Soft Tissue Masses of the Hand: A Review of Clinical Presentation and Imaging Features

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Benign Masses
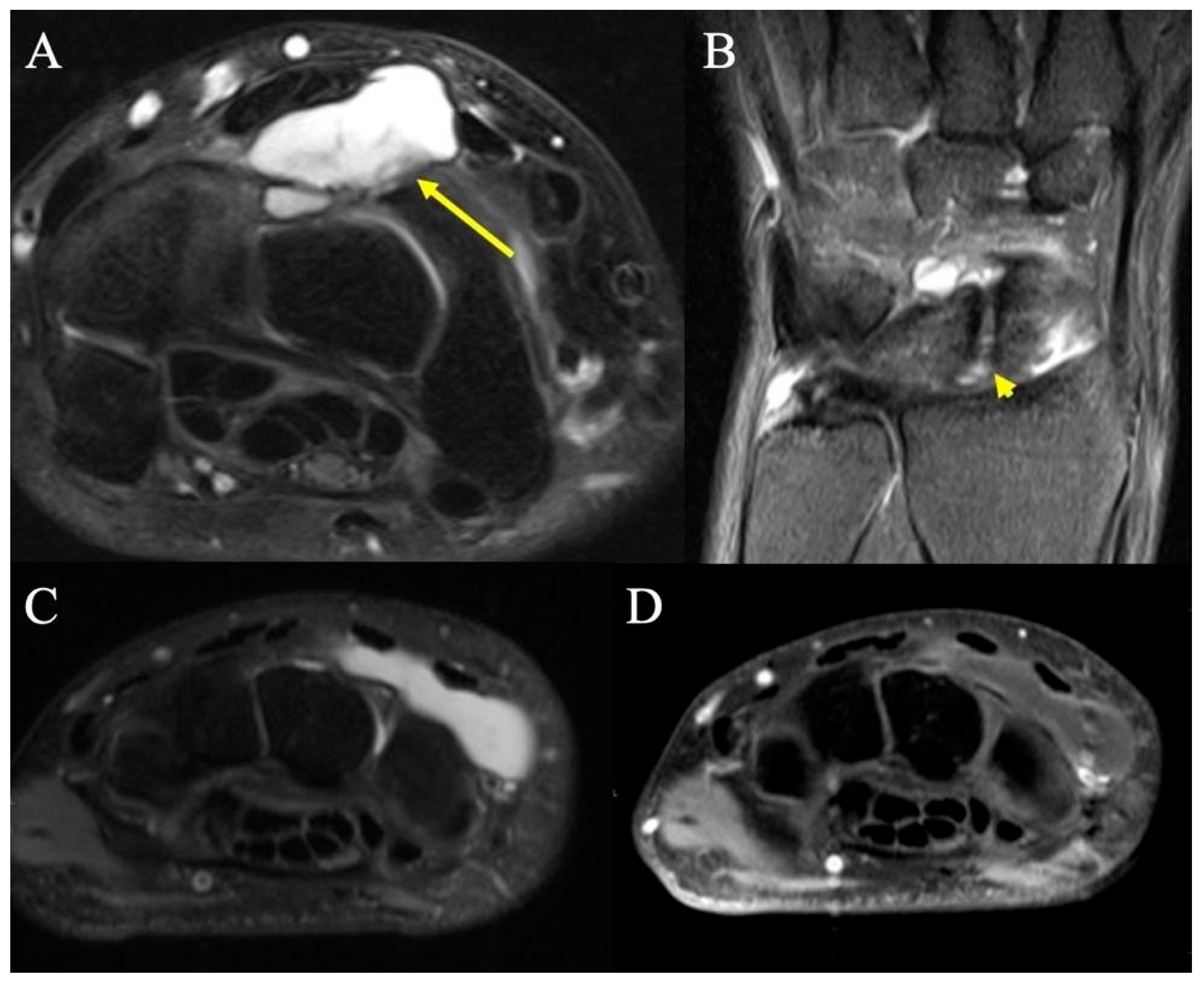
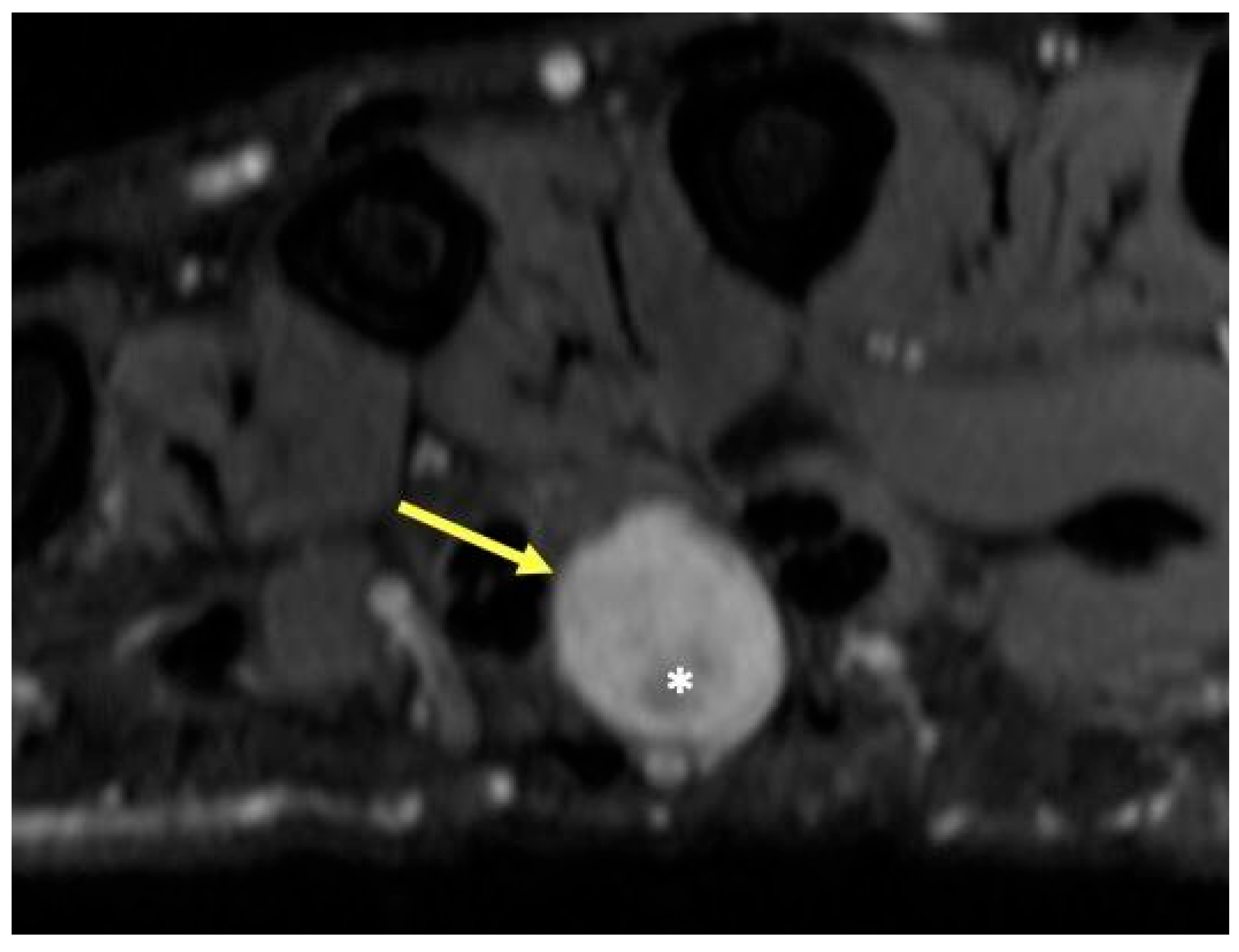
2.1. Ganglion Cysts
2.1.1. Clinical Features
2.1.2. Imaging Appearance
2.2. Tenosynovial Giant Cell Tumors
2.2.1. Clinical Features
2.2.2. Imaging Appearance
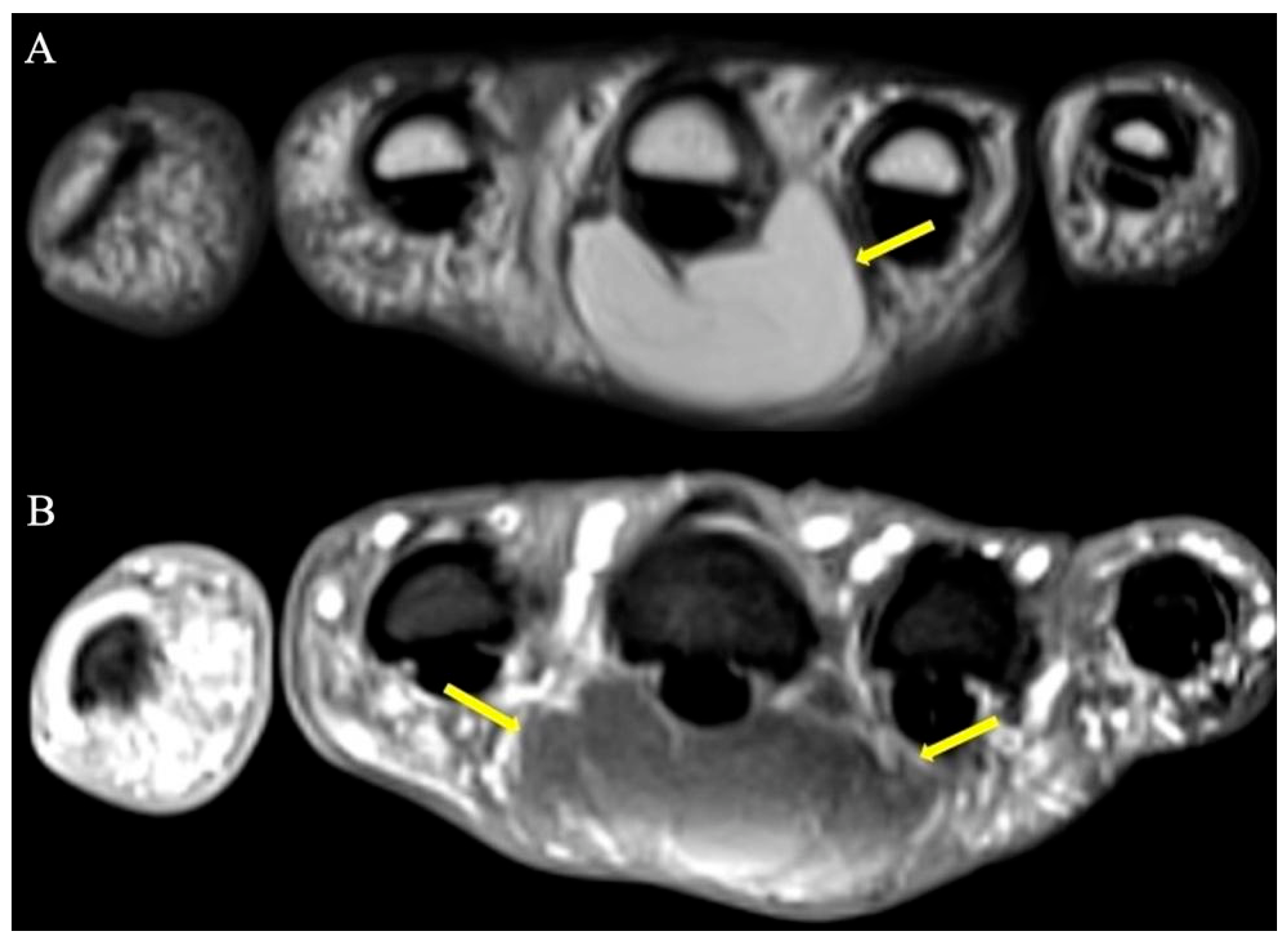
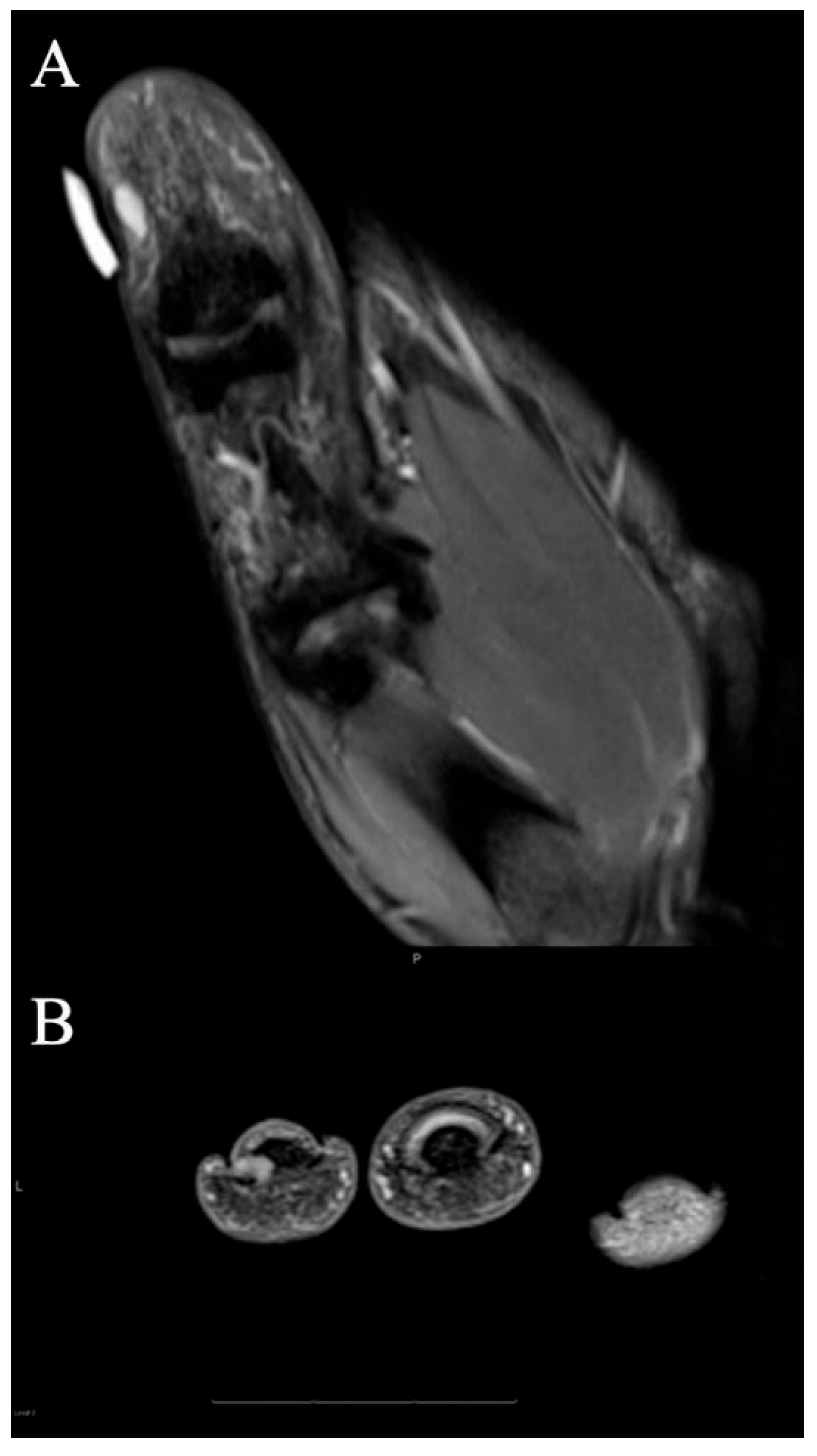
2.3. Lipoma
2.3.1. Clinical Features
2.3.2. Radiographic Appearance
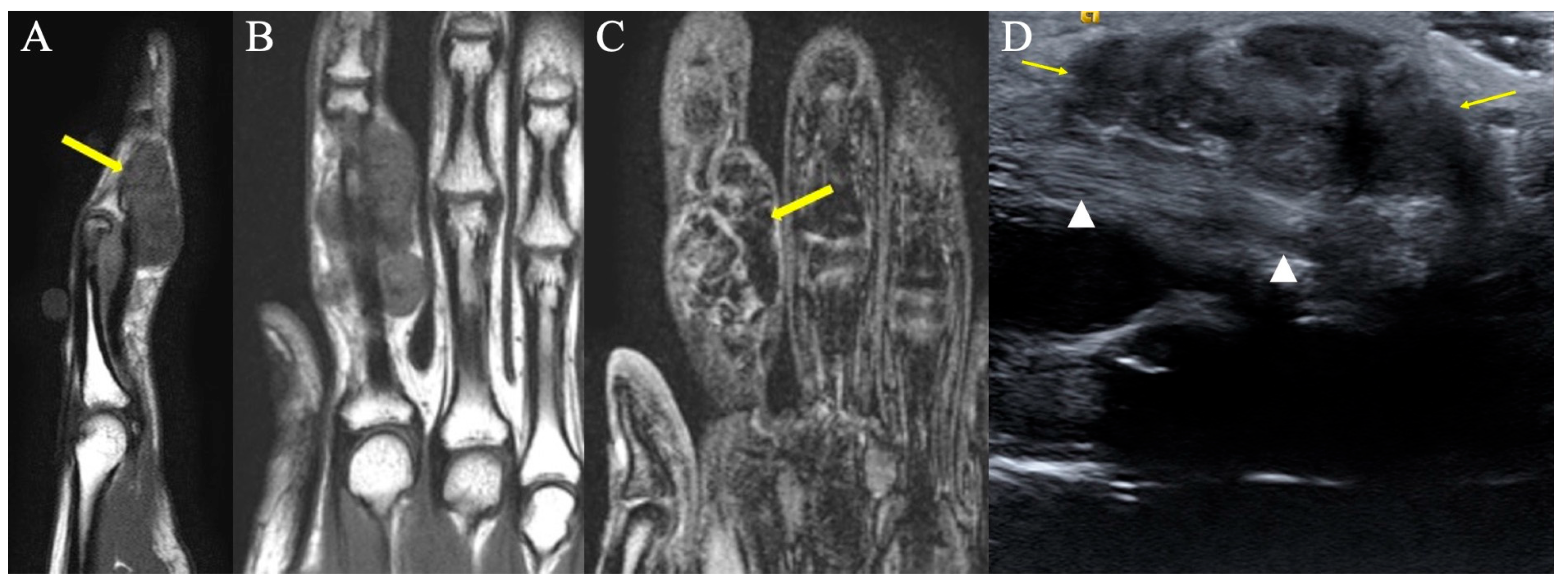
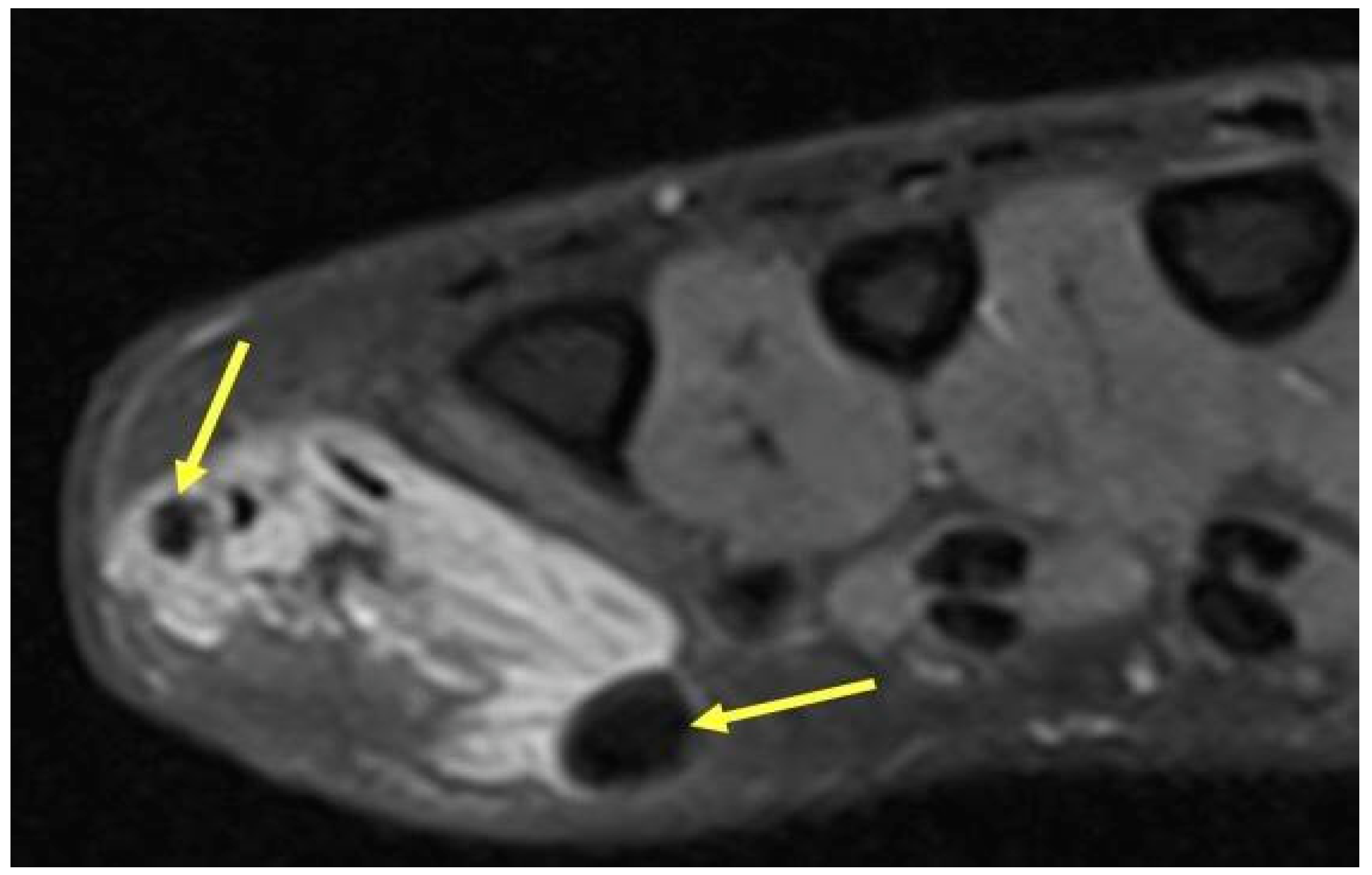
2.4. Schwannoma
2.4.1. Clinical Features
2.4.2. Radiographic Appearance
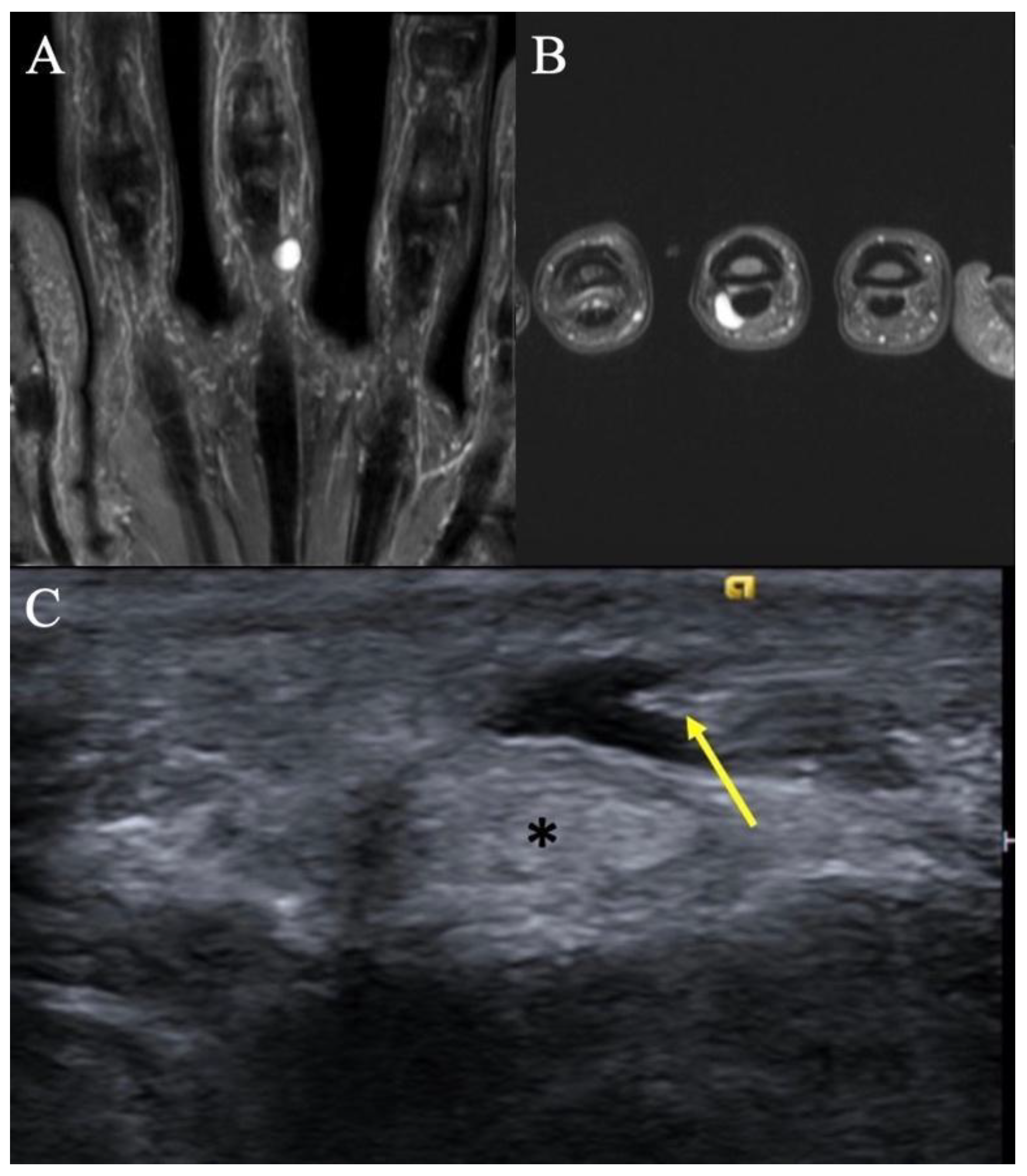
2.5. Glomus Tumors
2.5.1. Clinical Features
2.5.2. Imaging Appearance
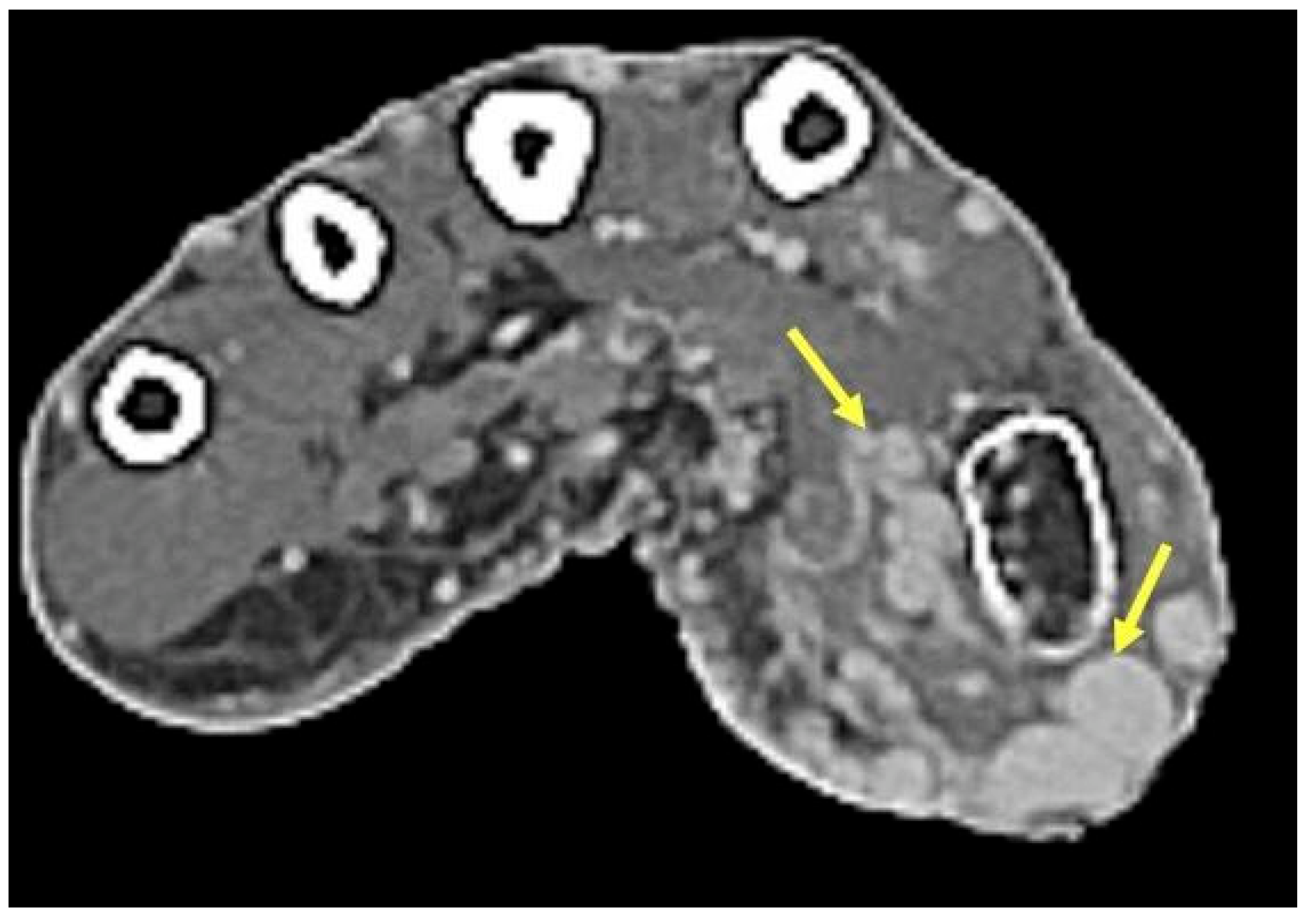
2.6. Vascular Tumors and Malformations
2.6.1. Clinical Features
2.6.2. Imaging Appearance
2.7. Superficial Fibromatoses
2.7.1. Clinical Features
2.7.2. Imaging Appearance
2.8. Synovial Chondromatosis
2.8.1. Clinical Features
2.8.2. Imaging Appearance
2.9. Infectious Tenosynovitis
2.9.1. Clinical Features
2.9.2. Imaging Appearance
2.10. Foreign Bodies of the Hand
2.10.1. Clinical Features
2.10.2. Imaging Appearance
3. Soft-Tissue Malignancies
3.1. Clinical Features
3.2. Surgical Considerations
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Nepal, P.; Songmen, S.; Alam, S.I.; Gandhi, D.; Ghimire, N.; Ojili, V. Common Soft Tissue Tumors Involving the Hand with Histopathological Correlation. J. Clin. Imaging Sci. 2019, 9, 1–10. [Google Scholar] [CrossRef]
