study. Surg. Oncol. 2020, 35, 540–546. [Google Scholar] [CrossRef]
- Benz, S.; Barlag, H.; Gerken, M.; Fürst, A.; Klinkhammer-Schalke, M. Laparoscopic surgery in patients with colon cancer: A population-based analysis. Surg. Endosc. 2016, 31, 2586–2595. [Google Scholar] [CrossRef]
- Sussman, J.; Bainbridge, D.; Whelan, T.J.; Brazil, K.; Parpia, S.; Wiernikowski, J.; Schiff, S.; Rodin, G.; Sergeant, M.; Howell, D. Evaluation of a specialized oncology nursing supportive care intervention in newly diagnosed breast and colorectal cancer patients following surgery: A cluster randomized trial. Support. Care Cancer 2017, 26, 1533–1541. [Google Scholar] [CrossRef] [Green Version]
- Thong, M.S.Y.; Jansen, L.; Chang-Claude, J.; Hoffmeister, M.; Brenner, H.; Arndt, V. Association of laparoscopic colectomy versus open colectomy on the long-term health-related quality of life of colon cancer survivors. Surg. Endosc. 2020, 34, 5593–5603. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. From Cancer Patients to Cancer Survivors: Lost in Transition; The National Academies Press: Washington, DC, USA, 2006. [Google Scholar]
- Vaz-Luis, I.; Masiero, M.; Cavaletti, G.; Cervantes, A.; Chlebowski, R.; Curigliano, G.; Felip, E.; Ferreira, A.; Ganz, P.; Hegarty, J.; et al. ESMO Expert Consensus Statements on Cancer Survivorship: Promoting high-quality survivorship care and research in Europe. Ann. Oncol. 2022, 33, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Muls, A.C.; Watson, L.; Shaw, C.; Andreyev, H.J.N. Managing gastrointestinal symptoms after cancer treatment: A practical approach for gastroenterologists. Front. Gastroenterol. 2012, 4, 57–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) | Respondents (n = 506) | Non- Respondents (n = 418) | Died (n = 292) | p-Value |
|---|---|---|---|---|
| Mean age at initial survey ± SD | 67.8 ± 8.4 | 71.2 ± 8.5 | 73.7 ± 7.9 | <0.0001 |
| Time to initial survey since diagnosis ± SD | 8.4 ± 2.5 | 8.5 ± 2.5 | 8.8 ± 2.5 | 0.1 |
| Sex | <0.0001 | |||
| Female | 207 (41) | 208 (50) | 89 (30) | |
| Male | 300 (59) | 210 (50) | 203 (70) | |
| Tumor type | 0.0009 | |||
| Colon | 280 (55) | 275 (66) | 157 (54) | |
| Rectal | 227 (45) | 143 834) | 135 (46) | |
| Tumor stage | 0.03 | |||
| I | 123 (24) | 103 (25) | 54 (18) | |
| II | 145 (29) | 113 (27) | 80 (27) | |
| III | 134 (26) | 94 (22) | 83 (28) | |
| IV | 16 (3) | 18 (4) | 22 (8) | |
| Missing | 89 (18) | 90 (22) | 53 (18) | |
| Surgery | 0.003 | |||
| Yes | 408 (80) | 293 (70) | 207 (71) | |
| No | 90 (18) | 105 (25) | 75 (26) | |
| Missing | 9 (2) | 16 (5) | 10 (3) | |
| Chemotherapy | 0.01 | |||
| Yes | 235 (46) | 163 (39) | 146 (50) | |
| No | 269 (51) | 239 (57) | 137 (47) | |
| Missing | 13 (3) | 16 (4) | 9 (3) | |
