
Changes in Alcohol Consumption during the COVID-19 Pandemic: Evidence from Wisconsin
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Survey of the Health of Wisconsin (SHOW)
2.2. The SHOW COVID-19 Community Impact Survey
2.2.1. Study Participants and Recruitment
2.2.2. Alcohol Consumption Assessment
2.2.3. Demographics and Characteristics
2.2.4. Statistical Analysis
3. Results
3.1. Demographics
3.2. Univariate Comparisons of Changes in Alcohol Consumption
3.3. Logistic Regression Modeling of Increased Alcohol Consumption
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moon, A.M.; Curtis, B.; Mandrekar, P.; Singal, A.K.; Verna, E.C.; Fix, O.K. Alcohol-Associated Liver Disease Before and After COVID-19—An Overview and Call for Ongoing Investigation. Hepatol. Commun. 2021, 5, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- Bott, K.; Meyer, C.; Rumpf, H.-J.; Hapke, U.; John, U. Psychiatric disorders among at-risk consumers of alcohol in the general population. J. Stud. Alcohol 2005, 66, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Markman Geisner, I.; Larimer, M.E.; Neighbors, C. The relationship among alcohol use, related problems, and symptoms of psychological distress: Gender as a moderator in a college sample. Addict. Behav. 2004, 29, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Okoro, C.A.; Brewer, R.D.; Naimi, T.S.; Moriarty, D.G.; Giles, W.H.; Mokdad, A.H. Binge drinking and health-related quality of life. Am. J. Prev. Med. 2004, 26, 230–233. [Google Scholar] [CrossRef] [PubMed]
- Brière, F.N.; Rohde, P.; Seeley, J.R.; Klein, D.; Lewinsohn, P.M. Comorbidity between major depression and alcohol use disorder from adolescence to adulthood. Compr. Psychiatry 2014, 55, 526–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolton, J.; Cox, B.; Clara, I.; Sareen, J. Use of Alcohol and Drugs to Self-Medicate Anxiety Disorders in a Nationally Representative Sample. J. Nerv. Ment. Dis. 2006, 194, 818–825. [Google Scholar] [CrossRef]
- Robinson, J.; Sareen, J.; Cox, B.J.; Bolton, J. Self-medication of anxiety disorders with alcohol and drugs: Results from a nationally representative sample. J. Anxiety Disord. 2009, 23, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet. Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Kornreich, B. The Economic Impact of the COVID-19 Pandemic on the United States. Available online: https://sites.lsa.umich.edu/mje/2022/01/09/the-economic-impact-of-the-covid-19-pandemic-on-the-united-states/ (accessed on 27 January 2023).
- Fairbairn, C.E.; Sayette, M.A. A social-attributional analysis of alcohol response. Psychol. Bull. 2014, 140, 1361–1382. [Google Scholar] [CrossRef] [Green Version]
- Keyes, K.M.; Hatzenbuehler, M.L.; Grant, B.F.; Hasin, D.S. Stress and alcohol: Epidemiologic evidence. Alcohol Res. Curr. Rev. 2012, 34, 391–400. [Google Scholar]
- Clay, J.M.; Parker, M.O. Alcohol use and misuse during the COVID-19 pandemic: A potential public health crisis? Lancet. Public Health 2020, 5, e259. [Google Scholar] [CrossRef] [PubMed]
- Baker, T.B.; Piper, M.E.; McCarthy, D.E.; Majeskie, M.R.; Fiore, M.C. Addiction Motivation Reformulated: An Affective Processing Model of Negative Reinforcement. Psychol. Rev. 2004, 111, 33–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldmann, E.; Galea, S. Mental Health Consequences of Disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef] [PubMed]
