
The Role of Health Behaviors in Quality of Life: A Longitudinal Study of Patients with Colorectal Cancer
 ,
,
Abstract
:1. Introduction
2. Method
2.1. Materials and Methods
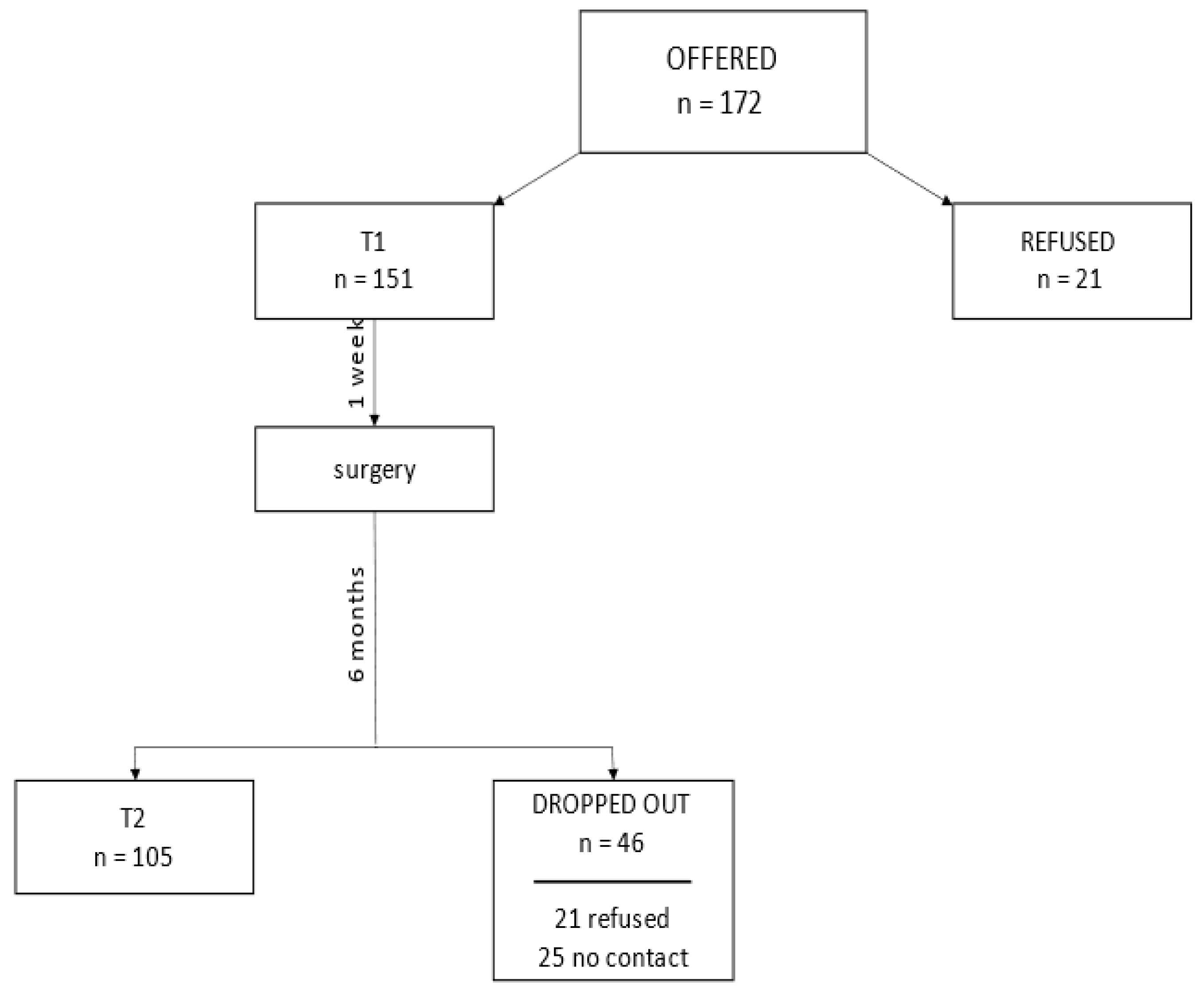
Sampling
2.2. Measures
2.2.1. Health-Related Behaviors
2.2.2. Quality of Life
2.2.3. Demographics and Medical Data
2.3. Study Procedure
2.4. Participants
2.5. Statistical Analyses
2.6. Ethical Approval
3. Results
4. Discussion
4.1. Limitations
4.2. Implications for Research and Practice
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| QoL | Quality of Life |
| CRC | Colorectal Cancer |
| ERAS | Enhanced Recovery After Surgery |
| FOLFOX | a combination of chemotherapy drugs (folinic acid, fluorouracil, and oxaliplatin) |
| BMI | Body Mass Index |
| EHIS | European Health Interview Survey |
| EORTC QLQ-C30 questionnaire | European Organization for Research and Treatment of Cancer Quality of Life Questionnaire |
| CTx | chemotherapy |
| RT | radiotherapy |
| LH | laparoscopic hemicolectomy |
| LAR | low rectal anterior resection, |
| APR | abdominoperineal resection |
| FCR | Fear of Cancer Recurrence |
| KRN | National Cancer Registry in Poland |
References
- The World Health Organization quality of life assessment (WHOQOL): Position paper from the World Health Organization. Soc. Sci. Med. 1995, 41, 1403–1409. [CrossRef] [PubMed]
- Bullinger, M. Lebensqualitätsforschung: Bedeutung—Anforderungen—Akzeptanz; Schattauer: Stuttgart, Germany, 1997. [Google Scholar]
- Wang, C.C.; Sung, W.W.; Yan, P.Y.; Ko, P.Y.; Tsai, M.C. Favorable colorectal cancer mortality-to-incidence ratios in countries with high expenditures on health and development index: A study based on GLOBOCAN database. Medicine 2021, 100, e27414. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.; Arnold, M.; Gini, A.; Lorenzoni, V.; Cabasag, C.J.; Laversanne, M.; Vignat, J.; Ferlay, J.; Murphy, N.; Bray, F. Global burden of colorectal cancer in 2020 and 2040: Incidence and mortality estimates from GLOBOCAN. Published online September 8, 2022:gutjnl-2022. Gut 2023, 72, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Jaroszyńska, Z.; Wiśniewska, K. Epidemiologia raka jelita grubego (C18-C21) w Polsce. J. Educ. Health Sport. 2021, 11, 143–156. [Google Scholar] [CrossRef]
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) [Continuous Update Project report]: Diet, Nutrition, Physical Activity, and Colorectal Cancer, 2016; World Cancer Research Fund International: London, UK, 2018.
