COVID-19 Emotional and Mental Impact on Cancer Patients Receiving Radiotherapy: An Interpretation of Potential Explaining Descriptors

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Measures
2.3. Design-Outcomes
2.4. Statistical Analysis
3. Results
3.1. Survey Participants
3.2. Exposure to COVID-19
3.3. Coping and Support Mechanisms
3.4. Correlation between Scores of the Questionnaire GAD-7, PHQ-9, and WHO-5
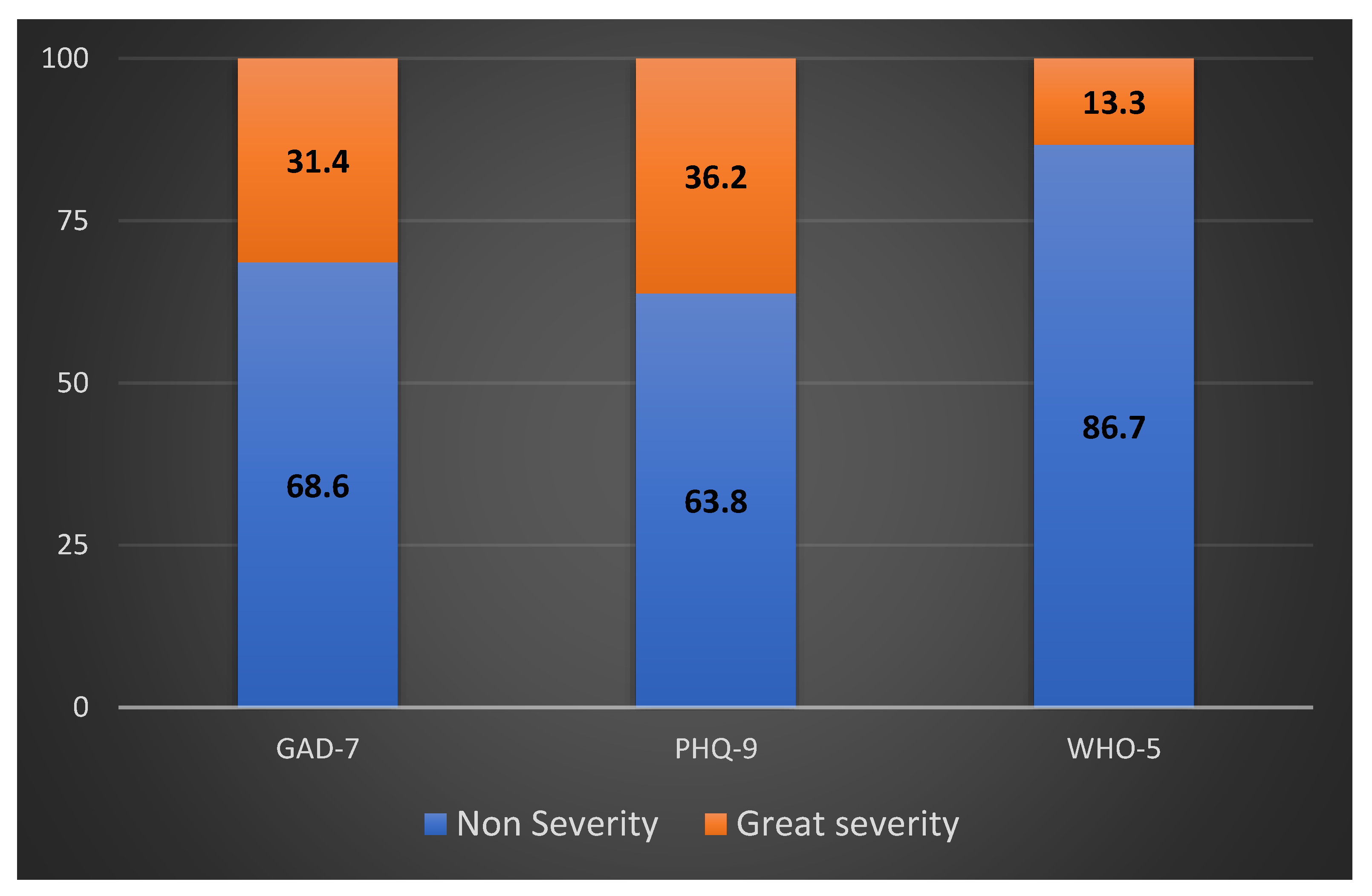
3.5. Assessing the Emotional and Mental Health Impact of COVID-19
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease 2019 (COVID-19): Situation Report. 2019 (NO. 45. World Health Organization, 2020). Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200305-sitrep-45-covid-19.pdf (accessed on 15 July 2022).