- Cepeda, A.; Valdez, A.; Kaplan, C.; Hill, L.E. Patterns of substance use among hurricane Katrina evacuees in Houston, Texas. Disasters 2010, 34, 426–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bor, J.; Basu, S.; Coutts, A.; McKee, M.; Stuckler, D. Alcohol Use During the Great Recession of 2008–2009. Alcohol Alcohol. 2013, 48, 343–348. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Liu, X.; Fang, Y.; Fan, B.; Fuller, C.J.; Guan, Z.; Yao, Z.; Kong, J.; Lu, J.; Litvak, I.J. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol Alcohol. 2008, 43, 706–712. [Google Scholar] [CrossRef] [Green Version]
- Richman, J.A.; Cloninger, L.; Rospenda, K.M. Macrolevel stressors, terrorism, and mental health outcomes: Broadening the stress paradigm. Am. J. Public Health 2008, 98, 323–329. [Google Scholar] [CrossRef]
- Kanehara, A.; Ando, S.; Araki, T.; Usami, S.; Kuwabara, H.; Kano, Y.; Kasai, K. Trends in psychological distress and alcoholism after The Great East Japan Earthquake of 2011. SSM-Popul. Health 2016, 2, 807–812. [Google Scholar] [CrossRef] [Green Version]
- Lau, J.T.F.; Yang, X.; Pang, E.; Tsui, H.Y.; Wong, E.; Wing, Y.K. SARS-related perceptions in Hong Kong. Emerg. Infect. Dis. 2005, 11, 417–424. [Google Scholar] [CrossRef]
- Yao, H.; Chen, J.-H.; Xu, Y.-F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Lee, S.A.; Mathis, A.A.; Jobe, M.C.; Pappalardo, E.A. Clinically significant fear and anxiety of covid-19: A psychometric examination of the coronavirus anxiety scale. Psychiatry Res. 2020, 290, 113112. [Google Scholar] [CrossRef] [PubMed]
- Lechner, W.V.; Laurene, K.R.; Patel, S.; Anderson, M.; Grega, C.; Kenne, D.R. Changes in alcohol use as a function of psychological distress and social support following COVID-19 related university closings. Addict. Behav. 2020, 110, 106527. [Google Scholar] [CrossRef] [PubMed]
- Pollard, M.S.; Tucker, J.S.; Green, H.D. Changes in adult alcohol use and consequences during the COVID-19 pandemic in the US. JAMA Netw. Open 2020, 3, e2022942. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bremner, J. Newsweek. Available online: https://www.newsweek.com/us-alcohol-sales-increase-55-percent-one-week-amid-coronavirus-pandemic-1495510 (accessed on 2 November 2022).
- Wisconsin Department of Health Services. Alcohol in Wisconsin. Available online: https://www.dhs.wisconsin.gov/alcohol/index.htm (accessed on 2 November 2022).
- Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion (CDC). BRFSS Prevalence & Trends Data. Available online: https://www.cdc.gov/brfss/brfssprevalence/ (accessed on 2 November 2022).
- Nieto, F.J.; Peppard, P.E.; Engelman, C.D.; McElroy, J.A.; Galvao, L.W.; Friedman, E.M.; Bersch, A.J.; Malecki, K.C. The survey of the Health of Wisconsin (Show), a novel infrastructure for Population Health Research: Rationale and Methods. BMC Public Health 2010, 10, 785. [Google Scholar] [CrossRef] [Green Version]
- Malecki, K.M.C.; Nikodemova, M.; Schultz, A.A.; LeCaire, T.J.; Bersch, A.J.; Cadmus-Bertram, L.; Engelman, C.D.; Hagen, E.; McCulley, L.; Palta, M.; et al. The Survey of the Health of Wisconsin (SHOW) Program: An Infrastructure for Advancing Population Health. Front. Public Health 2022, 10, 818777. [Google Scholar] [CrossRef]
- Survey of the Health of Wisconsin (SHOW). COVID-19 Public Use Data. Available online: https://show.wisc.edu/data/covid-19-public-use-data/ (accessed on 2 November 2022).
- Malecki, K.M.C.; Schultz, A.A.; Nikodemova, M.; Walsh, M.C.; Bersch, A.J.; Cronin, J.; Cadmus-Bertram, L.; Engelman, C.D.; Lubsen, J.R.; Peppard, P.E.; et al. Statewide Impact of COVID-19 on Social Determinants of Health—A First Look: Findings from the Survey of the Health of Wisconsin. Preprint 2022. [Google Scholar] [CrossRef]
- Burakoff, M. COVID-19 in 2021: A Timeline of Wisconsin’s Second Pandemic Year. Available online: https://spectrumnews1.com/wi/milwaukee/news/2021/12/30/covid-19-in-2021--a-timeline-of-wisconsin-s-second-pandemic-year (accessed on 3 March 2023).