- Mavrogenis, A.F.; Panagopoulos, G.N.; Angelini, A.; Lesenský, J.; Vottis, C.; Megaloikonomos, P.D.; Kokkalis, Z.; Kontogeorgakos, V.; Ruggieri, P.; Papagelopoulos, P.; et al. Tumors of the hand. Eur. J. Orthop. Surg. Traumatol. 2017, 27, 747–762. [Google Scholar] [CrossRef] [PubMed]
- Angelides, A.C. Ganglions of the hand and wrist. In Operative Hand Surgery, 3rd ed.; Green, D.P., Ed.; Churchill Livingstone: New York, NY, USA, 1993; pp. 2171–2183. [Google Scholar]
- Barnes, W.E.; Larsen, R.D.; Posch, J.L. Review of ganglia of the hand and wrist with analysis of surgical treatment. Plast Reconstr. Surg. 1964, 34, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Soren, A. Pathogenesis and treatment of ganglion. Clin. Orthop. Relat. Res. 1966, 48, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Minotti, P.; Taras, J.S. Ganglion cysts of the wrist. J. Hand Surg. Am. 2002, 2, 102–107. [Google Scholar] [CrossRef]
- Jebson, P.J.L.; Spencer, E.E. Flexor tendon sheath ganglions: Results of surgical excision. Hand 2007, 2, 94–100. [Google Scholar] [CrossRef]
- Chang, Y.-M.; Chan, C.-P.; King Wu, S.-F.; Hao, S.-P.; Chang, L.C. Ganglion cyst and synovial cyst of the temporomandibular joint. Int. J. Oral. Maxillofac. Surg. 1997, 26, 179–181. [Google Scholar] [CrossRef]
- Gude, W.; Morelli, V. Ganglion cysts of the wrist: Pathophysiology, clinical picture, and management. Curr. Rev. Musculoskelet Med. 2008, 1, 205–211. [Google Scholar] [CrossRef]
- Kurkis, G.; Anastasio, A.; DeVos, M.; Gottschalk, M. Ultrasound-Guided Aspiration Does Not Reduce the Recurrence Rate of Ganglion Cysts of the Wrist. J. Wrist Surg. 2019, 08, 100–103. [Google Scholar] [CrossRef]
- Gitto, S.; Lee, S.C.; Miller, T.T. Ultrasound-guided percutaneous treatment of volar radiocarpal ganglion cysts: Safety and efficacy. J. Clin. Ultrasound 2019, 47, 339–344. [Google Scholar] [CrossRef]
