
Coping as a Mediator and Moderator between Psychological Distress and Disordered Eating Behaviors and Weight Changes during the COVID-19 Pandemic
 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Sociodemographic Questionnaire
2.2.2. Depression Anxiety Stress Scale
2.2.3. Eating Disorder Examination Questionnaire
2.2.4. Brief COPE
2.3. Procedure
3. Data Analysis
4. Results
4.1. Relationships between Psychological Distress, Disordered Eating, Coping Strategies and Weight Change
4.2. The Mediating Role of Coping Strategies in Weight Gain
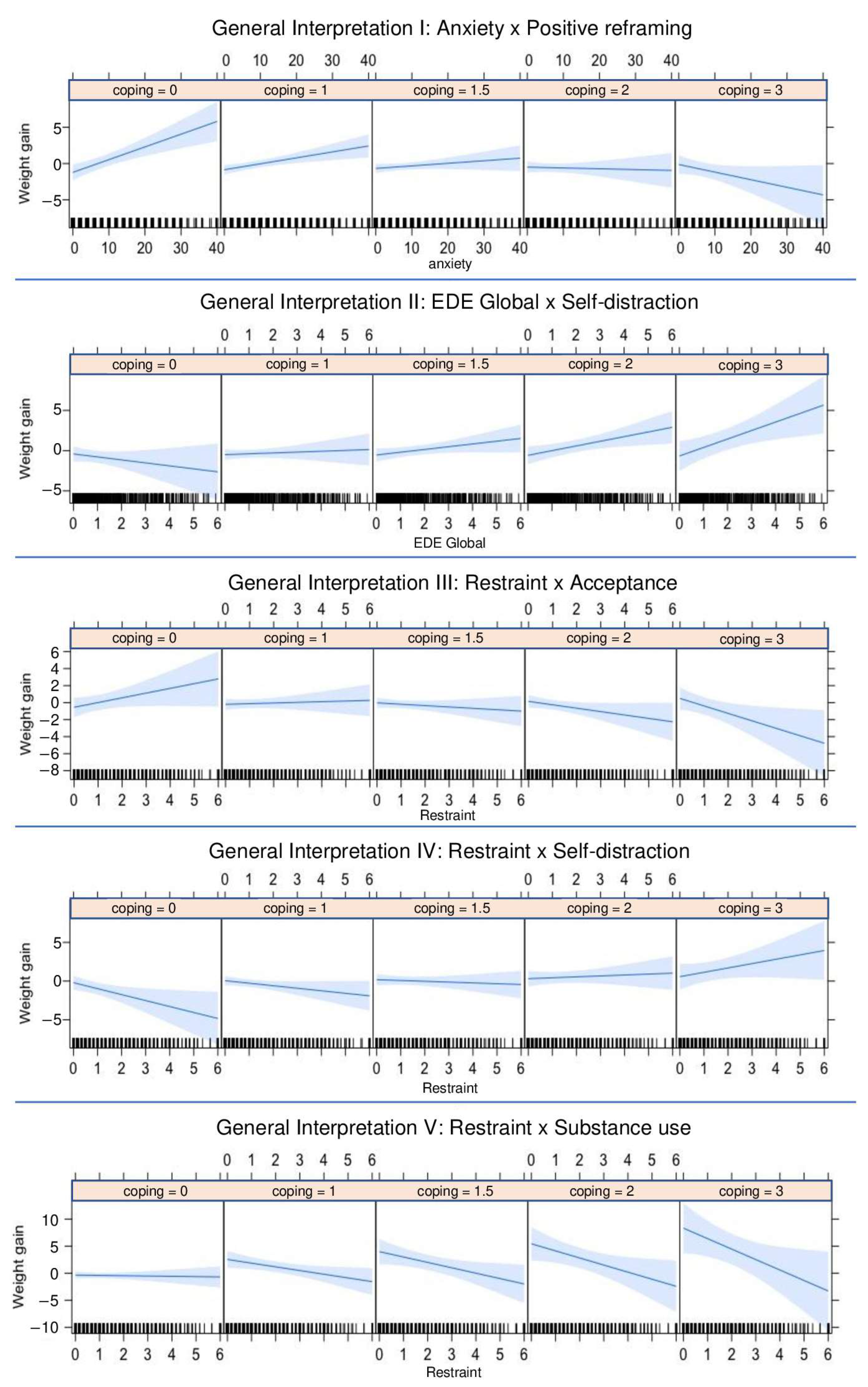
4.3. The Moderating Role of Coping Strategies in Weight Gain
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Xia, Q.; Xiong, Z.; Li, Z.; Xiang, W.; Yuan, Y.; Liu, Y.; Li, Z. The psychological distress and coping styles in the early stages of the 2019 coronavirus disease (COVID-19) epidemic in the general mainland Chinese population: A web-based survey. PLoS ONE 2020, 15, e0233410. [Google Scholar] [CrossRef]
- Ho, C.S.; Chee, C.Y.; Ho, R.C. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann. Acad. Med. Singap. 2020, 49, 1–3. [Google Scholar]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simone, M.; Emery, R.L.; Hazzard, V.M.; Eisenberg, M.E.; Larson, N.; Neumark-Sztainer, D. Disordered eating in a population-based sample of young adults during the COVID-19 outbreak. Int. J. Eat. Disord. 2021, 54, 1189–1201. [Google Scholar] [CrossRef]
- Marzo, R.R.; Ismail, Z.; Htay, M.N.; Bahari, R.; Ismail, R.; Villanueva, E.Q., III; Singh, A.; Lotfizadeh, M.; Respati, T.; Irasanti, S.N.; et al. Psychological distress during pandemic COVID-19 among adult general population: Result across 13 countries. Clin. Epidemiol. Glob. Health 2021, 1, 100708. [Google Scholar] [CrossRef]
- Prowse, R.; Sherratt, F.; Abizaid, A.; Gabrys, R.L.; Hellemans, K.G.; Patterson, Z.R.; McQuaid, R.J. Coping with the COVID-19 pandemic: Examining gender differences in stress and mental health among university students. Front. Psychiatry 2021, 12, 650759. [Google Scholar] [CrossRef]
- Machado, B.C.; Pinto, E.; Silva, M.; Veiga, E.; Sá, C.; Kuhz, S.; Silva, P.O.; Pimenta, A.; Gomes, A.; Almeida, A.; et al. Impact of the COVID-19 pandemic on the mental and physical health and overall wellbeing of university students in Portugal. PLoS ONE 2022, 10, 312. [Google Scholar]
- Liu, S.; Yang, L.; Zhang, C.; Xiang, Y.-T.; Liu, Z.; Hu, S.; Zhang, B. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e17–e18. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. QJM Int. J. Med. 2020, 113, 531–537. [Google Scholar] [CrossRef]