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76, Erratum in Int. J. Surg. 2020, 77, 217. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.P.; Natale, G.; Link, B.G. Socioeconomic inequalities in the spread of coronavirus-19 in the United States: A examination of the emergence of social inequalities. Soc. Sci. Med. 2021, 268, 113554. [Google Scholar] [CrossRef]
- Mauri, D.; Tzachanis, D.; Valachis, A.; Kamposioras, K.; Tolia, M.; Dambrosio, M.; Zarkavelis, G.; Gkoura, S.; Gazouli, I.; De Lorenzo, F.; et al. Behind the numbers and the panic of a viral pandemic: Fixed restrictive oncology guidance may jeopardize patients’ survival. J. BUON 2020, 25, 1277–1280. [Google Scholar] [PubMed]
- Symvoulakis, E.K.; Sourvinos, G.; Spandidos, D.A.; Lionis, C. COVID-19 pandemic: Monitoring space-time data and learning from global experience. Exp. Ther. Med. 2020, 20, 73. [Google Scholar] [CrossRef] [PubMed]
- Lima, N.T.; Buss, P.M.; Paes-Sousa, R. COVID-19 pandemic: A health and humanitarian crisis. Cad. De SaúdePública 2020, 36, e00177020, (In English and Portuguese). [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Sharafeldin, N.; Bates, B.; Song, Q.; Madhira, V.; Yan, Y.; Dong, S.; Lee, E.; Kuhrt, N.; Shao, Y.R.; Liu, F.; et al. Outcomes of COVID-19 in Patients With Cancer: Report From the National COVID Cohort Collaborative (N3C). J. Clin. Oncol. 2021, 39, 2232–2246. [Google Scholar] [CrossRef]
- Stefana, A.; Youngstrom, E.A.; Hopwood, C.J.; Dakanalis, A. The COVID-19 pandemic brings a second wave of social isolation and disrupted services. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 785–786. [Google Scholar] [CrossRef]
- Bartmann, C.; Fischer, L.M.; Hübner, T.; Müller-Reiter, M.; Wöckel, A.; McNeill, R.V.; Schlaiss, T.; Kittel-Schneider, S.; Kämmerer, U.; Diessner, J. The effects of the COVID-19 pandemic on psychological stress in breast cancer patients. BMC Cancer 2021, 21, 1356. [Google Scholar] [CrossRef]
- Bao, Y.; Sun, Y.; Meng, S.; Shi, J.; Lu, L. 2019-nCoV epidemic: Address mental health care to empower society. Lancet 2020, 395, e37–e38. [Google Scholar] [CrossRef]
- Eckford, R.D.; Gaisser, A.; Arndt, V.; Baumann, M.; Kludt, E.; Mehlis, K.; Ubels, J.; Winkler, E.C.; Weg-Remers, S.; Schlander, M. The COVID-19 Pandemic and Cancer Patients in Germany: Impact on Treatment, Follow-Up Care and Psychological Burden. Front. Public Health 2022, 9, 788598. [Google Scholar] [CrossRef]
- Marron, J.M.; Joffe, S.; Jagsi, R.; Spence, R.A.; Hlubocky, F.J. Ethics and Resource Scarcity: ASCO Recommendations for the Oncology Community During the COVID-19 Pandemic. J. Clin. Oncol. 2020, 38, 2201–2205. [Google Scholar] [CrossRef]
- März, J.W.; Holm, S.; Schlander, M. Resource allocation in the COVID-19 health crisis: Are COVID-19 preventive measures consistent with the Rule of Rescue? Med. Health Care Philos. 2021, 24, 487–492. [Google Scholar] [CrossRef]
