

The Effects of a 12-Week-Long Sand Exercise Training Program on Neuromechanical and Functional Parameters in Type II Diabetic Patients with Neuropathy
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
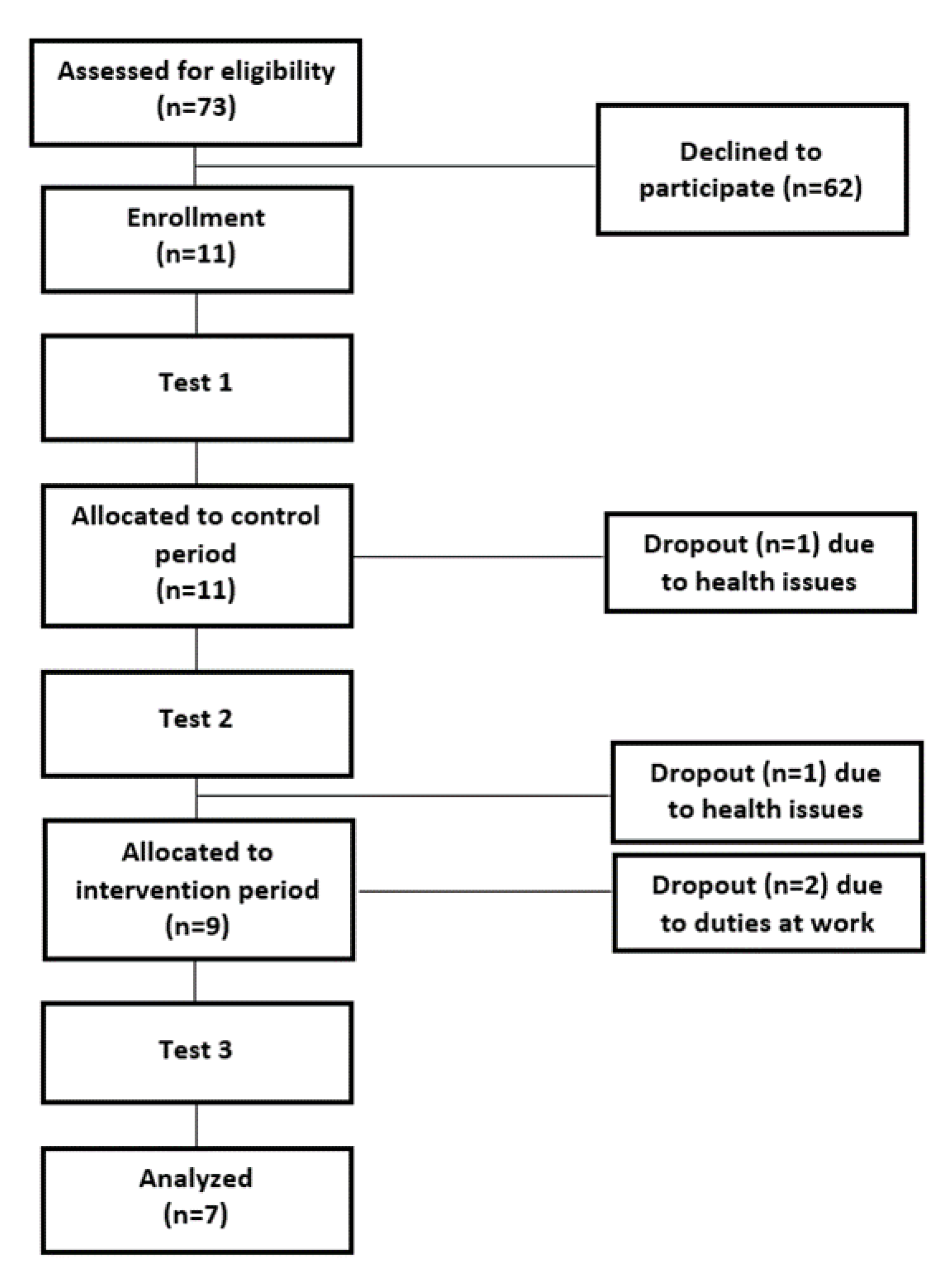
2.1. Participants
2.2. Experimental Protocol
2.3. Body Composition
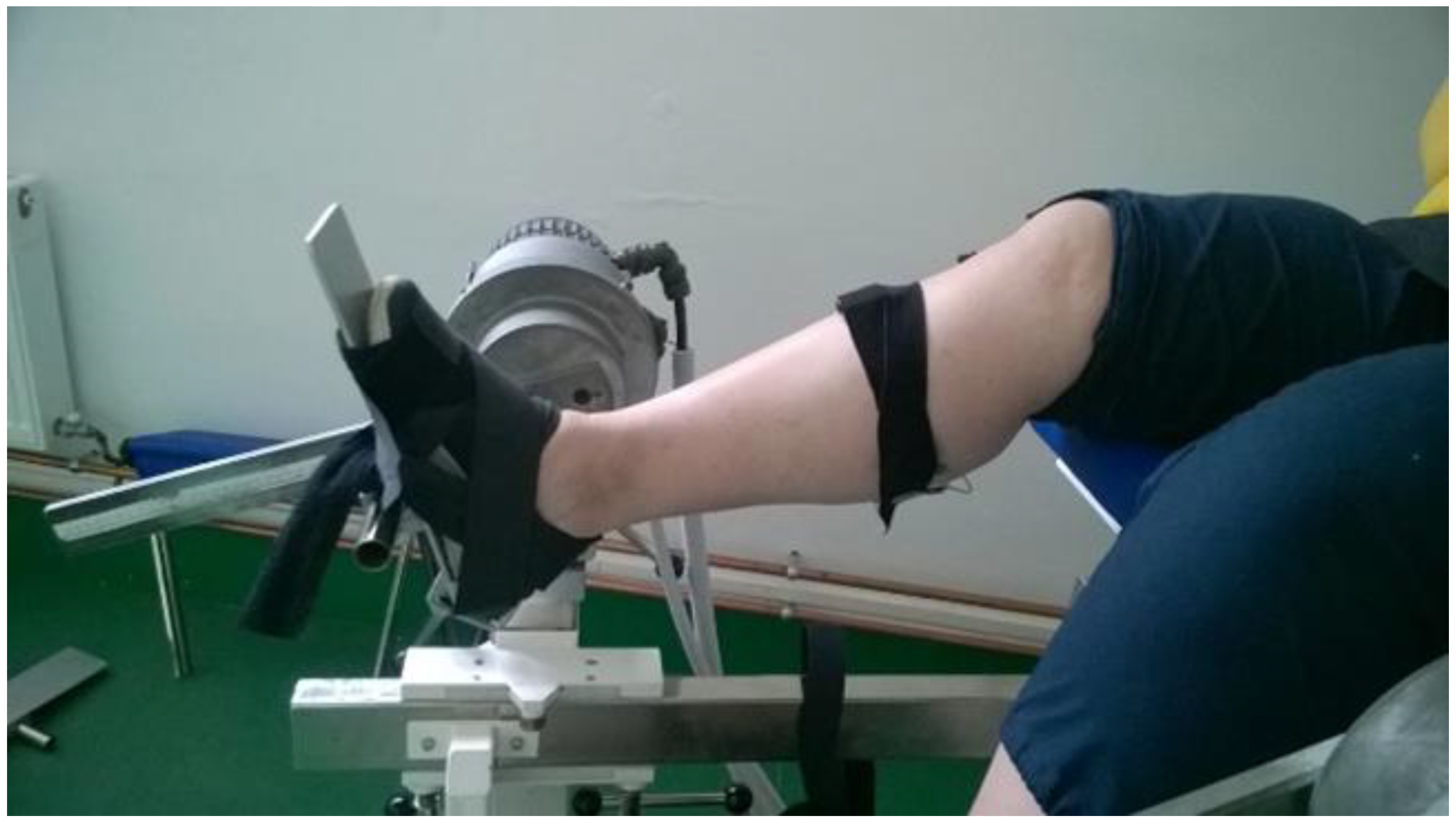
2.4. Maximal Voluntary Isometric Contraction (MVIC) Testing
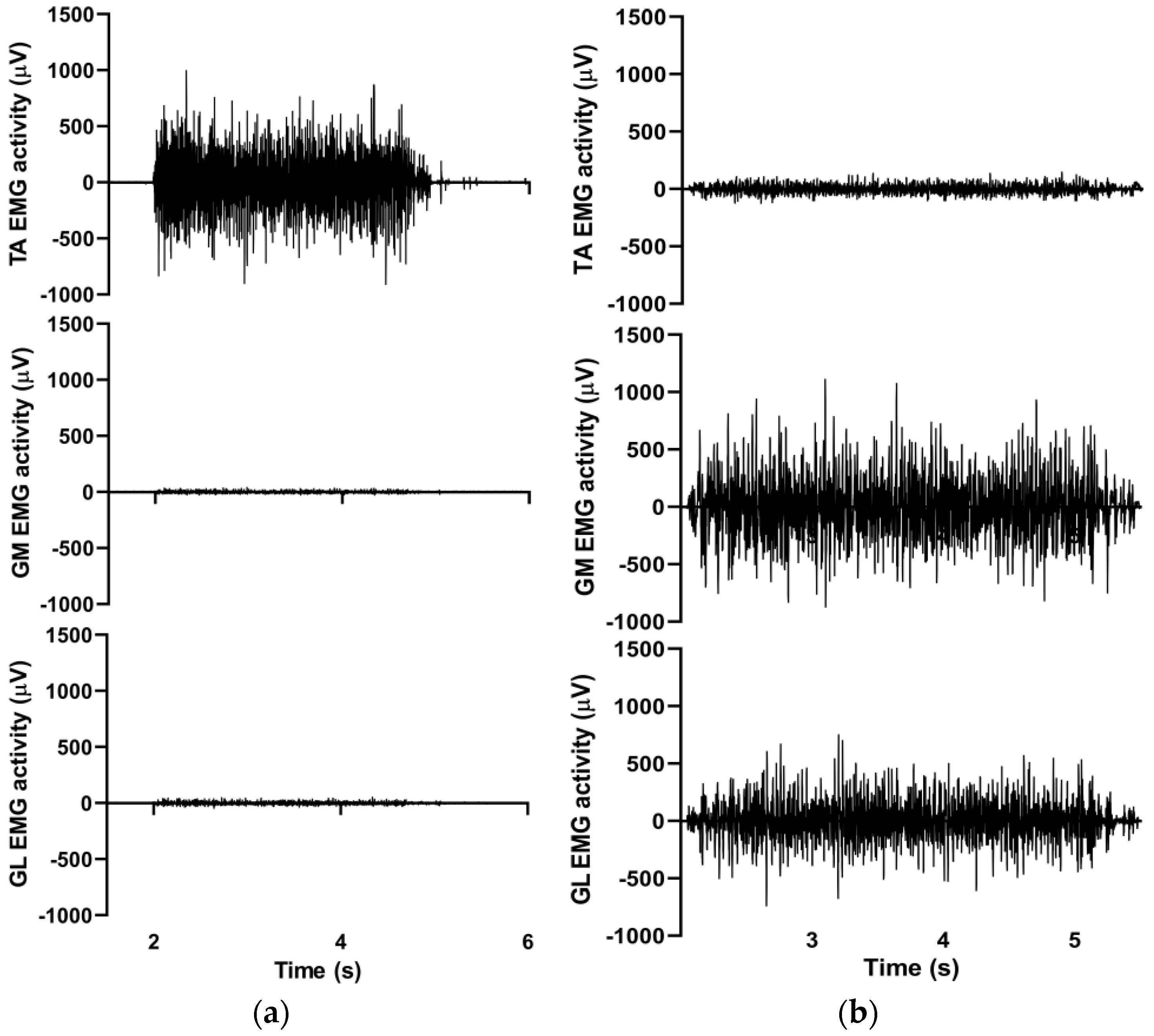
2.5. Surface Electromyography
2.6. Range of Motion (ROM) Testing
2.7. Balance Testing
2.8. Timed up and Go (TUG) Test
2.9. Sand Exercise Training
2.10. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Dyck, P.J.; Kratz, K.M.; Karnes, J.L.; Litchy, W.J.; Klein, R.; Pach, J.M.; Wilson, D.M.; O’Brien, P.C.; Melton, L.J.; Service, F.J. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population-based cohort: The Rochester Diabetic Neuropathy Study. Neurology 1993, 43, 817–824. [Google Scholar] [CrossRef] [PubMed]
- Young, M.J.; Boulton, A.J.; MacLeod, A.F.; Williams, D.R.; Sonksen, P.H. A multicentre study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologia 1993, 36, 150–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, S.; Ashe, H.A.; Parnell, L.N.; Fernando, D.J.; Tsigos, C.; Young, R.J.; Ward, J.D.; Boulton, A.J. The prevalence of foot ulceration and its correlates in type 2 diabetic patients: A population-based study. Diabet. Med. J. Br. Diabet. Assoc. 1994, 11, 480–484. [Google Scholar] [CrossRef]
- Cabezas-Cerrato, J. The prevalence of clinical diabetic polyneuropathy in Spain: A study in primary care and hospital clinic groups. Neuropathy Spanish Study Group of the Spanish Diabetes Society (SDS). Diabetologia 1998, 41, 1263–1269. [Google Scholar] [CrossRef] [Green Version]