- Smith, K.R.; Jansen, E.; Thapaliy, G.; Aghababian, A.H.; Chen, L.; Sadler, J.R.; Carnell, S. The influence of COVID-19-related stress on food motivation. Appetite 2021, 1, 105233. [Google Scholar] [CrossRef]
- Gonçalves, S.; Félix, S.; Martins, F.; Lapenta, O.; Machado, B.C.; Conceição, E.M. Food addiction problems in college students: The relationship between weight-related variables, eating habits, and food choices. Int. J. Environ. Res. Public Health 2022, 19, 14588. [Google Scholar] [CrossRef] [PubMed]
- Coulthard, H.; Sharps, M.; Cunliffe, L.; van den Tol, A. Eating in the lockdown during the COVID-19 pandemic; self-reported changes in eating behaviour, and associations with BMI, eating style, coping and health anxiety. Appetite 2021, 1, 105082. [Google Scholar] [CrossRef]
- Salazar-Fernández, C.; Palet, D.; Haeger, P.A.; Román Mella, F. The perceived impact of COVID-19 on comfort food consumption over time: The mediational role of emotional distress. Nutrients 2021, 13, 1910. [Google Scholar] [CrossRef]
- Ramalho, S.M.; Trovisqueira, A.; de Lourdes, M.; Gonçalves, S.; Ribeiro, I.; Vaz, A.R.; Machado, P.P.; Conceição, E. The impact of COVID-19 lockdown on disordered eating behaviors: The mediation role of psychological distress. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2022, 27, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Neumark-Sztainer, D.; Wall, M.; Guo, J.; Story, M.; Haines, J.; Eisenberg, M. Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: How do dieters fare 5 years later? J. Am. Diet. Assoc. 2006, 106, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Goldschmidt, A.B.; Wall, M.M.; Zhang, J.; Loth, K.A.; Neumark-Sztainer, D. Overeating and binge eating in emerging adulthood: 10-year stability and risk factors. Dev. Psychol. 2016, 52, 475. [Google Scholar] [CrossRef] [Green Version]
- Vuillier, L.; May, L.; Greville-Harris, M.; Surman, R.; Moseley, R.L. The impact of the COVID-19 pandemic on individuals with eating disorders: The role of emotion regulation and exploration of online treatment experiences. J. Eat. Disord. 2021, 9, 1–8. [Google Scholar] [CrossRef]
- Tavolacci, M.P.; Ladner, J.; Déchelotte, P. Sharp increase in eating disorders among university students since the COVID-19 pandemic. Nutrients 2021, 13, 3415. [Google Scholar] [CrossRef]
- Fluharty, M.; Bu, F.; Steptoe, A.; Fancourt, D. Coping strategies and mental health trajectories during the first 21 weeks of COVID-19 lockdown in the United Kingdom. Soc. Sci. Med. 2021, 279, 113958. [Google Scholar] [CrossRef]
