
The Prevalence of Compassion Fatigue among Oncology Healthcare Professionals in Three Public Healthcare Facilities in Kwazulu-Natal, South Africa


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
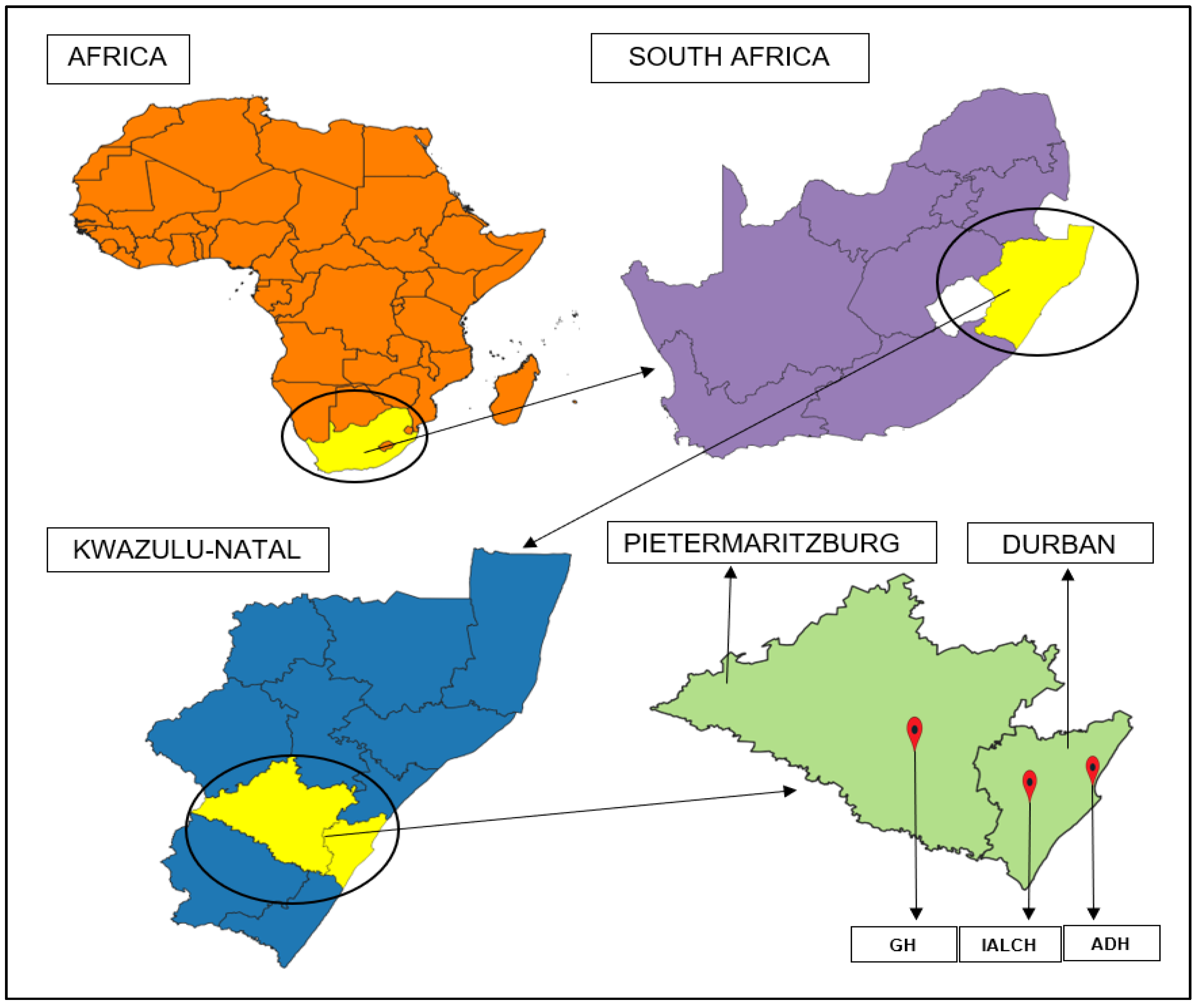
2.2. Study Setting
2.2.1. ADH
2.2.2. IALCH
2.2.3. GH
2.3. Study Population and Sampling
2.4. Data Collection Procedure
2.5. Data Collection Tool
2.6. Data Analysis
- Low CF: ≤22
- Average CF: between 23 and 41
- High CF: ≥42
2.7. Ethical Considerations
3. Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Agency for Research on Cancer. Latest Global Cancer Data: Cancer Burden Rises to 18.1 Million New Cases and 9.6 Million Cancer Deaths in 2018; International Agency for Research on Cancer: Lyon, France, 2018. [Google Scholar]
- Medisauskaite, A.; Kamau, C. Prevalence of oncologists in distress: Systematic review and meta-analysis. Psychooncology 2017, 26, 1732–1740. [Google Scholar] [CrossRef] [PubMed]
- Wentzel, D.; Brysiewicz, P. A survey of compassion satisfaction, burnout and compassion fatigue in nurses practicing in three oncology departments in Durban, South Africa. Int. J. Afr. Nurs. Sci. 2018, 8, 82–86. [Google Scholar] [CrossRef]
- Duarte, J.; Pinto-Gouveia, J. The role of psychological factors in oncology nurses’ burnout and compassion fatigue symptoms. Eur. J. Oncol. Nurs. 2017, 28, 114–121. [Google Scholar] [CrossRef]
- Newell, J.M.; MacNeil, G.A. Professional burnout, vicarious trauma, secondary traumatic stress, and compassion fatigue. Best Pract. Ment. Health 2010, 6, 57–68. [Google Scholar]
- Adams, R.E.; Boscarino, J.A.; Figley, C.R. Compassion fatigue and psychological distress among social workers: A validation study. Am. J. Orthopsychiatry 2006, 76, 103–108. [Google Scholar] [CrossRef] [Green Version]
- Figley, C.R. Treating Compassion Fatigue; Routledge: London, UK, 2002. [Google Scholar]
- Medland, J.; Howard-Ruben, J.; Whitaker, E. Fostering psychosocial wellness in oncology nurses: Addressing burnout and social support in the workplace. Oncol. Nurs. Forum 2004, 31, 47–54. [Google Scholar] [CrossRef] [Green Version]
- McHolm, F. Rx for compassion fatigue. J. Christ Nurs. 2006, 23, 12–19. [Google Scholar] [CrossRef]
- Potter, P.; Deshields, T.; Divanbeigi, J.; Berger, J.; Cipriano, D.; Norris, L.; Olsen, S. Compassion fatigue and burnout: Prevalence among oncology nurses. Clin. J. Oncol. Nurs. 2010, 14, E56. [Google Scholar] [CrossRef]