- Hanna, T.P.; King, W.D.; Thibodeau, S.; Jalink, M.; Paulin, G.A.; Harvey-Jones, E.; O’Sullivan, D.E.; Booth, C.M.; Sullivan, R.; Aggarwal, A. Mortality due to cancer treatment delay: Systematic review and meta-analysis. BMJ 2020, 371. [Google Scholar] [CrossRef]
- Mauri, D.; Kamposioras, K.; Tolia, M.; Alongi, F.; Tzachanis, D. International Oncology Panel and European Cancer Patient Coalition collaborators. Summary of international recommendations in 23 languages for patients with cancer during the COVID-19 pandemic. Lancet Oncol. 2020, 21, 759–760. [Google Scholar] [CrossRef]
- Apostolou, K.; Vogli, S.; Frountzas, M.; Syllaios, A.; Tolia, M.; Papanikolaou, I.S.; Schizas, D. Upper Gastrointestinal Cancer Management in the COVID-19 Era: Risk of Infection, Adapted Role of Endoscopy, and Potential Treatment Algorithm Alterations. J. Gastrointest. Cancer 2021, 52, 407–413. [Google Scholar] [CrossRef]
- Kamposioras, K.; Mauri, D.; Papadimitriou, K.; Anthoney, A.; Hindi, N.; Petricevic, B.; Dambrosio, M.; Valachis, A.; Kountourakis, P.; Kopecky, J.; et al. Synthesis of Recommendations From 25 Countries and 31 Oncology Societies: How to Navigate Through COVID-19 Labyrinth. Front. Oncol. 2020, 10, 575148. [Google Scholar] [CrossRef]
- Mauri, D.; Kamposioras, K.; Tsali, L.; Dambrosio, M.; De Bari, B.; Hindi, N.; Salembier, C.; Nixon, J.; Dimitrios, T.; Alongi, F.; et al. COVID-19 Vaccinations: Summary Guidance for Cancer Patients in 28 Languages: Breaking Barriers to Cancer Patient Information. Rev. Recent Clin. Trials 2022, 17, 11–14. [Google Scholar] [CrossRef]
- Mitra, S.; Simson, D.K.; Khurana, H.; Tandon, S.; Ahlawat, P.; Bansal, N.; Barik, S.; Sethi, J.S.; Chufal, K.S.; Gairola, M. Treatment Delay during Radiotherapy of Cancer Patients due to COVID-19 Pandemic. Asian Pac. J. Cancer Prev. 2022, 23, 2415–2420. [Google Scholar] [CrossRef]
- Venkatasai, J.; John, C.; Kondavetti, S.S.; Appasamy, M.; Parasuraman, L.; Ambalathandi, R.; Masilamani, H. Impact of COVID-19 Pandemic on Patterns of Care and Outcome of Head and Neck Cancer: Real-World Experience From a Tertiary Care Cancer Center in India. JCO Glob. Oncol. 2022, 8, e2100339. [Google Scholar] [CrossRef]
- Wang, Q.; Berger, N.A.; Xu, R. Analyses of Risk, Racial Disparity, and Outcomes Among US Patients With Cancer and COVID-19 Infection. JAMA Oncol. 2021, 7, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: A systematic review and meta-analysis of observational studies. Aging Male 2020, 23, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Giannakoulis, V.G.; Papoutsi, E.; Siempos, I.I. Effect of Cancer on Clinical Outcomes of Patients With COVID-19: A Meta-Analysis of Patient Data. JCO Glob. Oncol. 2020, 6, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Lunski, M.J.; Burton, J.; Tawagi, K.; Maslov, D.; Simenson, V.; Barr, D.; Yuan, H.; Johnson, D.; Matrana, M.; Cole, J.; et al. Multivariate mortality analyses in COVID-19, Comparing patients with cancer and patients without cancer in Louisiana. Cancer 2021, 127, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Saini, K.S.; Tagliamento, M.; Lambertini, M.; McNally, R.; Romano, M.; Leone, M.; Curigliano, G.; de Azambuja, E. Mortality in patients with cancer and coronavirus disease2019, A systematic review and pooled analysis of 52 studies. Eur. J. Cancer 2020, 139, 43–50. