1. Introduction
Biomonitoring California is a legislatively mandated program that measures and tracks levels of selected environmental chemicals in people. Chemicals can be chosen for biomonitoring studies from the program’s list of designated chemicals [
1], which includes metals, perfluoroalkyl and polyfluoroalkyl substances, phenols, quaternary ammonium compounds, and many other chemical groups. The primary focus of these studies is to develop robust chemical exposure data, which can inform research by other groups exploring the linkages between these exposures and health. Biomonitoring California study results also help guide and evaluate the State’s efforts to reduce specific chemical exposures.
The enabling legislation, signed into law in 2006, requires trained program staff to consult with study participants and recommend follow-up steps if their biomonitoring results indicate a significant known health risk [
2]. To guide this process, Biomonitoring California’s Scientific Guidance Panel advised the program to adopt biological levels determined by state or federal agencies to be of concern (which we deem “levels of concern [LOCs]”). Of the chemicals we measure, we have identified LOCs for
total arsenic (urine), cadmium (blood and urine), lead (blood), and mercury (blood and urine). Total arsenic reflects both inorganic and organic forms; however, the inorganic form is of most concern for human health. We therefore developed a practical approach to identify and follow up on elevated
inorganic urinary arsenic levels, in addition to total arsenic.
Inorganic arsenic compounds are listed under California’s Proposition 65 (Title 27, California Code of Regulations, § 27001) as known to cause cancer and reproductive toxicity (developmental endpoint) [
3]. Human exposure to inorganic arsenic is also linked with other health effects, such as cardiovascular disease [
4,
5,
6,
7,
8] and neurotoxicity [
9,
10]. Inorganic arsenic has been detected in some groundwater sources [
11], public drinking water [
12], and cropland soils [
13] in California, making it an ongoing public health concern for the state. The Centers for Disease Control and Prevention (CDC) established a case definition for inorganic arsenic poisoning, which recommends speciation of urine samples with total arsenic levels > 50 μg/L but does not address inorganic arsenic levels [
14]. We adopted this value as our program’s LOC for total urinary arsenic. We did not identify an established LOC for urinary inorganic arsenic in the general population, nor an applicable urinary threshold for the toxic effects of inorganic arsenic from the scientific literature [
15]. Caldwell et al. [
16] statistically determined a “cut-point” of 20 µg/L for urinary inorganic arsenic, which we selected as the LOC for inorganic arsenic. Any participants with urinary inorganic arsenic at or above 20 µg/L are considered to have elevated levels. We use 20 µg/L total urinary arsenic to identify urine samples for speciation to ensure that all samples with potentially elevated inorganic arsenic are tested. This is a more health-protective approach than using the existing guidance value of 50 μg/L for total arsenic, while still practical in focusing on the most highly exposed participants for required follow-up. We also conducted literature research to develop a detailed survey about potentially important sources of inorganic arsenic exposures for impacted participants. Here, we discuss the results of applying this protocol in four example studies.
2. Methods
2.1. Biomonitoring California Studies
We illustrate the development and application of this protocol in four Biomonitoring California studies: the Maternal and Infant Environmental Exposure Project (MIEEP) [
17], the Firefighter Occupational Exposures (FOX) Project [
18,
19], the Pilot Biomonitoring Exposures Study (PBEST) [
20], and Expanded BEST (EBEST) [
21]. Study participants included Californians who may be particularly vulnerable to the effects of inorganic arsenic (e.g., pregnant women). Urine samples were collected and analyzed for arsenic, as part of a metals panel [
22], during the years 2010 to 2013. For MIEEP, FOX, and PBEST, the Environmental Health Laboratory (EHL) in the California Department of Public Health (CDPH) (one of Biomonitoring California’s laboratories) conducted the arsenic testing and speciation [
23]. For EBEST, Brooks Applied Labs (
https://brooksapplied.com/, accessed on 13 March 2023) conducted the testing to implement the arsenic protocol, due to limited program laboratory capacity at that time. All arsenic testing is now being conducted by EHL. We adhered to study protocols approved by the relevant Institutional Review Boards. More information on these example studies, including the other analytes measured, is available on the Biomonitoring California website [
24] and in selected Program publications [
25].