- Suen, M.; Fung, B.; Lung, C.P. Treatment of Ganglion Cysts. ISRN Orthop 2013, 2013, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Varley, G.W.; Needoff, M.; Davis, T.R.C.; Clay, N.R. Conservative Management of Wrist Ganglia. J. Hand Surg. Am. 1997, 22, 636–637. [Google Scholar] [CrossRef] [PubMed]
- Ehrenstein, V.; Andersen, S.L.; Qazi, I.; Sankar, N.; Pedersen, A.B.; Sikorski, R.; Acquavella, J. Tenosynovial Giant Cell Tumor: Incidence, Prevalence, Patient Characteristics, and Recurrence. A Registry-based Cohort Study in Denmark. J. Rheumatol. 2017, 44, 1476–1483. [Google Scholar] [CrossRef]
- Reilly, K.E.; Stern, P.J.; Dale, J.A. Recurrent giant cell tumors of the tendon sheath. J. Hand Surg. Am. 1999, 24, 1298–1302. [Google Scholar] [CrossRef] [PubMed]
- Gouin, F.; Noailles, T. Localized and diffuse forms of tenosynovial giant cell tumor (formerly giant cell tumor of the tendon sheath and pigmented villonodular synovitis). Orthop. Traumatol. Surg. Res. 2017, 103, S91–S97. [Google Scholar] [CrossRef]
- Ho, J.; Peters, T.; Dickson, B.C.; Swanson, D.; Fernandez, A.; Frova-Seguin, A.; Valentin, M.-A.; Schramm, U.; Sultan, M.; Nielsen, T.; et al. Detection of CSF1 rearrangements deleting the 3′ UTR in tenosynovial giant cell tumors. Genes Chromosomes Cancer 2020, 59, 96–105. [Google Scholar] [CrossRef]
- Tap, W.; Wainberg, Z.; Anthony, S.; Ibrahim, P.; Zhang, C.; Healey, J.; Chmielowski, B.; Staddon, A.; Cohn, A.L.; Shapiro, G.; et al. Structure-Guided Blockade of CSF1R Kinase in Tenosynovial Giant-Cell Tumor. N. Engl. J. Med. 2015, 373, 428–437. [Google Scholar] [CrossRef]
- Wang, C.; Song, R.-R.; Kuang, P.-D.; Wang, L.-H.; Zhang, M.-M. Giant cell tumor of the tendon sheath: Magnetic resonance imaging findings in 38 patients. Oncol. Lett. 2017, 13, 4459–4462. [Google Scholar] [CrossRef]