- Sartor, C.D.; Watari, R.; Pássaro, A.C.; Picon, A.P.; Hasue, R.H.; Sacco, I.C.N. Effects of a combined strengthening, stretching and functional training program versus usual-care on gait biomechanics and foot function for diabetic neuropathy: A randomized controlled trial. BMC Musculoskelet. Disord. 2012, 13, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulton, A.J.M. The diabetic foot: From art to science. The 18th Camillo Golgi lecture. Diabetologia 2004, 47, 1343–1353. [Google Scholar] [CrossRef] [PubMed]
- Goldsmith, J.R.; Lidtke, R.H.; Shott, S. The effects of range-of-motion therapy on the plantar pressures of patients with diabetes mellitus. J. Am. Podiatr. Med. Assoc. 2002, 92, 483–490. [Google Scholar] [CrossRef]
- Zimny, S.; Schatz, H.; Pfohl, M. The role of limited joint mobility in diabetic patients with an at-risk foot. Diabetes Care 2004, 27, 942–946. [Google Scholar] [CrossRef] [Green Version]
- Sartor, C.D.; Hasue, R.H.; Cacciari, L.P.; Butugan, M.K.; Watari, R.; Pássaro, A.C.; Giacomozzi, C.; Sacco, I.C.N. Effects of strengthening, stretching and functional training on foot function in patients with diabetic neuropathy: Results of a randomized controlled trial. BMC Musculoskelet. Disord. 2014, 15, 137. [Google Scholar] [CrossRef] [Green Version]
- Sawacha, Z.; Cristoferi, G.; Guarneri, G.; Corazza, S.; Donà, G.; Denti, P.; Facchinetti, A.; Avogaro, A.; Cobelli, C. Characterizing multisegment foot kinematics during gait in diabetic foot patients. J. Neuroeng. Rehabil. 2009, 6, 37. [Google Scholar] [CrossRef] [Green Version]