- Solopov, P.A. Covid-19 vaccination and alcohol consumption: Justification of risks. Pathogens 2023, 12, 163. [Google Scholar] [CrossRef]
- Awijen, H.; Ben Zaied, Y.; Nguyen, D.K. COVID-19 vaccination, fear and anxiety: Evidence from google search trends. Soc. Sci. Med. 2022, 297, 114820. [Google Scholar] [CrossRef]
- Chen, S.; Aruldass, A.R.; Cardinal, R.N. Mental health outcomes after SARS-COV-2 vaccination in the United States: A national cross-sectional study. J. Affect. Disord. 2022, 298, 396–399. [Google Scholar] [CrossRef]
- Rolland, B.; Haesebaert, F.; Zante, E.; Benyamina, A.; Haesebaert, J.; Franck, N. Global changes and factors of increase in caloric/salty food intake, screen use, and substance use during the early COVID-19 containment phase in the general population in France: Survey study. JMIR Public Health Surveill. 2020, 6, e19630. [Google Scholar] [CrossRef] [PubMed]
- Grossman, E.R.; Benjamin-Neelon, S.E.; Sonnenschein, S. Alcohol consumption during the covid-19 pandemic: A cross-sectional survey of US adults. Int. J. Environ. Res. Public Health 2020, 17, 9189. [Google Scholar] [CrossRef] [PubMed]
- Dumas, T.M.; Ellis, W.; Litt, D.M. What does adolescent substance use look like during the COVID-19 pandemic? examining changes in frequency, social contexts, and pandemic-related predictors. J. Adolesc. Health 2020, 67, 354–361. [Google Scholar] [CrossRef]
- Rodriguez, L.M.; Litt, D.M.; Stewart, S.H. Drinking to cope with the pandemic: The unique associations of covid-19-related perceived threat and psychological distress to drinking behaviors in American men and women. Addict. Behav. 2020, 110, 106532. [Google Scholar] [CrossRef] [PubMed]
- Karadayian, A.; Merlo, A.; Czerniczyniec, A.; Lores-Arnaiz, S.; Hendriksen, P.A.; Kiani, P.; Bruce, G.; Verster, J.C. Alcohol Consumption, hangovers, and smoking among Buenos Aires University students during the COVID-19 pandemic. J. Clin. Med. 2023, 12, 1491. [Google Scholar] [CrossRef]
- Sugaya, N.; Yamamoto, T.; Suzuki, N.; Uchiumi, C. Change in alcohol use during the prolonged COVID-19 pandemic and its psychosocial factors: A one-year longitudinal study in Japan. Int. J. Environ. Res. Public Health 2023, 20, 3871. [Google Scholar] [CrossRef]