- Bogumill, G.P.; Sullivan, D.J.; Baker, G.I. Tumors of the hand. Clin. Orthop. Relat. Res. 1975, 108, 214–222. [Google Scholar] [CrossRef]
- Nadar, M.M.; Bartoli, C.R.; Kasdan, M.L. Lipomas of the hand: A review and 13 patient case series. Eplasty 2010, 10, e66. [Google Scholar]
- Sandberg, A.A. Updates on the cytogenetics and molecular genetics of bone and soft tissue tumors: Lipoma. Cancer Genet. Cytogenet. 2004, 150, 93–115. [Google Scholar] [CrossRef] [PubMed]
- Beird, H.C.; Wu, C.-C.; Ingram, D.R.; Wang, W.-L.; Alimohamed, A.; Gumbs, C.; Little, L.; Song, X.; Feig, B.; Roland, C.; et al. Genomic profiling of dedifferentiated liposarcoma compared to matched well-differentiated liposarcoma reveals higher genomic complexity and a common origin. Mol. Case Stud. 2018, 4, a002386. [Google Scholar] [CrossRef] [PubMed]
- Paunipagar, B.K.; Griffith, J.F.; Rasalkar, D.D.; Chow, L.T.C.; Kumta, S.M.; Ahuja, A. Ultrasound features of deep-seated lipomas. Insights Imaging 2010, 1, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Zhou, H.-Y.; Jiang, S.; Ma, F.-X.; Lu, H. Peripheral nerve tumors of the hand: Clinical features, diagnosis, and treatment. World J. Clin. Cases 2020, 8, 5086–5098. [Google Scholar] [CrossRef] [PubMed]
- Funata, N. Tumors(4), Pathology of tumours of the peripheral nerves, pituitary gland and benign epithelial cysts. No. 12 in series of articles: Basic knowledge of neuropathology for neurosurgeons. No. Shinkei. Geka. 2003, 31, 683–690. [Google Scholar] [PubMed]
- Becher Carstens, P.H.; Schrodt, G.R. Malignant Transformation of a Benign Encapsulated Neurilemoma. Am. J. Clin. Pathol. 1969, 51, 144–149. [Google Scholar] [CrossRef]
