
Occupational Risk Factors by Sectors: An Observational Study of 20,000 Workers
 , , ,
, , ,  , , , , and
, , , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Sample
2.3. Occupational Risk Factors
2.4. Sectors of Activity
2.5. Statistics
3. Results


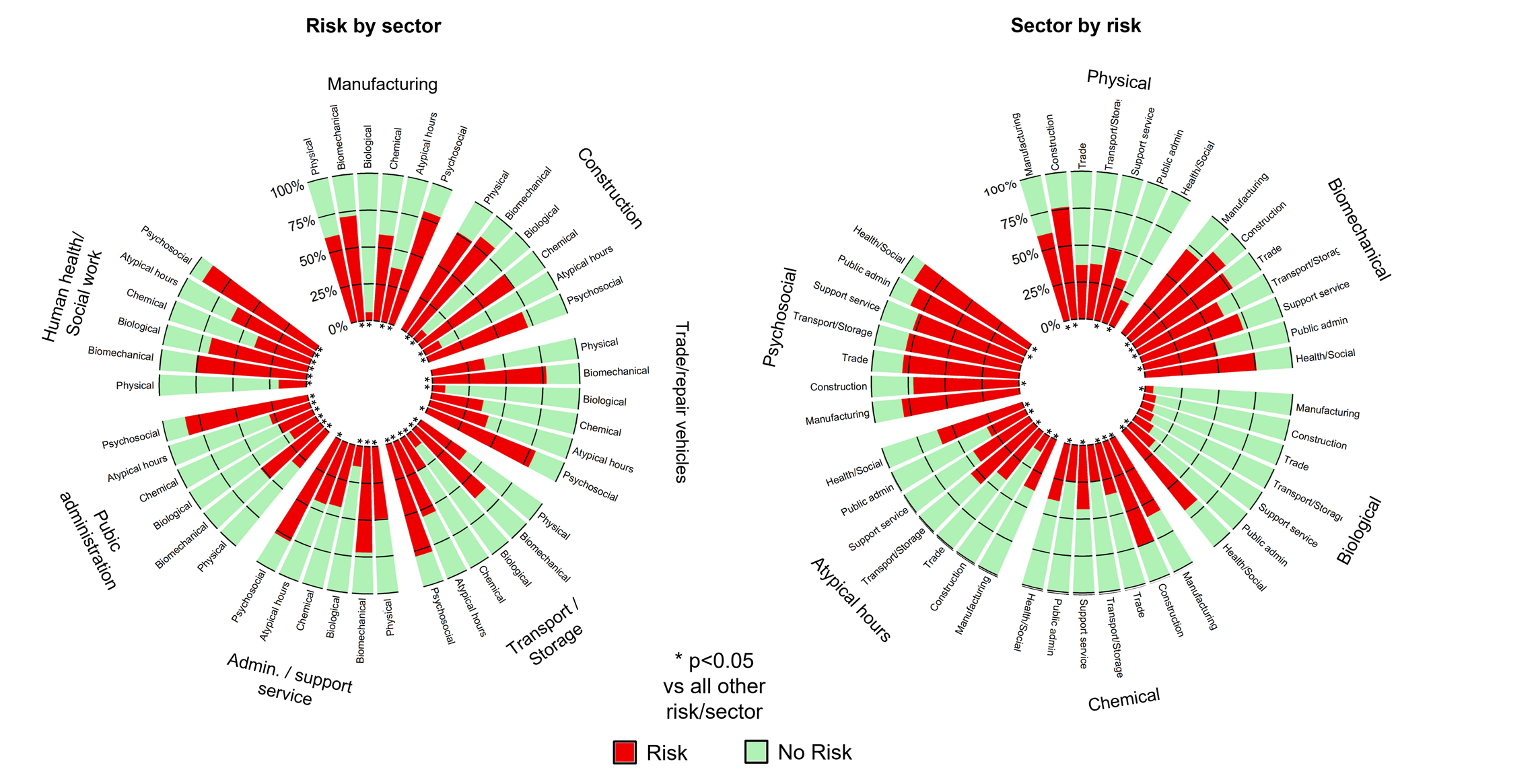
3.1. Prevalence of Occupational Risk Factors by Sector (Risks by Sector)
3.2. Prevalence of Sectors for Each Occupational Risk Factor (Sectors by Risk)
3.3. Odds Ratio for each Sector by Risk

4. Discussion
4.1. Prevalence
4.2. Odds Ratios
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Details of the Composition of Exposure Groups
| Physical factors | Noise |
| Working in bad weather | |
| Vibrating machines and tools | |
| Ultrasound | |
| Extreme temperatures (hot or cold) | |
| Non-ionizing radiation | |
| Ionizing radiation | |
| Biomechanical factors | Awkward postures |
| Handling and carrying of loads | |
| Repetitive motions | |
| Biological factors | Work in contact with humans or products of human origin |
| Waste treatment and disposal | |
| Processing in the environment or in the food industry | |
| Work in contact with animals or their products | |
| Chemical agents | Handling chemicals or cosmetics |
| Exposure to fumes, gases, and/or dust | |
| Fiber (asbestos, refractory ceramic, insulation wool, etc.) | |
| Atypical hours | Weekend work |
| Working irregular hours | |
| Work in alternating shifts | |
| Night work | |
| Night shifts | |
| Psychosocial factors | Emotional demands of the job |
| Work requirements | |
| Autonomy of organization | |
| Socioeconomic fears | |
| Support at work (colleagues, employer, supervisor) | |
| Recognition at work (colleagues, employer, supervisor) | |
| Conflict at work |
Appendix B. Details of the Activities Related to Each Sector
| Administrative and support service activities | Rental and leasing activities, employment-related activities, investigation and security, building and landscape maintenance services, other support activities |
| Manufacturing | Manufacturing of food, beverages, tobacco-based products, textiles, and others |
| Construction | All construction activities |
| Wholesale and retail trade, repair of motor vehicles and motorbikes | Wholesale and retail trade, and repair of automobiles and motorcycles |
| Transport and storage | Land transportation and pipeline transportation, postal and courier activities, storage, and transportation support services |
| Public administration | Public administration and defense, compulsory social security |
| Human health and social work | Human health activities, medical and social care, and social action without accommodation |
Appendix C. Table for the Interpretation of Cramer’s V
| Cramer’s V | Interpretation |
|---|---|