{kind=link}
| Wave 1 (n = 1290) | Wave 2 (n = 1868) | Wave 3 (n = 1585) | ||||
|---|---|---|---|---|---|---|
| n | Percent (%) | n | Percent (%) | n | Percent (%) | |
| Gender | ||||||
| Male | 464 | 36.2 | 725 | 39.1 | 593 | 37.8 |
| Female | 817 | 63.8 | 1129 | 60.9 | 978 | 62.3 |
| Age | ||||||
| 21–35 years | 151 | 11.7 | 175 | 9.4 | 139 | 8.8 |
| 36–55 years | 422 | 32.8 | 608 | 32.6 | 484 | 30.8 |
| 56–75 years | 614 | 47.7 | 883 | 47.3 | 787 | 50.0 |
| Greater than 75 years | 101 | 7.8 | 201 | 10.8 | 163 | 10.4 |
| Race | ||||||
| White (Non-Hispanic) | 1139 | 88.4 | 1624 | 87.0 | 1371 | 87.9 |
| Non-White | 149 | 11.6 | 242 | 13.0 | 189 | 12.1 |
| Education | ||||||
| H.S./G.E.D. or Less | 197 | 15.4 | 301 | 16.2 | 246 | 15.7 |
| Some College | 411 | 32.0 | 648 | 34.8 | 555 | 35.4 |
| Bachelor’s or Higher | 675 | 52.6 | 912 | 49.0 | 769 | 49.0 |
| Income | ||||||
| <$30,000 | 163 | 13.9 | 252 | 15.0 | 208 | 14.7 |
| $30,000–$59,999 | 301 | 25.6 | 447 | 26.7 | 362 | 25.5 |
| $60,000–$99,999 | 347 | 29.5 | 498 | 29.7 | 417 | 29.4 |
| >$100,000 | 364 | 31.0 | 480 | 28.6 | 431 | 30.4 |
| Self-Reported Health | ||||||
| Excellent or Very Good | 783 | 60.7 | 1091 | 58.4 | 939 | 59.3 |
| Good | 393 | 30.5 | 609 | 32.6 | 484 | 30.6 |
| Fair or Poor | 113 | 8.8 | 167 | 8.9 | 160 | 10.1 |
| Children in Home | ||||||
| Children Present | 379 | 29.4 | 528 | 28.3 | 401 | 25.3 |
| No Children Present | 911 | 70.6 | 1340 | 71.7 | 1184 | 74.7 |
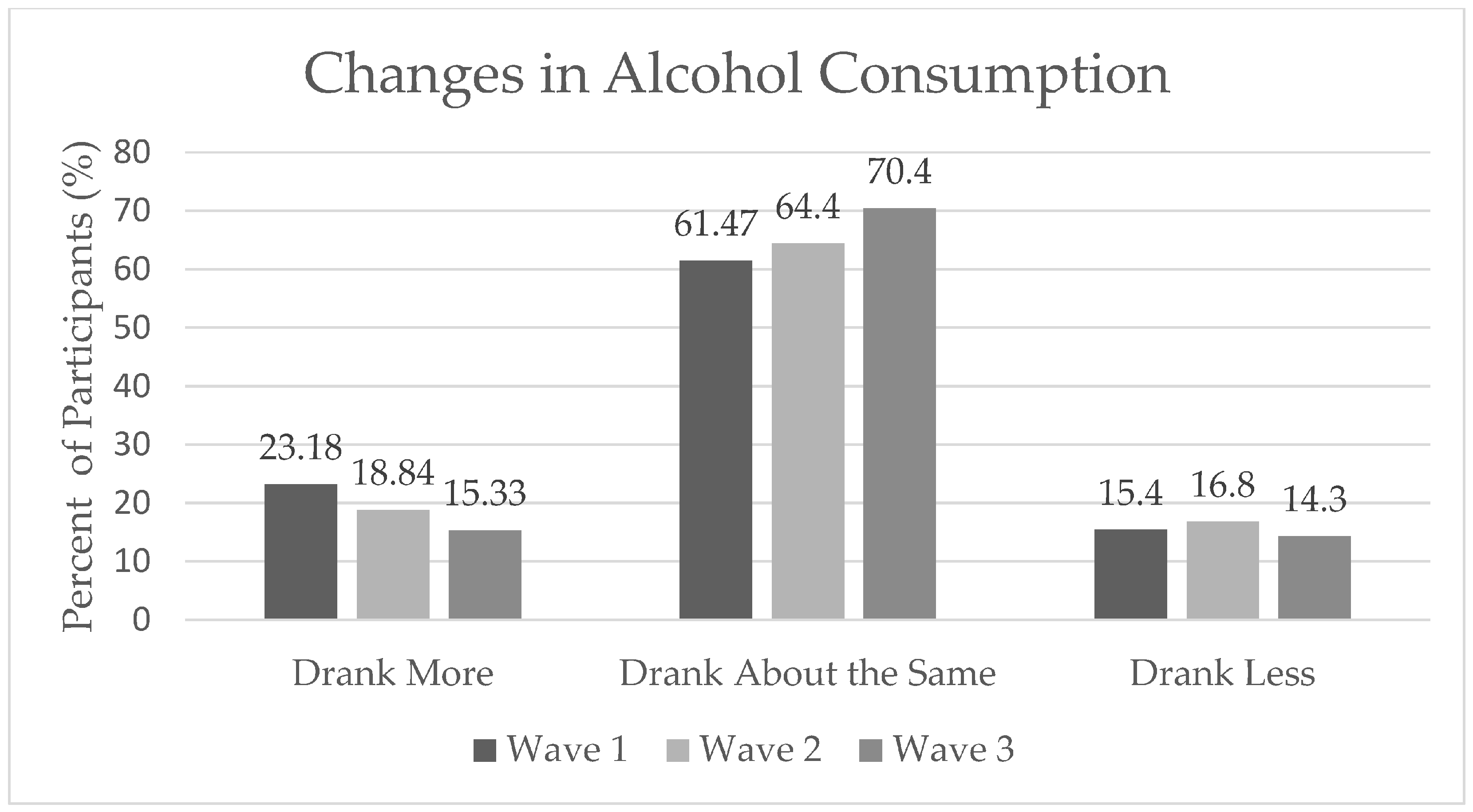
| Change in Alcohol Consumption | ||||||
| Drank More | 299 | 23.2 | 352 | 18.8 | 243 | 15.3 |
| Drank about the Same | 793 | 61.5 | 1208 | 64.4 | 1116 | 70.4 |
| Drank Less | 198 | 15.4 | 313 | 16.8 | 216 | 14.3 |
| Wave I | Wave II | Wave III | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Drank More (%) | Drank the Same (%) | Drank Less (%) | p-Trend | Drank More (%) | Drank the Same (%) | Drank Less (%) | p-Trend | Drank More (%) | Drank the Same (%) | Drank Less (%) | p-Trend | |
| Race | ||||||||||||
| White | 23.09 | 62.86 | 14.05 | 0.0006 | 18.72 | 64.35 | 16.93 | 0.7832 | 16.27 | 68.65 | 15.08 | 0.6943 |
| Non-White | 24.16 | 50.34 | 25.5 | 19.83 | 64.88 | 15.29 | 14.54 | 68.72 | 16.74 | |||
| Gender | ||||||||||||