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, J.; Tu, Y.; Zhou, X.; Huang, H.; Shao, L.; Chen, L.; Zhao, Y.; Ge, M. Cancer patients in SARS-CoV-2 infection: A single-center experience from Wuhan. J. Cancer 2020, 11, 6243–6247. [Google Scholar] [CrossRef]
- Galea, S.; Merchant, R.M.; Lurie, N. The Mental Health Consequences of COVID-19 and Physical Distancing: The Need for Prevention and Early Intervention. JAMA Intern. Med. 2020, 180, 817–818. [Google Scholar] [CrossRef] [Green Version]
- Sojli, E.; Tham, W.W.; Bryant, R.; McAleer, M. COVID-19 restrictions and age-specific mental health-U.S. probability-based panel evidence. Transl. Psychiatry 2021, 11, 418. [Google Scholar] [CrossRef]
- Tegola, D.; Rossi, E.; Colmegna, F.; Riva, M.A.; Paladino, M.E.; Belingheri, M.; Latocca, R.; Sibilla, M.; Dakanalis, A.; Stefana, A.; et al. Health Care Workers During the COVID-19 Pandemic: Focus on Psychological Distress and Burnout. Prim. Care Companion CNS Disord. 2022, 24, 41888. [Google Scholar] [CrossRef]
- Imperatori, C.; Dakanalis, A.; Farina, B.; Pallavicini, F.; Colmegna, F.; Mantovani, F.; Clerici, M. Global Storm of Stress-Related Psychopathological Symptoms: A Brief Overview on the Usefulness of Virtual Reality in Facing the Mental Health Impact of COVID-19. Cyberpsychology Behav. Soc. Netw. 2020, 23, 782–788. [Google Scholar] [CrossRef]
- Sapra, A.; Bhandari, P.; Sharma, S.; Chanpura, T.; Lopp, L. Using Generalized Anxiety Disorder-2 (GAD-2) and GAD-7 in a Primary Care Setting. Cureus 2020, 12, e8224. [Google Scholar] [CrossRef]
- Vicinanza, F.; Ippolito, E.; Sisto, A.; Santo, B.; Fiore, M.; Trodella, L.E.; Silipigni, S.; Quintiliani, L.; Ramella, S. The psychological impact of the covid-19 pandemic on radiotherapy cancer patients. Transl. Oncol. 2022, 22, 101457. [Google Scholar] [CrossRef]
- Rodrigues-Oliveira, L.; Kauark-Fontes, E.; Alves, C.G.B.; Tonaki, J.O.; Gueiros, L.A.; Moutinho, K.; Marta, G.N.; Barros, L.R.C.; Santos-Silva, A.R.; Brandão, T.B.; et al. COVID-19 impact on anxiety and depression in head and neck cancer patients: A cross-sectional study. Oral Dis. 2022, 28 (Suppl. S2), 2391–2399. [Google Scholar] [CrossRef]
- Nieder, C.; Johnsen, S.K.; Winther, A.M. Symptom Burden in Patients Treated with Palliative Radiotherapy Before and during the COVID-19 Pandemic. Anticancer Res. 2021, 41, 1971–1974. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9, validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- World Health Organization; Regional Office for Europe. Wellbeing measures in primary health care/the Dep Care Project: Report on a WHO Meeting: Stockholm, Sweden, 12–13 February 1998. World Health Organization. Regional Office for Europe. Available online: https://apps.who.int/iris/handle/10665/349766 (accessed on 27 July 2022).