| > 0.25 | Very strong |
| > 0.15 | Strong |
| > 0.10 | Moderate |
| > 0.05 | Weak |
| > 0 | No or very weak |
Appendix D. Frequency Tables of Workers Included in the Study
| Sectors | n (%) | Men | Women |
|---|---|---|---|
| Manufacturing | 3145 (15.8) | 994 (31.7) | 2141 (68.3) |
| Construction | 4351 (21.8) | 1083 (25.7) | 3135 (74.3) |
| Wholesale and retail trade, and repair of motor vehicles and motorbikes | 1998 (10.0) | 120 (6.0) | 1873 (94.0) |
| Transport and storage | 3752 (18.9) | 1445 (38.7) | 2293 (61.3) |
| Administrative and support service activities | 1556 (5.8) | 165 (14.5) | 977 (85.6) |
| Public administration | 2256 (11.3) | 1441 (64.0) | 811 (36.0) |
| Human health and social work | 3233 (16.3) | 2521 (78.0) | 712 (22.0) |
| Total | 19,711 (100) | 7769 (39.4) | 11,942 (60.6) |
Appendix E. Heatmap of Cramer’s V (i.e., Effect Size (ES)): Sectors by Risks

References
- Si, S.; Lewkowski, K.; Fritschi, L.; Heyworth, J.; Liew, D.; Li, I. Productivity Burden of Occupational Noise-Induced Hearing Loss in Australia: A Life Table Modelling Study. Int. J. Environ. Res. Public Health 2020, 17, 4667. [Google Scholar] [CrossRef] [PubMed]
- Fadel, M.; Evanoff, B.; Andersen, J.H.; D’Errico, A.; Dale, A.M.; Leclerc, A.; Descatha, A. Not just a research method: If used with caution, can job-exposure matrices be a useful tool in the practice of occupational medicine and public health? Scand. J. Work. Environ. Health 2020, 46, 552–553. [Google Scholar] [CrossRef] [PubMed]
- Scarselli, A.; Corfiati, M.; Di Marzio, D.; Marinaccio, A.; Iavicoli, S. Gender differences in occupational exposure to carcinogens among Italian workers. BMC Public Health 2018, 18, 413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Havet, N.; Penot, A.; Morelle, M.; Perrier, L.; Charbotel, B.; Fervers, B. Varied exposure to carcinogenic, mutagenic, and reprotoxic (CMR) chemicals in occupational settings in France. Int. Arch. Occup. Environ. Health 2017, 90, 227–241. [Google Scholar] [CrossRef]
- Kromhout, H.; Symanski, E.; Rappaport, S.M. A comprehensive evaluation of within- and between-worker components of occupational exposure to chemical agents. Ann. Occup. Hyg. 1993, 37, 253–270. [Google Scholar] [CrossRef] [Green Version]
- Hulshof, C.T.; Pega, F.; Neupane, S.; van der Molen, H.F.; Colosio, C.; Daams, J.G.; Descatha, A.; Kc, P.; Kuijer, P.P.; Mandic-Rajcevic, S.; et al. The prevalence of occupational exposure to ergonomic risk factors: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ. Int. 2021, 146, 106157. [Google Scholar] [CrossRef]
- Mathieu, S.; Naughton, G.; Descatha, A.; Soubrier, M.; Dutheil, F. Dupuytren’s Disease and exposure to vibration: Systematic review and Meta-analysis. Jt. Bone Spine 2020, 87, 203–207. [Google Scholar] [CrossRef]