2.2. Development of Elevated Arsenic Protocol
2.2.1. Levels of Concern for Urinary Arsenic
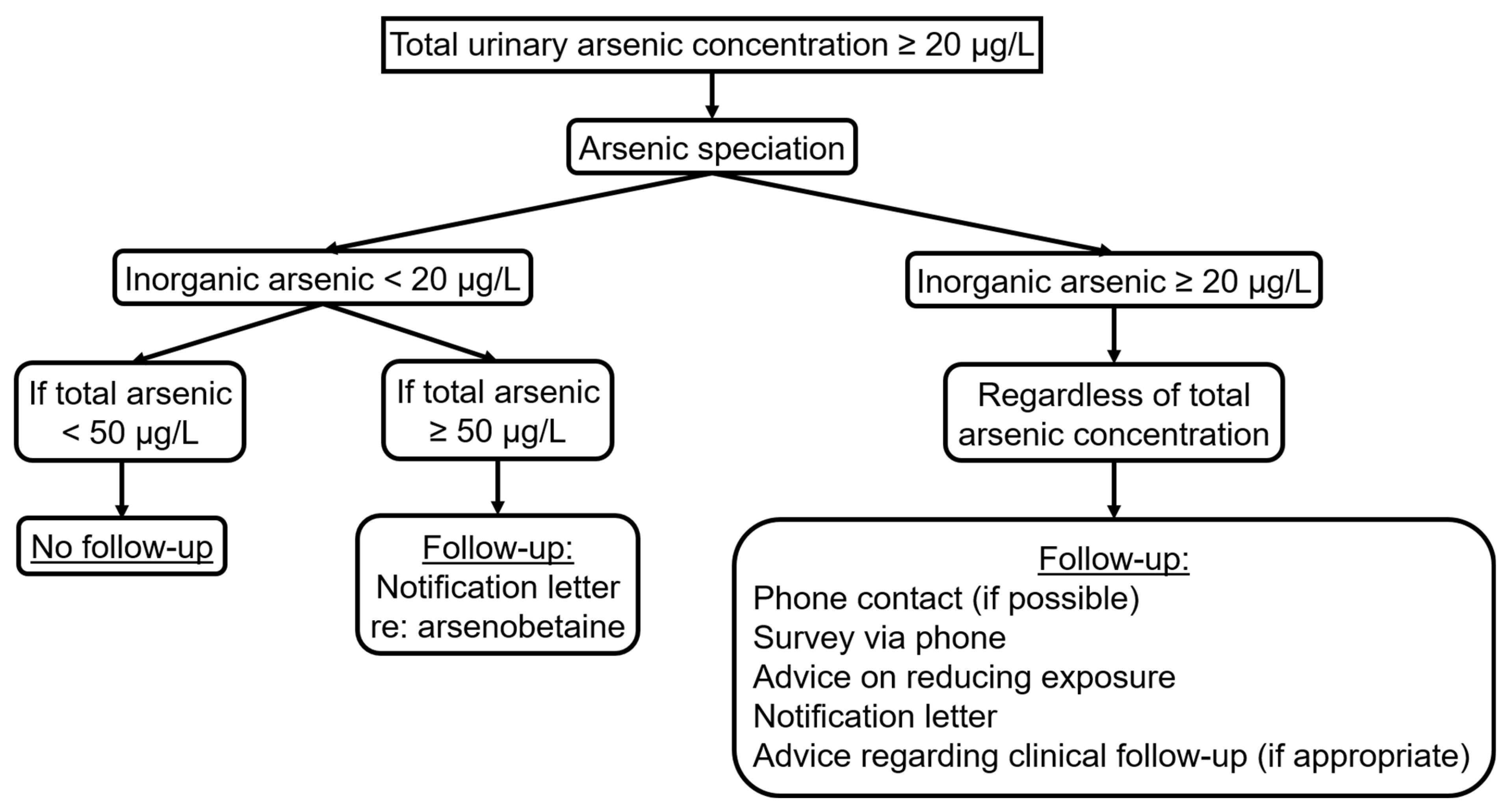
Biomonitoring California’s LOC for total urinary arsenic is ≥50 µg/L. We adopted the Caldwell et al. cut point of 20 µg/L as the LOC for urinary inorganic arsenic, which they defined as the sum of the metabolites dimethylarsinic acid (DMA), monomethylarsonic acid (MMA), arsenic (V) acid, and arsenous (III) acid. This corresponded roughly to the 95th percentile for a random one-third subsample of all participants (age ≥ 6 years) in the National Health and Nutrition Examination Survey (NHANES) 2003–2004 [
16]. To ensure that we capture all participants with urinary inorganic arsenic above the LOC, we use 20 µg/L total arsenic to identify samples for speciation.