- Sawacha, Z.; Spolaor, F.; Guarneri, G.; Contessa, P.; Carraro, E.; Venturin, A.; Avogaro, A.; Cobelli, C. Abnormal muscle activation during gait in diabetes patients with and without neuropathy. Gait Posture 2012, 35, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, L.J.; Hastings, M.K.; Mueller, M.J. A moderate-intensity weight-bearing exercise program for a person with type 2 diabetes and peripheral neuropathy. Phys. Ther. 2012, 92, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Praet, S.F.E.; Jonkers, R.A.M.; Schep, G.; Stehouwer, C.D.A.; Kuipers, H.; Keizer, H.A.; van Loon, L.J. Long-standing, insulin-treated type 2 diabetes patients with complications respond well to short-term resistance and interval exercise training. Eur. J. Endocrinol. 2008, 158, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Savelberg, H.H.C.M.; Ilgin, D.; Angin, S.; Willems, P.J.B.; Schaper, N.C.; Meijer, K. Prolonged activity of knee extensors and dorsal flexors is associated with adaptations in gait in diabetes and diabetic polyneuropathy. Clin. Biomech. Bristol Avon 2010, 25, 468–475. [Google Scholar] [CrossRef]
- Ahmad, I.; Verma, S.; Noohu, M.M.; Shareef, M.Y.; Hussain, M.E. Sensorimotor and gait training improves proprioception, nerve function, and muscular activation in patients with diabetic peripheral neuropathy: A randomized control trial. J. Musculoskelet. Neuronal Interact. 2020, 20, 234–248. [Google Scholar] [PubMed]