- Pearce, M.; Strain, T.; Wijndaele, K.; Sharp, S.J.; Mok, A.; Brage, S. Is occupational physical activity associated with mortality in UK Biobank? Int. J. Behav. Nutr. Phys. Act. 2021, 18, 102. [Google Scholar] [CrossRef]
- Themann, C.L.; Masterson, E.A. Occupational noise exposure: A review of its effects, epidemiology, and impact with recommendations for reducing its burden. J. Acoust. Soc. Am. 2019, 146, 3879. [Google Scholar] [CrossRef] [Green Version]
- Nataletti, P.; Bogi, A.; Borra, M.; Gioia, D.; Falsaperla, R.; Marchetti, E.; Militello, A.; Nicolini, O.; Rossi, P.; Sacco, F.; et al. Occupational Exposure to Physical Agents: The New Italian Database for Risk Assessment and Control. Int. J. Occup. Saf. Ergon. 2014, 20, 407–420. [Google Scholar] [CrossRef] [Green Version]
- Baussano, I.; Nunn, P.; Williams, B.; Pivetta, E.; Bugiani, M.; Scano, F. Tuberculosis among Health Care Workers. Emerg. Infect. Dis. 2011, 17, 488–494. [Google Scholar] [CrossRef]
- Fitzsimons, D.; François, G.; De Carli, G.; Shouval, D.; Pruss-Ustun, A.; Puro, V.; Williams, I.; Lavanchy, D.; De Schryver, A.; Kopka, A.; et al. Hepatitis B virus, hepatitis C virus and other blood-borne infections in healthcare workers: Guidelines for prevention and management in industrialised countries. Occup. Environ. Med. 2008, 65, 446–451. [Google Scholar] [CrossRef]
- Leroyer, A.; Molinié, A.-F.; Buisset, C.; Archambault, C.; Volkoff, S. Equipe Projet Nationale EVREST: The EVREST plan: Establishing an observatory through an occupational health questionnaire. Sante Publique 2008, 20, S49–S56. [Google Scholar] [CrossRef]
- Gan, W.Q.; Davies, H.W.; Demers, A.P. Exposure to occupational noise and cardiovascular disease in the United States: The National Health and Nutrition Examination Survey 1999–2004. Occup. Environ. Med. 2011, 68, 183–190. [Google Scholar] [CrossRef] [Green Version]
- Havet, N.; Fournier, J.; Stefanelli, J.; Plantier, M.; Penot, A. Disparate exposure to physically demanding working conditions in France. Rev. D'épidémiologie St. Publique 2020, 68, 327–336. [Google Scholar] [CrossRef]
- Weinberg, A.; Creed, F. Stress and psychiatric disorder in healthcare professionals and hospital staff. Lancet 2000, 355, 533–537. [Google Scholar] [CrossRef]
- Utzet, M.; Moncada, S.; Molinero, E.; Llorens, C.; Moreno, N.; Navarro, A. The changing patterns of psychosocial exposures at work in the South of Europe: Spain as a labor market laboratory. Am. J. Ind. Med. 2014, 57, 1032–1042. [Google Scholar] [CrossRef]
- Leroyer, A.; Murcia, M.; Chastang, J.-F.; Rollin, L.; Volkoff, S.; Molinié, A.-F.; Niedhammer, I. Weighting Methodology for the National EVREST Survey Data. Sante Publique 2020, 31, 645–655. [Google Scholar] [CrossRef]
