Adaptive Volumetric-Modulated Arc Radiation Therapy for Head and Neck Cancer: Evaluation of Benefit on Target Coverage and Sparing of Organs at Risk

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
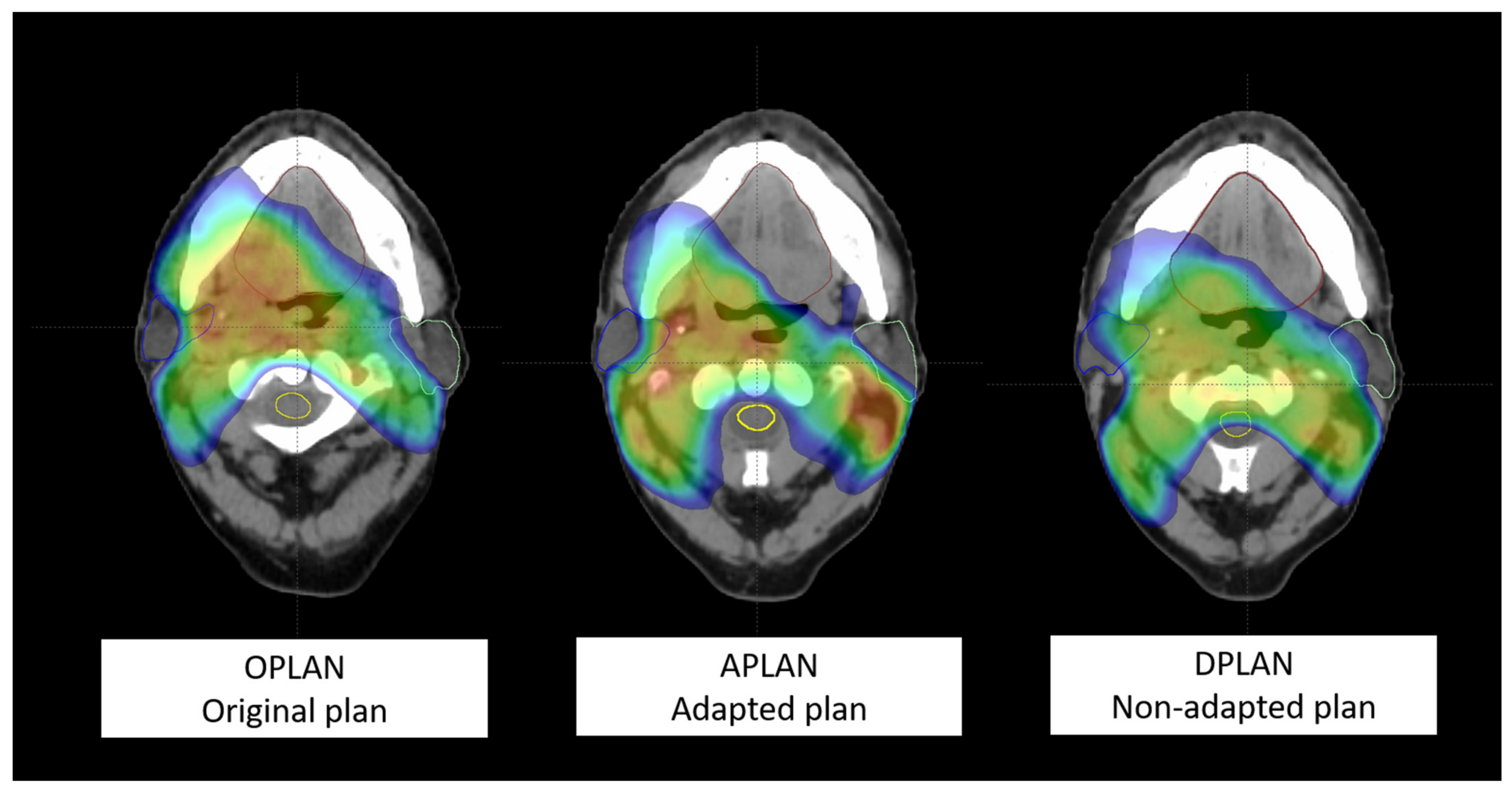
- (1)
- first simulation CT and original plan (OPLAN);
- (2)
- second simulation CT and adapted plan (APLAN);
- (3)
- second simulation CT and original plan (DPLAN).