- Zaytseva, Y. Lipid metabolism as a targetable metabolic vulnerability in colorectal cancer. Cancers 2021, 13, 301. [Google Scholar] [CrossRef]
- Silva, A.; Faria, G.; Araújo, A.; Monteiro, M.P. Impact of adiposity on staging and prognosis of colorectal cancer. Crit. Rev. Oncol. Hematol. 2020, 145, 102857. [Google Scholar] [CrossRef]
- Win, A.K.; Macinnis, R.J.; Hopper, J.L.; Jenkins, M.A. Risk prediction models for colorectal cancer: A review. Cancer Epidemiol. Biomark. Prev. 2012, 21, 398–410. [Google Scholar] [CrossRef] [Green Version]
- Amersi, F.; Agustin, M.; Ko, C.Y. Colorectal cancer: Epidemiology, risk factors, and health services. Clin. Colon. Rect. Surg. 2005, 18, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Fearon, K.C.H.; Ljungqvist, O.; Von Meyenfeldt, M.; Revhaug, A.; Dejong, C.H.; Lassen, K.; Nygren, J.; Hausel, J.; Soop, M.; Andersen, J.; et al. Enhanced recovery after surgery: A consensus review of clinical care for patients undergoing colonic resection. Clin. Nutr. 2005, 24, 466–477. [Google Scholar] [CrossRef]
- Gustafsson, U.O.; Scott, M.J.; Hubner, M.; Nygren, J.; Demartines, N.; Francis, N.; Rockall, T.A.; Young-Fadok, T.M.; Hill, A.G.; Soop, M.; et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced recovery after surgery (ERAS®) society recommendations: 2018. World J. Surg. 2019, 43, 659–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Rooijen, S.; Carli, F.; Dalton, S.O.; Johansen, C.; Dieleman, J.; Roumen, R.; Slooter, G. Preoperative modifiable risk factors in colorectal surgery: An observational cohort study identifying the possible value of prehabilitation. Acta Oncol. 2017, 56, 329–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovell, M.; Corbett, M.; Dong, S.; Siddall, P. Spiritual well-being in people living with persistent non-cancer and cancer-related pain. Pain Med. 2021, 22, 1345–1352. [Google Scholar] [CrossRef] [PubMed]
- Park, C.L. Meaning making following trauma. Front. Psychol. 2022, 23, 844891. [Google Scholar] [CrossRef]
- Krok, D.; Telka, E.; Zarzycka, B. Modeling psychological well-being among abdominal and pelvic cancer patients: The roles of total pain, meaning in life, and coping. Psycho-Oncol. 2022, 31, 1852–1859. [Google Scholar] [CrossRef]
- Lewis, C.; Xun, P.; He, K. Vitamin D supplementation and quality of life following diagnosis in stage II colorectal cancer patients: A 24-month prospective study. Support. Care Cancer 2016, 24, 1655–1661. [Google Scholar] [CrossRef]