| Radiotherapy | 0.01 | |||
| Yes | 117 (23) | 68 (16) | 66 (23) | |
| No | 360 (71) | 321 (77) | 193 (66) | |
| Missing | 30 (6) | 29 (7) | 33 (11) | |
| Immuno-/antibody therapy | 0.6 | |||
| Yes | 19 (4) | 12 (3) | 12 (4) | |
| No | 451 (89) | 368 (88) | 249 (85) | |
| Missing | 37 (7) | 38 (9) | 31 (11) | |
| Permanent stoma | <0.0001 | |||
| Yes | 55 (11) | 35 (8) | 59 (20) | |
| No | 452 (89) | 382 (92) | 233 (80) | |
| Missing | 0 | 1 (0.2) | 0 |
| CRC Survivors | Population Controls | Pcrude (χ2) | Padjusted (CMH) a | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | %adj a | |||
| Total | 506 | 100.0 | 1489 | 100.0 | |||
| Age at survey | <0.0001 | - | |||||
| <65 years | 52 | 10.3 | 665 | 44.7 | 10.3 | ||
| 65–74 years | 118 | 23.3 | 401 | 26.9 | 23.3 | ||
| 75–84 years | 268 | 53.0 | 317 | 21.3 | 53.0 | ||
| ≥85 years | 68 | 13.4 | 106 | 7.1 | 13.4 | ||
| Mean age at survey(SD) | 76.1 | (8.4) | 67.0 | (11.8) | |||
| Sex: Male | 299 | 59.1 | 717 | 48.2 | 59.1 | <0.0001 | - |
| Education | 0.0006 | 0.61 | |||||
| ≤9 years | 264 | 52.1 | 631 | 42.4 | 51.8 | ||
| 10–11 years | 111 | 21.9 | 374 | 25.1 | 19.3 | ||
| ≥12 years | 131 | 25.9 | 484 | 32.5 | 28.9 | ||
| Employment at survey | <0.0001 | <0.0001 | |||||
| Full-time | 19 | 3.8 | 315 | 21.1 | 5.5 | ||
| Part-time | 15 | 3.0 | 169 | 11.4 | 3.5 | ||
| Early retired/unemployed | 394 | 77.9 | 790 | 53.1 | 75.9 | ||
| Houseman/wife | 49 | 9.6 | 157 | 10.5 | 11.3 | ||
| Other | 29 | 5.7 | 58 | 3.9 | 3.8 | ||
| In partnered relationship | 390 | 77.0 | 1104 | 74.2 | 68.5 | 0.20 | 0.0002 |
| Self-reported comorbidities | |||||||
| Stroke | 30 | 5.9 | 71 | 4.8 | 7.2 | 0.3 | 0.3 |
| Myocardial infarction | 39 | 7.6 | 70 | 4.7 | 7.5 | 0.01 | 0.9 |
| Angina pectoris | 43 | 8.5 | 152 | 10.2 | 16.4 | 0.2 | <0.0001 |
| Chronic heart failure | 63 | 12.4 | 168 | 11.3 | 19.4 | 0.4 | 0.002 |
| Neurological disease | 13 | 2.6 | 66 | 4.4 | 6.0 | 0.06 | 0.006 |
| Upper gastrointestinal problems | 51 | 10.1 | 193 | 13.0 | 14.1 | 0.08 | 0.04 |
| Arthrosis | 202 | 39.9 | 525 | 35.3 | 40.0 | 0.06 | 0.9 |
| Rheumatism/arthritis | 55 | 10.8 | 233 | 15.6 | 20.7 | 0.007 | <0.0001 |
| Osteoporosis | 69 | 13.7 | 167 | 11.2 | 16.5 | 0.1 | 0.2 |
| Diabetes mellitus | 76 | 15.1 | 216 | 14.5 | 18.9 | 0.7 | 0.07 |
| Chronic obstructive pulmonary disorder | 35 | 6.8 | 58 | 3.9 | 4.8 | 0.007 | 0.1 |
| Asthma | 32 | 6.3 | 89 | 6.0 | 5.5 | 0.7 | 0.6 |
| Hearing problems | 150 | 29.5 | 301 | 20.2 | 32.7 | <0.0001 | 0.2 |
| Chronic back pain | 187 | 37.0 | 522 | 35.0 | 38.3 | 0.4 | 0.6 |
| Depression (ever) | 53 | 10.5 | 242 | 16.2 | 13.4 | 0.001 | 0.1 |
| Anxiety/panic attack (ever) | 25 | 5.0 | 139 | 9.3 | 7.0 | 0.002 | 0.1 |
| Number of comorbidities | 0.01 | 0.001 | |||||