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Santuray, R.T.; Johnson, D.E.; Grandis, J.R. New Therapies in Head and Neck Cancer. Trends Cancer 2018, 4, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Veresezan, O.; Troussier, I.; Lacout, A.; Kreps, S.; Maillard, S.; Toulemonde, A.; Marcy, P.-Y.; Huguet, F.; Thariat, J. Adaptive radiation therapy in head and neck cancer for clinical practice: State of the art and practical challenges. Jpn. J. Radiol. 2016, 35, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Eisbruch, A. Clinical aspects of IMRT for head-and-neck cancer. Med. Dosim. 2002, 27, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Ezzell, G.A.; Galvin, J.M.; Low, D.; Palta, J.R.; Rosen, I.; Sharpe, M.B.; Xia, P.; Xiao, Y.; Xing, L.; Yu, C.X. Guidance document on delivery, treatment planning, and clinical implementation of IMRT: Report of the IMRT subcommittee of the AAPM radiation therapy committee. Med. Phys. 2003, 30, 2089–2115. [Google Scholar] [CrossRef]
- Mazzola, R.; Fersino, S.; Ferrera, G.; Targher, G.; Figlia, V.; Triggiani, L.; Pasinetti, N.; Casto, A.L.; Ruggieri, R.; Magrini, S.M.; et al. Stereotactic body radiotherapy for lung oligometastases impacts on systemic treatment-free survival: A cohort study. Int. J. Radiat. Oncol. Biol. Phys. 2018, 127, 121. [Google Scholar] [CrossRef]
- Hansen, E.K.; Bucci, M.K.; Quivey, J.M.; Weinberg, V.; Xia, P. Repeat CT imaging and replanning during the course of IMRT for head-and-neck cancer. Int. J. Radiat. Oncol. 2006, 64, 355–362. [Google Scholar] [CrossRef]
- Ballivy, O.; Parker, W.; Vuong, T.; Shenouda, G.; Patrocinio, H. Impact of Geometric Uncertainties on Dose Distribution During Intensity Modulated Radiotherapy of Head-and-neck Cancer: The Need for a Planning Target Volume and A Planning Organ-at-Risk Volume. Curr. Oncol. 2006, 13, 108–115. [Google Scholar] [CrossRef]
- Wu, Q.; Chi, Y.; Chen, P.Y.; Krauss, D.J.; Yan, D.; Martinez, A. Adaptive Replanning Strategies Accounting for Shrinkage in Head and Neck IMRT. Int. J. Radiat. Oncol. 2009, 75, 924–932. [Google Scholar] [CrossRef]
