
Role of Maternal Diet in the Risk of Childhood Acute Leukemia: A Systematic Review and Meta-Analysis
 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Definition of the Outcome
2.2. Definition of the Risk Factors
2.3. Systematic Review Registration
2.4. Search Strategy
2.5. Selection of the Studies and Quality Assessment

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Extracted Factors (Maternal Factors during Pregnancy) | Number of Included Articles 1 | References |
|---|---|---|
| Food group intake (vegetables, fruits, cereals and grains, meats, diary) | 7 | [11,12,13,14,15,16,17] |
| Coffee intake | 11 | [15,18,19,20,21,22,23,24,25,26,27] |
| Tea intake | 7 | [15,18,19,21,22,23,24] |
| Soft drink intake (cola drinks) | 3 | [15,16,22] |
| Micronutrient intake (glutathione, carotenoids, folates, etc.) | 4 | [11,14,28,29] |
| Supplements of vitamins and minerals (folic acid, iron, etc.) | 21 | [11,14,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46] |
2.6. Data Extraction
2.7. Quantitative Meta-Analysis
3. Results
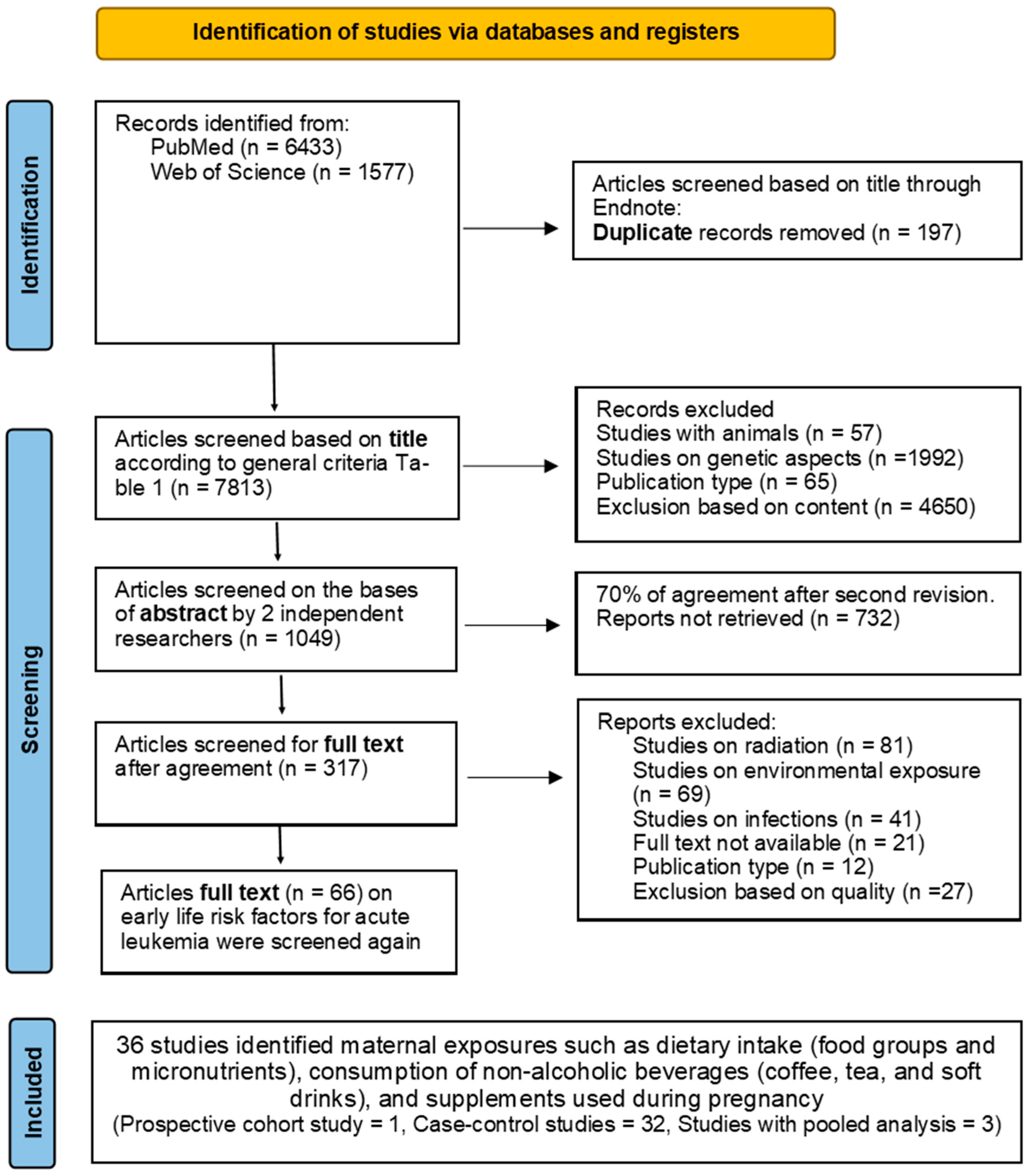
3.1. Selected Studies
3.2. Study Characteristics
3.3. Quality Assessment
3.4. Maternal Intake
3.4.1. Food Group Intakes
3.4.2. Non-Alcoholic Drinks
- A.
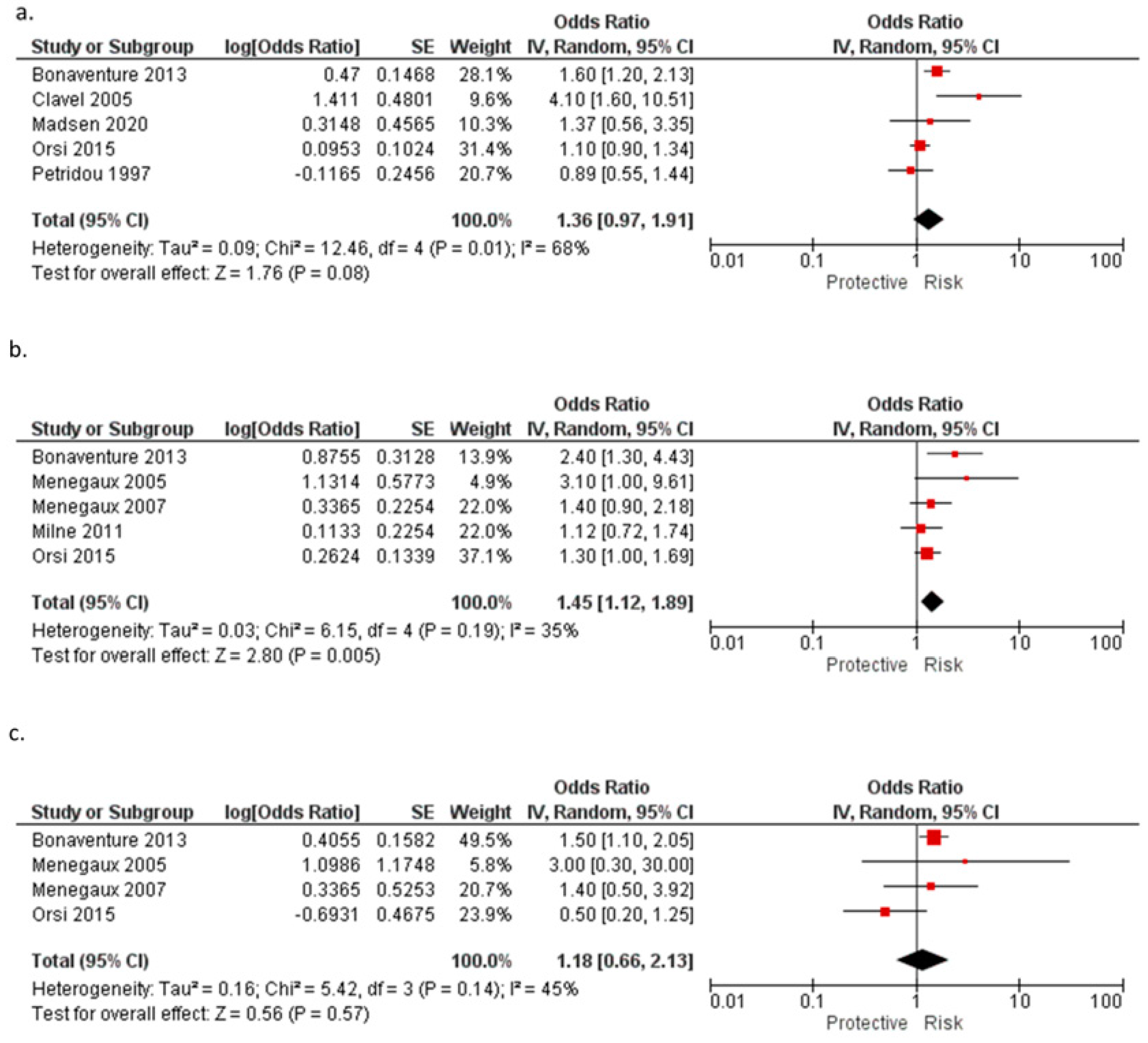
- Coffee
- B.
- Tea
- C.