- Pfifferling, J.-H.; Gilley, K. Overcoming compassion fatigue. Fam. Pract. Manag. 2000, 7, 39. [Google Scholar]
- Perry, B.; Toffner, G.; Merrick, T.; Dalton, J. An exploration of the experience of compassion fatigue in clinical oncology nurses. Can. Oncol. Nurs. J. 2011, 21, 91–105. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, A.; Graham, J.; Richards, M.; Cull, A.; Gregory, W.; Leaning, M.; Snashall, D.; Timothy, A. Burnout and psychiatric disorder among cancer clinicians. Br. J. Cancer 1995, 71, 1263–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mougalian, S.S.; Lessen, D.S.; Levine, R.L.; Panagopoulos, G.; Von Roenn, J.H.; Arnold, R.M.; Block, S.D.; Buss, M.K. Palliative care training and associations with burnout in oncology fellows. J. Support Oncol. 2013, 11, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, S.; Wallace, J.E. Oncologist burnout and compassion fatigue: Investigating time pressure at work as a predictor and the mediating role of work-family conflict. BMC Health Serv. Res. 2017, 17, 639. [Google Scholar] [CrossRef] [Green Version]
- Flinton, D.; Cherry, P.; Thorne, R.; Mannion, L.; O’Sullivan, C.; Khine, R. Compassion satisfaction and fatigue: An investigation into levels being reported by radiotherapy students. J. Radiother. Pract. 2018, 17, 364–367. [Google Scholar] [CrossRef]
- Rasmussen, V.; Turnell, A.; Butow, P.; Juraskova, I.; Kirsten, L.; Wiener, L.; Patenaude, A.; Hoekstra-Weebers, J.; Grassi, L.; IPOS Research Committee. Burnout among psychosocial oncologists: An application and extension of the effort–reward imbalance model. Psycho-Oncology 2016, 25, 194–202. [Google Scholar] [CrossRef] [Green Version]
- Omair, A. Selecting the appropriate study design for your research: Descriptive study designs. J. Health Spec. 2015, 3, 153. [Google Scholar] [CrossRef]
- Ground, T. Addington Hospital. 2008. Available online: https://www.travelground.com/attractions/addington-hospital (accessed on 1 July 2020).
- COGTA. ETHEKWINI Metropolitan KZN. Available online: https://www.cogta.gov.za/ddm/wp-content/uploads/2020/07/Metro-Profile_Ethekwini.pdf (accessed on 16 September 2022).
- KwaZulu-Natal Department of Health. Inkosi Albert Luthuli Central Hospital. 2017. Available online: https://www.ialch.co.za/about-us/ (accessed on 1 July 2020).
- Ground, T. Inkosi Albert Luthuli Central Hospital. 2008. Available online: https://www.travelground.com/attractions/inkosi-albert-luthuli-central-hospital (accessed on 1 July 2020).