- Gigic, B.; Boeing, H.; Toth, R.; Böhm, J.; Habermann, N.; Scherer, D.; Schrotz-King, P.; Abbenhardt-Martin, C.; Skender, S.; Brenner, H.; et al. Associations between dietary patterns and longitudinal quality of life changes in colorectal cancer patients: The ColoCare study. Nutr. Cancer 2018, 70, 51–60. [Google Scholar] [CrossRef]
- Grimmett, C.; Bridgewater, J.; Steptoe, A.; Wardle, J. Lifestyle and quality of life in colorectal cancer survivors. Qual. Life Res. 2011, 20, 1237–1245. [Google Scholar] [CrossRef]
- Lewis, C.; Xun, P.; He, K. Physical activity in relation to quality of life in newly diagnosed colon cancer patients: A 24-month follow-up. Qual. Life Res. 2014, 23, 2235–2246. [Google Scholar] [CrossRef]
- Ray, A.D.; Twarozek, A.M.; Williams, B.T.; Erwin, D.O.; Underwood, W., 3rd; Mahoney, M.C. Exercise in African American and white colorectal cancer survivors: A mixed methods approach. Rehabil. Oncol. 2018, 36, 188–197. [Google Scholar] [CrossRef]
- Chambers, S.K.; Meng, X.; Youl, P.; Aitken, J.; Dunn, J.; Baade, P. A five-year prospective study of quality of life after colorectal cancer. Qual. Life Res. 2012, 21, 1551–1564. [Google Scholar] [CrossRef]
- Hsu, H.T.; Wu, L.M.; Lin, P.C.; Juan, C.H.; Huang, Y.Y.; Chou, P.L.; Chen, J.L. Emotional distress and quality of life during folinic acid, fluorouracil, and oxaliplatin in colorectal cancer patients with and without chemotherapy-induced peripheral neuropathy: A cross-sectional study. Medicine 2020, 99, e19029. [Google Scholar] [CrossRef]
- Röhrl, K.; Guren, M.G.; Astrup, G.L.; Småstuen, M.C.; Rustøen, T. High symptom burden is associated with impaired quality of life in colorectal cancer patients during chemotherapy:A prospective longitudinal study. Eur. J. Oncol. Nurs. 2020, 44, 101679. [Google Scholar] [CrossRef] [Green Version]
- Tarkowska, M.; Głowacka-Mrotek, I.; Skonieczny, B.; Jankowski, M.; Nowikiewicz, T.; Jarzemski, M.; Zegarski, W.; Jarzemski, P. Prospective evaluation of the quality of life of patients after surgical treatment of rectal cancer: A 12-month cohort observation. J. Clin. Med. 2022, 11, 5912. [Google Scholar] [CrossRef]
- Piekarzewska, M.; Wieczorkowski, R.; Zajenkowska-Kozłowska, A. Health status of population in Poland in 2014. Available online: https://stat.gov.pl/obszary-tematyczne/zdrowie/zdrowie/stan-zdrowia-ludnosci-polski-w-2014-r-,6,6.html (accessed on 20 March 2020).