2.2.2. Notification
As mandated by our enabling legislation, individual biomonitoring results are made available to study participants. The results packet includes fact sheets on the measured chemicals and other resources. For the four studies discussed here, participants with urinary inorganic arsenic levels ≥20 µg/L were initially contacted about their elevated results via a telephone call. As a health-protective measure, we also contacted one EBEST participant with 19.2 µg/L inorganic arsenic. For interested participants, the telephone survey on arsenic exposures (see
Section 2.2.3) was administered to help determine potential sources. Possible ways to reduce exposures were also discussed. Notification letters were mailed to all participants with urinary inorganic arsenic levels ≥20 µg/L, regardless of whether phone contact was successful. These letters included the speciated arsenic results and a fact sheet [
26] with possible ways to reduce exposures; this same information was provided again in the complete results packet. For participants who had not been reached by telephone, the letters included an invitation to contact us for administration of the voluntary survey.
Participants with total arsenic levels ≥ 50 µg/L and inorganic arsenic levels < 20 µg/L received a notification letter that their elevated urinary total arsenic levels were likely attributable to arsenobetaine from recent seafood consumption. The letter explained that this form of arsenic is not considered a health concern.
Participants with concerns or questions about their arsenic levels were offered the opportunity to speak with Dr. Craig Steinmaus, an arsenic expert and Public Health Medical Officer at the Office of Environmental Health Hazard Assessment (OEHHA).
2.2.3. Telephone Survey for Arsenic Exposures
Biomonitoring California study participants provide information on demographics and potential chemical exposures via surveys administered in person or online as part of the standard protocol. The goal of the additional telephone survey described here was to help identify arsenic exposure sources for participants with elevated urinary levels and address any concerns or questions related to their results. We based this survey on the arsenic poisoning case report form developed by the Florida Department of Health [
27] and expanded it to include questions about potentially important exposure sources gleaned from ongoing comprehensive literature searches. The additional questions covered consumption of rice and rice-based foods [
28,
29,
30], hijiki seaweed [
31], mushrooms [
32,
33], and some types of juice [
34,
35]; participants’ travel (e.g., to an international location) in the week prior to providing their urine sample; nutritional supplement intake [
36]; and other newly identified sources of arsenic. An example of the telephone survey is provided as a
Supplemental File. Trained staff administering the survey deviated from the script as needed to clarify participants’ answers or respond to questions.
2.3. Application of Elevated Arsenic Protocol
Figure 1 shows how the protocol was applied.
For the four studies discussed here, the telephone survey was administered 1.5 to 3 years following the collection of the urine samples. The delay was primarily due to lengthy recruitment periods and limited laboratory capacity. We informed participants that the survey was voluntary and that they could refuse to take it, skip questions, or stop at any time.