- Brouwer, C.L.; Steenbakkers, R.J.; Bourhis, J.; Budach, W.; Grau, C.; Grégoire, V.; van Herk, M.; Lee, A.; Maingon, P.; Nutting, C.; et al. CT-based delineation of organs at risk in the head and neck region: Dahanca, eortc, gortec, hknpcsg, ncic ctg, ncri, nrg Oncology and trog consensus guidelines. Radiother. Oncol. 2015, 117, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Christianen, M.E.; Langendijk, J.A.; Westerlaan, H.E.; van de Water, T.A.; Bijl, H.P. Delineation of organs at risk involved in swallowing for radiotherapy treatment planning. Radiother. Oncol. 2011, 101, 394–402. [Google Scholar] [CrossRef]
- Tukey, J.W. Exploratory Data Analysis; Addison-Wesley: Reading, MA, USA, 1977. [Google Scholar]
- Schwartz, D.L.; Garden, A.S.; Thomas, J.; Chen, Y.; Zhang, Y.; Lewin, J.; Chambers, M.S.; Dong, L. Adaptive Radiotherapy for Head-and-Neck Cancer: Initial Clinical Outcomes from a Prospective Trial. Int. J. Radiat. Oncol. 2012, 83, 986–993. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.; Langen, K.M.; Lu, W.; Haimerl, J.; Schnarr, E.; Ruchala, K.J.; Olivera, G.H.; Meeks, S.L.; Kupelian, P.A.; Shellenberger, T.D.; et al. Assessment of Parotid Gland Dose Changes During Head and Neck Cancer Radiotherapy Using Daily Megavoltage Computed Tomography and Deformable Image Registration. Int. J. Radiat. Oncol. 2008, 71, 1563–1571. [Google Scholar] [CrossRef]
- Han, C.; Chen, Y.-J.; Liu, A.; Schultheiss, T.E.; Wong, J.Y. Actual Dose Variation of Parotid Glands and Spinal Cord for Nasopharyngeal Cancer Patients During Radiotherapy. Int. J. Radiat. Oncol. 2008, 70, 1256–1262. [Google Scholar] [CrossRef]
- Lin, A.; Kim, H.M.; Terrell, J.E.; Dawson, L.A.; Ship, J.A.; Eisbruch, A. Quality of life after parotid-sparing IMRT for head-and-neck cancer: A prospective longitudinal study. Int. J. Radiat. Oncol. 2003, 57, 61–70. [Google Scholar] [CrossRef]
- Nutting, C.M.; Morden, J.P.; Harrington, K.J.; Urbano, T.G.; Bhide, S.A.; Clark, C.; Miles, E.A.; Miah, A.B.; Newbold, K.; Tanay, M.; et al. Parotid-sparing intensity modulated versus conventional radiotherapy in head and neck cancer (parsport): A phase 3 multicentre randomised controlled trial. Lancet Oncol. 2011, 12, 127–136. [Google Scholar] [CrossRef] [Green Version]