- Elkayal, M.M.; Shahin, M.A.; Hussien, R.M. Psychological distress related to the emerging COVID-19 pandemic and coping strategies among general population in Egypt. J. Egypt. Public Health Assoc. 2022, 97, 1–2. [Google Scholar]
- Yan, L.; Gan, Y.; Ding, X.; Wu, J.; Duan, H. The relationship between perceived stress and emotional distress during the COVID-19 outbreak: Effects of boredom proneness and coping style. J. Anxiety Disord. 2021, 77, 102328. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, L.; Steinhoff, A.; Bechtiger, L.; Murray, A.L.; Nivette, A.; Hepp, U.; Ribeaud, D.; Eisner, M. Emotional distress in young adults during the COVID-19 pandemic: Evidence of risk and resilience from a longitudinal cohort study. Psychol. Med. 2020, 52, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.; Yi, Z.; Zhang, S.; Veldhuis, C.B. Predictors of psychological distress and resilience in the post-COVID-19 era. Int. J. Behav. Med. 2022, 29, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Galatzer-Levy, I.R.; Huang, S.H.; Bonanno, G.A. Trajectories of resilience and dysfunction following potential trauma: A review and statistical evaluation. Clin. Psychol. Rev. 2018, 63, 41–55. [Google Scholar] [CrossRef]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Ribeiro, J.L.; Honrado, A.A.; Leal, I.P. Contribuição para o estudo da adaptação portuguesa das escalas de ansiedade, depressão e stress (EADS) de 21 itens de Lovibond e Lovibond. Psicol. Saúde Doenças 2004, 5, 2229–2239. [Google Scholar]
- Lee, S.H.; Shin, H.S.; Park, H.Y.; Kim, J.L.; Lee, J.J.; Lee, H.; Won, S.D.; Han, W. Depression as a mediator of chronic fatigue and post-traumatic stress symptoms in Middle East respiratory syndrome survivors. Psychiatry Investig. 2019, 16, 59. [Google Scholar] [CrossRef] [Green Version]
- Apóstolo, J.L.; Mendes, A.C.; Azeredo, Z.A. Adaptación para la lengua portuguesa de la depression, anxiety and stress scale (DASS). Rev. Lat. Am. De Enferm. 2006, 14, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [CrossRef]
- Machado, P.P.; Martins, C.; Vaz, A.R.; Conceição, E.; Bastos, A.P.; Gonçalves, S. Eating disorder examination questionnaire: Psychometric properties and norms for the Portuguese population. Eur. Eat. Disord. Rev. 2014, 22, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Personal. Soc. Psychol. 1989, 56, 267. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, J.L.; Rodrigues, A.P. Questões acerca do coping: A propósito do estudo de adaptação do Brief Cope. Psicol. Saúde E Doenças 2004, 1, 3–15. [Google Scholar]
- Meyer, B. Coping with severe mental illness: Relations of the Brief COPE with symptoms, functioning, and well-being. J. Psychopathol. Behav. Assess. 2001, 23, 265–277. [Google Scholar] [CrossRef]