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A systematic review of the literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Ryan, H.; Schofield, P.; Cockburn, J.; Butow, P.; Tattersall, M.; Turner, J.; Girgis, A.; Bandaranayake, D.; Bowman, D. How to recognize and manage psychological distress in cancer patients. Eur. J. Cancer Care 2005, 14, 7–15. [Google Scholar] [CrossRef]
- Chen, W.; Lv, X.; Xu, X.; Gao, X.; Wang, B. Meta-analysis for psychological impact of breast reconstruction in patients with breast cancer. Breast Cancer 2018, 25, 464–469. [Google Scholar] [CrossRef]
- Kamposioras, K.; Lim, K.H.J.; Williams, J.; Alani, M.; Barriuso, J.; Collins, J.; Marti, K.; Braun, M.; Mullamitha, S.; Hasan, J.; et al. Modification to Systemic Anticancer Therapy at the Start of the COVID-19 Pandemic and its Overall Impact on Survival Outcomes in Patients with Colorectal Cancer. Clin. Color. Cancer 2022, 21, e117–e125. [Google Scholar] [CrossRef]
- Lee, L.Y.; Cazier, J.-B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Middleton, G. UK Coronavirus Monitoring Project Team. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Yan, B.; Yang, L.-M.; Hao, L.-P.; Yang, C.; Quan, L.; Wang, L.H.; Yuan, J.M. Determinants of quality of life for breast cancer patients in Shanghai, China. PLoS ONE 2016, 11, e0153714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Haar, J.; Hoes, L.R.; Coles, C.E.; Seamon, K.; Fröhling, S.; Jäger, D.; Valenza, F.; de Braud, F.; De Petris, L.; Bergh, J.; et al. Caring for patients with cancer in the COVID-19 era. Nat Med. 2020, 26, 665–671, Correct in Nat Med. 2020, 26, 1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Poll-Franse, L.V.; de Rooij, B.H.; Horevoorts, N.J.E.; May, A.M.; Vink, G.R.; Koopman, M.; van Laarhoven, H.W.M.; Besselink, M.G.; Oerlemans, S.; Husson, O.; et al. Perceived Care and Well-being of Patients With Cancer and Matched Norm Participants in the COVID-19 Crisis: Results of a Survey of Participants in the Dutch PROFILES Registry. JAMA Oncol. 2021, 7, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Mukherji, R.; Marshall, J.L. Lessons Learned in Managing Patients with Colorectal Cancer During the COVID-19 Pandemic. Curr. Treat. Options Oncol. 2021, 22, 93. [Google Scholar] [CrossRef]
- Lionis, C.; Symvoulakis, E.K.; Markaki, A.; Petelos, E.; Papadakis, S.; Sifaki-Pistolla, D.; Papadakakis, M.; Souliotis, K.; Tziraki, C. Integrated people-centred primary health care in Greece: Unravelling Ariadne’s thread. Prim. Health Care Res. Dev. 2019, 20, e113. [Google Scholar] [CrossRef] [Green Version]
- Symvoulakis, E.K.; Zaravinos, A.; Panutsopulos, D.; Zoras, O.; Papalambros, E.; Sigala, F.; Spandidos, D.A. Highly conserved sequence of exon 15 BRAF gene and KRAS codon 12 mutation among Greek patients with colorectal cancer. Int. J. Biol. Markers 2007, 22, 12–18. [Google Scholar] [CrossRef]


{kind=link}
| Sex | Male | 41 | 39.0% | Primary Tumor | Breast | 43 | 41% |
|---|---|---|---|---|---|---|---|
| female | 64 | 61.0% | Lung | 17 | 16.2% | ||