- Monteiro, R.L.; Ferreira, J.S.S.P.; Silva, É.Q.; Cruvinel-Júnior, R.H.; Veríssimo, J.L.; Bus, S.A.; Sacco, I.C.N. Foot-ankle therapeutic exercise program can improve gait speed in people with diabetic neuropathy: A randomized controlled trial. Sci. Rep. 2022, 12, 7561. [Google Scholar] [CrossRef]
- Kruse, R.L.; Lemaster, J.W.; Madsen, R.W. Fall and balance outcomes after an intervention to promote leg strength, balance, and walking in people with diabetic peripheral neuropathy: “feet first” randomized controlled trial. Phys. Ther. 2010, 90, 1568–1579. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Song, R. Effects of Tai Chi Exercise on glucose control, neuropathy scores, balance, and quality of life in patients with type 2 diabetes and neuropathy. J. Altern. Complement. Med. 2012, 18, 1172–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allet, L.; Armand, S.; Aminian, K.; Pataky, Z.; Golay, A.; de Bie, R.A.; de Bruin, E.D. An exercise intervention to improve diabetic patients’ gait in a real-life environment. Gait Posture 2010, 32, 185–190. [Google Scholar] [CrossRef]
- Andersen, H. Motor function in diabetic neuropathy. Acta Neurol. Scand. 1999, 100, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, F.M.; Rampinini, E.; Castagna, C.; Martino, F.; Fiorini, S.; Wisloff, U. Effect of plyometric training on sand versus grass on muscle soreness and jumping and sprinting ability in soccer players. Br. J. Sport. Med. 2008, 42, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Miyama, M.; Nosaka, K. Influence of surface on muscle damage and soreness induced by consecutive drop jumps. J. Strength Cond. Res. 2004, 18, 206–211. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Assocation. Steps to Prevent or Delay Nerve Damage. 2022. Available online: https://diabetes.org/diabetes/neuropathy/steps-prevent-or-delay-nerve-damage (accessed on 10 November 2022).
