

Microbial Air Contamination in a Dental Setting Environment and Ultrasonic Scaling in Periodontally Healthy Subjects: An Observational Study
 , , , , , , ,
, , , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Ultrasonic Scaling Procedures
2.3. Operating Area Disinfection and Cleaning Procedures
- Cleaning and disinfecting all operating room surfaces;
- Cleaning the surfaces and handles of the furniture;
- Disinfecting the dental chair in the open and closed positions, especially the equipment that cannot be sterilized or the most frequently touched parts.
2.4. Air Samples Collection
- -
- the availability and adequacy of the materials and equipment necessary for the collection, preparation, and shipment of samples;
- -
- the verification of the sterile buffer solution used to collect and ship the samples for the absence of turbidity, flocculation, debris, or other foreign matter;
- -
- the availability of the laboratory to receive and process the samples on schedule (within a maximum of 24 h after sample collection, keeping them refrigerated).
2.5. Colony-Forming Unit Assessment
2.6. Statistical Analysis
3. Results
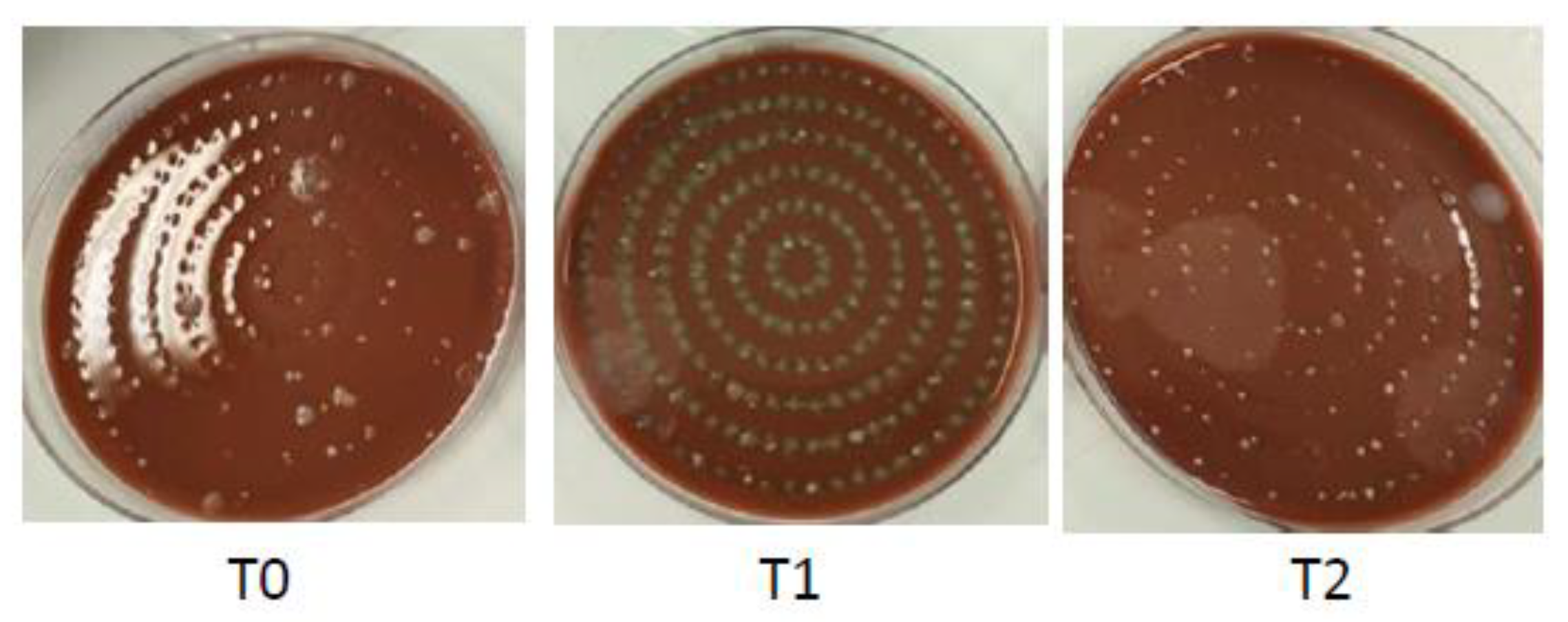
3.1. Air Samples Collected before Starting the Ultrasonic Scaling (T0)
3.2. Air Samples Collected during the Ultrasonic Scaling (T1)
3.3. Air Samples Collected Immediately after the Ultrasonic Scaling (T2)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amato, A. Oral-Systemic Health and Disorders: Latest Advances on Oral–Gut–Lung Microbiome Axis. Appl. Sci. 2022, 12, 8213. [Google Scholar] [CrossRef]
- Harrel, S.K.; Molinari, J. Aerosols and Splatter in Dentistry. J. Am. Dent. Assoc. 2004, 135, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Ishihama, K. Occupational Safety among Dental Health-Care Workers. Adv. Med. Educ. Pract. 2010, 1, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; di Spirito, F.; D’Ambrosio, F.; Boccia, G.; Moccia, G.; de Caro, F. Probiotics in Periodontal and Peri-Implant Health Management: Biofilm Control, Dysbiosis Reversal, and Host Modulation. Microorganisms 2022, 10, 2289. [Google Scholar] [CrossRef]
- Fennelly, M.; Gallagher, C.; Harding, M.; Hellebust, S.; Wenger, J.; O’Sullivan, N.; O’Connor, D.; Prentice, M. Real-Time Monitoring of Aerosol Generating Dental Procedures. J. Dent. 2022, 120, 104092. [Google Scholar] [CrossRef]
- Innes, N.; Johnson, I.G.; Al-Yaseen, W.; Harris, R.; Jones, R.; KC, S.; McGregor, S.; Robertson, M.; Wade, W.G.; Gallagher, J.E. A Systematic Review of Droplet and Aerosol Generation in Dentistry. J. Dent. 2021, 105, 103556. [Google Scholar] [CrossRef]
- Sehulster, L.; Chinn, R.Y.W. HICPAC Guidelines for Environmental Infection Control in Health-Care Facilities. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC). MMWR Recomm. Rep. 2003, 52, 1–42. [Google Scholar]