One survey question focused on the water source(s) used for drinking and cooking. For PBEST and EBEST, we also obtained average arsenic concentrations in local water systems from data used for the drinking water indicator in OEHHA’s CalEnviroScreen tool [
37].
3. Results
Table 1 provides brief descriptions of the four studies discussed in this paper. It also includes the numbers of urine samples analyzed for total arsenic; the subsets that were speciated; the samples with inorganic arsenic levels ≥20 µg/L; and response rates for the telephone survey.
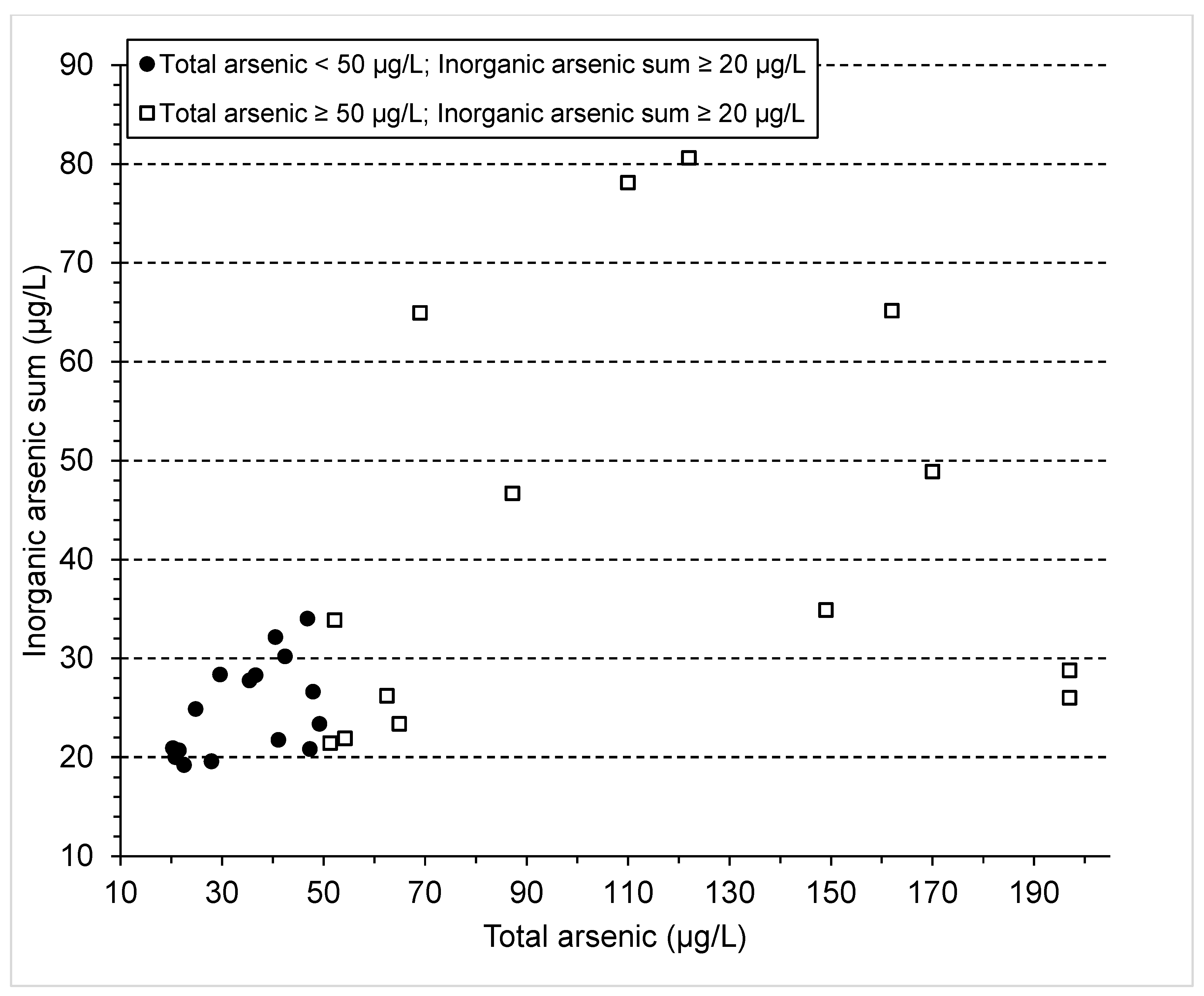
Results from the 30 EBEST participants with elevated urinary levels of inorganic arsenic are plotted in
Figure 2. Urinary inorganic arsenic levels ranged from 19.2 to 80.6 µg/L. Twenty-nine EBEST participants had levels of inorganic arsenic ≥ 20 µg/L. Fifteen of these would have been missed if we had speciated only the samples with total arsenic ≥50 µg/L instead of ≥20 µg/L.
The majority of EBEST participants (27/30) with elevated inorganic arsenic levels elected to take the telephone survey to help determine their potential exposure sources. Only one of the three remaining participants declined the survey; the other two could not be reached within our IRB-approved limit of three calls.
Table 2 displays some potential contributing sources of arsenic exposures identified from their responses and the supplementary drinking water information. Consumption of rice and rice-based products was the most common potential contributor to elevated inorganic arsenic, with seafood consumption likely responsible for elevated organic arsenic. Other possible sources of inorganic arsenic were beer, wine, and/or sake; hijiki seaweed; occupational exposures (see
Table 2); and drinking water.
The survey responses we obtained from FOX and PBEST participants identified similar potential arsenic exposure sources. Both FOX survey respondents reported consumption of rice and rice-based products as well as fish and/or shellfish. The three PBEST survey respondents also reported consumption of rice and rice-based products as well as fish and/or shellfish. Other possible inorganic arsenic sources identified for these PBEST participants included beer, wine, and/or sake consumption, and occupational exposures (e.g., employment at a glass manufacturing plant; contact with pressure-treated wood).
Participants’ reactions to learning about their elevated arsenic levels varied. In general, they were curious to learn more about arsenic and its sources, and in most cases they were not overly concerned. Some participants expressed concerns about health effects, the potential for ongoing exposures, and similar exposures for family members. Several participants questioned the relevance of results that were several years old and requested follow-up testing for themselves and others in their household, the latter of which was not possible under the study protocols. Given the large number of EBEST participants affected by the delay in arsenic speciation, we made special arrangements for participants who expressed interest in follow-up testing (25/30) to collect and ship additional urine samples. Due to logistics and other complications, only 15 of the 25 participants sent their urine samples for repeat analyses. These 15 participants all took the associated exposure survey, showing a high motivation to learn about their potential exposure sources.