- Johnson, C.M.; Wei, C.; Ensor, J.E.; Smolenski, D.J.; Amos, C.I.; Levin, B.; Berry, D.A. Meta-analyses of colorectal cancer risk factors. Cancer Causes Control. 2013, 24, 1207–1222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nashar, R.M.; Almurshed, K.S. Colorectal cancer: A case control study of dietary factors, king Faisal specialist hospital and researh center, Riyadh, Saudi arabia. J. Family Community Med. 2008, 15, 57–64. [Google Scholar]
- Gonzalez, C.A. The European prospective investigation into cancer and nutrition (EPIC). Public Health Nutr. 2006, 9, 124–126. [Google Scholar] [CrossRef] [Green Version]
- Norat, T.; Bingham, S.; Ferrari, P.; Slimani, N.; Jenab, M.; Mazuir, M.; Overvad, K.; Olsen, A.; Tjønneland, A.; Clavel, F.; et al. Meat, fish, and colorectal cancer risk: The European prospective investigation into cancer and nutrition. J. Natl. Cancer Inst. 2005, 97, 906–916. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C. The European Organization for Research and Treatment of Cancer QLQ-C30: A quality-of-life instrument for use in international clinical trials in oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Field, A. Discovering Statistics Using IBM SPSS Statistic; SAGE Publications Ltd.: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Nduaguba, S.O.; Ford, K.H.; Rascati, K. The role of physical activity in the association between smoking status and quality of life. Nicotine Tob. Res. 2019, 21, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, M.; Danovitch, I.; IsHak, W.W. Quality of life and smoking. Am. J. Addict. 2014, 23, 540–562. [Google Scholar] [CrossRef]
- Moayeri, F.; Hsueh, Y.A.; Dunt, D.; Clarke, P. Smoking Cessation and quality of life: Insights from analysis of longitudinal Australian data, an application for economic evaluations. Value Health 2021, 24, 724–732. [Google Scholar] [CrossRef]
- Grover, K.W.; Goodwin, R.D.; Zvolensky, M.J. Does current versus former smoking play a role in the relationship between anxiety and mood disorders and nicotine dependence? Addict. Behav. 2012, 37, 682–685. [Google Scholar] [CrossRef]
- Mojtabai, R.; Crum, R.M. Cigarette smoking and onset of mood and anxiety disorders. Am. J. Public Health 2013, 103, 1656–1665. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, N.A.; Berkowitz, Z.; Rodriguez, J.L. Awareness of dietary and alcohol guidelines among colorectal cancer survivors. Am. J. Prev. Med. 2015, 49 (Suppl. S5), S509–S517. [Google Scholar] [CrossRef] [Green Version]
- Lewis, C.M.; Wolf, W.A.; Xun, P.; Sandler, R.S.; He, K. Racial differences in dietary changes and quality of life after a colorectal cancer diagnosis: A follow-up of the Study of Outcomes in Colorectal Cancer Survivors cohort. Am. J. Clin. Nutr. 2016, 103, 1523–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyman, B.A. Psychology of Food: More Than a Matter of Taste; Van Nostrand Reinhold: New York, NY, USA, 1989. [Google Scholar]