- Micik, R.E.; Miller, R.L.; Mazzarella, M.A.; Ryge, G. Studies on Dental Aerobiology: I. Bacterial Aerosols Generated during Dental Procedures. J. Dent. Res. 1969, 48, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.L.; Micik, R.E.; Abel, C.; Ryge, G. Studies on Dental Aerobiology: II. Microbial Splatter Discharged from the Oral Cavity of Dental Patients. J. Dent. Res. 1971, 50, 621–625. [Google Scholar] [CrossRef]
- Micik, R.E.; Miller, R.L.; Leong, A.C. Studies on Dental Aerobiology: III. Efficacy of Surgical Masks in Protecting Dental Personnel from Airborne Bacterial Particles. J. Dent. Res. 1971, 50, 626–630. [Google Scholar] [CrossRef]
- Abel, L.C.; Miller, R.L.; Micik, R.E.; Ryge, G. Studies on Dental Aerobiology: IV. Bacterial Contamination of Water Delivered by Dental Units. J. Dent. Res. 1971, 50, 1567–1569. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.L.; Micik, R.E. Air Pollution and Its Control in the Dental Office. Dent. Clin. North. Am. 1978, 22, 453–476. [Google Scholar] [CrossRef]
- Dudding, T.; Sheikh, S.; Gregson, F.; Haworth, J.; Haworth, S.; Main, B.G.; Shrimpton, A.J.; Hamilton, F.W.; Ireland, A.J.; Maskell, N.A.; et al. A Clinical Observational Analysis of Aerosol Emissions from Dental Procedures. PLoS ONE 2022, 17, e0265076. [Google Scholar] [CrossRef]
- Ou, Q.; Placucci, R.G.; Danielson, J.; Anderson, G.; Olin, P.; Jardine, P.; Madden, J.; Yuan, Q.; Grafe, T.H.; Shao, S.; et al. Characterization and Mitigation of Aerosols and Spatters from Ultrasonic Scalers. J. Am. Dent. Assoc. 2021, 152, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Setti, L.; Passarini, F.; de Gennaro, G.; Barbieri, P.; Perrone, M.G.; Borelli, M.; Palmisani, J.; di Gilio, A.; Piscitelli, P.; Miani, A. Airborne Transmission Route of COVID-19: Why 2 Meters/6 Feet of Inter-Personal Distance Could Not Be Enough. Int. J. Environ. Res. Public Health 2020, 17, 2932. [Google Scholar] [CrossRef] [PubMed]
- Matys, J.; Grzech-Leśniak, K. Dental Aerosol as a Hazard Risk for Dental Workers. Materials 2020, 13, 5109. [Google Scholar] [CrossRef]
- Veena, H.R.; Mahantesha, S.; Joseph, P.A.; Patil, S.R.; Patil, S.H. Dissemination of Aerosol and Splatter during Ultrasonic Scaling: A Pilot Study. J. Infect. Public Health 2015, 8, 260–265. [Google Scholar] [CrossRef]
- Nóbrega, M.T.C.; Bastos, R.T.D.R.M.; Mecenas, P.; Toledo, I.P.; Richardson-Lozano, R.; Altabtbaei, K.; Flores-Mir, C. Aerosol Generated by Dental Procedures: A Scoping Review. J. Evid. Based Med. 2021, 14, 303–312. [Google Scholar] [CrossRef]
- Virdi, M.K.; Durman, K.; Deacon, S. The Debate: What Are Aerosol-Generating Procedures in Dentistry? A Rapid Review. JDR Clin. Transl. Res. 2021, 6, 115–127. [Google Scholar] [CrossRef]
- van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and Surface Stability of HCoV-19 (SARS-CoV-2) Compared to SARS-CoV-1. medRxiv 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Bennett, A.M.; Fulford, M.R.; Walker, J.T.; Bradshaw, D.J.; Martin, M.V.; Marsh, P.D. Microbial Aerosols in General Dental Practice. Br. Dent. J. 2000, 189, 664–667. [Google Scholar] [CrossRef] [PubMed]