4. Discussion
We developed a practical approach for identifying and following up with participants who had elevated urinary arsenic levels and illustrated its application in four Biomonitoring California studies. We chose 20 µg/L as the inorganic arsenic LOC, based on Caldwell et al. This is a statistically determined cut-point approximately corresponding to the 95th percentile of urinary inorganic arsenic from NHANES 2003–2004 for a subsample of all participants (age ≥ 6 years) [
16]. We examined the 95th percentile for urinary inorganic arsenic reported by CDC for random subsamples of all participants in subsequent NHANES cycles [
38]. It initially declined through the 2007–2008 cycle (16.8 µg/L), rising again in 2009–2010 (20.8 µg/L). Since then, it has steadily dropped (2011–2012: 17.2 µg/L; 2013–2014: 14.7 µg/L; 2015–2016: 14.5 µg/L; 2017–2018: 13.4 µg/L). Younger children (3–5 years) were included in the two most recent cycles. We have retained the Caldwell et al. [
16] cut-point of 20 µg/L as the inorganic arsenic LOC in the Biomonitoring California protocol, but the program could reevaluate this in the future, particularly if a clinically based value is established by CDC or other agencies.
We speciate all urine samples with total urinary arsenic ≥20 µg/L. This health-conservative approach identified a total of 27 participants in the four example studies with elevated inorganic arsenic whose total arsenic levels were less than 50 µg/L. If we had speciated only the samples with total arsenic ≥ 50 µg/L, these participants would not have received important follow up on their potentially harmful exposures to inorganic arsenic.
The telephone surveys consistently identified rice and rice-based products as a potential source of inorganic arsenic exposures for the PBEST, EBEST, and FOX participants with whom we were able to follow up. This is in line with information reported in other publications [
28,
39,
40].
Our findings on likely arsenic sources are limited by the small numbers of participants who completed the telephone survey in the example studies we chose to illustrate this protocol. The highest response rate was in EBEST. We attribute this in part to having current telephone numbers for almost all participants, because KPNC, our study partner, routinely updates members’ contact information. MIEEP participants were particularly difficult to reach, partially due to challenges in obtaining reliable contact information. Records for these prenatal patients were closed and stored by SF General after childbirth and were inaccessible to Biomonitoring California staff.
Following Caldwell et al. [
16], our protocol defines urinary inorganic arsenic as the sum of DMA, MMA, arsenic (V) acid, and arsenous (III) acid. However, DMA is not exclusively a metabolite of inorganic arsenic. There are some types of fish and shellfish that can contain high levels of organic arsenosugars and arsenolipids, which are metabolized by humans to DMA [
41,
42]. Therefore, our identification of elevated urinary inorganic arsenic for some participants could instead reflect DMA exposure from recent consumption of fish and shellfish. Our protocol uses one-on-one consultation with each participant to address the possible identification of some samples as having high inorganic arsenic when the source is more likely DMA from seafood consumption.
Some seafood might be actual sources of inorganic arsenic (e.g., some clams and crabs [
43]). However, we had insufficient information to determine how important this is for seafood consumed in California.
Extended study recruitment periods and limitations in laboratory capacity resulted in a time lag between participants’ urine sample collection and the administration of the telephone survey, particularly for EBEST. Given this delay, participants could have had difficulty in recalling information relevant to possible sources of inorganic arsenic exposures. For more recent program studies, the time lag has been reduced. For example, in the California Regional Exposure (CARE) Study, participants were offered the follow-up telephone survey within one month of identifying urine samples with elevated arsenic levels, which was typically within eight months of sample collection. CARE Study participants were also asked questions related to potential arsenic exposures at the time of urine sample collection, which improved data on likely sources.
5. Conclusions
Our protocol is a practical approach for identifying and following up with Biomonitoring California participants who are most highly exposed to arsenic, using speciation to evaluate their levels of urinary inorganic forms. The detailed telephone survey helps identify potentially important sources of inorganic arsenic exposures for these participants. We conduct individual consultations to delve into their specific exposures and provide an opportunity for them to ask questions and have their concerns addressed. We also explain that elevated arsenic levels linked to seafood consumption are not considered to be of concern. Setting 20 µg/L as the total urinary arsenic level to identify samples for speciation is a more health-protective approach than previously published guidance (i.e., 50 µg/L total arsenic). Choosing this lower level to screen samples is warranted by the serious health concerns associated with exposure to inorganic arsenic.
Author Contributions
Conceptualization, S.H.; Methodology, D.K. and C.S.; Investigation, D.K.; Data curation, S.I. and D.K.; Writing—original draft, S.I. and S.H.; Writing—review & editing, S.I., D.K., C.S. and S.H.; Supervision, S.H.; Project administration, S.H. All authors have read and agreed to the published version of the manuscript.
Funding
The four Biomonitoring California studies discussed in this paper were supported in part by external funding received from the Centers for Disease Control and Prevention (CDC) via Cooperative Agreement Numbers U38EH000481 and U88EH001148.