- Fujisawa, D.; Umezawa, S.; Basaki-Tange, A.; Fujimori, M.; Miyashita, M. Smoking status, service use and associated factors among Japanese cancer survivors—A web-based survey. Support. Care Cancer 2014, 22, 3125–3134. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, N.A.; Smith, T.; Zhao, L.; Rodriguez, J.; Berkowitz, Z.; Stein, K.D. Health-related behavior change after cancer: Results of the American Cancer Society’s studies of cancer survivors (SCS). J. Cancer Surviv. 2010, 4, 20–32. [Google Scholar] [CrossRef]
- Koch-Gallenkamp, L.; Bertram, H.; Eberle, A.; Holleczek, B.; Schmid-Höpfner, S.; Waldmann, A.; Zeissig, S.R.; Brenner, H.; Arndt, V. Fear of recurrence in long-term cancer survivors-Do cancer type, sex, time since diagnosis, and social support matter? Health Psychol. 2016, 35, 1329–1333. [Google Scholar] [CrossRef]
- Chen, T.Y.T.; Wiltink, L.M.; Nout, R.A.; Meershoek-Klein Kranenbarg, E.; Laurberg, S.; Marijnen, C.A.; van de Velde, C.J. Bowel function 14 years after preoperative short-course radiotherapy and total mesorectal excision for rectal cancer: Report of a multicenter randomized trial. Clin. Colorectal Cancer 2015, 14, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Hendren, S.K.; O’Connor, B.I.; Liu, M.; Asano, T.; Cohen, Z.; Swallow, C.J.; Macrae, H.M.; Gryfe, R.; McLeod, R.S. Prevalence of male and female sexual dysfunction is high following surgery for rectal cancer. Ann. Surg. 2005, 242, 212–223. [Google Scholar] [CrossRef]
- Ledebo, A.; Bock, D.; Prytz, M.; Haglind, E.; Angenete, E. Urogenital function 3 years after abdominoperineal excision for rectal cancer. Color. Dis. 2018, 20, O123–O134. [Google Scholar] [CrossRef] [Green Version]
- Monastyrska, E.; Hagner, W.; Jankowski, M.; Głowacka, I.; Zegarska, B.; Zegarski, W. Prospective assessment of the quality of life in patients treated surgically for rectal cancer with lower anterior resection and abdominoperineal resection. Eur. J. Surg. Oncol. 2016, 42, 1647–1653. [Google Scholar] [CrossRef] [PubMed]
- Akechi, T.; Uchida, M.; Nakaguchi, T.; Okuyama, T.; Sakamoto, N.; Toyama, T.; Yamashita, H. Difference of patient’s perceived need in breast cancer patients after diagnosis. Jpn. J. Clin. Oncol. 2015, 45, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Buczkowski, K.; Marcinowicz, L.; Czachowski, S.; Piszczek, E.; Sowinska, A. ‘What kind of general practitioner do I need for smoking cessation?’ Results from a qualitative study in Poland. BMC Fam. Pract. 2013, 14, 159. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.J.; Mottershead, T.A.; Ronksley, P.E.; Sigal, R.J.; Campbell, T.S.; Hemmelgarn, B.R. Motivational interviewing to improve weight loss in overweight and/or obese patients: A systematic review and meta-analysis of randomized controlled trials. Obes. Rev. 2011, 12, 709–723. [Google Scholar] [CrossRef] [PubMed]
- Report from the Polish National Cancer Registry C18–C21. Available online: http://onkologia.org.pl/nowotwory-zlosliwe-jelita-grubego-c18-21/#q (accessed on 31 October 2019).