- Ventilation, Water and Environmental Cleaning in Dental Surgeries Relating to COVID-19 National Service Scothland. Available online: https://Www.Scottishdental.Org/Ventilation-Water-and-Environmentalcleaning-in-Dental-Surgeries-Relating-to-Covid-19/ (accessed on 20 August 2020).
- NHS Dental Statistics for England—2019-20 Annual Report. Available online: https://Digital.Nhs.Uk/Data-and-Information/Publications/Statistical/Nhsdental-Statistics/2019-20-Annual-Report (accessed on 7 November 2020).
- Gandolfi, M.G.; Zamparini, F.; Spinelli, A.; Sambri, V.; Prati, C. Risks of Aerosol Contamination in Dental Procedures during the Second Wave of COVID-19—Experience and Proposals of Innovative IPC in Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 8954. [Google Scholar] [CrossRef] [PubMed]
- Arabaci, T.; Çiçek, Y.; Çanakçi, C. Sonic and Ultrasonic Scalers in Periodontal Treatment: A Review. Int. J. Dent. Hyg. 2007, 5, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and Surgical Treatment of Periodontitis: How Many Options for One Disease? Periodontol. 2000 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Barnes, J.B.; Harrel, S.K.; Rivera-Hidalgo, F. Blood Contamination of the Aerosols Produced by In Vivo Use of Ultrasonic Sealers. J. Periodontol. 1998, 69, 434–438. [Google Scholar] [CrossRef]
- Johnson, I.G.; Jones, R.J.; Gallagher, J.E.; Wade, W.G.; Al-Yaseen, W.; Robertson, M.; McGregor, S.; KC, S.; Innes, N.; Harris, R. Dental Periodontal Procedures: A Systematic Review of Contamination (Splatter, Droplets and Aerosol) in Relation to COVID-19. BDJ Open 2021, 7, 15. [Google Scholar] [CrossRef]
- Gallagher, J.E.; KC, S.; Johnson, I.G.; Al-Yaseen, W.; Jones, R.; McGregor, S.; Robertson, M.; Harris, R.; Innes, N.; Wade, W.G. A Systematic Review of Contamination (Aerosol, Splatter and Droplet Generation) Associated with Oral Surgery and Its Relevance to COVID-19. BDJ Open 2020, 6, 25. [Google Scholar] [CrossRef]
- Ali, K.; Raja, M. COVID-19: Dental Aerosol Contamination in Open Plan Dental Clinics and Future Implications. Evid. Based Dent. 2021, 22, 54–55. [Google Scholar] [CrossRef]
- Ge, Z.; Yang, L.; Xia, J.; Fu, X.; Zhang, Y. Possible Aerosol Transmission of COVID-19 and Special Precautions in Dentistry. J. Zhejiang Univ.-SCI. B 2020, 21, 361–368. [Google Scholar] [CrossRef]
- Holliday, R.; Allison, J.R.; Currie, C.C.; Edwards, D.C.; Bowes, C.; Pickering, K.; Reay, S.; Durham, J.; Lumb, J.; Rostami, N.; et al. Evaluating Contaminated Dental Aerosol and Splatter in an Open Plan Clinic Environment: Implications for the COVID-19 Pandemic. J. Dent. 2021, 105, 103565. [Google Scholar] [CrossRef]
- Dar-Odeh, N.; Babkair, H.; Abu-Hammad, S.; Borzangy, S.; Abu-Hammad, A.; Abu-Hammad, O. COVID-19: Present and Future Challenges for Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3151. [Google Scholar] [CrossRef] [PubMed]