Institutional Review Board Statement
MIEEP was approved by the California Health & Human Services Agency Committee for the Protection of Human Subjects (CPHS) (Project No. 10-04-05 approved on 7 April 2010) and the University of California, San Francisco (UCSF) Human Research Protection Program Committee on Human Research (IRB #10-00861 approved on 26 March 2010). The FOX Project was approved by CPHS (Project No. 10-06-01 approved on 4 June 2010) and the University of California, Irvine (UC Irvine) Institutional Review Board (IRB #2010-7623 approved on 10 July 2010). Pilot BEST was approved by CPHS (Project No. 11-02-04 approved on 4 February 2011) and the Kaiser Permanente Northern California (KPNC) Institutional Review Board (IRB #CN-10SVanD-16-H approved on 20 January 2011). Expanded BEST was approved by CPHS (Protocol #12-05-0177, a continuation of Project No. 11-02-04, approved on 29 June 2012) and the KPNC IRB as an expansion of the Pilot BEST protocol (IRB #CN-10SVanD-16-H approved on 20 January 2011).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the four Biomonitoring California studies.
Data Availability Statement
Data are available upon request from the corresponding author, except when release of the data would compromise study participant identity.
Acknowledgments
We thank Stephen Van Den Eeden of KPNC Division of Research and co-principal investigator (co-PI) for BEST (Pilot and Expanded). We acknowledge Tracey Woodruff (UCSF co-PI), Rachel Morello-Frosch of UC Berkeley, and our other MIEEP collaborators. We also acknowledge Leslie Israel, who was UC Irvine co-PI for the FOX Project and is currently with the Los Angeles Department of Water & Power. We thank Biomonitoring California staff in CDPH for leadership in designing and implementing these four projects over many years. We acknowledge Daniel Sultana of OEHHA for reviewing the temporal trends in NHANES inorganic arsenic levels. We thank Komal Bangia of OEHHA for providing the CalEnviroScreen data on arsenic in drinking water. We are also grateful to Komal Bangia and Mark Miller of OEHHA for reviewing this manuscript and providing helpful feedback. We acknowledge other Biomonitoring California staff in OEHHA, CDPH, and the Department of Toxic Substances Control for ongoing input to this work. The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of OEHHA, the California Environmental Protection Agency, CDPH, the California Department of Health and Human Services, CDC, or the US Department of Health and Human Services.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Biomonitoring California. Designated Chemicals, June 2021. Available online: https://www.biomonitoring.ca.gov/sites/default/files/downloads/DesignatedChemicalsList_July2022.pdf (accessed on 13 January 2023).
- California Environmental Contaminant Biomonitoring Program. Codified at California Health and Safety Code, Section 105440 et seq. Available online: https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=200520060SB1379 (accessed on 13 March 2023).
- Office of Environmental Health Hazard Assessment (OEHHA). Chemicals Known to the State to Cause Cancer or Reproductive Toxicity. February 2022. Available online: https://oehha.ca.gov/proposition-65/proposition-65-list (accessed on 18 January 2023).
- Kuo, C.C.; Moon, K.A.; Wang, S.L.; Silbergeld, E.; Navas-Acien, A. The association of arsenic metabolism with cancer, cardiovascular disease, and diabetes: A systematic review of the epidemiological evidence. Environ. Health Perspect. 2017, 125, 087001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moon, K.A.; Oberoi, S.; Barchowsky, A.; Chen, Y.; Guallar, E.; Nachman, K.E.; Rahman, M.; Sohel, N.; D’Ippoliti, D.; Wade, T.J.; et al. A dose-response meta-analysis of chronic arsenic exposure and incident cardiovascular disease. Int. J. Epidemiol. 2017, 46, 1924–1939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuji, J.S.; Perez, V.; Garry, M.R.; Alexander, D.D. Association of low-level arsenic exposure in drinking water with cardiovascular disease: A systematic review and risk assessment. Toxicology 2014, 323, 78–94. [Google Scholar] [CrossRef] [PubMed]
- Moon, K.; Guallar, E.; Navas-Acien, A. Arsenic exposure and cardiovascular disease: An updated systematic review. Curr. Atheroscler. Rep. 2012, 14, 542–555. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Y.; Graziano, J.H.; Parvez, F.; Liu, M.; Slavkovich, V.; Kalra, T.; Argos, M.; Islam, T.; Ahmed, A.; Rakibuz-Zaman, M.; et al. Arsenic exposure from drinking water and mortality from cardiovascular disease in Bangladesh: Prospective cohort study. BMJ 2011, 342, d2431. [Google Scholar] [CrossRef] [Green Version]
- Sińczuk-Walczak, H.; Szymczak, M.; Hałatek, T. Effects of occupational exposure to arsenic on the nervous system: Clinical and neurophysiological studies. Int. J. Occup. Med. Environ. Health 2010, 23, 347–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasserman, G.A.; Liu, X.; Parvez, F.; Ahsan, H.; Factor-Litvak, P.; Kline, J.; Van Geen, A.; Slavkovich, V.; LoIacono, N.J.; Levy, D.; et al. Water arsenic exposure and intellectual function in 6-year-old children in Araihazar, Bangladesh. Environ. Health Perspect. 2007, 115, 285–289. [Google Scholar] [CrossRef]
- State Water Resources Control Board. Groundwater Information Sheet—Arsenic. Available online: https://www.waterboards.ca.gov/water_issues/programs/gama/docs/coc_arsenic.pdf (accessed on 15 February 2022).