- Mueller, M.J.; Tuttle, L.J.; Lemaster, J.W.; Strube, M.J.; McGill, J.B.; Hastings, M.K.; Sinacore, D.R. Weight-bearing versus nonweight-bearing exercise for persons with diabetes and peripheral neuropathy: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 829–838. [Google Scholar] [CrossRef] [Green Version]
- Javorek, I. EQUIPMENT DESIGN: Sand boxes (sand stairs) and their use in developing explosive response. Strength Cond. J. 1991, 13, 84–87. [Google Scholar] [CrossRef]
- Colberg, S.R.; Sigal, R.J.; Yardley, J.E.; Riddell, M.C.; Dunstan, D.W.; Dempsey, P.C.; Horton, E.S.; Castorino, K.; Tate, D.F. Physical Activity/Exercise and Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care 2016, 39, 2065–2079. [Google Scholar] [CrossRef] [Green Version]
- Arazi, H.; Mohammadi, M.; Asadi, A. Muscular adaptations to depth jump plyometric training: Comparison of sand vs. land surface. Interv. Med. Appl. Sci. 2014, 6, 125–130. [Google Scholar] [CrossRef]
- Shin, H.-J.; Kim, S.-H.; Jeon, E.-T.; Lee, M.-G.; Lee, S.-J.; Cho, H.-Y. Effects of therapeutic exercise on sea sand on pain, fatigue, and balance in patients with chronic ankle instability: A feasibility study. J. Sport. Med. Phys. Fit. 2019, 59, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- The Effects of Sand Exercise Program on Balance Capability, Extremity Muscle Activity, and Inflammatory Markers in Older Women. Available online: https://www.ksep-es.org/journal/view.php?number=785 (accessed on 14 October 2022).