- Brooks, M.E.; Kristensen, K.; Van Benthem, K.J.; Magnusson, A.; Berg, C.W.; Nielsen, A.; Skaug, H.J.; Machler, M.; Bolker, B.M. glmmTMB balances speed and flexibility among packages for zero-inflated generalized linear mixed modeling. R J. 2017, 9, 378–400. [Google Scholar] [CrossRef]
- Long, J.A. interactions: Comprehensive, user-friendly toolkit for probing interactions. R Package Version 2019, 1, 33. [Google Scholar]
- Rosseel, Y. lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Hawken, T.; Turner-Cobb, J.; Barnett, J. Coping and adjustment in caregivers: A systematic review. Health Psychol. Open 2018, 5, 2055102918810659. [Google Scholar] [CrossRef]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: Berlin/Heidelberg, Germany, 1984. [Google Scholar]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef]
- Giuntella, O.; Hyde, K.; Saccardo, S.; Sadoff, S. Lifestyle and mental health disruptions during COVID-19. Proc. Natl. Acad. Sci. USA 2021, 118, e2016632118. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Mean | SD | Range [Min, Max] |
|---|---|---|---|
| Weight change | 0.03 | 1.73 | [−6.66, 7.26] |
| Psychological distress | |||
| Depression | 0.77 | 0.78 | [0, 3] |
| Anxiety | 0.62 | 0.69 | [0, 3] |
| Stress | 1.1 | 0.86 | [0, 3] |
| Disordered eating | |||
| EDE global | 1.28 | 1.40 | [0, 6] |
| Restraint | 1.09 | 1.38 | [0, 6] |
| Weight concern | 1.71 | 1.85 | [0, 6] |
| Shape concern | 1.63 | 1.71 | [0, 6] |
| Eating concern | 0.69 | 1.22 | [0, 6] |
| Coping strategies | |||
| Active coping | 1.17 | 0.79 | [0, 3] |
| Planning | 1.41 | 0.86 | [0, 3] |
| Use of instrumental support | 0.93 | 0.87 | [0, 3] |
| Use of emotional support | 1.05 | 0.90 | [0, 3] |
| Religion | 0.69 | 0.92 | [0, 3] |
| Positive reframing | 1.32 | 0.89 | [0, 3] |
| Self-blame | 1.07 | 0.87 | [0, 3] |
| Acceptance | 1.39 | 0.84 | [0, 3] |
| Venting | 1.03 | 0.84 | [0, 3] |
| Denial | 0.38 | 0.58 | [0, 3] |
| Self-distraction | 0.99 | 0.82 | [0, 3] |
| Behavioral disengagement | 0.44 | 0.64 | [0, 3] |
| Substance use | 0.14 | 0.48 | [0, 3] |
| Humor | 1.09 | 0.87 | [0, 3] |
| Variable | Estimate | SE | p-Value | R2 | F-Statistic |
|---|---|---|---|---|---|
| Psychological distress | |||||
| Depression | 0.31 | 0.08 | <0.001 *** | 0.020 | 14.99 |
| Anxiety | 0.20 | 0.09 | 0.033 * | 0.006 | 4.54 |
| Stress | 0.17 | 0.07 | 0.022 * | 0.007 | 5.26 |
| Disordered eating | |||||
| EDE global | 0.15 | 0.05 | 0.002 ** | 0.014 | 9.99 |
| Restraint | −0.01 | 0.05 | 0.925 | 0.000 | 0.01 |
| Weight concern | 0.12 | 0.03 | <0.001 *** | 0.017 | 12.03 |