- Ahlawat, S.; Fayad, L.M. Imaging cellularity in benign and malignant peripheral nerve sheath tumors: Utility of the “target sign” by diffusion weighted imaging. Eur. J. Radiol. 2018, 102, 195–201. [Google Scholar] [CrossRef]
- Pan, W.; Wang, Z.; Lin, N.; Huang, X.; Liu, M.; Yan, X.; Ye, Z. Clinical features and surgical treatment of sacral schwannomas. Oncotarget 2017, 8, 38061–38068. [Google Scholar] [CrossRef]
- Carroll, R.E.; Berman, A.T. Glomus tumors of the hand: Review of the literature and report on twenty-eight cases. J. Bone Joint Surg. Am. 1972, 54, 691–703. [Google Scholar] [CrossRef] [PubMed]
- Karamzadeh Dashti, N.; Bahrami, A.; Lee, S.J.; Jenkins, S.M.; Rodriguez, F.J.; Folpe, A.L.; Boland, J. BRAF V600E Mutations Occur in a Subset of Glomus Tumors, and Are Associated With Malignant Histologic Characteristics. Am. J. Surg. Pathol. 2017, 41, 1532–1541. [Google Scholar] [CrossRef]
- Agaram, N.P.; Zhang, L.; Jungbluth, A.A.; Dickson, B.C.; Antonescu, C.R. A Molecular Reappraisal of Glomus Tumors and Related Pericytic Neoplasms With Emphasis on NOTCH-gene Fusions. Am. J. Surg. Pathol. 2020, 44, 1556–1562. [Google Scholar] [CrossRef] [PubMed]
- Macharia, C.; Nthumba, P.M. Glomus tumor presenting as complex regional pain syndrome of the left upper limb: A case report. J. Med. Case Rep. 2015, 9, 293. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H. Glomus tumor of the finger tip and MRI appearance. Iowa Orthop J. 1999, 19, 136–138. [Google Scholar]