| Male | 20.91 | 64.66 | 14.44 | 0.1671 | 17.93 | 63.72 | 18.34 | 0.2587 | 14.29 | 69.39 | 16.33 | 0.273 |
| Female | 24.6 | 59.36 | 16.03 | 19.57 | 64.92 | 15.5 | 16.93 | 68.26 | 14.8 | |||
| Income | ||||||||||||
| <$29,999 | 17.79 | 58.28 | 23.93 | 0.0001 | 15.08 | 66.27 | 18.65 | 0.0001 | 13.28 | 70.12 | 16.6 | 0.0139 |
| $30,000-$59,999 | 18.94 | 65.12 | 15.95 | 18.12 | 66.44 | 15.44 | 14.25 | 70.05 | 15.7 | |||
| $60,000-$99,999 | 23.92 | 64.84 | 11.24 | 17.87 | 67.87 | 14.26 | 17.49 | 69.55 | 12.96 | |||
| >$100,000 | 30.22 | 54.95 | 14.84 | 25.42 | 54.17 | 20.42 | 20.6 | 61.2 | 18.2 | |||
| Anxiety Status | ||||||||||||
| Anxiety | 30.68 | 54.58 | 14.74 | 0.0066 | 24.93 | 60.98 | 14.09 | 0.0027 | 20.74 | 65.34 | 13.92 | 0.0265 |
| No Anxiety | 21.37 | 63.14 | 15.5 | 17.34 | 65.24 | 17.41 | 14.92 | 69.42 | 15.66 | |||
| Depression Status | ||||||||||||
| Depression | 30.13 | 56.33 | 13.54 | 0.0224 | 23.77 | 60.93 | 15.3 | 0.0261 | 18.42 | 68.42 | 13.16 | 0.2486 |
| No Depression | 21.68 | 62.58 | 15.74 | 17.64 | 65.25 | 17.11 | 15.49 | 68.69 | 15.82 | |||
| Remote Work Status | ||||||||||||
| Remote Work | 35.17 | 52.91 | 11.93 | <0.0001 | 26.41 | 54.52 | 19.07 | <0.0001 | 23.49 | 58.43 | 18.07 | 0.0067 |
| No Remote Work | 19.11 | 64.38 | 16.51 | 16.72 | 67.17 | 16.11 | 15.29 | 69.66 | 15.05 | |||
| Health Status | ||||||||||||
| Excellent/Very Good | 23.37 | 62.45 | 14.18 | 0.3322 | 20.16 | 62.97 | 16.87 | 0.0233 | 16.59 | 67.68 | 15.73 | 0.1929 |
| Good | 24.43 | 59.03 | 16.54 | 19.05 | 65.19 | 15.76 | 15.66 | 67.99 | 16.35 | |||
| Fair/Poor | 17.7 | 62.83 | 19.47 | 9.58 | 70.66 | 19.76 | 14.29 | 75.66 | 10.05 | |||
| Education | ||||||||||||
| HS/GED or less | 15.23 | 67.51 | 17.26 | 0.0016 | 14.95 | 70.43 | 14.62 | <0.0001 | 13.54 | 73.61 | 12.85 | <0.0001 |
| Some College | 19.95 | 63.26 | 16.79 | 16.82 | 68.36 | 14.81 | 12.81 | 73.91 | 13.28 | |||
| Bachelor’s Degree or Higher | 27.7 | 58.37 | 13.93 | 21.49 | 59.87 | 18.64 | 19.1 | 63.16 | 17.74 | |||
| Age Group | ||||||||||||
| 21–40 | 35.27 | 48.06 | 16.67 | <0.0001 | 26.85 | 56.79 | 16.36 | <0.0001 | 22.56 | 58.92 | 18.52 | <0.0001 |
| 41–60 | 28.84 | 56.63 | 14.53 | 23.72 | 59.97 | 16.31 | 20.72 | 64.8 | 14.49 | |||