- Soft drinks
3.5. Nutrients
3.5.1. Micronutrient Intake
3.5.2. Supplements of Vitamins and Minerals
4. Discussion
4.1. Summary of the Main Findings
4.2. Potential Mechanisms
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Correction Statement
IARC Disclaimer
References
- Steliarova-Foucher, E.; Colombet, M.; Ries, L.A.G.; Moreno, F.; Dolya, A.; Bray, F.; Hesseling, P.; Shin, H.Y.; Stiller, C.A.; Bouzbid, S.; et al. International incidence of childhood cancer, 2001–10: A population-based registry study. Lancet. Oncol. 2017, 18, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Coebergh, J.W.; Reedijk, A.M.; de Vries, E.; Martos, C.; Jakab, Z.; Steliarova-Foucher, E.; Kamps, W.A. Leukaemia incidence and survival in children and adolescents in Europe during 1978-1997. Report from the Automated Childhood Cancer Information System project. Eur. J. Cancer 2006, 42, 2019–2036. [Google Scholar] [CrossRef] [PubMed]
- Belson, M.; Kingsley, B.; Holmes, A. Risk factors for acute leukemia in children: A review. Environ. Health Persp. 2007, 115, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Wiemels, J. Perspectives on the causes of childhood leukemia. Chem. Biol. Interact. 2012, 196, 59–67. [Google Scholar] [CrossRef]
- Greaves, M. A causal mechanism for childhood acute lymphoblastic leukaemia. Nat. Rev. Cancer. 2018, 18, 471–484. [Google Scholar] [CrossRef]
- dos Santos Silva, I. Cancer Epidemiology: Principles and Methods; IARC Press: Lyon, France, 1999; pp. 1–34. [Google Scholar]
- Cao, Y.; Lu, J. Paternal Smoking Before Conception and During Pregnancy Is Associated With an Increased Risk of Childhood Acute Lymphoblastic Leukemia: A Systematic Review and Meta-Analysis of 17 Case-Control Studies. J. Pediatr. Hematol. Oncol. 2020, 42, 32–40. [Google Scholar]
- Karalexi, M.A.; Dessypris, N.; Thomopoulos, T.P.; Ntouvelis, E.; Kantzanou, M.; Diamantaras, A.A.; Moschovi, M.; Baka, M.; Hatzipantelis, E.; Kourti, M.; et al. Parental alcohol consumption and risk of leukemia in the offspring: A systematic review and meta-analysis. Eur. J. Cancer Prev. 2017, 26, 433–441. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Fowkes, F.; Fulton, P. Critical appraisal of published research: Introductory guidelines. Brit. Med. J. 1991, 302, 1136–1140. [Google Scholar] [CrossRef]
- Jensen, C.D.; Block, G.; Buffler, P.; Ma, X.; Selvin, S.; Month, S. Maternal dietary risk factors in childhood acute lymphoblastic leukemia (United States). Cancer Causes Control 2004, 15, 559–570. [Google Scholar] [CrossRef]
- Sarasua, S.; Savitz, D.A. Cured and broiled meat consumption in relation to childhood cancer: Denver, Colorado (United States). Cancer Causes Control 1994, 5, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Petridou, E.; Ntouvelis, E.; Dessypris, N.; Terzidis, A.; Trichopoulos, D. Maternal Diet and Acute Lymphoblastic Leukemia in Young Children. Cancer Epidem. Biomar. 2005, 14, 1935–1939. [Google Scholar] [CrossRef]
- Kwan, M.L.; Block, G.; Hudes, M.L.; Chu, L.W.; Buffler, P.A. Maternal diet and risk of childhood acute lymphoblastic leukemia. Public Health Rep. 2009, 124, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.A.; Potter, J.D.; Reaman, G.H.; Pendergrass, T.W.; Robison, L.L. Maternal exposure to potential inhibitors of DNA topoisomerase II and infant leukemia (United States): A report from the Children’s Cancer Group. Cancer Causes Control 1996, 7, 581–590. [Google Scholar] [CrossRef]
- Peters, J.M.; Preston-Martin, S.; London, S.J.; Bowthan, J.D.; Buckley, J.D.; Thomas, D.C. Processed meats and risk of childhood leukemia (California, USA). Am. J. Epidemiol. 1994, 5, 195–202. [Google Scholar] [CrossRef]
- Singer, A.W.; Carmichael, S.L.; Selvin, S.; Fu, C.; Block, G.; Metayer, C. Maternal diet quality before pregnancy and risk of childhood leukaemia. Br. J. Nutr. 2016, 116, 1469–1478. [Google Scholar] [CrossRef]
- Karalexi, M.A.; Dessypris, N.; Clavel, J.; Metayer, C.; Erdmann, F.; Orsi, L.; Kang, A.Y.; Schuz, J.; Bonaventure, A.; Greenop, K.R.; et al. Coffee and tea consumption during pregnancy and risk of childhood acute myeloid leukemia: A Childhood Leukemia International Consortium (CLIC) study. Cancer Epidemiol. 2019, 62, 101581. [Google Scholar] [CrossRef]
- Milne, E.; Greenop, K.R.; Petridou, E.; Bailey, H.D.; Orsi, L.; Kang, A.Y.; Baka, M.; Bonaventure, A.; Kourti, M.; Metayer, C.; et al. Maternal consumption of coffee and tea during pregnancy and risk of childhood ALL: A pooled analysis from the childhood Leukemia International Consortium. Cancer Causes Control 2018, 29, 539–550. [Google Scholar] [CrossRef]
- Menegaux, F.; Ripert, M.; Hemon, D.; Clavel, J. Maternal alcohol and coffee drinking, parental smoking and childhood leukaemia: A French population-based case-control study. Paediatr. Perinat. Epidemiol. 2007, 21, 293–299. [Google Scholar] [CrossRef]
- Menegaux, F.; Steffen, C.; Bellec, S.; Baruchel, A.; Lescoeur, B.; Leverger, G.; Nelken, B.; Philippe, N.; Sommelet, D.; Hemon, D.; et al. Maternal coffee and alcohol consumption during pregnancy, parental smoking and risk of childhood acute leukaemia. Cancer Detect Prev. 2005, 29, 487–493. [Google Scholar] [CrossRef]
- Bonaventure, A.; Rudant, J.; Goujon-Bellec, S.; Orsi, L.; Leverger, G.; Baruchel, A.; Bertrand, Y.; Nelken, B.; Pasquet, M.; Michel, G.; et al. Childhood acute leukemia, maternal beverage intake during pregnancy, and metabolic polymorphisms. Cancer Causes Control 2013, 24, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Milne, E.; Royle, J.A.; Bennett, L.C.; de Klerk, N.H.; Bailey, H.D.; Bower, C.; Miller, M.; Attia, J.; Scott, R.J.; Kirby, M.; et al. Maternal consumption of coffee and tea during pregnancy and risk of childhood ALL: Results from an Australian case-control study. Cancer Causes Control 2011, 22, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Orsi, L.; Rudant, J.; Ajrouche, R.; Leverger, G.; Baruchel, A.; Nelken, B.; Pasquet, M.; Michel, G.; Bertrand, Y.; Ducassou, S.; et al. Parental smoking, maternal alcohol, coffee and tea consumption during pregnancy, and childhood acute leukemia: The ESTELLE study. Cancer Causes Control 2015, 26, 1003–1017. [Google Scholar] [CrossRef]
- Petridou, E.; Trichopoulos, D.; Kalapothaki, V.; Pourtsidis, A.; Kogevinas, M.; Kalmanti, M.; Koliouskas, D.; Kosmidis, H.; Panagiotou, J.P.; Piperopoulou, F.; et al. The risk profile of childhood leukaemia in Greece: A nationwide case-control study. Br. J. Cancer. 1997, 76, 1241–1247. [Google Scholar] [CrossRef]
- Clavel, J.; Bellec, S.; Rebouissou, S.; Menegaux, F.; Feunteun, J.; Bonaiti-Pellie, C.; Baruchel, A.; Kebaili, K.; Lambilliotte, A.; Leverger, G.; et al. Childhood leukaemia, polymorphisms of metabolism enzyme genes, and interactions with maternal tobacco, coffee and alcohol consumption during pregnancy. Eur. J. Cancer. Prev 2005, 14, 531–540. [Google Scholar] [PubMed]
- Madsen, C.N.; Henriksen, T.B.; Ramlau-Hansen, C.H.; Parner, E.T.; Olsen, J.; Bech, B.H. Coffee intake during pregnancy and childhood acute leukemia-A cohort study. Cancer Epidemiol. 2020, 67, 101747. [Google Scholar] [CrossRef]