- Hulbert-Williams, N.; Neal, R.; Morrison, V.; Hood, K.; Wilkinson, C. Anxiety, depression and quality of life after cancer diagnosis: What psychosocial variables best predict how patients adjust? Psycho. Oncol. 2012, 21, 857–867. [Google Scholar] [CrossRef]


{kind=link}
| T1 Before Surgery | T2 Half a Year after Surgery | |||
|---|---|---|---|---|
| Number | % | Number | % | |
| Age (years (SD)) Men (years (SD)) Women (years (SD)) | 64.89 (10.14) 65.21 (10.73) 64.27 (9.86) | 64.30 (10.51) 64.15 (10.20) 64.62 (11.29) | ||
| Gender Men Women | 100 51 | 66.23 33.77 | 71 34 | 67.62 32.38 |
| Place of residence: City Country | 101 50 | 66.89 33.11 | 65 40 | 61.90 38.10 |
| Marital status Single Married Widowed Divorced | 7 115 24 5 | 4.64 76.16 15.89 3.31 | 5 82 16 2 | 4.76 78.10 15.24 1.90 |
| Education Primary Vocational Secondary Higher | 22 52 54 23 | 14.57 34.44 35.76 15.23 | 12 37 37 19 | 11.43 35.24 35.24 18.09 |
| Absence of concomitant illnesses Concomitant illnesses | 74 77 | 49.01 50.99 | 50 55 | 47.62 52.38 |
| Cancer Colon Rectosigmoid junction Rectum and anal canal Of colon or rectum of uncertain/unknown origin | 51 17 73 10 | 33.77 11.26 48.34 6.62 | 37 13 48 7 | 35.24 12.38 45.71 6.67 |
| Neoadjuvant therapy Not applied Chemotherapy Radiotherapy Chemo-radiotherapy | 90 2 21 38 | 59.60 1.32 13.91 25.17 | 66 2 15 22 | 62.86 1.90 14.29 20.95 |
| Adjuvant therapy Not applied Chemotherapy Radiotherapy Chemo-radiotherapy | 86 56 1 8 | 56.95 37.09 0.01 5.30 | 59 43 0 3 | 56.19 40.95 0.00 2.86 |
| Kind of surgery Laparoscopic hemicolectomy Low rectal anterior resection Abdominoperineal resection | 48 69 34 | 31.79 45.70 22.52 | 33 52 20 | 31.43 49.52 19.05 |
| The range of the spread of cancer 0 I II III IV | 9 30 42 67 3 | 5.96 19.87 27.81 44.37 1.99 | 5 21 33 44 2 | 4.76 20.00 31.43 49.90 1.90 |
| T1 (n = 151) | T2 (n = 105) | Comparing the Change between T1 and T2 F(dt), p, η2 (n = 105) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| M | SD | Min | Max | M | SD | Min | Max | ||
| Number of cigarettes (items/day) | 2.12 | 5.65 | 0.00 | 20.00 | 1.48 | 5.40 | 0.00 | 40.00 | F(1,104) = 1.83; p = 0.180; η2 = 0.02 |
| Alcohol consumption (portions/week) | 1.20 | 4.74 | 0.00 | 45.50 | 0.80 | 2.40 | 0.00 | 14.00 | F(1,104) = 2.68; p = 0.012.; η2 = 0.06 |
| Frequency of consuming healthy food | 15.01 | 3.25 | 5.00 | 22.00 | 15.69 | 2.64 | 7.00 | 21.00 | F(1,104) = 0.19; p = 0.663.; η2 = 0.002 |
| Physical activity (minutes/week) | 388.61 | 308.28 | 0.00 | 1680.00 | 319.43 | 206.71 | 0.00 | 1065.00 | F(1,104) = 6.55; p = 0.012; η2 = 0.06 |
| Global QoL | 63.58 | 19.21 | 0.00 | 100.00 | 67.67 | 19.62 | 16.67 | 100.00 | F(1,104) = 1.73; p = 0.192.; η2 = 0.02 |
| Physical functioning | 83.84 | 16.17 | 6.67 | 100.00 | 80.44 | 19.13 | 6.67 | 100.00 | F(1,104) = 10.16; p = 0.002.; η2 = 0.09 |
| Role-related functioning | 85.76 | 23.76 | 0.00 | 100.00 | 82.06 | 24.32 | 0.00 | 100.00 | F(1,104) = 4.86; p = 0.029.; η2 = 0.05 |