| Age, years | <50 | 30 | 28.6% | Prostate | 10 | 9.5% | |
| 51–60 | 18 | 17.1% | Endometrium | 9 | 8.6% | ||
| 61–70 | 31 | 29.5% | Rectum | 6 | 5.7% | ||
| >70 | 26 | 24.8% | Cervix | 5 | 4.8% | ||
| Family status | married/in civil partnership | 68 | 64.8% | Larynx | 4 | 3.8% | |
| unmarried, divorced, widowed, in relationship | 37 | 35.3% | Brain | 2 | 1.9% | ||
| Child existence | 91 | 86.7% | Anum | 2 | 1.9% | ||
| Single-person household | no | 79 | 75.2% | Bladder | 1 | 1.0% | |
| Previous diagnosis of mental disorder/s * | Anxiety | 37 | 35.2% | Esophagus | 1 | 1.0% | |
| Panic attacks | 25 | 23.8% | Nasal Cavity | 1 | 1.0% | ||
| Depression | 14 | 13.3% | Pancreas | 1 | 1.0% | ||
| Anorexia | 9 | 8.6% | Parotid | 1 | 1.0% | ||
| Bulimia | 7 | 6.7% | Thymoma | 1 | 1.0% | ||
| Obsessive-compulsive disorder | 5 | 4.8% | Stage | I | 30 | 28.6% | |
| Social Phobia/Stress | 4 | 3.8% | II | 26 | 24.8% | ||
| Psychosis | 2 | 1.9% | III | 33 | 31.4% | ||
| Attention deficit disorder | 2 | 1.9% | IV | 16 | 15.2% | ||
| Alcohol/Drug Abuse | 1 | 1.0% | Conditions | Severe chronic obstructive pulmonary disease (e.g., COPD, bronchitis, cystic fibrosis) | 22 | 37.3% | |
| No previous diagnosis of mental disorder/s * | 53 | 50.5% | Immunosuppressive treatment | 18 | 30.5% | ||
| Self-reported perception of the current status of cancer | No active disease or under control | 56 | 54.4% | Diabetes Mellitus | 16 | 27.1% | |
| Progressive disease | 6 | 5.8% | Obesity | 2 | 3.4% | ||
| In progress, unknown, or other | 41 | 39.8% | Transplantation in the past (e.g., heart, kidney, bone marrow, etc.) | 1 | 1.7% | ||
| Pregnancy | 1 | 1.7% | |||||
| Change in physical activity (e.g., exercise) | 49 | 46.7% | |||||
| Coping mechanisms used during the pandemic | Positive attitude | 38 | 36.2% | ||||
| Time management | 32 | 30.5% | |||||
| Overlook | 28 | 26.7% | |||||
| Discuss with medical professionals | 28 | 26.7% | |||||
| Distract himself/herself | 26 | 24.8% | |||||
| Make use of humor | 26 | 24.8% | |||||
| Changes in diet (e.g., types of food, amount) | 16 | 15.2% | |||||
| Utilize religious or spiritual practice(s) | 11 | 10.5% | |||||
| Utilize meditation, mindfulness, or other relaxation techniques | 7 | 6.7% | |||||
| Change in substance intake (e.g., smoking, alcohol, other drugs) | 5 | 4.8% | |||||
| Other | 1 | 1.0% | |||||
| None of the above | 36 | 34.3% | |||||
| COVID-19-Related Questions | Response | N | % |
|---|---|---|---|
| Testing for COVID-19 | Yes | 104 | 99.0% |
| No | 1 | 1.0% | |
| Testing positive | Yes | 6 | 5.7% |
| No | 99 | 94.3% | |
| Willingness to be tested, before anticancer treatment | Yes | 98 | 93.3% |
| No | 7 | 6.7% | |
| Hospitalization for COVID-19 | Yes | 6 | 5.7% |
| No | 99 | 94.3% | |
| Concern about the negative impact of COVID-19 on cancer therapy | Yes | 46 | 43.8% |
| Greater concern about COVID-19 than cancer | Yes | 21 | 20.0% |
| No | 84 | 80.0% | |
| Concern for COVID-19 contraction | Not at all | 18 | 17.1% |
| Slightly | 51 | 48.6% | |