- Bailey, H.D.; Miller, M.; Langridge, A.; de Klerk, N.H.; van Bockxmeer, F.M.; Attia, J.; Scott, R.J.; Armstrong, B.K.; Milne, E. Maternal dietary intake of folate and vitamins B6 and B12 during pregnancy and the risk of childhood acute lymphoblastic leukemia. Nutr. Cancer 2012, 64, 1122–1130. [Google Scholar] [CrossRef]
- Singer, A.W.; Selvin, S.; Block, G.; Golden, C.; Carmichael, S.L.; Metayer, C. Maternal prenatal intake of one-carbon metabolism nutrients and risk of childhood leukemia. Cancer Causes Control 2016, 27, 929–940. [Google Scholar] [CrossRef]
- Bonaventure, A.; Simpson, J.; Ansell, P.; Roman, E.; Lightfoot, T. Prescription drug use during pregnancy and risk of childhood cancer - is there an association? Cancer Epidemiol. 2015, 39, 73–78. [Google Scholar] [CrossRef]
- Abudaowd, O.A.G.; Subki, S.; Alsaaedi, R.; Alsiyoufi, A.; Al-Khotany, B.; Altaifi, R.; Al-Kadi, H. Breast feeding and its association with childhood leukemia: A retrospective casecontrol study among children attending King Abdulaziz University Hospital in Jeddah, Saudi Arabia. Med. Sci. 2021, 25, 2624–2634. [Google Scholar]
- McKinney, P.A.; Juszczak, E.; Findlay, E.; Smith, K.; Thomson, C.S. Pre- and perinatal risk factors for childhood leukaemia and other malignancies: A Scottish case control study. Br. J. Cancer 1999, 80, 1844–1851. [Google Scholar] [CrossRef]
- Robison, L.L.; Buckley, J.D.; Daigle, A.E.; Wells, R.; Benjamin, D.; Arthur, D.C.; Hammond, G.D. Maternal drug use and risk of childhood nonlymphoblastic leukemia among offspring. An epidemiologic investigation implicating marijuana (a report from the Childrens Cancer Study Group). Cancer 1989, 63, 1904–1911. [Google Scholar] [PubMed]
- Van Steensel-Moll, H.A.; Valkenburg, H.A.; Vandenbroucke, J.P.; van Zanen, G.E. Are maternal fertility problems related to childhood leukaemia? Int. J. Epidemiol. 1985, 14, 555–559. [Google Scholar]
- Kwan, M.L.; Metayer, C.; Crouse, V.; Buffler, P.A. Maternal illness and drug/medication use during the period surrounding pregnancy and risk of childhood leukemia among offspring. Am. J. Epidemiol. 2006, 165, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Linabery, A.M.; Puumala, S.E.; Hilden, J.M.; Davies, S.M.; Heerema, N.A.; Roesler, M.A.; Ross, J.A.; Children’s Oncology, G. Maternal vitamin and iron supplementation and risk of infant leukaemia: A report from the Children’s Oncology Group. Br. J. Cancer 2010, 103, 1724–1728. [Google Scholar] [CrossRef] [PubMed]
- Schuz, J.; Weihkopf, T.; Kaatsch, P. Medication use during pregnancy and the risk of childhood cancer in the offspring. Eur. J. Pediatr. 2007, 166, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.K.; Infante-Rivard, C.; Morrison, H.I. Use of medication during pregnancy and risk of childhood leukemia (Canada). Cancer Causes Control 2004, 15, 931–937. [Google Scholar] [CrossRef]
- Wen, W.; Shu, X.O.; Potter, J.D.; Severson, R.K.; Buckley, J.D.; Reaman, G.H.; Robison, L.L. Parental medication use and risk of childhood acute lymphoblastic leukemia. Cancer 2002, 95, 1786–1794. [Google Scholar] [CrossRef]
- Ajrouche, R.; Rudant, J.; Orsi, L.; Petit, A.; Baruchel, A.; Nelken, B.; Pasquet, M.; Michel, G.; Bergeron, C.; Ducassou, S.; et al. Maternal reproductive history, fertility treatments and folic acid supplementation in the risk of childhood acute leukemia: The ESTELLE study. Cancer Causes Control 2014, 25, 1283–1293. [Google Scholar] [CrossRef]
- Amigou, A.; Rudant, J.; Orsi, L.; Goujon-Bellec, S.; Leverger, G.; Baruchel, A.; Bertrand, Y.; Nelken, B.; Plat, G.; Michel, G.; et al. Folic acid supplementation, MTHFR and MTRR polymorphisms, and the risk of childhood leukemia: The ESCALE study (SFCE). Cancer Causes Control 2012, 23, 1265–1277. [Google Scholar] [CrossRef]
- Dockerty, J.D.; Herbison, P.; Skegg, D.C.; Elwood, M. Vitamin and mineral supplements in pregnancy and the risk of childhood acute lymphoblastic leukaemia: A case-control study. BMC Public Health 2007, 7, 136. [Google Scholar] [CrossRef] [PubMed]
- Milne, E.; Royle, J.A.; Miller, M.; Bower, C.; de Klerk, N.H.; Bailey, H.D.; van Bockxmeer, F.; Attia, J.; Scott, R.J.; Norris, M.D.; et al. Maternal folate and other vitamin supplementation during pregnancy and risk of acute lymphoblastic leukemia in the offspring. Int. J. Cancer 2010, 126, 2690–2699. [Google Scholar] [CrossRef] [PubMed]
- Ognjanovic, S.; Blair, C.; Spector, L.G.; Robison, L.L.; Roesler, M.; Ross, J.A. Analgesic use during pregnancy and risk of infant leukaemia: A Children’s Oncology Group study. Br. J. Cancer 2011, 104, 532–536. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.R.; Gerald, P.F.; Willoughby, M.L.; Armstrong, B.K. Maternal folate supplementation in pregnancy and protection against acute lymphoblastic leukaemia in childhood: A case-control study. Lancet 2001, 358, 1935–1940. [Google Scholar] [CrossRef]
- Metayer, C.; Milne, E.; Dockerty, J.D.; Clavel, J.; Pombo-de-Oliveira, M.S.; Wesseling, C.; Spector, L.G.; Schuz, J.; Petridou, E.; Ezzat, S.; et al. Maternal supplementation with folic acid and other vitamins and risk of leukemia in offspring: A Childhood Leukemia International Consortium study. Epidemiology 2014, 25, 811–822. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S.; Cochrane, C. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Chichester, UK, 2008; pp. 245–246. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. Brit. Med. J. 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- RevMan Web. Review Manager Web (RevMan Web), Version 5.4; The Cochrane Collaboration: London, UK, 2020. [Google Scholar]
- Dessypris, N.; Karalexi, M.A.; Ntouvelis, E.; Diamantaras, A.A.; Papadakis, V.; Baka, M.; Hatzipantelis, E.; Kourti, M.; Moschovi, M.; Polychronopoulou, S.; et al. Association of maternal and index child’s diet with subsequent leukemia risk: A systematic review and meta analysis. Cancer Epidemiol. 2017, 47, 64–75. [Google Scholar] [CrossRef]
- Charalampopoulou, A.; Petridou, E.; Spyridopoulos, T.; Dessypris, N.; Oikonomou, A.; Athanasiadou-Piperopoulou, F.; Baka, M.; Kalmanti, M.; Polychronopoulou, S.; Trichopoulos, D. An integrated evaluation of socioeconomic and clinical factors in the survival from childhood acute lymphoblastic leukaemia: A study in Greece. Eur. J. Cancer Prev. 2004, 13, 397–401. [Google Scholar] [CrossRef]
- Thomopoulos, T.P.; Ntouvelis, E.; Diamantaras, A.A.; Tzanoudaki, M.; Baka, M.; Hatzipantelis, E.; Kourti, M.; Polychronopoulou, S.; Sidi, V.; Stiakaki, E.; et al. Maternal and childhood consumption of coffee, tea and cola beverages in association with childhood leukemia: A meta-analysis. Cancer Epidemiol. 2015, 39, 1047–1059. [Google Scholar] [CrossRef]
- Yan, K.; Xu, X.; Liu, X.; Wang, X.; Hua, S.; Wang, C.; Liu, X. Corrigendum: The Associations Between Maternal Factors During Pregnancy and the Risk of Childhood Acute Lymphoblastic Leukemia: A Meta-Analysis. Pediatr. Blood Cancer 2016, 63, 953–954. [Google Scholar] [CrossRef]