- Lin, A.; Helgeson, E.S.; Treister, N.S.; Schmidt, B.L.; Patton, L.L.; Elting, L.S.; Lalla, R.V.; Brennan, M.T.; Sollecito, T.P. The impact of head and neck radiotherapy on salivary flow and quality of life: Results of the orarad study. Oral Oncol. 2022, 127, 105783. [Google Scholar] [CrossRef]
- Ahn, P.H.; Chen, C.-C.; Ahn, A.I.; Hong, L.; Scripes, P.G.; Shen, J.; Lee, C.-C.; Miller, E.; Kalnicki, S.; Garg, M.K. Adaptive Planning in Intensity-Modulated Radiation Therapy for Head and Neck Cancers: Single-Institution Experience and Clinical Implications. Int. J. Radiat. Oncol. 2011, 80, 677–685. [Google Scholar] [CrossRef]
- Beltran, M.; Ramos, M.; Rovira, J.J.; Pérez-Hoyos, S.; Sancho, M.; Puertas, E.; Benavente, S.; Ginjaume, M.; Giralt, J. Dose variations in tumor volumes and organs at risk during IMRT for head-and-neck cancer. J. Appl. Clin. Med. Phys. 2012, 13, 101–111. [Google Scholar] [CrossRef] [Green Version]
- Berwouts, D.; Olteanu, L.A.M.; Duprez, F.; Vercauteren, T.; De Gersem, W.; De Neve, W.; Van de Wiele, C.; Madani, I. Three-phase adaptive dose-painting-by-numbers for head-and-neck cancer: Initial results of the phase I clinical trial. Radiother. Oncol. 2013, 107, 310–316. [Google Scholar] [CrossRef]
- Hunter, K.U.; Fernandes, L.L.; Vineberg, K.A.; McShan, D.; Antonuk, A.E.; Cornwall, C.; Feng, M.; Schipper, M.J.; Balter, J.M.; Eisbruch, A. Parotid Glands Dose–Effect Relationships Based on Their Actually Delivered Doses: Implications for Adaptive Replanning in Radiation Therapy of Head-and-Neck Cancer. Int. J. Radiat. Oncol. 2013, 87, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Nishi, T.; Nishimura, Y.; Shibata, T.; Tamura, M.; Nishigaito, N.; Okumura, M. Volume and dosimetric changes and initial clinical experience of a two-step adaptive intensity modulated radiation therapy (IMRT) scheme for head and neck cancer. Radiother. Oncol. 2013, 106, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Castelli, J.; Simon, A.; Louvel, G.; Henry, O.; Chajon, E.; Nassef, M.; Haigron, P.; Cazoulat, G.; Ospina, J.D.; Jegoux, F.; et al. Impact of head and neck cancer adaptive radiotherapy to spare the parotid glands and decrease the risk of xerostomia. Radiat. Oncol. 2015, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.D.; Nill, S.; Huber, P.E.; Bendl, R.; Debus, J.; Münter, M.W. A Clinical Concept for Interfractional Adaptive Radiation Therapy in the Treatment of Head and Neck Cancer. Int. J. Radiat. Oncol. 