| >60 | 12.77 | 71.94 | 15.29 | 12.26 | 70.49 | 17.25 | 10.21 | 74.66 | 15.14 | |||
| Employment Change During COVID-19 | ||||||||||||
| Changes in Employment | 25.36 | 59.52 | 15.12 | 0.0387 | 19 | 64.03 | 16.97 | 0.8673 | 15.24 | 69.4 | 15.36 | 0.6743 |
| No Changes in Employment | 19.11 | 65.11 | 15.78 | 18.45 | 65.31 | 16.24 | 16.75 | 67.95 | 15.3 | |||
| Presence of Children in the Home | ||||||||||||
| Children in Home | 34.56 | 51.98 | 13.46 | <0.0001 | 25.57 | 59.66 | 14.77 | <0.0001 | 22.38 | 63.81 | 13.81 | <0.0001 |
| No Children in Home | 18.44 | 65.42 | 16.14 | 16.19 | 66.27 | 17.54 | 13.79 | 70.35 | 15.86 | |||
| Wave I | Wave II | Wave III | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Unadjusted | Adjusted a | Unadjusted | Adjusted b | Unadjusted | Adjusted c | |||||||||||||
| OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | |
| 55 vs. 21 years old | 0.63 | 0.36 | 1.11 | 0.64 | 0.34 | 1.19 | 0.75 | 0.45 | 1.28 | 0.81 | 0.43 | 1.52 | 0.81 | 0.48 | 1.37 | 0.87 | 0.44 | 1.71 |
| 55 vs. 25 years old | 0.65 | 0.4 | 1.05 | 0.66 | 0.38 | 1.13 | 0.77 | 0.49 | 1.21 | 0.82 | 0.47 | 1.41 | 0.82 | 0.52 | 1.28 | 0.87 | 0.48 | 1.56 |
| 55 vs. 30 years old | 0.67 | 0.46 | 0.99 | 0.69 | 0.44 | 1.06 | 0.78 | 0.54 | 1.12 | 0.82 | 0.53 | 1.28 | 0.82 | 0.57 | 1.18 | 0.87 | 0.54 | 1.39 |
| 55 vs. 35 years old | 0.69 | 0.52 | 0.93 | 0.71 | 0.51 | 1 | 0.79 | 0.6 | 1.05 | 0.83 | 0.59 | 1.17 | 0.82 | 0.63 | 1.08 | 0.87 | 0.61 | 1.24 |
| 55 vs. 40 years old | 0.72 | 0.59 | 0.87 | 0.74 | 0.59 | 0.94 | 0.81 | 0.67 | 0.98 | 0.84 | 0.66 | 1.06 | 0.83 | 0.69 | 0.99 | 0.87 | 0.68 | 1.11 |
| 55 vs. 45 years old | 0.75 | 0.67 | 0.84 | 0.78 | 0.68 | 0.89 | 0.83 | 0.75 | 0.93 | 0.85 | 0.74 | 0.98 | 0.84 | 0.76 | 0.94 | 0.88 | 0.76 | 1.01 |
| 55 vs. 50 years old | 0.83 | 0.79 | 0.87 | 0.85 | 0.8 | 0.9 | 0.88 | 0.85 | 0.93 | 0.89 | 0.84 | 0.95 | 0.89 | 0.85 | 0.93 | 0.91 | 0.86 | 0.97 |
| 55 vs. 60 years old | 1.35 | 1.25 | 1.46 | 1.33 | 1.23 | 1.43 | 1.23 | 1.16 | 1.3 | 1.23 | 1.16 | 1.32 | 1.21 | 1.13 | 1.28 | 1.17 | 1.1 | 1.25 |
| Wave I | Wave II | Wave III | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Children Present | No Children Present | Children Present | No Children Present | Children Present | No Children Present | |||||||||||||
| OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | OR | CI Lower | CI Upper | |
| Difference 55 vs. 21 | 0.32 | 0.09 | 1.16 | 2.13 | 0.50 | 9.06 | 0.46 | 0.12 | 1.76 | 0.43 | 0.12 | 1.53 | 1.57 | 0.36 | 6.88 | 0.70 | 0.17 | 2.85 |
| Difference 55 vs. 25 | 0.29 | 0.10 | 0.85 | 1.68 | 0.55 | 5.15 | 0.44 | 0.15 | 1.31 | 0.55 | 0.20 | 1.46 | 1.26 | 0.38 | 4.22 | 0.78 | 0.27 | 2.29 |
| Difference 55 vs. 30 | 0.26 | 0.10 | 0.62 | 1.25 | 0.59 | 2.66 | 0.42 | 0.17 | 1.00 | 0.74 | 0.38 | 1.45 | 0.95 | 0.37 | 2.46 | 0.89 | 0.43 | 1.84 |
| Difference 55 vs. 35 | 0.23 | 0.10 | 0.53 | 0.93 | 0.54 | 1.60 | 0.40 | 0.17 | 0.91 | 1.01 | 0.60 | 1.70 | 0.72 | 0.31 | 1.67 | 1.02 | 0.59 | 1.75 |
| Difference 55 vs. 40 | 0.22 | 0.09 | 0.54 | 0.75 | 0.43 | 1.31 | 0.41 | 0.17 | 0.97 | 1.25 | 0.71 | 2.20 | 0.58 | 0.24 | 1.38 | 1.11 | 0.63 | 1.94 |
| Difference 55 vs. 45 | 0.30 | 0.14 | 0.63 | 0.74 | 0.45 | 1.21 | 0.51 | 0.25 | 1.02 | 1.28 | 0.78 | 2.10 | 0.59 | 0.27 | 1.25 | 1.11 | 0.69 | 1.79 |
| Difference 55 vs. 50 | 0.53 | 0.35 | 0.79 | 0.84 | 0.64 | 1.11 | 0.70 | 0.48 | 1.02 | 1.15 | 0.88 | 1.49 | 0.74 | 0.49 | 1.12 | 1.06 | 0.82 | 1.36 |
| Difference 55 vs. 60 | 1.90 | 1.27 | 2.86 | 1.19 | 0.90 | 1.56 | 1.42 | 0.98 | 2.07 | 0.87 | 0.67 | 1.13 | 1.35 | 0.89 | 2.04 | 0.94 | 0.73 | 1.21 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pomazal, R.; Malecki, K.M.C.; McCulley, L.; Stafford, N.; Schowalter, M.; Schultz, A. Changes in Alcohol Consumption during the COVID-19 Pandemic: Evidence from Wisconsin. Int. J. Environ. Res. Public Health 2023, 20, 5301. https://doi.org/10.3390/ijerph20075301
Pomazal R, Malecki KMC, McCulley L, Stafford N, Schowalter M, Schultz A. Changes in Alcohol Consumption during the COVID-19 Pandemic: Evidence from Wisconsin. International Journal of Environmental Research and Public Health. 2023; 20(7):5301. https://doi.org/10.3390/ijerph20075301
Chicago/Turabian StylePomazal, Rachel, Kristen M. C. Malecki, Laura McCulley, Noah Stafford, Mikayla Schowalter, and Amy Schultz. 2023. "Changes in Alcohol Consumption during the COVID-19 Pandemic: Evidence from Wisconsin" International Journal of Environmental Research and Public Health 20, no. 7: 5301. https://doi.org/10.3390/ijerph20075301