- Wan Ismail, W.R.; Abdul Rahman, R.; Rahman, N.A.A.; Atil, A.; Nawi, A.M. The Protective Effect of Maternal Folic Acid Supplementation on Childhood Cancer: A Systematic Review and Meta-analysis of Case-control Studies. J. Prev. Med. Public Health 2019, 52, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Ye, F.; Wu, J.; How, B.; Li, W.; Zhang, D.Y. Signaling proteins and pathways affected by flavonoids in leukemia cells. Nutr. Cancer 2015, 67, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, P.; Clifford, C.K.; Milner, J.A. Diet and cancer prevention. Eur. J. Cancer 2001, 37, 948–965. [Google Scholar] [CrossRef]
- Cacciatore, I.; Cornacchia, C.; Pinnen, F.; Mollica, A.; Di Stefano, A. Prodrug approach for increasing cellular glutathione levels. Molecules 2010, 15, 1242–1264. [Google Scholar] [CrossRef] [PubMed]
- Tricker, A.R. Carcinogenic N-nitrosamines in the diet: Occurrence, formation, mechanisms and carcinogenic potential. Mutat. Res. 1991, 259, 277–289. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, M.; Block, G.; Pogoda, J.M.; Buffler, P.; Hecht, S.; Preston-Martin, S. A review: Dietary and endogenously formed N-nitroso compounds and risk of childhood brain tumors. Cancer Causes Control 2005, 16, 619–635. [Google Scholar] [CrossRef] [PubMed]
- Cantarella, C.D.; Ragusa, D.; Giammanco, M.; Tosi, S. Folate deficiency as predisposing factor for childhood leukaemia: A review of the literature. Genes Nutr. 2017, 12, 14. [Google Scholar] [CrossRef]
- Jang, S.; Bae, J.; Lee, Y.; Oh, K.; Park, K.; Bae, Y. Caffeic acid and quercitrin purified from Houttuynia cordata inhibit DNA topoisomerase I activity. Nat. Prod. Res. 2011, 25, 222–231. [Google Scholar] [CrossRef]
- Naowaratwattana, W.; De-Eknamkul, W.; De Mejia, E.G. Phenolic-containing organic extracts of mulberry (Morus alba L.) leaves inhibit HepG2 hepatoma cells through G2/M phase arrest, induction of apoptosis, and inhibition of topoisomerase IIα activity. J. Med. Food. 2010, 13, 1045–1056. [Google Scholar] [CrossRef]
- Burgos-Moron, E.; Calderon-Montano, J.M.; Orta, M.L.; Pastor, N.; Perez-Guerrero, C.; Austin, C.; Mateos, S.; Lopez-Lazaro, M. The coffee constituent chlorogenic acid induces cellular DNA damage and formation of topoisomerase I- and II-DNA complexes in cells. J. Agric. Food Chem. 2012, 60, 7384–7391. [Google Scholar] [CrossRef]
- Kleinjans, J.; Botsivali, M.; Kogevinas, M.; Merlo, D.F. Fetal exposure to dietary carcinogens and risk of childhood cancer: What the NewGeneris project tells us. Bmj 2015, 351, h4501. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffman, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.K.; Akl, E.A.; Brenan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar]




| General inclusion criteria |
| All studies describing the maternal dietary factors and their influence on the incidence of acute leukemia in children and adolescents were included in the systematic review. The risk factors considered were maternal nutrition (food and beverages) and supplement use during pregnancy. Pooled analysis including new data was also included in the review. |
| General exclusion criteria |
|
| Exclusion criteria based on content |
|
| Exclusion criteria based on study scope and data quality |
|
| Parameter | Criterion |
|---|---|
| Participants | Children and adolescents diagnosed with acute leukemia |
| Interventions | Maternal dietary intake (including food groups and caffeinated beverages) and supplements |
| Control/comparator group | Healthy children and adolescents |
| Outcomes | Childhood acute leukemia |
| Study design | Observational studies with a comparison group (cohort studies, case-control studies) |
| Study/Reference | Location and Study Period | Leukemia Type | Age Range (Years) | Cases/Controls | Control Source | Maternal Exposure Variable(s) | Source(s)/Assessment Tool |
|---|---|---|---|---|---|---|---|
| Cohort | |||||||
| Madsen et al. [27] | Denmark, 1996–2002 | Acute leukemia | 0–14 | 96/Cohort 141, 216 | Coffee and tea consumption | Health registries | |
| Case control | |||||||
| Abudaowd et al. [31] | Saudi Arabia, 2008–2019 | ALL, AML | 1–19 | 74/148 | Community controls matched on age and gender | Use of supplements | Structured telephone interview |
| Ajrouche et al. [40] (ESTELLE a) | France, 2010–2011 | ALL, AML | 0–14 | 747/1421 | Population controls matched on age and gender | Use of supplements | Structured telephone questionnaires |
| Amigou et al. [41] (ESCALE a) | France, 2003–2004 | ALL, AML | 0–14 | 764/1681 | Randomly selected from French households with a landline telephone | Use of supplements | Standardized telephone interview |
| Bailey et al. [28] (Aus-ALL b) | Australia, 2003–2007 | ALL | 0–14 | 333/695 | Prospectively recruited by random digit dialing and matched on age, sex and residence | Micronutrients and supplements | Mailed, self-administered questionnaires and Food Frequency Questionaries |
| Bonaventure et al. [22] 2013 (ESCALE a) | France, 2003–2004 | ALL, AML | 0–14 | 764/1681 | Randomly selected with a landline telephone | Coffee, tea and cola drink consumption | Interviewed with standardized questionnaires |
| Bonaventure et al. [30] 2015 (UKCCS c) | UK, 1991–1996 | ALL, AML | 0–14 | 864/2524 | Community controls matched on sex, month and year of birth and region of residence | Use of supplements | Primary care (general practice) records |
| Clavel et al. [26] (ADELE a) | France, 1995–1999 | ALL, AML | 0–14 | 247/288 | Hospitalized controls (for diseases other than cancer or birth defects) matched on age, gender and center | Coffee consumption | Interviewer-administered questionnaire |
| Dockerty et al. [42] | New Zealand, 1990–1993 | ALL | 0–14 | 97/303 | Randomly from birth records, on age and sex | Use of supplements | Interviewer-administered questionnaire |
| Jensen et al. [11] (NCCLS d) | Northern California, 1995–1999 | ALL | 0–14 | 138/138 | Community controls matched on age, sex, Hispanic ethnicity and maternal race | Dietary intake, micronutrient and supplement use | Interviewer-administered questionnaire |
| Kwan et al. [35] (NCCLS d) | California, 1995–2002 | Acute leukemia | 0–14 | 311/398 | Community controls matched on age, sex, Hispanic ethnicity and maternal race | Use of supplements | Interviewer-administered questionnaire |
| Kwan et al. [14] (NCCLS d) | California, 1995–2002 | ALL | 0–14 | 282/359 | Community controls matched on age, sex, Hispanic ethnicity and maternal race | Dietary intake and micronutrients | Interviewer-administered questionnaire |
| Linabery et al. [36] (COG e) | USA, Canada, 1996–2006 | ALL, AML | <1 year | 443/324 | Community controls matched on birth year and location of residence | Use of supplements | Telephone interviews |
| McKinney et al. [32] | Scotland, 1976–1994 | Acute leukemia | 0–14 | 144/716 | Community controls matched on age, sex, region (for four studies) | Use of supplements | Interviewer-administered questionnaire |
| Menegaux et al. [20] (ELECTRE a) | France, 1995–1998 | ALL, AML | 0–14 | 534/567 | Community controls matched on age, sex, region | Coffee consumption | Self-administered standardized questionnaire |
| Menegaux et al. [21] (ADELE a) | France, 1995–1999 | ALL, AML | 0–14 | 280/288 | Hospitalized controls (for diseases other than cancer or birth defects) matched on age, gender and center | Coffee and tea consumption | Interviewer-administered questionnaire |