- Corrao, C.R.N.; Mazzotta, A.; LA Torre, G.; DE Giusti, M. Biological Risk and Occupational Health. Ind. Health 2012, 50, 326–337. [Google Scholar] [CrossRef] [Green Version]
- Squicciarini, M.; Asikainen, A.-L. A value chain statistical definition of construction and the performance of the sector. Constr. Manag. Econ. 2011, 29, 671–693. [Google Scholar] [CrossRef]
- Kusideł, E.; Antczak, E. The Polish Labour Force by Industry in 1995–2019: Estimates Based on a New Classification of Economic Activities. Gospod. Nar. Pol. J. Econ. 2021, 307, 125–144. [Google Scholar] [CrossRef]
- Fourneau, C.; Sanchez, M.; Perouel, G.; Frery, N.; Coutrot, T.; Boulanger, G.; Courrier, B.; Pernelet-Joly, V.; Bastos, H. Plan santé au travail 2016–2020: Mieux connaître la polyexposition. Environ. Risques Santé 2021, 20, 377–382. [Google Scholar] [CrossRef]
- Burström, L.; Järvholm, B.; Nilsson, T.; Wahlström, J. White fingers, cold environment, and vibration—Exposure among Swedish construction workers. Scand. J. Work. Environ. Health 2010, 36, 509–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewkowski, K.; Ytterstad, E.; Pugliese, M.J.; McCausland, K.; Heyworth, J.S.; Li, I.W.; Pettersson, H.; Williams, W.; Fritschi, L. Exposure to Hand-Arm Vibration in the Australian Workforce. Ann. Work. Expo. Health 2021, 65, 659–667. [Google Scholar] [CrossRef]
- Konkani, A.; Oakley, B. Noise in hospital intensive care units—A critical review of a critical topic. J. Crit. Care 2012, 27, 522.e1–522.e9. [Google Scholar] [CrossRef]
- Teixeira, L.R.; Pega, F.; de Abreu, W.; de Almeida, M.S.; de Andrade, C.A.; Azevedo, T.M.; Dzhambov, A.M.; Hu, W.; Macedo, M.R.; Martínez-Silveira, M.S.; et al. The prevalence of occupational exposure to noise: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ. Int. 2021, 154, 106380. [Google Scholar] [CrossRef]
- Bertin, M.; Nguyen, T.; Bonvallot, N.; Bodin, J.; Roquelaure, Y. Occupational co-exposure to biomechanical factors and neurotoxic chemicals in a representative sample of French employees. J. Occup. Health 2019, 62, e12090. [Google Scholar] [CrossRef]
- van der Kolk, B. Performance measurement in the public sector: Mapping 20 years of survey research. Financ. Account. Manag. 2022, 38, 703–729. [Google Scholar] [CrossRef]
- Deltreil, G.; Tardivel, P.; Graczyk, P.; Escobar-Bach, M.; Descatha, A. How to Use Biomechanical Job Exposure Matrices with Job History to Access Work Exposure for Musculoskeletal Disorders? Application of Mathematical Modeling in Severe Knee Pain in the Constances Cohort. Int. J. Environ. Res. Public Health 2022, 19, 16217. [Google Scholar] [CrossRef]
- Punnett, L.; Prüss-Ütün, A.; Nelson, D.I.; Fingerhut, M.A.; Leigh, J.; Tak, S.; Phillips, S. Estimating the global burden of low back pain attributable to combined occupational exposures. Am. J. Ind. Med. 2005, 48, 459–469. [Google Scholar] [CrossRef]