| Moderately | 18 | 17.1% | |
| Very much | 17 | 16.2% | |
| Extremely | 1 | 1.0% |
| Scales | Variables | Odds Ratio (95% CI) | p-Value |
|---|---|---|---|
| Anxiety (GAD-7 ≥ 5) | Previous/Underlying diagnosis of a mental health condition (“No” vs. “Yes”) | 3.743 (1.372–10.210) | 0.010 |
| Felt the COVID-19 pandemic has affected mental health | 1.841 (0.839–4.041) | 0.128 | |
| Needing more support for mental health during COVID-19 | 0.422 (0.126–1.420) | 0.163 | |
| Concern about getting COVID-19 | 0.977 (0.446–2.141) | 0.953 | |
| Stage category (Stage I/II vs. III/IV) | 3.832 (1.380–10.640) | 0.010 | |
| Depression (PHQ-9 ≥ 10) | Age | 1.637 (1.163–2.305) | 0.005 |
| Previous/Underlying diagnosis of a mental health condition (“No” vs. “Yes”) | 14.242 (2.478–81.847) | 0.003 | |
| Concerned that COVID-19 had/will have a negative impact on their cancer treatment (“No” vs. “Yes”) | 0.193 (0.045–0.828) | 0.027 | |
| Concern about getting COVID-19 | 1.145 (0.433–3.033) | 0.785 | |
| Felt the COVID-19 pandemic has affected mental health | 3.561 (1.304–9.726) | 0.013 | |
| Needing more support for mental health during COVID-19 | 1.359 (0.262–7.059) | 0.715 | |
| Well-being (WHO-5 ≥ 50) | Previous/Underlying diagnosis of a mental health condition (“No” vs. “Yes”) | 0.278 (0.056–1.366) | 0.118 |
| Self-reported perception of the current status of cancer | 0.561 (0.117–2.691) | 0.470 | |
| Concerned that COVID-19 had/will have a negative impact on their cancer treatment (“No” vs. “Yes”) | 1.827 (0.404–8.252) | 0.434 | |
| Concern about getting COVID-19 | 0.561 (0.188–1.677) | 0.301 | |
| Felt the COVID-19 pandemic has affected mental health | 0.876 (0.318–2.411) | 0.797 | |
| Needing more support for mental health during COVID-19 | 1.086 (0.176–6.707) | 0.929 | |
| Stage category (Stage IV vs. other) | 0.121 (0.023–0.651) | 0.014 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tolia, M.; Symvoulakis, E.K.; Matalliotakis, E.; Kamekis, A.; Adamou, M.; Kountourakis, P.; Mauri, D.; Dakanalis, A.; Alexidis, P.; Varveris, A.; et al. COVID-19 Emotional and Mental Impact on Cancer Patients Receiving Radiotherapy: An Interpretation of Potential Explaining Descriptors. Curr. Oncol. 2023, 30, 586-597. https://doi.org/10.3390/curroncol30010046
Tolia M, Symvoulakis EK, Matalliotakis E, Kamekis A, Adamou M, Kountourakis P, Mauri D, Dakanalis A, Alexidis P, Varveris A, et al. COVID-19 Emotional and Mental Impact on Cancer Patients Receiving Radiotherapy: An Interpretation of Potential Explaining Descriptors. Current Oncology. 2023; 30(1):586-597. https://doi.org/10.3390/curroncol30010046
Chicago/Turabian StyleTolia, Maria, Emmanouil K. Symvoulakis, Emmanouil Matalliotakis, Apostolos Kamekis, Marios Adamou, Panteleimon Kountourakis, Davide Mauri, Antonios Dakanalis, Petros Alexidis, Antonios Varveris, and et al. 2023. "COVID-19 Emotional and Mental Impact on Cancer Patients Receiving Radiotherapy: An Interpretation of Potential Explaining Descriptors" Current Oncology 30, no. 1: 586-597. https://doi.org/10.3390/curroncol30010046