- Clementini, M.; Raspini, M.; Barbato, L.; Bernardelli, F.; Braga, G.; di Gioia, C.; Littarru, C.; Oreglia, F.; Brambilla, E.; Iavicoli, I.; et al. Aerosol Transmission for SARS-CoV-2 in the Dental Practice. A Review by SIdP COVID-19 Task-force. Oral. Dis. 2022, 28, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Mahdi, S.S.; Ahmed, Z.; Allana, R.; Peretti, A.; Amenta, F.; Nadeem Bijle, M.; Sow, L.L.; Daood, U. Pivoting Dental Practice Management during the COVID-19 Pandemic—A Systematic Review. Medicina 2020, 56, 644. [Google Scholar] [CrossRef]
- D’Ambrosio, F.; Pisano, M.; Amato, A.; Iandolo, A.; Caggiano, M.; Martina, S. Periodontal and Peri-Implant Health Status in Traditional vs. Heat-Not-Burn Tobacco and Electronic Cigarettes Smokers: A Systematic Review. Dent. J. 2022, 10, 103. [Google Scholar] [CrossRef]
- Billings, M.; Holtfreter, B.; Papapanou, P.N.; Mitnik, G.L.; Kocher, T.; Dye, B.A. Age-Dependent Distribution of Periodontitis in Two Countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J. Periodontol. 2018, 89, S140–S158. [Google Scholar] [CrossRef]
- Mummolo, S.; Nota, A.; Albani, F.; Marchetti, E.; Gatto, R.; Marzo, G.; Quinzi, V.; Tecco, S. Salivary Levels of Streptococcus Mutans and Lactobacilli and Other Salivary Indices in Patients Wearing Clear Aligners versus Fixed Orthodontic Appliances: An Observational Study. PLoS ONE 2020, 15, e0228798. [Google Scholar] [CrossRef]
- Di Spirito, F.; Iandolo, A.; Amato, A.; Caggiano, M.; Raimondo, A.; Lembo, S.; Martina, S. Prevalence, Features and Degree of Association of Oral Lesions in COVID-19: A Systematic Review of Systematic Reviews. Int. J. Environ. Res. Public Health 2022, 19, 7486. [Google Scholar] [CrossRef]
- Caggiano, M.; Gasparro, R.; D’Ambrosio, F.; Pisano, M.; di Palo, M.P.; Contaldo, M. Smoking Cessation on Periodontal and Peri-Implant Health Status: A Systematic Review. Dent. J. 2022, 10, 162. [Google Scholar] [CrossRef]
- Iandolo, A.; Amato, A.; Martina, S.; Latif, D.A.; Pantaleo, G. Management of Severe Curvatures in Root Canal Treatment with the New Generation of Rotating Files Using a Safe and Predictable Protocol. Open Dent. J. 2020, 14, 421–425. [Google Scholar] [CrossRef]
- Di Spirito, F.; Argentino, S.; Martuscelli, R.; Sbordone, L. MRONJ Incidence after Multiple Teeth Extractions in Patients Taking Oral Bis-Phosphonates without “Drug Holiday”: A Retrospective Chart Review. Oral Implant. 2019, 12, 105–110. [Google Scholar]