- Boström, M.; Dellve, L.; Thomée, S.; Hagberg, M. Risk factors for generally reduced productivity—A prospective cohort study of young adults with neck or upper-extremity musculoskeletal symptoms. Scand. J. Work. Environ. Health 2008, 34, 120–132. [Google Scholar] [CrossRef] [Green Version]
- Geuskens, G.; Hazes, J.M.W.; Barendregt, P.J.; Burdorf, A. Predictors of sick leave and reduced productivity at work among persons with early inflammatory joint conditions. Scand. J. Work. Environ. Health 2008, 34, 420–429. [Google Scholar] [CrossRef]
- Burdorf, A. The role of assessment of biomechanical exposure at the workplace in the prevention of musculoskeletal disorders. Scand. J. Work. Environ. Health 2010, 36, 1–2. [Google Scholar] [CrossRef] [Green Version]
- Montano, D. Chemical and biological work-related risks across occupations in Europe: A review. J. Occup. Med. Toxicol. 2014, 9, 28. [Google Scholar] [CrossRef] [Green Version]
- Kauppinen, T.; Uuksulainen, S.; Saalo, A.; Mäkinen, I. Trends of Occupational Exposure to Chemical Agents in Finland in 1950––2020. Ann. Occup. Hyg. 2013, 57, 593–609. [Google Scholar] [CrossRef]
- Davies, H.W.; Gorman-Ng, M. Development of a Web-Based Tool for Risk Assessment and Exposure Control Planning of Silica-Producing Tasks in the Construction Sector. Front. Public Health 2020, 8, 371. [Google Scholar] [CrossRef]
- Leger, D.; Esquirol, Y.; Gronfier, C.; Metlaine, A. Le travail posté et de nuit et ses conséquences sur la santé: état des lieux et recommandations. La Presse Médicale 2018, 47, 991–999. [Google Scholar] [CrossRef]
- Roquelaure, Y.; Ha, C.; Gohier, B.; Dano, C.; Touranchet, A.; Leclerc, A.; Imbernon, E.; Goldberg, M. Exposition au stress psychosocial chez les salariés des Pays de la Loire en 2002. L’Encéphale 2007, 33, 160–168. [Google Scholar] [CrossRef]
- Rollin, L.; Gehanno, J.-F.; Leroyer, A. Occupational stressors in healthcare workers in France. Rev. D'épidémiologie St. Publique 2022, 70, 59–65. [Google Scholar] [CrossRef]
- Yang, Y.; Chan, A.P.-C. Heat stress intervention research in construction: Gaps and recommendations. Ind. Health 2017, 55, 201–209. [Google Scholar] [CrossRef] [Green Version]
- Capodaglio, E.M. Occupational risk and prolonged standing work in apparel sales assistants. Int. J. Ind. Ergon. 2017, 60, 53–59. [Google Scholar] [CrossRef]
- Kim, S.; Yoon, C.; Ham, S.; Park, J.; Kwon, O.; Park, D.; Choi, S.; Kim, S.; Ha, K.; Kim, W. Chemical use in the semiconductor manufacturing industry. Int. J. Occup. Environ. Health 2018, 24, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Groh, K.J.; Backhaus, T.; Carney-Almroth, B.; Geueke, B.; Inostroza, P.A.; Lennquist, A.; Leslie, H.A.; Maffini, M.; Slunge, D.; Trasande, L.; et al. Overview of known plastic packaging-associated chemicals and their hazards. Sci. Total. Environ. 2019, 651, 3253–3268. [Google Scholar] [CrossRef] [PubMed]