- Rodrigues, J.N.; Becker, G.W.; Ball, C.; Zhang, W.; Giele, H.; Hobby, J.; Pratt, A.; Davis, T. Surgery for Dupuytren’s contracture of the fingers. Cochrane Database Syst. Rev. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Becker, K.; Siegert, S.; Toliat, M.R.; Du, J.; Casper, R.; Dolmans, G.H.; Werker, P.M.; Tinschert, S.; Franke, A.; Gieger, C.; et al. German Dupuytren Study Group. Meta-Analysis of Genome-Wide Association Studies and Network Analysis-Based Integration with Gene Expression Data Identify New Suggestive Loci and Unravel a Wnt-Centric Network Associated with Dupuytren's Disease. PLoS ONE 2016, 11, e0158101. [Google Scholar] [CrossRef]
- Teh, J. Ultrasound of soft tissue masses of the hand. J. Ultrason 2012, 12, 381–401. [Google Scholar] [CrossRef]
- Cox, J.; Bartlett, E.; Lee, E. Vascular Malformations: A Review. Semin Plast Surg. 2014, 28, 058–063. [Google Scholar] [CrossRef]
- Masand, P. Radiographic Findings Associated with Vascular Anomalies. Semin Plast Surg. 2014, 28, 069–078. [Google Scholar] [CrossRef]
- Stewart, B.D.; Nascimento, A.F. Palmar and plantar fibromatosis: A review. J. Pathol. Transl. Med. 2021, 55, 265–270. [Google Scholar] [CrossRef]
- Grazina, R.; Teixeira, S.; Ramos, R.; Sousa, H.; Ferreira, A.; Lemos, R. Dupuytren’s disease: Where do we stand? EFORT Open Rev. 2019, 4, 63–69. [Google Scholar] [CrossRef]
- Walker, E.A.; Petscavage, J.M.; Brian, P.L.; Logie, C.I.; Montini, K.M.; Murphey, M.D. Imaging features of superficial and deep fibromatoses in the adult population. Sarcoma 2012, 2012, 215810. [Google Scholar] [CrossRef] [PubMed]
- Ramachandran, A.; Fox, T.; Wolfson, A.; Banks, J.; Subhawong, T.K. Superficial fibromatosis: MRI radiomics and T2 mapping correlate with treatment response. Magn Reson. Imaging 2021, 81, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Murphey, M.D.; Vidal, J.A.; Fanburg-Smith, J.C.; Gajewski, D.A. Imaging of Synovial Chondromatosis with Radiologic-Pathologic Correlation. RadioGraphics 2007, 27, 1465–1488. [Google Scholar] [CrossRef] [PubMed]