| Emotional functioning | 75.37 | 23.44 | 0.00 | 100.00 | 89.06 | 12.68 | 41.67 | 100.00 | F(1,104) = 36.29; p < 0.001; η2 = 0.26 |
| Cognitive functioning | 84.55 | 20.01 | 0.00 | 100.00 | 86.98 | 15.67 | 33.33 | 100.00 | F(1,104) = 2.09; p = 0.151; η2 = 0.02 |
| Social functioning | 86.98 | 17.64 | 0.00 | 100.00 | 88.57 | 17.50 | 33.33 | 100.00 | F(1,104) = 0.32; p = 0.571; η2 < 0.01 |
| Fatigue | 27.08 | 24.16 | 0.00 | 100.00 | 24.23 | 21.23 | 0.00 | 100.00 | F(1,104) = 0.58; p = 0.446; η2 = 0.01 |
| Pain | 19.09 | 24.97 | 0.00 | 100.00 | 14.29 | 21.49 | 0.00 | 100.00 | F(1,104) = 3.00; p = 0.086; η2 = 0.03 |
| Type of Surgery | The Stoma Application | |||||
|---|---|---|---|---|---|---|
| Laparoscopic Hemicolectomy | Low Rectal Anterior Resection | Abdominoperineal Resection | Without a Stoma | Applied Stoma | ||
| n = 33 | n = 52 | n = 20 | n = 67 | n = 38 | ||
| Global QoL | M (SD) | 66.41 (20.46) | 68.59 (18.64) | 65.83 (21.44) | 68.91 (18.49) | 64.69 (21.44) |
| H(2,105) = 0.31; p = 0.857 | U = 1122.50; p = 0.317 | |||||
| Physical functioning | M (SD) | 79.60 (16.58) | 80.64 (20.34) | 81.33 (20.70) | 80.80 (18.48) | 79.82 (20.47) |
| H(2,105) = 0.97; p = 0.615 | U = 1272.50; p = 1.00 | |||||
| Role functioning | M (SD) | 79.29 (25.01) | 82.69 (24.47) | 85.00 (23.51) | 82.34 (22.64) | 81.58 (27.34) |
| H(2,105) = 1.41; p = 0.494 | U = 1229.00; p = 0.772 | |||||
| Emotional functioning | M (SD) | 86.36 (14.85) | 90.71 (10.90) | 89.17 (12.99) | 89.30 (12.96) | 88.60 (12.32) |
| H(2,105) = 1.54; p = 0.463 | U = 1228.00; p = 0.767 | |||||
| Cognitive functioning | M (SD) | 88.38 (14.72) | 86.22 (15.38) | 86.67 (18.42) | 86.57 (14.86) | 87.72 (17.19) |
| H(2,105) = 0.41; p = 0.816 | U = 1165.50; p = 0.713 | |||||
| Social functioning | M (SD) | 87.37 (19.11) | 87.50 (18.04) | 93.33 (12.57) | 88.81 (16.76) | 88.16 (18.95) |
| H(2,105) = 1.77; p = 0.413 | U = 1263.00; p = 0.949 | |||||
| Variables | T1; R2 =.21; R2 Adjusted = 0.18 F(5,142) = 7.52; p < 0.001 VIF = 5.34 | Variables | T2; R2 = 0.27; R2 Adjusted = 0.22 F(5,93) = 6.90; p < 0.001 VIF = 5.70 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE β | t | p | R2 | β | SE β | t | p | R2 | ||
| Absolute term | 9.82 | <0.001 | Absolute term | 5.48 | <0.001 | ||||||
| Number of cigarettes (items/day) | −0.18 | 0.08 | −2.34 | 0.020 | 0.04 | Number of cigarettes (items/day) | −0.13 | 0.10 | −1.29 | 0.200 | 0.02 |
| Alcohol intake (portions/week) | 0.08 | 0.08 | 1.12 | 0.266 | <0.01 | Alcohol intake (portions/week) | 0.06 | 0.10 | 0.58 | 0.566 | <0.01 |
| Frequency of consuming healthy food | 0.22 | 0.08 | 2.81 | 0.006 | 0.04 | Frequency of consuming healthy food | 0.19 | 0.09 | 2.02 | 0.046 | 0.03 |
| Physical activity (minutes/week) | 0.26 | 0.08 | 3.37 | <0.001 | 0.10 | Physical activity (minutes/week) | 0.41 | 0.09 | 4.60 | <0.001 | 0.19 |
| Neoadjuvant therapy | −0.18 | 0.08 | −2.54 | 0.012 | 0.03 | Adjuvant therapy | −0.19 | 0.09 | −2.09 | 0.039 | 0.02 |