- Galey, L.; Albert, M.; Brossard, M.; Noël-Suberville, C.; Garrigou, A. Industry 4.0 design project based on exposure situations: A case study in aeronautics. Work 2022, 73, S223–S234. [Google Scholar] [CrossRef] [PubMed]
- Fort, E.; Gadegbeku, B.; Gat, E.; Pelissier, C.; Hours, M.; Charbotel, B. Working conditions and risk exposure of employees whose occupations require driving on public roads—Factorial analysis and classification. Accid. Anal. Prev. 2019, 131, 254–267. [Google Scholar] [CrossRef] [Green Version]
- Pearce, N.; Checkoway, H.; Kriebel, D. Bias in occupational epidemiology studies. Occup. Environ. Med. 2007, 64, 562–568. [Google Scholar] [CrossRef] [Green Version]
- Althubaiti, A. Information bias in health research: Definition, pitfalls, and adjustment methods. J. Multidiscip. Healthc. 2016, 9, 211–217. [Google Scholar] [CrossRef] [Green Version]
- Donnay, C.; Denis, M.-A.; Magis, R.; Fevotte, J.; Massin, N.; Dumas, O.; Pin, I.; Choudat, D.; Kauffmann, F.; Le Moual, N. Under-estimation of self-reported occupational exposure by questionnaire in hospital workers. Occup. Environ. Med. 2011, 68, 611–617. [Google Scholar] [CrossRef] [Green Version]
- Jager, K.; Zoccali, C.; MacLeod, A.; Dekker, F. Confounding: What it is and how to deal with it. Kidney Int. 2008, 73, 256–260. [Google Scholar] [CrossRef] [Green Version]
- Mannetje, A.; Kromhout, H. The use of occupation and industry classifications in general population studies. Int. J. Epidemiol. 2003, 32, 419–428. [Google Scholar] [CrossRef] [Green Version]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dogbla, L.; Gouvenelle, C.; Thorin, F.; Lesage, F.-X.; Zak, M.; Ugbolue, U.C.; Charbotel, B.; Baker, J.S.; Pereira, B.; Dutheil, F. Occupational Risk Factors by Sectors: An Observational Study of 20,000 Workers. Int. J. Environ. Res. Public Health 2023, 20, 3632. https://doi.org/10.3390/ijerph20043632
Dogbla L, Gouvenelle C, Thorin F, Lesage F-X, Zak M, Ugbolue UC, Charbotel B, Baker JS, Pereira B, Dutheil F. Occupational Risk Factors by Sectors: An Observational Study of 20,000 Workers. International Journal of Environmental Research and Public Health. 2023; 20(4):3632. https://doi.org/10.3390/ijerph20043632
Chicago/Turabian StyleDogbla, Luther, Cédric Gouvenelle, Florence Thorin, François-Xavier Lesage, Marek Zak, Ukadike Chris Ugbolue, Barbara Charbotel, Julien S. Baker, Bruno Pereira, and Frédéric Dutheil. 2023. "Occupational Risk Factors by Sectors: An Observational Study of 20,000 Workers" International Journal of Environmental Research and Public Health 20, no. 4: 3632. https://doi.org/10.3390/ijerph20043632