- Amary, F.; Perez-Casanova, L.; Ye, H.; Cottone, L.; Strobl, A.-C.; Cool, P.; Miranda, E.; Berisha, F.; Aston, W.; Rocha, M.; et al. Synovial chondromatosis and soft tissue chondroma: Extraosseous cartilaginous tumor defined by FN1 gene rearrangement. Mod. Pathol. 2019, 32, 1762–1771. [Google Scholar] [CrossRef] [PubMed]
- Spinnato, P.; Patel, D.B.; di Carlo, M.; Bartoloni, A.; Cevolani, L.; Matcuk, G.R.; Crombé, A. Imaging of Musculoskeletal Soft-Tissue Infections in Clinical Practice: A Comprehensive Updated Review. Microorganisms 2022, 10, 2329. [Google Scholar] [CrossRef] [PubMed]
- Altmayer, S.; Verma, N.; Dicks, E.A.; Oliveira, A. Imaging musculoskeletal soft tissue infections. Semin. Ultrasound CT MR 2020, 41, 85–98. [Google Scholar] [CrossRef] [PubMed]
- Spann, M.; Talmor, M.; Nolan, W.B. Hand infections: Basic principles and management. Surg. Infect. 2004, 5, 210–220. [Google Scholar] [CrossRef]
- Saaiq, M. Epidemiology and Management of Foreign Bodies in the Hand: Pakistani Perspective. World J. Plast Surg.. 2014, 3, 13. [Google Scholar]
- Russell, R.C.; Williamson, D.A.; Sullivan, J.W.; Suchy, H.; Suliman, O. Detection of foreign bodies in the hand. J. Hand Surg. Am. 1991, 16, 2–11. [Google Scholar] [CrossRef]
- Duran-Moreno, J.; Kontogeorgakos, V.; Koumarianou, A. Soft tissue sarcomas of the upper extremities: Maximizing treatment opportunities and outcomes (Review). Oncol. Lett. 2019, 18, 2179–2191. [Google Scholar] [CrossRef]