- Schneiders, A.G.; Sullivan, S.J.; O’Malley, K.J.; Clarke, S.V.; Knappstein, S.A.; Taylor, L.J. A valid and reliable clinical determination of footedness. Phys. Med. Rehabil. 2010, 2, 835–841. [Google Scholar] [CrossRef] [PubMed]
- Prókai, J.; Geszler, C.; Lukácsi, B.; Váczi, M. Rövidtávú TRX edzés izommechanikai és funkcionális hatása edzetlen személyeknél. Magy. Sport. Szle. 2016, 17, 17–22. [Google Scholar]
- Moreira, B.D.S.; Dos Anjos, D.M.D.C.; Pereira, D.S.; Sampaio, R.F.; Pereira, L.S.M.; Dias, R.C.; Kirkwood, R.N. The geriatric depression scale and the timed up and go test predict fear of falling in community-dwelling elderly women with type 2 diabetes mellitus: A cross-sectional study. BMC Geriatr. 2016, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Pados, G. Up-to-date treatment of obesity. Orv. Hetil. 2010, 151, 501–504. [Google Scholar] [CrossRef]
- Allet, L.; Armand, S.; de Bie, R.A.; Golay, A.; Monnin, D.; Aminian, K.; Staal, J.B.; de Bruin, E.D. The gait and balance of patients with diabetes can be improved: A randomised controlled trial. Diabetologia 2010, 53, 458–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katics, L. Kondicionális és Koordinációs Képességek Fejlesztése (a Testnevelésben, Szabadidő-és Versenysportban); PTE TTK: Pécs, Hungary, 2015. [Google Scholar]
- Venkataraman, K.; Tai, B.C.; Khoo, E.Y.H.; Tavintharan, S.; Chandran, K.; Hwang, S.W.; Phua, M.S.L.A.; Wee, H.L.; Koh, G.C.H.; Tai, E.S. Short-term strength and balance training does not improve quality of life but improves functional status in individuals with diabetic peripheral neuropathy: A randomised controlled trial. Diabetologia 2019, 62, 2200–2210. [Google Scholar] [CrossRef] [Green Version]
- Andersen, H.; Nielsen, S.; Mogensen, C.E.; Jakobsen, J. Muscle strength in type 2 diabetes. Diabetes 2004, 53, 1543–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alter, M.J. Science of Flexibility; Human Kinetics: Champaign, IL, USA, 1996. [Google Scholar]
- Lee, K.; Lee, S.; Song, C. Whole-body vibration training improves balance, muscle strength and glycosylated hemoglobin in elderly patients with diabetic neuropathy. Tohoku J. Exp. Med. 2013, 231, 305–314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, C.H.; Petrofsky, J.S.; Lee, S.W.; Lee, K.J.; Yim, J.E. Effects of an exercise program on balance and trunk proprioception in older adults with diabetic neuropathies. Diabetes Technol. Ther. 2011, 13, 803–811. [Google Scholar] [CrossRef]
- Hirase, T.; Inokuchi, S.; Matsusaka, N.; Okita, M. Effects of a balance training program using a foam rubber pad in community-based older adults: A randomized controlled trial. J. Geriatr. Phys. Ther. 2015, 38, 62–70. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Control Period | Intervention Period | ||||