- COGTA. UMGUNGUNDLOVU District Municipality, KZN. Available online: https://www.cogta.gov.za/ddm/wp-content/uploads/2020/08/Umgungundlovu-District-Municipality-Profile.pdf (accessed on 17 September 2022).
- KwaZulu-Natal Department of Health. Grey’s Hospital. 2001. Available online: http://www.kznhealth.gov.za/Greys/tertiary_health_institution.htm (accessed on 1 July 2020).
- KwaZulu-Natal Department of Health. Grey’s Hospital Annual Report 2021/2022; KwaZulu-Natal Department of Health: Pietermaritzburg, South Africa, 2022.
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of convenience sampling and purposive sampling. Am. J. Theor. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Stamm, B.H. The Concise ProQOL Manual; ProQOL: Pocatello, ID, USA, 2010. [Google Scholar]
- Hooper, C.; Craig, J.; Janvrin, D.R.; Wetsel, M.A.; Reimels, E. Compassion satisfaction, burnout, and compassion fatigue among emergency nurses compared with nurses in other selected inpatient specialties. J. Emerg. Nurs. 2010, 36, 420–427. [Google Scholar] [CrossRef]
- Katsantoni, K.; Zartaloudi, A.; Papageorgiou, D.; Drakopoulou, M.; Misouridou, E. Prevalence of compassion fatigue, burn-out and compassion satisfaction among maternity and gynecology care providers in Greece. Mater. Socio-Med. 2019, 31, 172. [Google Scholar] [CrossRef]
- Mason, H.D.; Nel, J.A. Compassion fatigue, burnout and compassion satisfaction: Prevalence among nursing students. J. Psychol. Afr. 2012, 22, 451–455. [Google Scholar] [CrossRef]
- Parker, A.; Karamchand, S.; Schrueder, N.; Lahri, S.; Rabie, H.; Aucamp, M.; Abrahams, R.; Ciapparelli, P.; Erasmus, D.; Cotton, M. Leadership and early strategic response to the SARS-CoV-2 pandemic at a COVID-19 designated hospital in South Africa. SAMJ S. Afr. Med. J. 2020, 110, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochbati, L.; Vanderpuye, V.; Moujahed, R.; Rejeb, M.B.; Naimi, Z.; Olasinde, T. Cancer care and COVID-19: Tailoring recommendations for the African radiation oncology context. Ecancermedicalscience 2020, 14, 1144. [Google Scholar] [CrossRef]
- Vanderpuye, V.; Elhassan, M.M.A.; Simonds, H. Preparedness for COVID-19 in the oncology community in Africa. Lancet Oncol. 2020, 21, 621–622. [Google Scholar] [CrossRef] [PubMed]
- De Villiers, C.; Cerbone, D.; Van Zijl, W. The South African government’s response to COVID-19. J. Public Budg. Account. Financ. Manag. 2020, 32, 797–811. [Google Scholar] [CrossRef]
- Cano-Valderrama, O.; Morales, X.; Ferrigni, C.; Martín-Antona, E.; Turrado, V.; García, A.; Cuñarro-López, Y.; Zarain-Obrador, L.; Duran-Poveda, M.; Balibrea, J. Reduction in emergency surgery activity during COVID-19 pandemic in three Spanish hospitals. J. Br. Surg. 2020, 107, e239. [Google Scholar] [CrossRef]
- Mlaba, P.C.; Ginindza, T.G.; Hlongwana, K.W. The social burden experienced by families caring for members living with cancer in KwaZulu-Natal, South Africa. Afr. J. Prim. Health Care Fam. Med. 2021, 13, 2955. [Google Scholar] [CrossRef]
- Mbeje, N.P.; Ginindza, T.G.; Jafta, N. Establishing and evaluating cancer surveillance system in KwaZulu-Natal, South Africa. Cancer Inform. 2021, 20, 11769351211029967. [Google Scholar] [CrossRef] [PubMed]
- Boniol, M.; McIsaac, M.; Xu, L.; Wuliji, T.; Diallo, K.; Campbell, J. Gender Equity in the Health Workforce: Analysis of 104 Countries; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Turgoose, D.; Maddox, L. Predictors of compassion fatigue in mental health professionals: A narrative review. Traumatology 2017, 23, 172. [Google Scholar] [CrossRef]