- Mirous, M.P.; Coulet, B.; Chammas, M.; Cupissol, D.; Lazerges, C. Extensive limb-sparing surgery with reconstruction for sarcoma of the hand and wrist. Orthop. Traumatol. Surg. Res. 2016, 102, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, S.; Milner, R.H.; Ragbir, M. Soft Tissue Sarcoma of the Hand and Wrist: Epidemiology and Management Challenges. J. Hand Microsurg. 2018, 10, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Gerrand, C.H.; Wunder, J.S.; Kandel, R.A.; O'Sullivan, B.; Catton, C.N.; Bell, R.S.; Griffin, A.M.; Davis, A.M. Classification of positive margins after resection of soft-tissue sarcoma of the limb predicts the risk of local recurrence. J. Bone Joint Surg. Br. 2001, 83, 1149–1155. [Google Scholar] [CrossRef] [PubMed]
- Puhaindran, M.E.; Rohde, R.S.; Chou, J.; Morris, C.D.; Athanasian, E.A. Clinical outcomes for patients with soft tissue sarcoma of the hand. Cancer 2011, 117, 175–179. [Google Scholar] [CrossRef] [PubMed]















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AbuMoussa, S.; Roshan, M.P.; Souza, F.F.; Daley, D.; Rosenberg, A.; Pretell, J.; Fullerton, N.; Subhawong, T. Soft Tissue Masses of the Hand: A Review of Clinical Presentation and Imaging Features. Curr. Oncol. 2023, 30, 2032-2048. https://doi.org/10.3390/curroncol30020158
AbuMoussa S, Roshan MP, Souza FF, Daley D, Rosenberg A, Pretell J, Fullerton N, Subhawong T. Soft Tissue Masses of the Hand: A Review of Clinical Presentation and Imaging Features. Current Oncology. 2023; 30(2):2032-2048. https://doi.org/10.3390/curroncol30020158
Chicago/Turabian StyleAbuMoussa, Samuel, Mona Pari Roshan, Felipe Ferreira Souza, Dane Daley, Andrew Rosenberg, Juan Pretell, Natalia Fullerton, and Ty Subhawong. 2023. "Soft Tissue Masses of the Hand: A Review of Clinical Presentation and Imaging Features" Current Oncology 30, no. 2: 2032-2048. https://doi.org/10.3390/curroncol30020158