|---|---|---|---|---|---|---|
| Test 1 | Test 2 | Test 3 | ∆% # | sig. | ||
| Plantarflexion MVIC test | ||||||
| Torque | (Nm) | 51 ± 32 | 43 ± 22 | 61 ± 36 | 18 (42) | * |
| EMGGL | (µV) | 99 ± 71 | 69 ± 69 | 82 ± 76 | 13 (19) | |
| EMGGM | (µV) | 104 ± 79 | 87 ± 109 | 106 ± 119 | 19 (22) | |
| EMGTA | (µV) | 26 ± 9 | 21 ± 11 | 20 ± 9 | −1 (5) | |
| EMGGL/TA | (ratio) | 3 ± 3 | 3 ± 2 | 4 ± 3 | 1 (33) | |
| EMGGM/TA | (ratio) | 4 ± 3 | 4 ± 4 | 5 ± 5 | 1 (25) | |
| Dorsiflexion MVIC test | ||||||
| Torque | (Nm) | 34 ± 21 | 35 ± 15 | 33 ± 15 | −2 (6) | |
| EMGGL | (µV) | 18 ± 9 | 17 ± 4 | 12 ± 3 | −5 (30) | ** |
| EMGGM | (µV) | 16 ± 10 | 19 ± 6 | 12 ± 6 | −7 (37) | ** |
| EMGTA | (µV) | 285 ± 130 | 297 ± 99 | 228 ± 99 | −69 (23) | ** |
| EMGTA/GL | (ratio) | 18 ± 10 | 18 ± 6 | 19 ± 9 | 1 (6) | |
| EMGTA/GM | (ratio) | 22 ± 13 | 17 ± 6 | 21 ± 12 | 4 (24) | |
| Functional measurements | ||||||
| Postural sway | (points) | 43 ± 17 | 43 ± 14 | 50 ± 12 | 7 (16) | * |
| ROMPF | (degree) | 51 ± 20 | 50 ± 21 | 59 ± 14 | 9 (18) | * |
| ROMDF | (degree) | −6 ± 9 | −5 ± 11 | −12 ± 11 | 7 (140) | * |
| TUG | (s) | 11 ± 3 | 11 ± 3 | 9 ± 3 | −2 (18) | ** |
| Body composition measurement | ||||||
| Body mass | (kg) | 101 ± 25 | 102 ± 27 | 97 ± 26 | −5 (5) | |
| Body fat | (%) | 38 ± 8 | 38 ± 7 | 36 ± 8 | −2 (5) | |
| Muscle mass | (kg) | 34 ± 9 | 35 ± 9 | 34 ± 9 | −1 (3) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prókai, J.; Murlasits, Z.; Bánhidi, M.; Csóka, L.; Gréci, V.; Atlasz, T.; Váczi, M. The Effects of a 12-Week-Long Sand Exercise Training Program on Neuromechanical and Functional Parameters in Type II Diabetic Patients with Neuropathy. Int. J. Environ. Res. Public Health 2023, 20, 5413. https://doi.org/10.3390/ijerph20075413
Prókai J, Murlasits Z, Bánhidi M, Csóka L, Gréci V, Atlasz T, Váczi M. The Effects of a 12-Week-Long Sand Exercise Training Program on Neuromechanical and Functional Parameters in Type II Diabetic Patients with Neuropathy. International Journal of Environmental Research and Public Health. 2023; 20(7):5413. https://doi.org/10.3390/ijerph20075413
Chicago/Turabian StylePrókai, Judit, Zsolt Murlasits, Miklós Bánhidi, László Csóka, Viktória Gréci, Tamás Atlasz, and Márk Váczi. 2023. "The Effects of a 12-Week-Long Sand Exercise Training Program on Neuromechanical and Functional Parameters in Type II Diabetic Patients with Neuropathy" International Journal of Environmental Research and Public Health 20, no. 7: 5413. https://doi.org/10.3390/ijerph20075413