- Iandolo, A.; Abdellatif, D.; Amato, M.; Pantaleo, G.; Blasi, A.; Franco, V.; Neelakantan, P. Dentinal Tubule Penetration and Root Canal Cleanliness Following Ultrasonic Activation of Intracanal-heated Sodium Hypochlorite. Aust. Endod. J. 2020, 46, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Boccia, G.; Di Spirito, F.; D’Ambrosio, F.; di Palo, M.P.; Giordano, F.; Amato, M. Local and Systemic Antibiotics in Peri-Implantitis Management: An Umbrella Review. Antibiotics 2023, 12, 114. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Toti, P.; Brevi, B.; Martuscelli, R.; Sbordone, L.; Sbordone, C. Computed Tomography Evaluation of Jaw Atrophies Before and After Surgical Bone Augmentation. Int. J. Clin. Dent. 2019, 12, 259–270. [Google Scholar]
- Vergara-Buenaventura, A.; Castro-Ruiz, C. Use of Mouthwashes against COVID-19 in Dentistry. Br. J. Oral Maxillofac. Surg. 2020, 58, 924–927. [Google Scholar] [CrossRef]
- Fine, D.H.; Furgang, D.; Korik, I.; Olshan, A.; Barnett, M.L.; Vincent, J.W. Reduction of Viable Bacteria in Dental Aerosols by Preprocedural Rinsing with an Antiseptic Mouthrinse. Am. J. Dent. 1993, 6, 219–221. [Google Scholar] [PubMed]
- di Spirito, F. Oral-Systemic Health and Disorders: Latest Prospects on Oral Antisepsis. Appl. Sci. 2022, 12, 8185. [Google Scholar] [CrossRef]
- Graetz, C.; Hülsbeck, V.; Düffert, P.; Schorr, S.; Straßburger, M.; Geiken, A.; Dörfer, C.E.; Cyris, M. Influence of Flow Rate and Different Size of Suction Cannulas on Splatter Contamination in Dentistry: Results of an Exploratory Study with a High-Volume Evacuation System. Clin. Oral. Investig. 2022, 26, 5687–5696. [Google Scholar] [CrossRef]
- Koch, M.; Graetz, C. Spray Mist Reduction by Means of a High-Volume Evacuation System—Results of an Experimental Study. PLoS ONE 2021, 16, e0257137. [Google Scholar] [CrossRef]
- Bentley, C.D.; Burkhart, N.W.; Crawford, J.J. Evaluating Spatter And Aerosol Contamination During Dental Procedures. J. Am. Dent. Assoc. 1994, 125, 579–584. [Google Scholar] [CrossRef]
- Macher, J.M. Positive-Hole Correction of Multiple-Jet Impactors for Collecting Viable Microorganisms. Am. Ind. Hyg. Assoc. J. 1989, 50, 561–568. [Google Scholar] [CrossRef]
- Ali, K.; Raja, M. Coronavirus Disease 2019 (COVID-19): Challenges and Management of Aerosol-Generating Procedures in Dentistry. Evid. Based Dent. 2020, 21, 44–45. [Google Scholar] [CrossRef]
- Jackson, T.; Deibert, D.; Wyatt, G.; Durand-Moreau, Q.; Adisesh, A.; Khunti, K.; Khunti, S.; Smith, S.; Chan, X.H.S.; Ross, L.; et al. Classification of Aerosol-Generating Procedures: A Rapid Systematic Review. BMJ Open Respir. Res. 2020, 7, e000730. [Google Scholar] [CrossRef] [PubMed]
- Prati, C.; Pelliccioni, G.A.; Sambri, V.; Chersoni, S.; Gandolfi, M.G. COVID-19: Its Impact on Dental Schools in Italy, Clinical Problems in Endodontic Therapy and General Considerations. Int. Endod. J. 2020, 53, 723–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amato, A.; Ciacci, C.; Martina, S.; Caggiano, M.; Amato, M. COVID-19: The Dentists’ Perceived Impact on the Dental Practice. Eur. J. Dent. 2021, 15, 469–474. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Jouhar, R. Dissemination of Aerosol and Splatter in Clinical Environment during Cavity Preparation: An In Vitro Study. Int. J. Environ. Res. Public Health 2021, 18, 3773. [Google Scholar] [CrossRef] [PubMed]