2012, 82, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Duma, M.; Kampfer, S.; Schuster, T.; Winkler, C.; Geinitz, H. Adaptive radiotherapy for soft tissue changes during helical tomotherapy for head and neck cancer. Strahlenther. Und. Onkol. 2012, 188, 243–247. [Google Scholar] [CrossRef]
- Capelle, L.; Mackenzie, M.; Field, C.; Parliament, M.; Ghosh, S.; Scrimger, R. Adaptive Radiotherapy Using Helical Tomotherapy for Head and Neck Cancer in Definitive and Postoperative Settings: Initial Results. Clin. Oncol. 2012, 24, 208–215. [Google Scholar] [CrossRef]
- Dewan, A.; Sharma, S.; Dewan, A.; Srivastava, H.; Rawat, S.; Kakria, A.; Mishra, M.; Suresh, T.; Mehrotra, K. Impact of Adaptive Radiotherapy on Locally Advanced Head and Neck Cancer-A Dosimetric and Volumetric Study. Asian Pac. J. Cancer Prev. 2016, 17, 985–992. [Google Scholar] [CrossRef] [Green Version]
- Olteanu, L.A.M.; Berwouts, D.; Madani, I.; De Gersem, W.; Vercauteren, T.; Duprez, F.; De Neve, W. Comparative dosimetry of three-phase adaptive and non-adaptive dose-painting IMRT for head-and-neck cancer. Radiother. Oncol. 2014, 111, 348–353. [Google Scholar] [CrossRef]
- Zhao, L.; Wan, Q.; Zhou, Y.; Deng, X.; Xie, C.; Wu, S. The role of replanning in fractionated intensity modulated radiotherapy for nasopharyngeal carcinoma. Radiother. Oncol. 2011, 98, 23–27. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Organs at Risk | Dose-Volume Histogram Metric | Constraint |
|---|---|---|
| Spinal cord | D2% | <40–45 Gy |
| Parotid glands | V45Gy V30Gy V15Gy Dmean | <24% <45% <67% <26 Gy |
| Oral cavity | V40Gy | <35% |
| Larynx (whole organ) | V40Gy Dmean | <50% <35 Gy |
| N. (%) | |
|---|---|
| Age at Diagnosis, Median (Range) | 69 years (39–95) |
| Sex Male Female | 36 (64%) 20 (36%) |
| ECOG Performance status 0 1 | 15 (27%) 41 (73%) |
| Smoking Yes Ex-smoker No | 22 (39%) 5 (9%) 29 (52%) |
| Primary tumor site Oral cavity Larynx Nasopharynx Oropharynx Hypopharynx Salivary glands Thyroid Paranasal sinus Unknown primary | 14 (25%) 8 (14%) 2 (4%) 17 (30%) 5 (9%) 6 (11%) 2 (4%) 1 (2%) 1 (2%) |
| Histology Squamous cell carcinoma Other histologies | 44 (79%) 12 (21%) |