- Balazs, C.; Bangia, K.; Depsky, N.; Renteria, A.; Morello-Frosch, R.; Cushing, L.J. Inequities in drinking water quality among domestic well communities and community water systems, California, 2011–2019. AJPH 2022, 112, 88–97. [Google Scholar]
- Chen, W.; Krage, N.; Wu, L.; Pan, G.; Khosrivafard, M.; Chang, A.C. Arsenic, cadmium, and lead in California cropland soils: Role of phosphate and micronutrient fertilizers. J. Environ. Qual. 2008, 37, 689–695. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Case Definitions for Chemical Poisoning. MMWR. Recomm. Rep. 2005, 54, 5–6. [Google Scholar]
- Schmidt, C.W. Low-dose arsenic: In search of a risk threshold. Environ Health Perspect. 2014, 122, A130–A134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caldwell, K.L.; Jones, R.L.; Verdon, C.P.; Jarrett, J.; Caudill, S.P.; Osterloh, J.D. Levels of urinary total and speciated arsenic in the US population: National Health and Nutrition Examination Survey 2003–2004. J. Expo. Sci. Environ. Epidemiol. 2009, 19, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Morello-Frosch, R.; Cushing, L.J.; Jesdale, B.M.; Schwartz, J.M.; Guo, W.; Guo, T.; Wang, M.; Harwani, S.; Petropoulou, S.S.E.; Duong, W.; et al. Environmental chemicals in an urban population of pregnant women and their newborns from San Francisco. Environ. Sci. Technol. 2016, 50, 12464–12472. [Google Scholar] [CrossRef]
- Dobraca, D.; Israel, L.; McNeel, S.; Voss, R.; Wang, M.; Gajek, R.; Park, J.S.; Harwani, S.; Barley, F.; She, J.; et al. Biomonitoring in California firefighters: Metals and perfluorinated chemicals. J. Occup. Environ. Med. 2015, 57, 88–97. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-S.; Voss, R.W.; McNeel, S.; Wu, N.; Guo, T.; Wang, Y.; Israel, L.; Das, R.; Petreas, M. High exposure of California firefighters to polybrominated diphenyl ethers. Environ. Sci. Technol. 2015, 49, 2948–2958. [Google Scholar] [CrossRef] [PubMed]
- Biomonitoring California. Biomonitoring Exposures Study (BEST)—1. Pilot. Available online: https://biomonitoring.ca.gov/projects/biomonitoring-exposures-study-best-1pilot (accessed on 18 October 2021).
- Biomonitoring California. Biomonitoring Exposures Study (BEST)—2. Expanded. Available online: https://biomonitoring.ca.gov/projects/biomonitoring-exposures-study-best-2expanded (accessed on 18 October 2021).
- Choe, K.Y.; Gajek, R. Determination of trace elements in human urine by ICP-MS using sodium chloride as a matrix-matching component in calibration. Anal. Methods 2016, 8, 6754–6763. [Google Scholar] [CrossRef]
- Sen, I.; Zou, W.; Alvaran, J.; Nguyen, L.; Gajek, R.; She, J. Development and validation of a simple and robust method for arsenic speciation in human urine using HPLC/ICP-MS. J. AOAC Int. 2015, 98, 517–523. [Google Scholar] [CrossRef] [PubMed]
- Biomonitoring California. All Projects. Available online: https://www.biomonitoring.ca.gov/projects/archive (accessed on 13 January 2023).
- Biomonitoring California. Biomonitoring California Publications. Available online: https://www.biomonitoring.ca.gov/biomonitoring-california-publications (accessed on 13 January 2023).
- Biomonitoring California. Arsenic Fact Sheet. 2018. Available online: https://biomonitoring.ca.gov/sites/default/files/ArsenicFactSheet.pdf (accessed on 6 July 2022).
- Florida Department of Health. Environmental Health Acute Arsenic Poisoning Case Report Form. 2009. Available online: http://www.floridahealth.gov/environmental-health/mercury-spills/mercury-poisoning/_documents/guidelines-for-arsenic.pdf (accessed on 18 October 2021).