| Variables | T1; R2 =.28; R2 Adjusted = 0.25 F(5,138) = 10.52; p < 0.001 VIF = 5.25 | Variables | T2; R2 = 0.24; R2 Adjusted = 0.20 F(5,94) = 6.10; p < 0.001 VIF = 5.44 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE β | t | p | R2 | β | SE β | t | p | R2 | ||
| Absolute term | 14.75 | <0.001 | Absolute term | 11.57 | <0.001 | ||||||
| Number of cigarettes (items/day) | −0.36 | 0.08 | −4.81 | <0.001 | 0.11 | Number of cigarettes (items/day) | −0.34 | 0.10 | −3.47 | <0.001 | 0.08 |
| Alcohol intake (portions/week) | 0.10 | 0.08 | 1.42 | 0.159 | 0.01 | Alcohol intake (portions/week) | 0.14 | 0.10 | 1.44 | 0.154 | 0.02 |
| Frequency of consuming healthy food | 0.33 | 0.08 | 4.32 | <0.001 | 0.09 | Frequency of consuming healthy food | 0.31 | 0.10 | 3.41 | <0.001 | 0.10 |
| Physical activity (minutes/week) | 0.19 | 0.08 | 2.62 | 0.010 | 0.04 | Physical activity (minutes/week) | 0.21 | 0.09 | 2.34 | 0.021 | 0.04 |
| Neoadjuvant therapy | −0.18 | 0.08 | 2.39 | 0.018 | 0.03 | Adjuvant therapy | −0.02 | 0.09 | −0.22 | 0.823 | <0.01 |
| Variables | T1; R2 =.22; R2 Adjusted = 0.20 F(5,145) = 8.31; p < 0.001 VIF = 5.25 | Variables | T2; R2 = 0.16; R2 Adjusted = 0.12 F(5,97) = 3.82; p < 0.001 VIF = 5.55 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| β | SE β | t | p | R2 | β | SE β | t | p | R2 | ||
| Absolute term | 8.94 | <0.001 | Absolute term | 22.15 | <0.001 | ||||||
| Number of cigarettes (items/day) | −0.38 | 0.08 | −5.03 | <0.001 | 0.09 | Number of cigarettes (items/day) | −0.31 | 0.10 | −3.00 | 0.003 | 0.03 |
| Alcohol consumption (portions/week) | 0.09 | 0.08 | 1.26 | 0.210 | <0.01 | Alcohol consumption (portions/week) | 0.20 | 0.10 | 2.01 | 0.047 | 0.03 |
| Frequency of consuming healthy food | 0.29 | 0.08 | 3.81 | <0.001 | 0.09 | Frequency of consuming healthy food | 0.21 | 0.09 | 2.22 | 0.029 | 0.05 |
| Physical activity (minutes/week) | 0.05 | 0.08 | 0.71 | 0.480 | <0.01 | Physical activity (minutes/week) | 0.01 | 0.09 | 0.05 | 0.957 | <0.01 |
| Neoadjuvant therapy | −0.19 | 0.08 | 2.57 | 0.011 | 0.04 | Adjuvant therapy | −0.21 | 0.10 | −3.00 | 0.003 | 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ocalewski, J.; Jankowski, M.; Zegarski, W.; Migdalski, A.; Buczkowski, K. The Role of Health Behaviors in Quality of Life: A Longitudinal Study of Patients with Colorectal Cancer. Int. J. Environ. Res. Public Health 2023, 20, 5416. https://doi.org/10.3390/ijerph20075416
Ocalewski J, Jankowski M, Zegarski W, Migdalski A, Buczkowski K. The Role of Health Behaviors in Quality of Life: A Longitudinal Study of Patients with Colorectal Cancer. International Journal of Environmental Research and Public Health. 2023; 20(7):5416. https://doi.org/10.3390/ijerph20075416
Chicago/Turabian StyleOcalewski, Jaroslaw, Michał Jankowski, Wojciech Zegarski, Arkadiusz Migdalski, and Krzysztof Buczkowski. 2023. "The Role of Health Behaviors in Quality of Life: A Longitudinal Study of Patients with Colorectal Cancer" International Journal of Environmental Research and Public Health 20, no. 7: 5416. https://doi.org/10.3390/ijerph20075416