| Shape concern | 0.15 | 0.04 | <0.001 *** | 0.020 | 14.93 |
| Eating concern | 0.22 | 0.05 | <0.001 *** | 0.024 | 17.90 |
| Coping strategies | |||||
| Active coping | −0.23 | 0.09 | 0.009 ** | 0.011 | 6.81 |
| Planning | −0.13 | 0.08 | 0.120 | 0.004 | 2.41 |
| Use of instrumental support | −0.24 | 0.08 | 0.003 ** | 0.015 | 9.15 |
| Use of emotional support | −0.05 | 0.08 | 0.522 | 0.001 | 0.41 |
| Religion | −0.09 | 0.08 | 0.245 | 0.002 | 1.35 |
| Positive reframing | −0.21 | 0.08 | 0.006 ** | 0.012 | 7.61 |
| Self-blame | 0.21 | 0.08 | 0.008 ** | 0.011 | 6.92 |
| Acceptance | −0.13 | 0.08 | 0.118 | 0.004 | 2.43 |
| Venting | −0.07 | 0.08 | 0.375 | 0.001 | 0.79 |
| Denial | 0.27 | 0.12 | 0.021 * | 0.008 | 5.31 |
| Self-distraction | 0.17 | 0.08 | 0.046 * | 0.006 | 3.95 |
| Behavioral disengagement | 0.55 | 0.11 | <0.001 *** | 0.041 | 26.86 |
| Substance use | 0.40 | 0.14 | 0.005 ** | 0.012 | 7.73 |
| Humor | −0.03 | 0.08 | 0.712 | 0.000 | 0.14 |
| Relationship | Mediator Effect (95% Bootstrap CI) | Direct Effect | Total Effect |
|---|---|---|---|
| Depression → Weight change | 0.100 (0.033, 0.158) | 0.061 | 0.161 * |
| Anxiety → Weight change | 0.113 (0.054, 0.178) | −0.029 | 0.085 * |
| Stress → Weight change | 0.104 (0.052, 0.164) | −0.002 | 0.101 * |
| EDE global → Weight change | 0.101 (0.036, 0.160) | 0.014 | 0.115 * |
| Restraint → Weight change | 0.065 (0.032, 0.104) | −0.089 * | −0.025 |
| Weight concern → Weight change | 0.099 (0.037, 0.162) | 0.025 | 0.124 * |
| Shape concern → Weight change | 0.095 (0.034, 0.158) | 0.047 | 0.142 * |
| Eating concern → Weight change | 0.085 (0.065, 0.295) | 0.093 * | 0.178 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machado, B.C.; Moreira, C.S.; Correia, M.; Veiga, E.; Gonçalves, S. Coping as a Mediator and Moderator between Psychological Distress and Disordered Eating Behaviors and Weight Changes during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2023, 20, 2504. https://doi.org/10.3390/ijerph20032504
Machado BC, Moreira CS, Correia M, Veiga E, Gonçalves S. Coping as a Mediator and Moderator between Psychological Distress and Disordered Eating Behaviors and Weight Changes during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2023; 20(3):2504. https://doi.org/10.3390/ijerph20032504
Chicago/Turabian StyleMachado, Bárbara Cesar, Célia S. Moreira, Marta Correia, Elisa Veiga, and Sónia Gonçalves. 2023. "Coping as a Mediator and Moderator between Psychological Distress and Disordered Eating Behaviors and Weight Changes during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 20, no. 3: 2504. https://doi.org/10.3390/ijerph20032504