| Radiotherapy aim Radical radiotherapy Adjuvant radiotherapy | 35 (62.5%) 21 (37.5%) |
| Concomitant systemic therapy Yes No | 36 (%) 20 (35%) |
| Organs at Risk | DVH Metric | S * | Median (P25–P75) | Difference with S1 * | % | p ** |
|---|---|---|---|---|---|---|
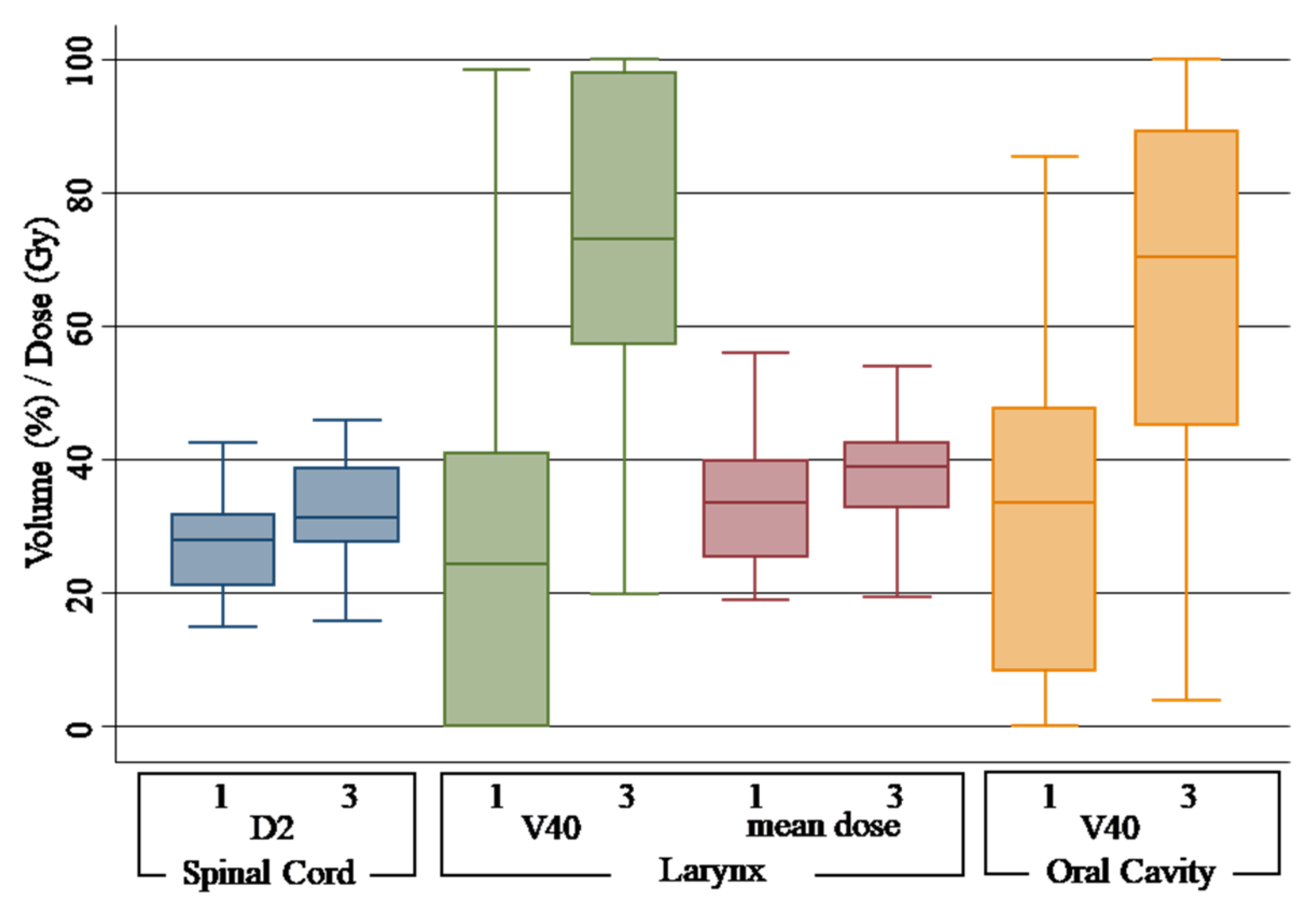
| Spinal cord | D2% | 1 | 27.91 Gy (21.06–31.76) | |||
| 2 | 26.48 Gy (22.10–32.51) | −1.43 Gy | −5.12% | 0.66 | ||
| 3 | 31.39 Gy (27.66–38.79) | 3.48 Gy | 12.46% | 0.00 | ||
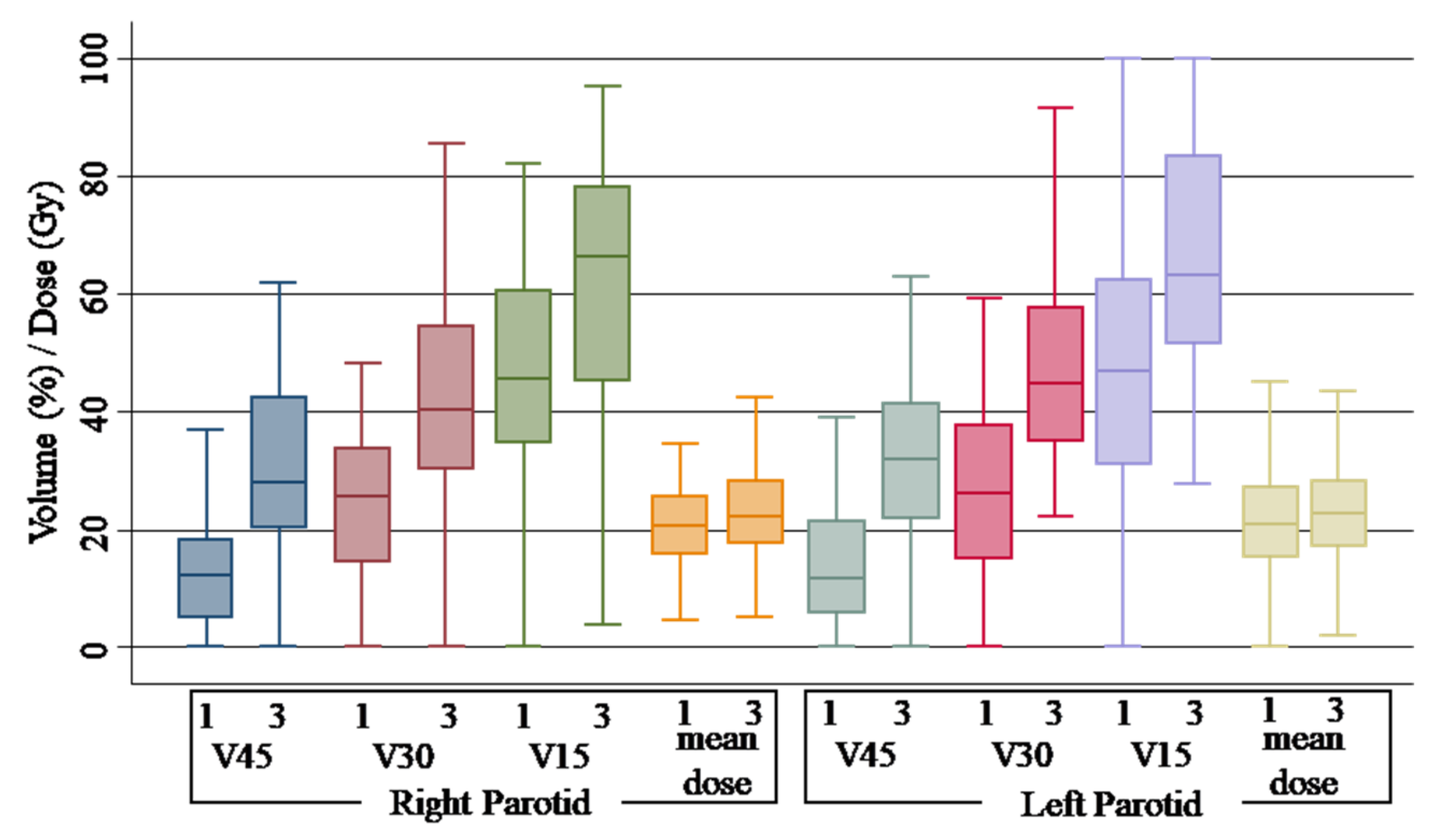
| Parotid right | Dmean | 1 | 20.54 Gy (15.86–25.52) | |||
| 2 | 20.82 Gy (17.56–25.67) | 0.28 Gy | 1.36% | 0.68 | ||
| 3 | 22.14 Gy (17.80–28.20) | 1.6 Gy | 7.78% | 0.30 | ||
| V15Gy | 1 | 45.70% (34.70–60.60) | ||||
| 2 | 47.50% (36.30–57.15) | 1.8% | 3.93% | 0.74 | ||
| 3 | 66.30% (45.10–78.10) | 20.6% | 45.07% | 0.00 | ||
| V30Gy | 1 | 25.50% (14.70–33.90) | ||||
| 2 | 26.20% (17.30–34.00) | 1.2% | 4.70% | 0.84 | ||
| 3 | 40.28% (30.30–54.60) | 14.78% | 57.96% | 0.00 | ||
| V45Gy | 1 | 12.40% (05.00–18.30) | ||||
| 2 | 14.80% (06.70–19.90) | 2.4% | 19.35% | 0.63 | ||
| 3 | 27.95% (20.20–42.40) | 15.55% | 124.40% | 0.00 | ||
| Parotid left | Dmean | 1 | 20.80 Gy (15.25–27.24) | |||
| 2 | 20.68 Gy (14.73–26.00) | −0.12 Gy% | −0.57% | 0.84 | ||
| 3 | 22.77 Gy (17.22–28.29) | 1.97 Gy% | 9.47% | 0.26 | ||
| V15Gy | 1 | 47.00% (30.90–62.40) | ||||
| 2 | 45.60% (34.40–58.30) | −1.4% | −2.97% | 0.51 | ||
| 3 | 63.25% (51.60–83.30) | 16.25% | 34.57% | 0.00 | ||
| V30Gy | 1 | 26.10% (15.20–37.70) | ||||
| 2 | 27.90% (14.90–36.30) | 1.8% | 6.89% | 0.93 | ||
| 3 | 44.80% (34.90–57.70) | 18.7% | 71.64% | 0.00 | ||
| V45Gy | 1 | 11.70% (05.70–21.40) | ||||
| 2 | 12.60% (05.50–22.90) | 0.9% | 7.69% | 0.88 | ||
| 3 | 31.89% (22.00–41.40) | 20.19% | 172.56% | 0.00 | ||
| Larynx | Dmean | 1 | 33.47 Gy (25.33–39.81) | |||
| 2 | 33.96 Gy (27.24–42.49) | 0.49 Gy | 1.46% | 0.56 | ||
| 3 | 39.00 Gy (32.85–42.50) | 5.53 Gy | 16.04% | 0.02 | ||
| V40Gy | 1 | 24.30% (00.00–40.84) | ||||
| 2 | 27.60% (00.00–51.50) | 3.3% | 13.58% | 0.41 | ||
| 3 | 72.95% (57.25–98.05) | 48.65% | 200.20% | 0.00 | ||
| Oral cavity | V40Gy | 1 | 33.45% (08.45–47.70) | |||
| 2 | 37.05% (14.50–52.65) | 3.6% | 10.76% | 0.53 | ||
| 3 | 70.40% (45.10–89.20) | 36.95% | 110.46% | 0.00 |