| None | 115 | 22.8 | 367 | 24.6 | 15.3 | ||
| One | 101 | 20.0 | 373 | 25.0 | 22.7 | ||
| Two to three | 173 | 34.1 | 412 | 27.7 | 32.1 | ||
| Four or more | 116 | 23.0 | 337 | 22.7 | 29.9 | ||
| Colon (n = 279) | Rectal (n = 227) | p-Value b | |||
|---|---|---|---|---|---|
| n | % MI a | n | % MI a | ||
| Sex | 0.2 | ||||
| Female | 121 | 43.4 | 86 | 37.9 | |
| Male | 158 | 56.6 | 141 | 62.1 | |
| Age at survey | 0.9 | ||||
| <65 years | 27 | 9.7 | 25 | 11.0 | |
| 65–74 years | 64 | 22.9 | 54 | 23.8 | |
| 75–84 years | 149 | 53.4 | 119 | 52.4 | |
| ≥85 years | 39 | 14.0 | 29 | 12.8 | |
| Mean age at survey(SD) | 76.3 | (8.6) | 75.8 | (8.1) | 0.5 |
| Mean time since diagnosis | 16.7 | (2.6) | 16.8 | (2.5) | 0.8 |
| Cancer stage at diagnosis (UICC) | 0.1 | ||||
| I | 70 | 25.2 | 73 | 32.2 | |
| II | 112 | 40.0 | 72 | 31.8 | |
| III | 83 | 29.7 | 74 | 32.8 | |
| IV | 14 | 5.1 | 7 | 3.3 | |
| Primary treatment | |||||
| Surgery | 221 | 79.4 | 193 | 85.2 | 0.09 |
| Chemotherapy | 120 | 42.9 | 121 | 53.2 | 0.02 |
| Radiotherapy | 23 | 8.2 | 103 | 45.5 | <0.0001 |
| Immuno-/antibody therapy | 5 | 5.2 | 5 | 2.3 | 0.09 |
| Permanent stoma | 2 | 0.7 | 53 | 23.3 | <0.0001 |
| Disease progression | 0.7 | ||||
| None | 208 | 74.6 | 170 | 74.9 | |
| Between diagnosis and 1st survey | 30 | 10.8 | 20 | 8.8 | |
| Between 1st and 2nd survey | 41 | 14.7 | 37 | 16.3 | |
| Number of comorbidities | 0.7 | ||||
| None | 60 | 21.6 | 55 | 24.3 | |
| One | 60 | 21.6 | 41 | 18.1 | |
| Two to three | 96 | 34.3 | 77 | 34.0 | |
| Four or more | 63 | 22.5 | 54 | 23.6 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thong, M.S.Y.; Doege, D.; Weißer, L.; Koch-Gallenkamp, L.; Jansen, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Nennecke, A.; Waldmann, A.; et al. Persisting Deficits in Health-Related Quality of Life of Colorectal Cancer Survivors 14–24 Years Post-Diagnosis: A Population-Based Study. Curr. Oncol. 2023, 30, 3373-3390. https://doi.org/10.3390/curroncol30030257
Thong MSY, Doege D, Weißer L, Koch-Gallenkamp L, Jansen L, Bertram H, Eberle A, Holleczek B, Nennecke A, Waldmann A, et al. Persisting Deficits in Health-Related Quality of Life of Colorectal Cancer Survivors 14–24 Years Post-Diagnosis: A Population-Based Study. Current Oncology. 2023; 30(3):3373-3390. https://doi.org/10.3390/curroncol30030257
Chicago/Turabian StyleThong, Melissa S. Y., Daniela Doege, Linda Weißer, Lena Koch-Gallenkamp, Lina Jansen, Heike Bertram, Andrea Eberle, Bernd Holleczek, Alice Nennecke, Annika Waldmann, and et al. 2023. "Persisting Deficits in Health-Related Quality of Life of Colorectal Cancer Survivors 14–24 Years Post-Diagnosis: A Population-Based Study" Current Oncology 30, no. 3: 3373-3390. https://doi.org/10.3390/curroncol30030257