| Milne et al. [43] (Aus-ALL b) | Australia, 2003–2007 | ALL | 0–14 | 416/1361 | Prospectively recruited by random digit dialing and matched on age, sex and residence | Use of supplements | Mailed, self-administered questionnaires and Food Frequency Questionaries |
| Milne et al. [23] (Aus-ALL b) | Australia, 2003–2007 | ALL | 0–14 | 393/1249 | Prospectively recruited by random digit dialing and matched on age, sex and residence | Coffee and tea consumption | Mailed, self-administered questionnaires and Food Frequency Questionaries |
| Ognjanovic et al. [44] (COG e) | USA, Canada, 1996–2006 | ALL, AML | <1 year | 434/323 | Community controls matched on birth year and location of residence | Use of supplements | Telephone interview |
| Orsi et al. [24] (ESTELLE a) | France, 2010–2011 | ALL, AML | 0–14 | 747/1421 | Community controls matched on age and gender | Coffee and tea consumption | Structured telephone questionnaires |
| Peters et al. [16] | California, USA, 1980–1987 | Acute leukemia | 0–10 | 232/288 | Community controls matched on age, ethnicity and sex by random digit dialing | Dietary intake and cola drink consumption | Interviewer-administered questionnaire |
| Petridou et al. [25] | Greece, 1993–1994 | Acute leukemia | 0–14 | 153/300 | Hospitalized controls matched on age and sex, contemporaneously hospitalized for minor conditions | Coffee consumption | Interviewer-administered questionnaire |
| Petridou et al. [13] | Greece, 1999–2003 | ALL | 0–4 | 131/131 | Hospitalized controls matched on age and sex, contemporaneously hospitalized for minor conditions | Dietary intake | Interviewer-administered questionnaire |
| Robison et al. [33] (CCG f) | USA, 1980–1984 | AML | 0–14 | 204/203 | Controls were chosen with random digit dialing and matched on age, race and location | Use of supplements | Interview |
| Ross et al. [15] (CCG f) | USA, 1983–1988 | AML | <18 months | 84/97 | Controls were chosen with random digit dialing and matched on age, race and location | Dietary intake, coffee, tea and cola drink consumption and use of supplements | Medical records and interview |
| Sarasua et al. [12] | USA, 1973–1986 | ALL | 0–14 | 56/206 | Community controls matched by age, sex and telephone exchange area. By random digit dialing | Dietary intake | Medical records and interview |
| Schuz et al. [37] | Germany, 1992–1997 | ALL, AML | 0–14 | 755/2057 | Community controls matched on age, sex and residence | Use of supplements | Self-administered questionnaire and telephone interview |
| Shaw et al. [38] | Canada, 1980–2000 | Acute leukemia | 0–14 | 789/789 | Community controls matched on age and sex | Use of supplements | Telephone interview |
| Singer et al. [17] (NCCLS d) | California, 1995–2008 | ALL, AML | 0–14 | 784/1,076 | Community controls matched on age, sex, Hispanic ethnicity and maternal race | Dietary intake | Interviewer-administered questionnaire |
| Singer et al. [29] (NCCLS d) | California, 1995–2008 | ALL, AML | 0–14 | 784/1,076 | Community controls matched on age, sex, Hispanic ethnicity and maternal race | Micronutrient intake and maternal supplement use | Interviewer-administered questionnaire |
| Thompson et al. [45] | Australia, 1984–1992 | ALL | 0–14 | 98/166 | Controls matched for age and sex randomly selected from the state electoral roll | Use of supplements | Self-administered questionnaire, interview and medical records |
| Van Steensel-Moll et al. [34] | Netherlands, 1973–2010 | ALL | 0–14 | 519/507 | Community controls matched on age, sex and residence | Use of supplements | Mailed questionnaires |
| Wen et al. [39] (CCG f) | USA, Canada, Australia, 1989–1993 | ALL | 0–14 | 1842/1986 | Controls were chosen with random digit dialing and matched on age, race and location | Use of supplements | Telephone interview |
| Pooled analysis | |||||||
| Karalexi et al. [18] (CLIC g) | France, Germany, Greece, USA, 1999–2003 | AML | 0–14 | 444/1255 | Community controls matched on age and sex | Coffee and tea consumption | Self-administered questionnaire and telephone interview |
| Metayer et al. [46] (CLIC g) | Australia, Canada, France, Germany, New Zealand and the United States (from CLIC) and Brazil, Costa Rica, Egypt and Greece, 1980–2012 | ALL, AML | 0–14 | 7548/11,635 | Controls participating in age-matched studies | Use of supplements | Self-administered questionnaire and telephone interview |
| Milne et al. [19] (CLIC g) | France, Australia, Greece, USA, 1995–2016 | ALL | 0–14 | 2552/4876 | Community controls (matched by study variables) | Coffee and tea consumption | Food frequency questionnaires and general questionnaires |
| Reference | Type of Leukemia | Food Group | OR | 95% CI | Adjustments | |
|---|---|---|---|---|---|---|
| Jensen et al. [11] & | ALL | Vegetables | 0.53 | 0.33–0.85 * | Total energy intake, income, history of | |
| Fruits | 0.71 | 0.49–1.04 | miscarriage or stillbirth, hours of exposure to other children in day care, indoor exposure to insecticide during pregnancy and the proportion of foods reported as great or very large | |||
| Grain products | 1.6 | 0.37–1.98 | ||||
| Dairy products | 1.16 | 0.78–1.72 | ||||
| Protein sources | 0.4 | 0.18–0.90 * | ||||
| Cured meat | 0.71 | 0.44–1.15 | ||||
| Fat, sweets and snacks | 1.18 | 0.67–2.06 | ||||
| Kwan et al. [14] & | ALL | Vegetables (excludes salad, potatoes, soup and stew) | 0.65 | 0.50–0.84 * | Adjusted for total energy intake, household income, indoor insecticide exposure during pregnancy and proportion of foods reported as large or extra-large portion size | |
| Fruit (excludes fruit juice) | 0.81 | 0.65–1.00 * | ||||
| Grain products | 1.2 | 0.70–2.05 | ||||
| Dairy products | 1.06 | 0.83–1.35 | ||||
| Legumes | 0.75 | 0.59–0.95 * | ||||
| Protein sources | 0.55 | 0.32–0.96 * | ||||
| Cured meat | 0.91 | 0.78–1.05 | ||||
| Peters et al. [16] | Acute leukemia | ≥12 servings/month: | Self-reported use of indoor pesticides, hair dryers, black-and-white televisions and fathers’ occupational exposure to spray paint during pregnancy and to other chemical exposures post-pregnancy | |||
| Ham, bacon and sausage | 1 | 0.50–2.00 | ||||
| Hot dogs | 2.4 | 0.70–8.10 | ||||
| Bologna, pastrami, corned beef and lunch meat | 1.3 | 0.80–2.40 | ||||
| Hamburgers | 1.2 | 0.50–2.50 | ||||
| Charbroiled meats | 0.9 | 0.50–1.80 | ||||
| ≥30 servings/month: | ||||||
| Oranges or orange juice | 0.8 | 0.50–1.40 | ||||
| Grapefruit or grapefruit juice | 1.1 | 0.50–2.70 | ||||
| Apple or apple juice | 0.9 | 0.50–1.40 | ||||
| Petridou et al. [13] | ALL | per quintile increase: | Sex and age, maternal age at birth, birth weight, maternal smoking during pregnancy, maternal education level, job occupation and total daily energy intake during pregnancy | |||
| Vegetables | 0.76 | 0.60–0.95 * | ||||
| Fruits | 0.72 | 0.57–0.91 * | ||||
| Grain products | 1.23 | 0.94–1.60 | ||||
| Milk and dairy products | 0.82 | 0.66–1.02 | ||||
| Meat and meat products | 1.25 | 1.00–1.57 * | ||||
| Butter and margarine | 1.41 | 0.97–2.06 | ||||
| Sugar and syrup | 1.32 | 1.05–1.67 * | ||||