- Harrel, S.K. Clinical Use of an Aerosol-Reduction Device with an Ultrasonic Scaler. Compend. Contin. Educ. Dent. 1996, 17, 1185–1193; quiz 1194. [Google Scholar] [PubMed]
- Llandro, H.; Allison, J.R.; Currie, C.C.; Edwards, D.C.; Bowes, C.; Durham, J.; Jakubovics, N.; Rostami, N.; Holliday, R. Evaluating Splatter and Settled Aerosol during Orthodontic Debonding: Implications for the COVID-19 Pandemic. Br. Dent. J. 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Di Spirito, F.; Iacono, V.J.; Alfredo, I.; Alessandra, A.; Sbordone, L.; Lanza, A. Evidence-Based Recommendations on Periodontal Practice and the Management of Periodontal Patients During and After the COVID-19 Era: Challenging Infectious Diseases Spread by Airborne Transmission. Open Dent J 2021, 15, 325–336. [Google Scholar] [CrossRef]
- Li, R.W.K.; Leung, K.W.C.; Sun, F.C.S.; Samaranayake, L.P. Severe Acute Respiratory Syndrome (SARS) and the GDP. Part II: Implications for GDPs. Br. Dent. J. 2004, 197, 130–134. [Google Scholar] [CrossRef]
- Indicazioni Operative per L’attività Odontoiatrica Durante La Pandemia COVID-19—REVISIONE 2022. Available online: https://cdn.andi.it/wp-content/uploads/2022/07/19144542/All.-2_Indicaz-operative-attivita-odont.-Covid-19_rev_2022.pdf (accessed on 7 November 2020).
- Available online: https://Apps.Who.Int/Iris/Rest/Bitstreams/1289841/Retrieve (accessed on 22 June 2021).
- Ezzat, R.T.; Al-Gowaihi, R.S.; Saha, B.Y.; Maher, Y.A.; Jastaniah, S.S. Evaluation of Microbial Air Contamination in Dental Surgery Clinics. Int. J. Med. Res. Prof. 2018, 4, 73–78. [Google Scholar]
- Kumbargere Nagraj, S.; Eachempati, P.; Paisi, M.; Nasser, M.; Sivaramakrishnan, G.; Verbeek, J.H. Interventions to Reduce Contaminated Aerosols Produced during Dental Procedures for Preventing Infectious Diseases. Cochrane Database Syst. Rev. 2020, 10, CD013686. [Google Scholar] [CrossRef]
- Fine, D.H.; Yip, J.; Furgang, D.; Barnett, M.L.; Olshan, A.M.; Vincent, J. Reducing Bacteria in Dental Aerosols: Pre Procedural Use of an Antiseptic Mouthrinse. J. Am. Dent. Assoc. 1993, 124, 56–58. [Google Scholar] [CrossRef]
- Martina, S.; Amato, A.; Rongo, R.; Caggiano, M.; Amato, M. The Perception of COVID-19 among Italian Dentists: An Orthodontic Point of View. Int. J. Environ. Res. Public Health 2020, 17, 4384. [Google Scholar] [CrossRef]
- Feres, M.; Figueiredo, L.C.; Faveri, M.; Stewart, B.; de Vizio, W. The Effectiveness of a Preprocedural Mouthrinse Containing Cetylpyridinium Chloride in Reducing Bacteria in the Dental Office. J. Am. Dent. Assoc. 2010, 141, 415–422. [Google Scholar] [CrossRef]
- Indicazioni Operative per L’attivita’ Odontoiatrica Durante La Fase 2 Della Pandemia COVID-19. Available online: https://Www.Salute.Gov.It/Imgs/C_17_pubblicazioni_2917_allegato.Pdf (accessed on 7 November 2020).