- US Food and Drug Administration. Analytical Results from Inorganic Arsenic in Rice and Rice Products Sampling. 2013. Available online: https://www.fda.gov/media/86074/download (accessed on 18 October 2021).
- Cascio, C.; Raab, A.; Jenkins, R.O.; Feldmann, J.; Meharg, A.A.; Haris, P.I. The impact of a rice based diet on urinary arsenic. J. Environ. Monit. 2011, 13, 257–265. [Google Scholar] [CrossRef] [PubMed]
- deCastro, B.R.; Caldwell, K.L.; Jones, R.L.; Blount, B.C.; Pan, Y.; Ward, C.; Mortensen, M.E. Dietary sources of methylated arsenic species in urine of the United States population, NHANES 2003–2010. PLoS ONE 2014, 9, e108098. [Google Scholar] [CrossRef]
- Rose, M.; Lewis, J.; Langford, N.; Baxter, M.; Origgi, S.; Barber, M.; MacBain, H.; Thomas, K. Arsenic in seaweed—Forms, concentration and dietary exposure. Food Chem. Toxicol. 2007, 45, 1263–1267. [Google Scholar] [CrossRef]
- Nearing, M.M.; Koch, I.; Reimer, K.J. Arsenic speciation in edible mushrooms. Environ. Sci. Technol. 2014, 48, 14203–14210. [Google Scholar] [CrossRef] [PubMed]
- Seyfferth, A.L.; McClatchy, C.; Paukett, M. Arsenic, lead, and cadmium in U.S. mushrooms and substrate in relation to dietary exposure. Environ. Sci. Technol. 2016, 50, 9661–9670. [Google Scholar] [CrossRef] [PubMed]
- Conkin, S.D.; Chen, P.E. Quantification of four arsenic species in fruit juices by ion-chromatography-inductively coupled plasma-mass spectrometry. Food Addit. Contam. 2012, 29, 1272–1279. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.; Hooper, C.; Shi, X. Arsenic and lead in juice: Apple, citrus, and apple-base. J. Environ. Health 2012, 75, 14–20. [Google Scholar]
- Hedegaard, R.V.; Rokkjær, I.; Sloth, J.J. Total and inorganic arsenic in dietary supplements based on herbs, other botanicals and algae—A possible contributor to inorganic arsenic exposure. Anal. Bioanal. Chem. 2013, 405, 4429–4435. [Google Scholar] [CrossRef]
- Office of Environmental Health Hazard Assessment (OEHHA). California Communities Environmental Health Screening Tool, Version 2.0. (CalEnviroScreen 2.0). 2014. Available online: https://oehha.ca.gov/media/CES20FinalReportUpdateOct2014.pdf (accessed on 18 October 2021).
- CDC. National Report on Human Exposure to Environmental Chemicals. Biomonitoring Data Tables for Environmental Chemicals. Available online: https://www.cdc.gov/exposurereport/data_tables.html (accessed on 25 April 2022).
- Gilbert-Diamond, D.; Cottingham, K.L.; Gruber, J.F.; Punshon, T.; Sayarath, V.; Gandolfi, A.J.; Baker, E.R.; Jackson, B.P.; Folt, C.L.; Karagas, M.R. Rice consumption contributes to arsenic exposure in US women. Proc. Natl. Acad. Sci. USA 2011, 108, 20656–20660. [Google Scholar] [CrossRef] [Green Version]
- Mantha, M.; Yeary, E.; Trent, J.; Creed, P.A.; Kubachka, K.; Hanley, T.; Shockey, N.; Heitkemper, D.; Caruso, J.; Xue, J.; et al. Estimating inorganic arsenic exposure from U.S. rice and total water intakes. Environ. Health Perspect. 2017, 125, 057005. [Google Scholar] [CrossRef]
- Molin, M.; Ulven, S.M.; Meltzer, H.M.; Alexander, J. Arsenic in the human food chain, biotransformation and toxicology—Review focusing on seafood arsenic. J. Trace Elem. Med. Biol. 2015, 31, 249–259. [Google Scholar] [CrossRef] [Green Version]
- Navas-Acien, A.; Francesconi, K.A.; Silbergeld, E.K.; Guallar, E. Seafood intake and urine concentrations of total arsenic, dimethylarsinate and arsenobetaine in the US population. Environ. Res. 2011, 111, 110–118. [Google Scholar] [CrossRef] [Green Version]
- Wolle, M.M.; Stadig, S.; Conklin, S.D. Market basket survey of arsenic species in the top ten most consumed seafoods in the United States. J. Agric. Food Chem. 2019, 67, 8253–8267. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}
{kind=link}