| Pulses and nuts | 0.96 | 0.77–1.20 | ||||
| Fish and seafood | 0.72 | 0.59–0.89 * | ||||
| Ross et al. [15] | Acute leukemia | Vegetables # (daily) | 2.8 | 1.20–6.40 * | Adjusted for maternal education | |
| Fruits # (daily) | 1.6 | 0.70–3.30 | ||||
| Beans # (≥1/week) | 1.2 | 0.50–3.10 | ||||
| Butter (≥1/week) | 1.4 | 0.70–3.00 | ||||
| Cured meats (≥4/week) | 1 | 0.50–2.20 | ||||
| Fish (≥4/week) | 0.5 | 0.20–1.10 | ||||
| Sarasua et al. [12] | ALL | ≥1 serving/week: | Adjusted for other types of meat (dichotomized), age at diagnosis and per capita income | |||
| Ham, bacon and sausage | 1.5 | 0.70–3.00 | ||||
| Hot dogs | 0.9 | 0.40–1.80 | ||||
| Hamburgers | 1.2 | 0.50–2.70 | ||||
| Charcoal-broiled foods | 1 | 0.50–1.90 | ||||
| Singer et al. [17] & | ALL | 1 serving/4184 kJ (1000 kcal) | Maternal Hispanic ethnicity, household income, mother’s education, father’s education, maternal age category and vitamin supplement use | |||
| Vegetables | 0.97 | 0.86–1.10 | ||||
| Fruits | 0.7 | 0.52–0.94 * | ||||
| Dairy products | 1.01 | 0.84–1.22 | ||||
| Dietary fiber from beans (1 g) | 0.95 | 0.88–1.02 | ||||
| Protein (10 g) | 0.91 | 0.79–1.05 | ||||
| Fatty acid ratio | 1.07 | 0.78–1.45 | ||||
| Trans fat (1 g) | 1.07 | 0.99–1.16 | ||||
| Percentage of energy content from sweets (10%) | 1.09 | 0.94–1.26 | ||||
| AML | 1 serving/4184 kJ (1000 kcal): | |||||
| Vegetables | 0.84 | 0.54–1.30 | ||||
| Fruits | 0.23 | 0.08–0.70* | ||||
| Dairy products | 0.87 | 0.48–1.57 | ||||
| Dietary fiber from beans (1 g) | 1.03 | 0.80–1.34 | ||||
| Protein (10 g) | 1 | 0.63–1.59 | ||||
| Fatty acid ratio | 1.08 | 0.42–2.77 | ||||
| Trans fat (1 g) | 1.11 | 0.85–1.44 | ||||
| Percentage of energy content from sweets (10%) | 1.4 | 0.84–2.34 | ||||
| Reference | Type of Leukemia | Consumption (Cups per Day) Never as Reference | OR | 95% CI | Adjustments |
|---|---|---|---|---|---|
| Cohort study | |||||
| Madsen et al. [27] | Acute leukemia | 0.5–3 | 0.89 | 0.48–1.65 | Adjusted for cohort (Danish National Birth/Aarhus Birth), smoking, maternal age at birth and parity |
| >3 | 1.37 | 0.56–3.32 | |||
| Case-control study | |||||
| Bonaventure et al. [22] | Acute leukemia | <1 | 1.00 | 0.80–1.30 | Gender, age, birth order, breastfeeding, maternal education and parental socio-professional category |
| 1–2 | 1.30 | 1.00–1.70 * | |||
| >2 | 1.60 | 1.20–2.10 * | |||
| ALL | <1 | 1.30 | 0.70–2.10 | ||
| 1–2 | 1.80 | 1.00–3.30 * | |||
| >2 | 2.40 | 1.30–4.30 * | |||
| AML | <1 | 1.00 | 0.80–1.30 | ||
| 1–2 | 1.30 | 1.00–1.70 * | |||
| >2 | 1.50 | 1.10–2.00 * | |||
| Clavel et al. [26] | Acute leukemia | <3 | 1.60 | 0.90–2.90 | Age, gender, center, origin and parental socio-professional category |
| ≥3 | 4.10 | 1.60–10.10 * | |||
| Menegaux et al. [21] | ALL | ≤3 | 1.10 | 0.70–1.80 | Child’s age, sex, center, origin |
| 4–8 | 2.40 | 1.30–4.70 * | |||
| >8 | 3.10 | 1.00–9.50 * | |||
| ANLL | ≤3 | 1.60 | 0.60–4.30 | ||
| 4–8 | 2.80 | 0.70–10.40 | |||
| >8 | 3.00 | 0.30–35.10 | |||
| Menegaux et al. [20] | ALL | ≤3 | 1.10 | 0.80–1.40 | Adjusted for age, gender, region, socio-professional category and birth order |
| >3 | 1.40 | 0.90–2.40 | |||
| AML | ≤3 | 1.60 | 0.80–3.00 | ||
| >3 | 1.40 | 0.50–4.40 | |||
| Milne et al. [23] | ALL | 0–1 | 0.77 | 0.51–1.16 | Age, sex, state of residence, maternal age, mother’s country of birth and parent education |
| >1 | 1.12 | 0.72–1.74 | |||
| Orsi et al. [24] | Acute leukemia | ≤1 | 0.80 | 0.70–1.00 | Age, sex, mother’s age at child’s birth, mother’s education and birth order |
| >1–2 | 1.00 | 0.70–1.30 | |||
| >2 | 1.10 | 0.90–1.50 | |||
| ALL | ≤1 | 0.80 | 0.60–1.10 | ||
| >1–2 | 1.00 | 0.70–1.30 | |||
| >2 | 1.30 | 1.00–1.70 * | |||
| AML | ≤1 | 0.90 | 0.60–1.50 | ||
| >1–2 | 1.10 | 0.60–1.90 | |||
| >2 | 0.50 | 0.20–1.10 | |||
| Petridou et al. [25] | Acute leukemia | >2 | 0.89 | 0.55–1.46 | Gender, age and place of residence |
| Ross et al. [15] | Acute leukemia | ≤3/week | 1.50 | 0.70–3.30 | Adjusted for maternal education |
| ≥4/week | 2.50 | 1.00–6.20 * | |||
| ALL | ≤3/week | 1.10 | 0.40–3.00 | ||
| ≥4/week | 2.30 | 0.70–8.20 | |||
| AML | ≤3/week | 2.40 | 0.60–9.20 | ||
| ≥4/week | 2.60 | 0.70–10.00 | |||
| Pooled analysis | |||||
| Karalexi et al. [18] | AML | 1 | 1.03 | 0.74–1.43 | Child’s age, sex, ethnicity, maternal age, household socioeconomic status, maternal smoking, birth weight |
| >1 | 1.40 | 1.03–1.92 * | |||
| 1 cup per day increment | 1.18 | 1.01–1.39 * | |||
| Milne et al. [19] | ALL | Any | 1.04 | 0.94–1.19 | Child’s age, sex and ethnicity, study of origin, birth order, birth year, maternal age and education, household socioeconomic status, maternal smoking during pregnancy and breastfeeding |
| >0–1 | 0.95 | 0.84–1.07 | |||
| >1–2 | 1.07 | 0.92–1.25 | |||
| >2 | 1.27 | 1.09–1.48 * | |||
| Reference | Type of Leukemia | Consumption (Cups per Day) Never as Reference | OR | 95% CI | Adjustments |
|---|---|---|---|---|---|
| Case control study | |||||
| Bonaventure et al. [22] | Acute leukemia | <1 | 1.10 | 0.80–1.50 | Gender, age, birth order, breastfeeding, maternal education and parental socio-professional category |
| 1 | 0.80 | 0.70–1.10 | |||
| >1 | 0.90 | 0.70–1.20 | |||
| ALL | <1 | 1.50 | 0.80–2.70 | ||
| 1 | 0.90 | 0.50–1.60 | |||
| >1 | 0.50 | 0.20–1.10 | |||
| AML | <1 | 1.10 | 0.80–1.50 | ||
| 1 | 0.80 | 0.60–1.10 | |||
| >1 | 1.00 | 0.70–1.30 | |||
| Menegaux et al. [21] | ALL | ≤3 | 1.20 | 0.80–1.90 | Child’s age, sex, center, origin |
| >3 | 1.20 | 0.60–2.60 | |||
| ANLL | ≤3 | 0.60 | 0.30–1.40 | ||
| >3 | – | – | |||
| Milne et al. [23] | ALL | Any | 0.82 | 0.56–1.18 | Age, sex, state of residence, maternal age, mother’s country of birth and parent education |
| 0–1 | 0.81 | 0.54–1.22 | |||
| >1 | 0.82 | 0.54–1.23 | |||
| Orsi et al. [24] | Acute leukemia | ≤1 | 0.90 | 0.60–1.20 | Age, sex, mother’s age at child’s birth, mother’s education and birth order. |
| 1 | 0.80 | 0.70–1.10 | |||
| >1 | 1.10 | 0.80–1.40 | |||
| ALL | ≤1 | 0.90 | 0.60–1.20 | ||
| 1 | 0.80 | 0.60–1.10 | |||
| >1 | 1.00 | 0.80–1.40 | |||
| AML | ≤1 | 0.90 | 0.40–1.90 | ||
| 1 | 1.20 | 0.70–2.10 | |||
| >1 | 1.00 | 0.50.–1.80 | |||
| Ross et al. [15] | AML | ≤3/week | 0.50 | 0.10–2.30 | Adjusted for maternal education |
| ≥4/week | 0.30 | 0.10–1.70 | |||
| Pooled analysis | |||||
| Karalexi et al. [18] | AML | 1 | 0.95 | 0.68–1.33 | Child’s age, sex, ethnicity, maternal age, household socioeconomic status, maternal smoking, birth weight |
| >1 | 0.70 | 0.42–1.15 | |||
| 1 cup per day increment | 0.87 | 0.70–1.08 | |||
| Milne et al. [19] | ALL | Any | 0.94 | 0.85–1.03 | Child’s age, sex and ethnicity, study of origin, birth order, birth year, maternal age and education, household socioeconomic status, maternal smoking during pregnancy and breastfeeding |
| >0–1 | 0.95 | 0.83–1.08 | |||
| >1–2 | 0.93 | 0.76–1.15 | |||
| >2 | 1.02 | 0.83–1.25 | |||
| Reference | Type of Leukemia | Consumption Never as Reference | OR | 95% CI | Adjustments |
|---|---|---|---|---|---|
| Bonaventure et al. [22] | Acute leukemia | 1 glass/day | 1.10 | 0.80–1.50 | Gender, age, birth order, breastfeeding, maternal education and parental socio-professional category |