| Organs at Risk | DVH Metric | S1 * % | S2 * % | S3 * % | p ** |
|---|---|---|---|---|---|
| Spinal cord | D2% | 00.00 | 00.00 | 06.25 | 0.060 |
| Parotids, either left or right | Dmean | 42.11 | 44.64 | 53.06 | 0.260 |
| V45Gy | 31.58 | 35.09 | 87.76 | 0.000 | |
| V30Gy | 21.05 | 15.79 | 69.39 | 0.001 | |
| V15Gy | 24.56 | 21.05 | 55.10 | 0.001 | |
| Larynx | V40Gy | 12.96 | 25.45 | 80.56 | 0.000 |
| Dmean | 43.75 | 46.94 | 69.44 | 0.019 | |
| Oral cavity | V40Gy | 46.43 | 51.79 | 77.55 | 0.001 |
| Primary Tumor. Target | DVH Metric | S * | Median (P25–P75) % | Difference with S1 * | % | p ** |
|---|---|---|---|---|---|---|
| Planning target volume (PTV) | V95% | 1 | 98.72 (97.96–99.34) | |||
| 2 | 98.64 (97.25–99.37) | −0.08 | −0.08% | 0.35 | ||
| 3 | 94.70 (87.10–97.60) | −4.02 | −4.07% | 0.00 | ||
| Clinical target volume (CTV) | V95% | 1 | 99.96 (99.77–99.99) | |||
| 2 | 99.91 (99.31–99.99) | −0.05 | −0.05 | 0.30 | ||
| 3 | 97.90 (92.33–99.58) | −2.06 | −2.06 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franzese, C.; Tomatis, S.; Bianchi, S.P.; Pelizzoli, M.; Teriaca, M.A.; Badalamenti, M.; Comito, T.; Clerici, E.; Franceschini, D.; Navarria, P.; et al. Adaptive Volumetric-Modulated Arc Radiation Therapy for Head and Neck Cancer: Evaluation of Benefit on Target Coverage and Sparing of Organs at Risk. Curr. Oncol. 2023, 30, 3344-3354. https://doi.org/10.3390/curroncol30030254
Franzese C, Tomatis S, Bianchi SP, Pelizzoli M, Teriaca MA, Badalamenti M, Comito T, Clerici E, Franceschini D, Navarria P, et al. Adaptive Volumetric-Modulated Arc Radiation Therapy for Head and Neck Cancer: Evaluation of Benefit on Target Coverage and Sparing of Organs at Risk. Current Oncology. 2023; 30(3):3344-3354. https://doi.org/10.3390/curroncol30030254
Chicago/Turabian StyleFranzese, Ciro, Stefano Tomatis, Sofia Paola Bianchi, Marco Pelizzoli, Maria Ausilia Teriaca, Marco Badalamenti, Tiziana Comito, Elena Clerici, Davide Franceschini, Pierina Navarria, and et al. 2023. "Adaptive Volumetric-Modulated Arc Radiation Therapy for Head and Neck Cancer: Evaluation of Benefit on Target Coverage and Sparing of Organs at Risk" Current Oncology 30, no. 3: 3344-3354. https://doi.org/10.3390/curroncol30030254