- Grenier, D. Quantitative Analysis of Bacterial Aerosols in Two Different Dental Clinic Environments. Appl. Environ. Microbiol. 1995, 61, 3165–3168. [Google Scholar] [CrossRef] [PubMed]
- Bifulco, M.; Amato, M.; Gangemi, G.; Marasco, M.; Caggiano, M.; Amato, A.; Pisanti, S. Dental Care and Dentistry Practice in the Medieval Medical School of Salerno. Br. Dent. J. 2016, 221, 87–89. [Google Scholar] [CrossRef]
- Kumar, P.S.; Geisinger, M.L.; Avila-Ortiz, G. Methods to Mitigate Infection Spread from Aerosol-generating Dental Procedures. J. Periodontol. 2021, 92, 784–792. [Google Scholar] [CrossRef] [PubMed]
- Pankhurst, C. Summary of: A Pilot Study of Bioaerosol Reduction Using an Air Cleaning System during Dental Procedures. Br. Dent. J. 2010, 209, 408–409. [Google Scholar] [CrossRef] [PubMed]
- Aurangjeb, A.M.; Zaman, T.; Badruddoza, M. Practice of Dental Surgeons about Dental Splatter and Aerosol. City Dent. Coll. J. 2013, 10, 10–16. [Google Scholar] [CrossRef]
- Timmerman, M.F.; Menso, L.; Steinfort, J.; van Winkelhoff, A.J.; van der Weijden, G.A. Atmospheric Contamination during Ultrasonic Scaling. J. Clin. Periodontol. 2004, 31, 458–462. [Google Scholar] [CrossRef]
- Meurman, J.H. Do Dental Aerosols Matter? J. Dent. Res. 2021, 100, 1423–1424. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Samaranayake, L. Emerging and Changing Viral Diseases in the New Millennium. Oral Dis. 2016, 22, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Samaranayake, L.; Anil, S. The Monkeypox Outbreak and Implications for Dental Practice. Int. Dent. J. 2022, 72, 589–596. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Species | T 0 | T 1 | T 2 | p-Value |
|---|---|---|---|---|
| Staphylococcus spp. (S. capitis, S. haemolyticus, S. hominis) | 50.0 CFU/m3 [45.0, 58.0] | 124.0 CFU/m3 [111.0, 140.0] | 70.0 CFU/m3 [65.5, 78.0] | <0.001 |
| Viridans streptococci (S. mitis, S. salivarius, S. mutans) | 0 CFU/m3 [0, 0] | 256.0 CFU/m3 [244.0, 288.0] | 6.0 CFU/m3 [5.0, 8.0] | <0.001 |
| Others (Bacillus spp. and fungi) | 7.0 CFU/m3 [6.0, 8.0] | 15.0 CFU/m3 [11.0, 17.0] | 18.0 CFU/m3 [15.5, 19.0] | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boccia, G.; Di Spirito, F.; D’Ambrosio, F.; De Caro, F.; Pecora, D.; Giorgio, R.; Fortino, L.; Longanella, W.; Franci, G.; Santella, B.; et al. Microbial Air Contamination in a Dental Setting Environment and Ultrasonic Scaling in Periodontally Healthy Subjects: An Observational Study. Int. J. Environ. Res. Public Health 2023, 20, 2710. https://doi.org/10.3390/ijerph20032710
Boccia G, Di Spirito F, D’Ambrosio F, De Caro F, Pecora D, Giorgio R, Fortino L, Longanella W, Franci G, Santella B, et al. Microbial Air Contamination in a Dental Setting Environment and Ultrasonic Scaling in Periodontally Healthy Subjects: An Observational Study. International Journal of Environmental Research and Public Health. 2023; 20(3):2710. https://doi.org/10.3390/ijerph20032710
Chicago/Turabian StyleBoccia, Giovanni, Federica Di Spirito, Francesco D’Ambrosio, Francesco De Caro, Domenico Pecora, Riccardo Giorgio, Luigi Fortino, Walter Longanella, Gianluigi Franci, Biagio Santella, and et al. 2023. "Microbial Air Contamination in a Dental Setting Environment and Ultrasonic Scaling in Periodontally Healthy Subjects: An Observational Study" International Journal of Environmental Research and Public Health 20, no. 3: 2710. https://doi.org/10.3390/ijerph20032710