| >1 glass/week | 1.30 | 1.00–1.60 * | |||
| >1 glass/day | 1.30 | 1.00–1.80 * | |||
| ALL | 1 glass/day | 0.80 | 0.40–1.80 | ||
| >1 glass/week | 1.30 | 0.80–2.20 | |||
| >1 glass/day | 1.10 | 0.50–2.10 | |||
| AML | 1 glass/day | 1.20 | 0.80–1.60 | ||
| >1 glass/week | 1.20 | 1.00–1.60 * | |||
| >1 glass/day | 1.30 | 1.00–1.80 * | |||
| Peters et al. [16] | Acute leukemia | ≥30 glasses/month | 1.00 | 0.60–1.60 | Adjustments for all factors thought to be potential confounders did not affect these associations |
| Ross et al. [15] | Acute leukemia | ≤3 glasses/week | 1.60 | 0.70–3.60 | Adjusted for maternal education |
| ≥4 glasses/week | 0.90 | 0.40–2.00 | |||
| ALL | ≤3 glasses/week | 2.60 | 0.90–7.50 | ||
| ≥4 glasses/week | 1.00 | 0.30–2.80 | |||
| AML | ≤3 glasses/week | 0.70 | 0.10–3.00 | ||
| ≥4 glasses/week | 0.60 | 0.10–2.30 |
| Reference | Type of Leukemia | Micronutrient Intake | OR | 95% CI | Adjustments |
|---|---|---|---|---|---|
| Folate | |||||
| Bailey et al. [28] | ALL | Energy-adjusted dietary folate (mcg) | Age, sex and state of residence in Australia | ||
| <395 | 1.00 | ||||
| >395 to 454 | 0.68 | 0.44–1.06 | |||
| >454 to 524 | 0.58 | 0.37–0.91 * | |||
| >524 to 624 | 0.44 | 0.27–0.71 * | |||
| >624 | 0.70 | 0.44–1.12 | |||
| Energy-adjusted dietary B6 (mg) | |||||
| <1.39 | 1.00 | ||||
| >1.39 to 1.54 | 1.04 | 0.67–1.62 | |||
| >1.54 to 1.67 | 1.15 | 0.74–1.81 | |||
| >1.67 to 1.85 | 1.28 | 0.82–2.00 | |||
| > 1.85 | 1.60 | 1.02–2.51 * | |||
| Energy-adjusted dietary B12 (mcg) | |||||
| <3.18 | 1.00 | ||||
| >3.18 to 3.75 | 0.72 | 0.47–1.10 | |||
| >3.75 to 4.27 | 0.79 | 0.52–1.21 | |||
| >4.27 to 5.34 | 0.85 | 0.56–1.31 | |||
| >5.34 | 0.49 | 0.31–0.77 * | |||
| Jensen et al. [11] & | ALL | Non-users of vitamin supplements (continuous) | Energy intake, income, miscarriages or stillbirths, exposure to other children at preschools, indoor exposure to insecticide during pregnancy and the proportions of the food | ||
| Folate (dietary folate equivalents) | – | – | |||
| Vitamin B6 (mg) | – | – | |||
| Vitamin B12 (mcg) | – | – | |||
| Alpha carotene (mcg) | 0.66 | 0.42–1.05 | |||
| Total glutathione (mg) | 0.15 | 0.02–0.96 * | |||
| Reduced glutathione (mg) | 0.19 | 0.03–1.07 | |||
| Kwan et al. [14] & | ALL | Median daily intake (continuous) | Energy intake, household income, indoor insecticide exposure during pregnancy and proportion of foods reported as large or extra-large portion size | ||
| Folate (dietary folate equivalents) | 1.02 | 0.71–1.47 | |||
| Vitamin B6 (mg) | 1.12 | 0.73–1.72 | |||
| Vitamin B12 (mcg) | 1.10 | 0.82–1.48 | |||
| Provitamin A carotenoids (mcg) | 0.77 | 0.60–0.98 * | |||
| Alpha-carotene (mcg) | 0.78 | 0.65–0.93 * | |||
| Total glutathione (mg) | 0.48 | 0.25–0.90 * | |||
| Reduced glutathione (mg) | 0.49 | 0.27–0.90 * | |||
| Singer et al. [29] & | ALL | From food only (continuous, one unit change) | Adjusted for parents’ education, household income, maternal age at child’s birth and energy intake. Models for all mothers also adjusted for mother’s ethnicity. Models for nutrient intake from food only also adjusted for intake of B | ||
| Folate (100 dietary folate equivalent/day) | 0.99 | 0.93–1.06 | |||
| Vitamin B6 (1 mg/day) | 0.91 | 0.74–1.12 | |||
| Vitamin B12 (1 mcg/day) | 0.97 | 0.92–1.02 | |||
| AML | From food only (continuous, one unit change) | ||||
| Folate (100 dietary folate equivalent/day) | 0.90 | 0.76–1.07 | |||
| Vitamin B6 (1 mg/day) | 0.47 | 0.23–0.98 * | |||
| Vitamin B12 (1 mcg/day) | 0.86 | 0.73–1.02 |
| Reference | Type of Leukemia | Type of Supplementation (vs. No-Use in the Index Period) | OR | 95% CI | Adjustments |
|---|---|---|---|---|---|
| Case control study | |||||
| Abudaowd et al. [31] | Acute leukemia | Folate | 0.181 | 0.076–0.43 * | Univariate analysis |
| Ajrouche et al. [40] | Acute leukemia | Folic acid (before) | 0.70 | 0.50–1.00 * | Age, gender, birth order, maternal educational and maternal age at child’s birth |
| Folic acid | 0.80 | 0.50–1.20 | |||
| ALL | Folic acid (before) | 0.70 | 0.50–1.10 | ||
| Folic acid (first trimester) | 1.10 | 0.90–1.50 | |||
| Folic acid (second trimester) | 1.10 | 0.90–1.50 | |||
| Folic acid (third trimester) | 1.20 | 0.90–1.60 | |||
| AML | Folic acid (three months before) | 0.40 | 0.10–1.20 | ||
| Folic acid (first trimester) | 1.00 | 0.50–1.70 | |||
| Folic acid (second trimester) | 1.10 | 0.60–2.00 | |||
| Folic acid (third trimester) | 1.20 | 0.70–2.20 | |||
| Amigou et al. [41] | Acute leukemia | Folic acid (pre-conception or first trimester) | 0.30 | 0.20–0.60 * | Age, gender and socioeconomic status |
| Folic acid (second trimester) | 0.60 | 0.30–1.00 * | |||
| Folic acid (third trimester) | 0.30 | 0.10–0.70 * | |||
| Folic acid | 0.40 | 0.30–0.60 * | |||
| Folic acid or multivitamin | 0.60 | 0.50–0.80 | |||
| ALL | Folic acid (pre-conception or first trimester) | 0.30 | 0.20–0.70 * | ||
| Folic acid (second trimester) | 0.60 | 0.30–1.10 | |||
| Folic acid (third trimester) | 0.20 | 0.10–0.80 * | |||
| Folic acid | 0.40 | 0.30–0.60 * | |||
| Folic acid or multivitamin | 0.70 | 0.50–0.90 * | |||
| ANLL | Folic acid (pre-conception or first trimester) | 0.20 | 0.00–1.40 | ||
| Folic acid (second trimester) | 0.50 | 0.10–2.00 | |||
| Folic acid (third trimester) | 0.40 | 0.10–2.80 | |||
| Folic acid | 0.30 | 0.10–0.90 * | |||
| Folic acid or multivitamin | 0.60 | 0.30–1.10 | |||
| Bailey et al. [28] | ALL | Any folate supplement use | 1.05 | 0.75–1.48 | Age, sex and state of residence |
| Any B6 or B12 supplement use | 1.22 | 0.87–1.71 | |||
| Bonaventure et al. [30] | ALL | Iron | 1.36 | 1.14–1.63 * | Year of birth |
| AML | 1.26 | 0.86–1.85 | |||
| Dockerty et al. [42] | ALL | Folic acid (with or without iron) | 1.10 | 0.50–2.70 | Age, sex, marital status and mother’s education |
| Multivitamins | 0.80 | 0.20–3.10 | |||
| Other vitamin or mineral supplements | 1.50 | 0.70–3.10 | |||
| Iron (with or without folic acid) | 1.20 | 0.70–2.10 | |||
| Iron without folic acid | 1.30 | 0.80–2.30 | |||
| Jensen et al. [11] & | ALL | Average daily intake, continuous (before pregnancy) | Total energy intake, income, history of miscarriage or stillbirth, hours of exposure to other children in day care, indoor exposure to insecticide during pregnancy and the proportions of food as great or very large | ||
| Vitamin A | 0.58 | 0.32–0.98 * | |||
| Folic acid | 0.78 | 0.33–1.81 | |||
| Vitamin B6 | 0.84 | 0.41–1.75 | |||
| Vitamin B12 | 0.86 | 0.45–1.45 | |||
| Iron | 0.89 | 0.51–1.53 | |||
| Kwan et al. [35] | Acute leukemia | Iron (3 months before pregnancy and during breastfeeding) | 0.70 | 0.51–0.97 * | Household income, maternal education, maternal age at birth |
| Iron (3 months before and during pregnancy) | 0.76 | 0.52–1.11 | |||
| ALL | Iron (3 months before pregnancy and during breastfeeding) | 0.67 | 0.47–0.94 * | ||
| Iron (3 months before and during pregnancy) | 0.72 | 0.47–1.09 | |||
| Kwan et al. [14] & | ALL | Median daily intake, continuous (before pregnancy) | Adjusted for total energy intake, household income, indoor insecticide exposure during pregnancy and proportion of foods reported as large or extra-large portion size | ||