- Lopez, A.; Sanderman, R.; Ranchor, A.V.; Schroevers, M.J. Compassion for Others and Self-Compassion: Levels, Correlates, and Relationship with Psychological Well-Being. Mindfulness 2018, 9, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eagly, A.H.; Crowley, M. Gender and helping behavior: A meta-analytic review of the social psychological literature. Psychol. Bull. 1986, 100, 283. [Google Scholar] [CrossRef]
- Yu, H.; Jiang, A.; Shen, J. Prevalence and predictors of compassion fatigue, burnout and compassion satisfaction among oncology nurses: A cross-sectional survey. Int. J. Nurs. Stud. 2016, 57, 28–38. [Google Scholar] [CrossRef]
- Coetzee, S.K.; Klopper, H.C. Compassion fatigue within nursing practice: A concept analysis. Nurs. Health Sci. 2010, 12, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Peters, E. Compassion fatigue in nursing: A concept analysis. Nurs. Forum 2018, 53, 466–480. [Google Scholar] [CrossRef]
- Aycock, N.; Boyle, D. Interventions to manage compassion fatigue in oncology nursing. Clin. J. Oncol. Nurs. 2009, 13, 183–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyle, D.A. Countering compassion fatigue: A requisite nursing agenda. Online J. Issues Nurs. 2011, 16, 2. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Demographic Category | N | (%) | |
|---|---|---|---|
| Age in years * Mean (SD) 39.16 (9.417) | 20–30 | 13 | 17.8 |
| 31–40 | 30 | 41.1 | |
| 41–50 | 14 | 19.2 | |
| 51–60 | 9 | 12.3 | |
| Missing Values | 7 | 9.6 | |
| Total | 73 | 100.0 | |
| Gender | Female | 59 | 80.8 |
| Male | 14 | 19.2 | |
| Total | 73 | 100.0 | |
| Occupation | Oncologist | 8 | 10.9 |
| Nurse | 34 | 46.6 | |
| Radiographer | 18 | 24.7 | |
| Radiation Therapist | 1 | 1.4 | |
| Psychologist | 2 | 2.7 | |
| Medical Officer (Oncology) | 1 | 1.4 | |
| Other | 9 | 12.3 | |
| Total | 73 | 100.0 | |
| Experience in years * Mean (SD) 11.45 (8.372) | 1–5 | 15 | 20.5 |
| 6–10 | 18 | 24.7 | |
| 11–20 | 25 | 34.2 | |
| 21–40 | 7 | 9.6 | |
| Missing Values | 8 | 11.0 | |
| Total | 73 | 100.0 | |
| Facility | AD | 18 | 24.6 |
| IALCH | 21 | 28.8 | |
| GH | 34 | 46.6 | |
| Total | 73 | 100.0 | |
| Facility | CF Level | ||||
| Low | Average | High | N | Mean Scores (SD) | |
| ADH | 11 | 7 | 0 | 18 | 21.17 (5.752) |
| IALCH | 4 | 17 | 0 | 21 | 26.76 (6.625) |
| GH | 17 | 17 | 0 | 34 | 22.85 (6.933) |
| Total N (%) | 32 (43.8) | 41 (56.2) | 0 (0.0) | 73 (100) | 23.56 (6.833) |
| p Value (F Value) | p = 0.025 (F = 3.879) | ||||
| Gender | Low | Average | High | N | Mean Scores (SD) |
| Female | 23 | 36 | 0 | 59 | 24.25 (6.506) |
| Male | 9 | 5 | 0 | 14 | 20.64 (7.642) |
| p Value (T Value) | p = 0.075 (t = 1.805) | ||||
| Variable | Age | Experience | CF Score | |
|---|---|---|---|---|
| Age | Pearson Correlation | - | 0.802 ** | 0.279 * |
| Sig. (2-tailed) | <0.001 | 0.023 | ||
| Experience | Pearson Correlation | - | 0.127 | |
| Sig. (2-tailed) | 0.313 | |||
| CF score | Pearson Correlation | - | ||
| Sig. (2-tailed) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mlaba, P.C.; Ginindza, T.G.; Hlongwana, K.W. The Prevalence of Compassion Fatigue among Oncology Healthcare Professionals in Three Public Healthcare Facilities in Kwazulu-Natal, South Africa. Int. J. Environ. Res. Public Health 2023, 20, 5412. https://doi.org/10.3390/ijerph20075412
Mlaba PC, Ginindza TG, Hlongwana KW. The Prevalence of Compassion Fatigue among Oncology Healthcare Professionals in Three Public Healthcare Facilities in Kwazulu-Natal, South Africa. International Journal of Environmental Research and Public Health. 2023; 20(7):5412. https://doi.org/10.3390/ijerph20075412
Chicago/Turabian StyleMlaba, Phindile C., Themba G. Ginindza, and Khumbulani W. Hlongwana. 2023. "The Prevalence of Compassion Fatigue among Oncology Healthcare Professionals in Three Public Healthcare Facilities in Kwazulu-Natal, South Africa" International Journal of Environmental Research and Public Health 20, no. 7: 5412. https://doi.org/10.3390/ijerph20075412