| Vitamin A | 0.82 | 0.62–1.08 | |||
| Folate | 1.02 | 0.71–1.47 | |||
| Vitamin B6 | 1.12 | 0.73–1.72 | |||
| Vitamin B12 | 1.10 | 0.82–1.48 | |||
| Iron | 1.05 | 0.77–1.44 | |||
| Linabery et al. [36] | ALL | Any prenatal vitamins | 0.63 | 0.34–1.18 | Race/ethnicity, household income |
| Vitamins (periconceptional) | 0.77 | 0.54–1.11 | |||
| Vitamins | 0.66 | 0.39–1.11 | |||
| Vitamins (the year before and during pregnancy) | 0.77 | 0.55–1.09 | |||
| Iron (before pregnancy) | 1.22 | 0.82–1.80 | |||
| Iron (periconceptional) | 1.30 | 0.62–2.72 | |||
| Iron | 1.22 | 0.81–1.84 | |||
| Iron (the year before and during pregnancy) | 3.04 | 0.77–12.03 | |||
| AML | Any prenatal vitamins | 1.20 | 0.53–2.73 | Race/ethnicity, household income | |
| Vitamins (periconceptional) | 1.05 | 0.68–1.61 | |||
| Vitamins | 1.05 | 0.55–2.04 | |||
| Vitamins (the year before and during pregnancy) | 0.88 | 0.60–1.31 | |||
| Iron (before pregnancy) | 0.82 | 0.51–1.33 | |||
| Iron (periconceptional) | 1.26 | 0.55–2.88 | |||
| Iron | 0.77 | 0.46–1.27 | |||
| Iron (the year before and during pregnancy) | 1.72 | 0.33–9.06 | |||
| McKinney et al. [32] | Acute leukemia | Iron supplements | 0.95 | 0.62–1.45 | Maternal age |
| ALL | Iron supplements | 0.80 | 0.51–1.25 | ||
| Milne et al. [43] | ALL | Folate (first trimester) | 1.19 | 0.91–1.56 | Age, sex, residence, ethnicity, education, birth order and maternal age |
| Folate (second and third trimester) | 0.83 | 0.65–1.06 | |||
| Iron (first trimester) | 1.08 | 0.43–2.75 | |||
| Iron (second and third trimester) | 1.04 | 0.57–1.89 | |||
| Ognjanovic et al. [44] | ALL | Multivitamin | 0.71 | 0.51–1.00 * | Child’s year of birth |
| AML | 0.79 | 0.53–1.17 | |||
| Robison et al. [33] | ALL | Vitamins/Iron | 1.00 | 0.51–1.96 | Adjusted for potential confounding factors |
| Schuz et al. [37] | ALL | Vitamins, folate and/or iron | 0.84 | 0.69–1.01 | Sex, age, year of birth, degree of urbanization and socioeconomic status |
| AML | 1.13 | 0.74–1.72 | |||
| Shaw et al. [38] | ALL | Vitamins with folic acid | 1.00 | 0.80–1.20 | Maternal education and maternal age at birth |
| Other vitamins | 1.00 | 0.70–1.30 | |||
| Singer et al. [29] & | ALL | Continuous, unite change (before pregnancy) | Father’s and mother’s education, household income, maternal age at child’s birth and energy intake. Models for all mothers also adjusted for mother’s ethnicity. Models for nutrient intake from food only also adjusted for intake of B vitamin-containing supplements (yes/no) | ||
| Folate (100 dietary folate equivalent/day) | 0.97 | 0.94–1.01 | |||
| Vitamin B12 (1 mg/day) | 0.96 | 0.93–1.00 * | |||
| Vitamin B6 (1 mg/day) | 0.89 | 0.79–1.00 * | |||
| AML | Continuous, unite change (before pregnancy) | ||||
| Folate 100 dietary folate equivalent/day | 0.93 | 0.85–1.03 | |||
| Vitamin B6 1 mg/day | 0.72 | 0.51–1.04 | |||
| Vitamin B12 1 mg/day | 0.92 | 0.84–1.02 | |||
| Thompson et al. [45] | ALL | Folate with or without iron | 0.40 | 0.21–0.73 * | Univariate analysis |
| Iron or folate | 0.37 | 0.21–0.65 * | |||
| Iron and folate | 0.41 | 0.22–0.75 * | |||
| Iron alone | 0.75 | 0.37–1.51 | |||
| Van Steensel-Moll et al. [34] | Acute leukemia | Iron preparations | 1.30 | 0.90–2.00 | Age and sex |
| Wen et al. [39] | ALL | Vitamins | 0.70 | 0.50–1.00 *† | Immuno-phenotype, sex, age, household income, maternal and paternal race, education, smoking and drinking before or during pregnancy |
| Iron supplements | 0.90 | 0.70–1.00 * | |||
| Pooled analysis | |||||
| Metayer et al. [46] | ALL | Folic acid (any time) | 0.80 | 0.71–0.89 * | Age, sex, ethnicity, parental education and study |
| Folic acid (pre-conception) | 0.82 | 0.70–0.96 * | |||
| Folic acid | 0.77 | 0.67–0.88 * | |||
| Folic acid (before and during pregnancy) | 0.78 | 0.78–0.91 * | |||
| Vitamins (any time) | 0.85 | 0.78–0.92 * | |||
| Vitamins (pre-conception) | 0.82 | 0.79–0.99 * | |||
| Vitamins | 0.81 | 0.74–0.88 * | |||
| Vitamins (before and during pregnancy) | 0.78 | 0.69–0.88 * | |||
| AML | Folic acid (any time) | 0.68 | 0.48–0.96 * | ||
| Folic acid (pre-conception) | 0.88 | 0.59–1.32 | |||
| Folic acid | 0.52 | 0.31–0.89 * | |||
| Vitamins (any time) | 0.92 | 0.75–1.14 | |||
| Vitamins (pre-conception) | 0.96 | 0.66–1.39 | |||
| Vitamins | 0.85 | 0.64–1.14 | |||
| Leukemia Type | No. of Studies | References | OR (95% CI) | Heterogeneity I2, p | |
|---|---|---|---|---|---|
| Food group | |||||
| Fruits | Acute leukemia | – | – | – | |
| ALL | 2 | [13,17] | 0.71 (0.59–0.86) | 0%, 0.0003 | |
| AML | – | – | – | ||
| Vegetables | Acute leukemia | – | – | – | |
| ALL | 2 | [13,17] | 0.88 (0.69–1.11) | 69%, 0.28 | |
| AML | – | – | – | ||
| Grains | Acute leukemia | – | – | – | |
| ALL | 2 | [13,17] | 1.22 (0.96–1.56) | 0%, 0.10 | |
| AML | – | – | – | ||
| Dairy products | Acute leukemia | – | – | – | |
| ALL | 2 | [13,17] | 0.92 (0.75–1.12) | 51%, 0.41 | |
| AML | – | – | – | ||
| Processed meat (cured meat) | Acute leukemia | – | – | – | |
| ALL | 2 | [13,17] | 1.01 (0.68–1.51) | 37%, 0.96 | |
| AML | – | – | – | ||
| Non-alcoholic drinks | |||||
| Coffee | Acute leukemia | 5 | [22,24,25,26,27] | 1.36 (0.97–1.91) | 68%, 0.08 |
| ALL | 5 | [20,21,22,23,24] | 1.45 (1.12–1.89) | 35%, 0.005 | |
| AML | 4 | [20,21,22,24] | 1.18 (0.66–2.13) | 45%, 0.56 | |
| Tea | Acute leukemia | 2 | [22,24] | 0.97 (0.80–1.51) | 0%, 0.78 |
| ALL | 4 | [22,23,24] | 0.95 (0.79–1.14) | 0%, 0.56 | |
| AML | 2 | [22,24] | 1.00 (0.73–1.37) | 0%, 1.00 | |
| Soft drinks | Acute leukemia | 2 | [16,22] | 1.23 (0.97–1.55) | 0%, 0.08 |
| ALL | – | – | – | ||
| AML | – | – | – | ||
| Supplements | |||||
| Folic Acid | Acute leukemia | 2 | [40,41] | 0.55 (0.28–1.09) | 84%, 0.08 |
| ALL | 6 | [28,29,40,41,43,45] | 0.77 (0.59–1.01) | 89%, 0.06 | |
| AML | 3 | [29,40,41] | 0.87 (0.56–1.36) | 59%, 0.54 | |
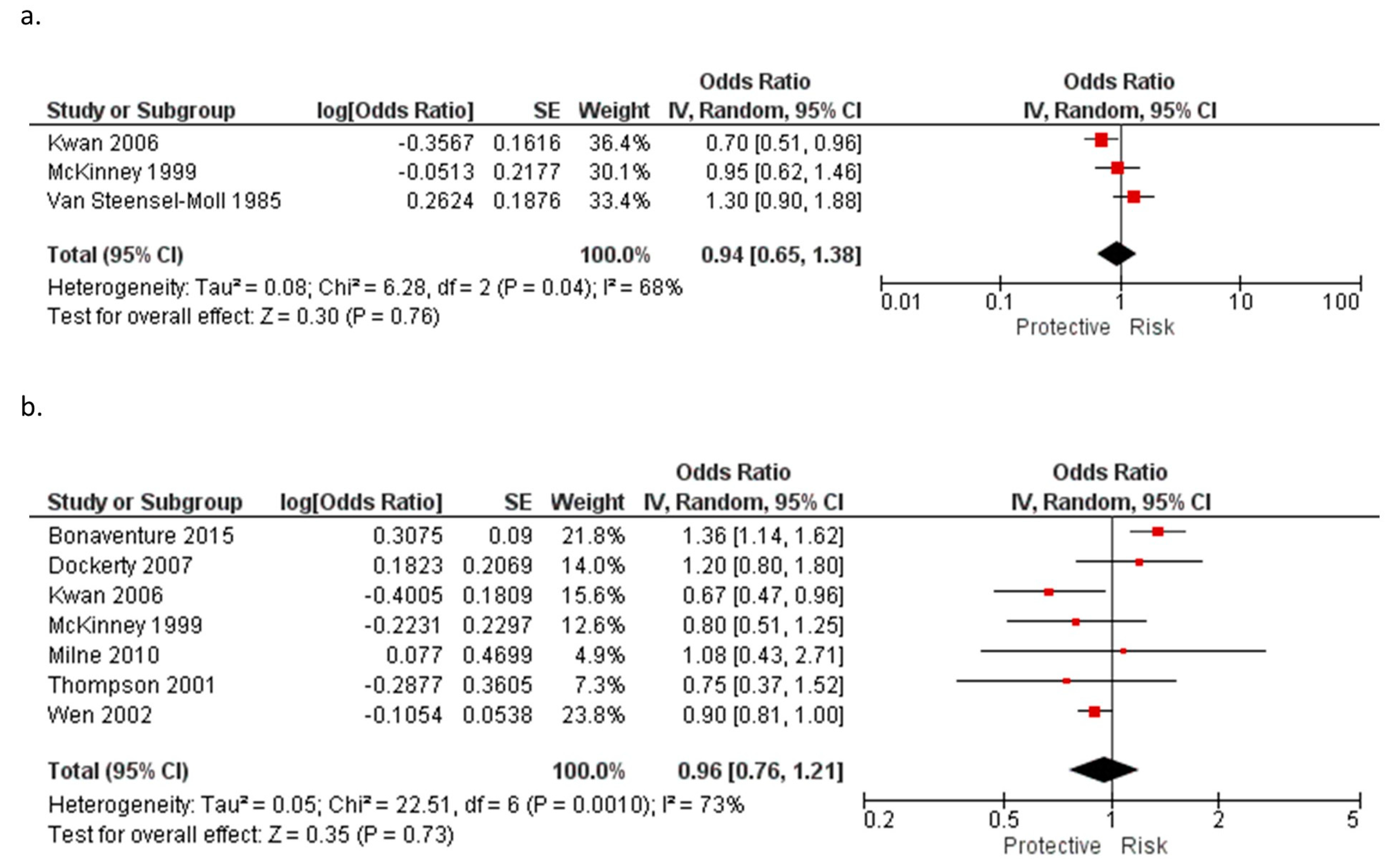
| Iron | Acute leukemia | 3 | [32,34,35] | 0.94 (0.65–1.38) | 68%, 0.30 |
| ALL | 7 | [30,32,35,39,42,43,44] | 0.96 (0.76–1.21) | 73%, 0.35 | |
| AML | – | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanco-Lopez, J.; Iguacel, I.; Pisanu, S.; Almeida, C.C.B.; Steliarova-Foucher, E.; Sierens, C.; Gunter, M.J.; Ladas, E.J.; Barr, R.D.; Van Herck, K.; et al. Role of Maternal Diet in the Risk of Childhood Acute Leukemia: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 5428. https://doi.org/10.3390/ijerph20075428
Blanco-Lopez J, Iguacel I, Pisanu S, Almeida CCB, Steliarova-Foucher E, Sierens C, Gunter MJ, Ladas EJ, Barr RD, Van Herck K, et al. Role of Maternal Diet in the Risk of Childhood Acute Leukemia: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(7):5428. https://doi.org/10.3390/ijerph20075428
Chicago/Turabian StyleBlanco-Lopez, Jessica, Isabel Iguacel, Silvia Pisanu, Claudia Choma Bettega Almeida, Eva Steliarova-Foucher, Ciska Sierens, Marc J. Gunter, Elena J. Ladas, Ronald D. Barr, Koen Van Herck, and et al. 2023. "Role of Maternal Diet in the Risk of Childhood Acute Leukemia: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 7: 5428. https://doi.org/10.3390/ijerph20075428