

High-Speed Dental Instruments: An Investigation of Protein-Contaminated Dental Handpieces with the Bicinchoninic Acid Assay in Dental Offices in Styria, Austria

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
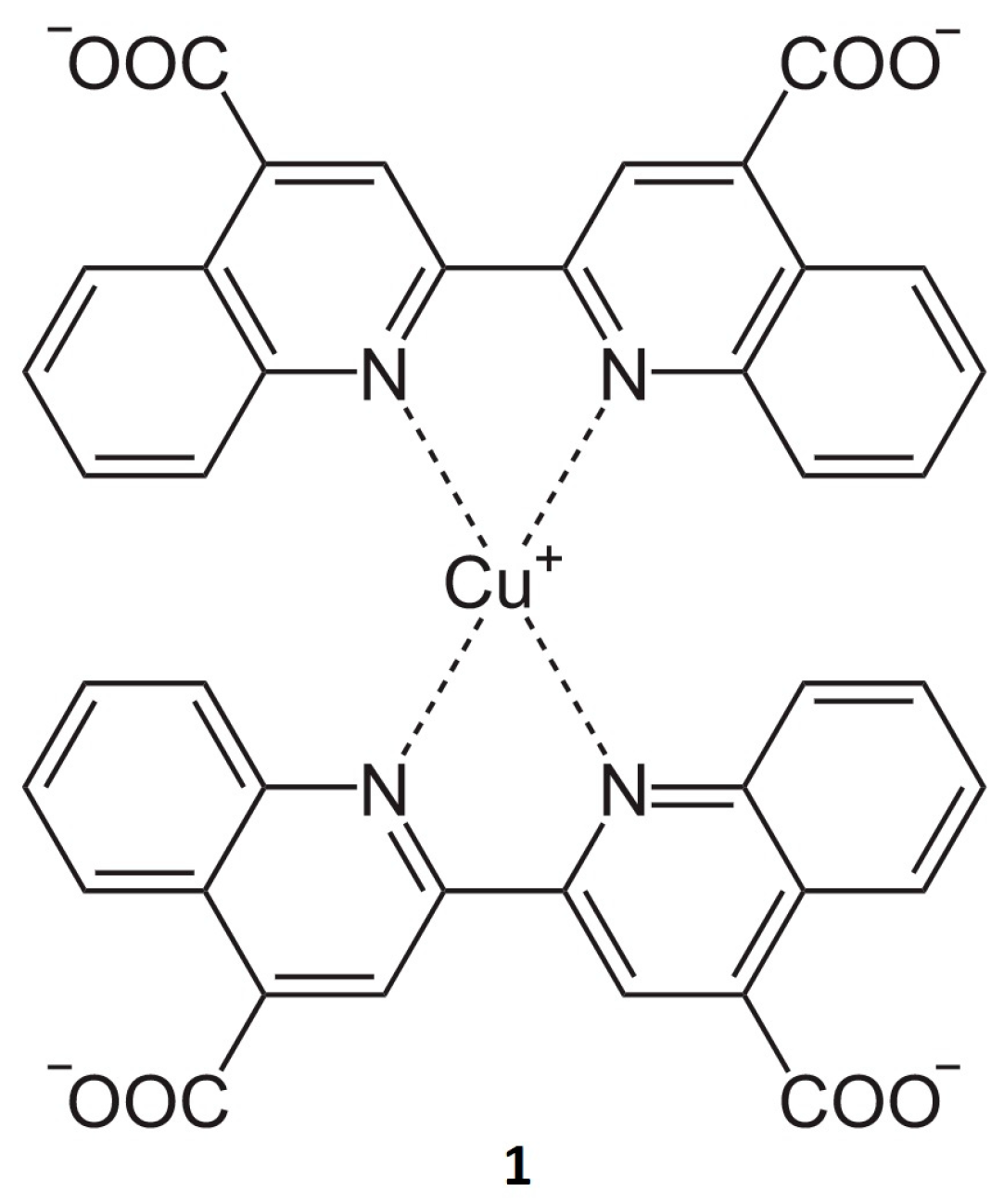
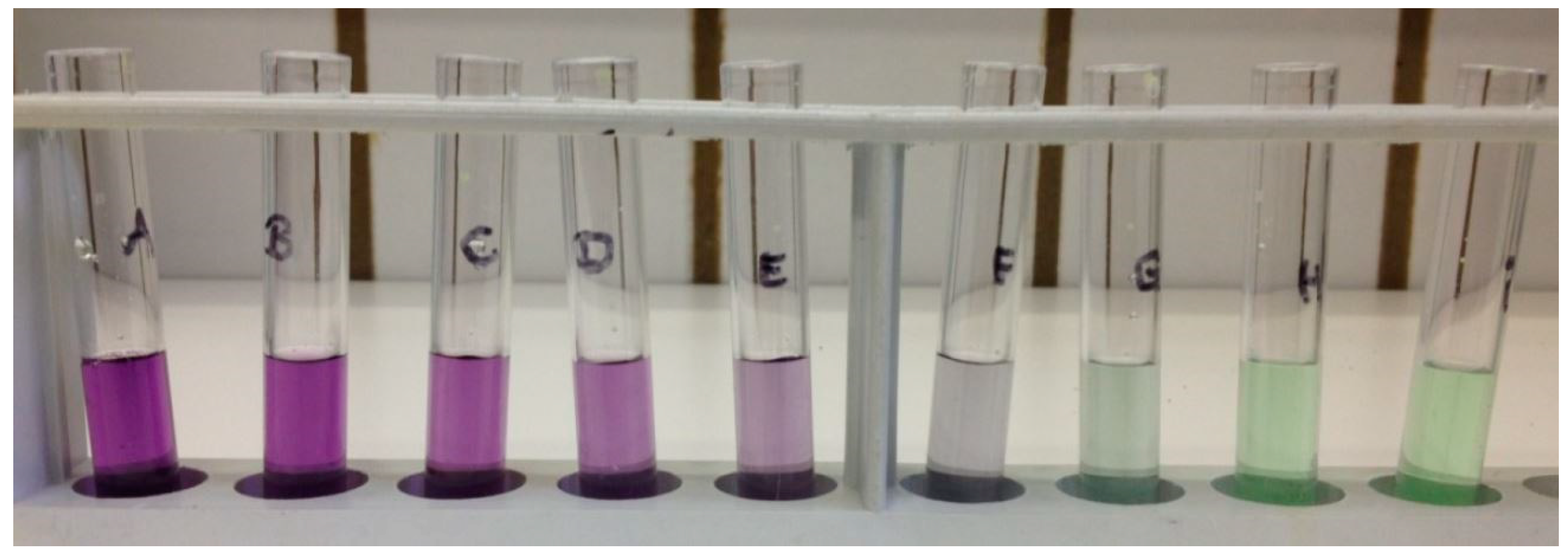
2.1. General Procedure for BCA Assay
2.2. Water Sample Collection
2.3. Data Analysis
3. Results
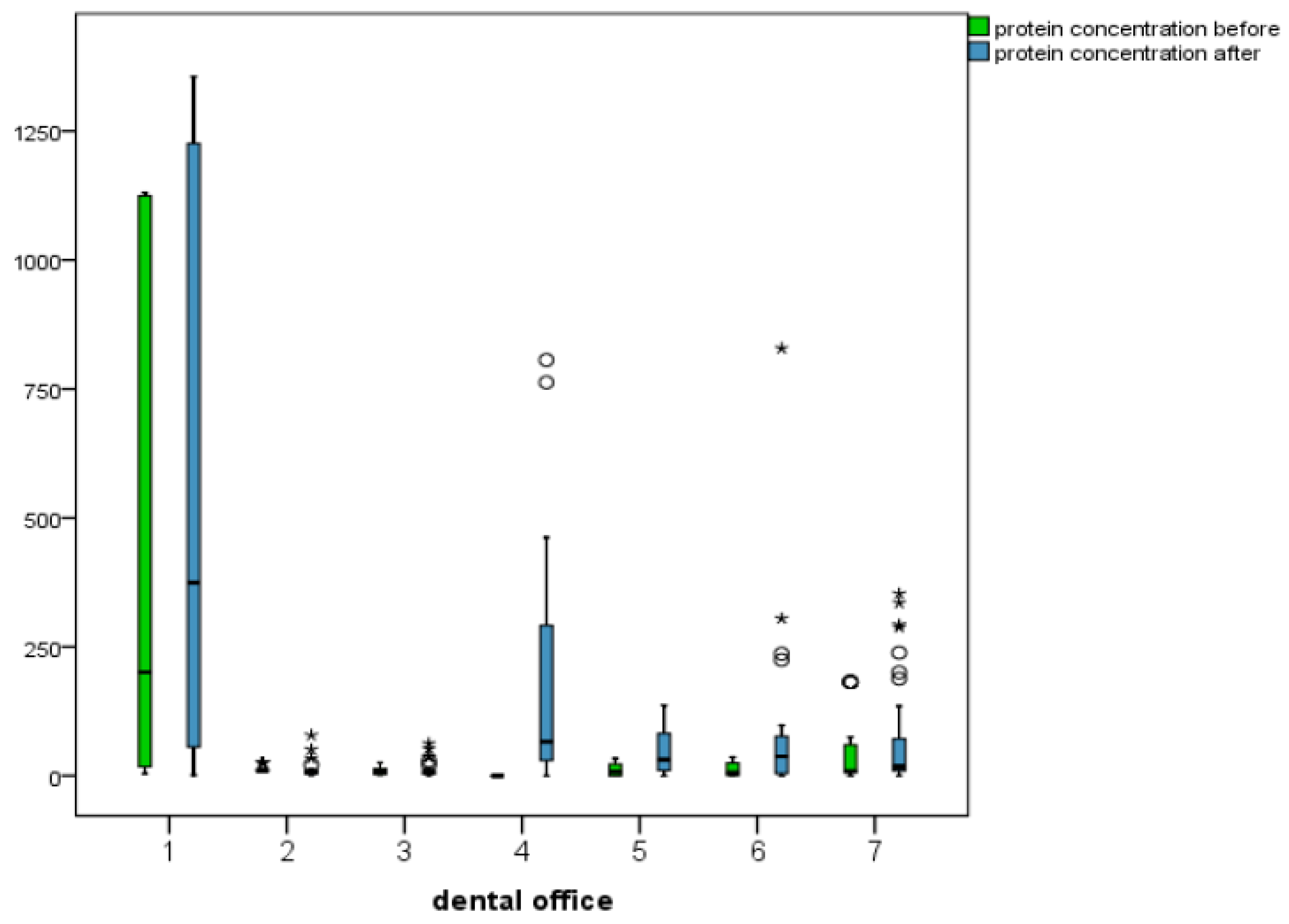
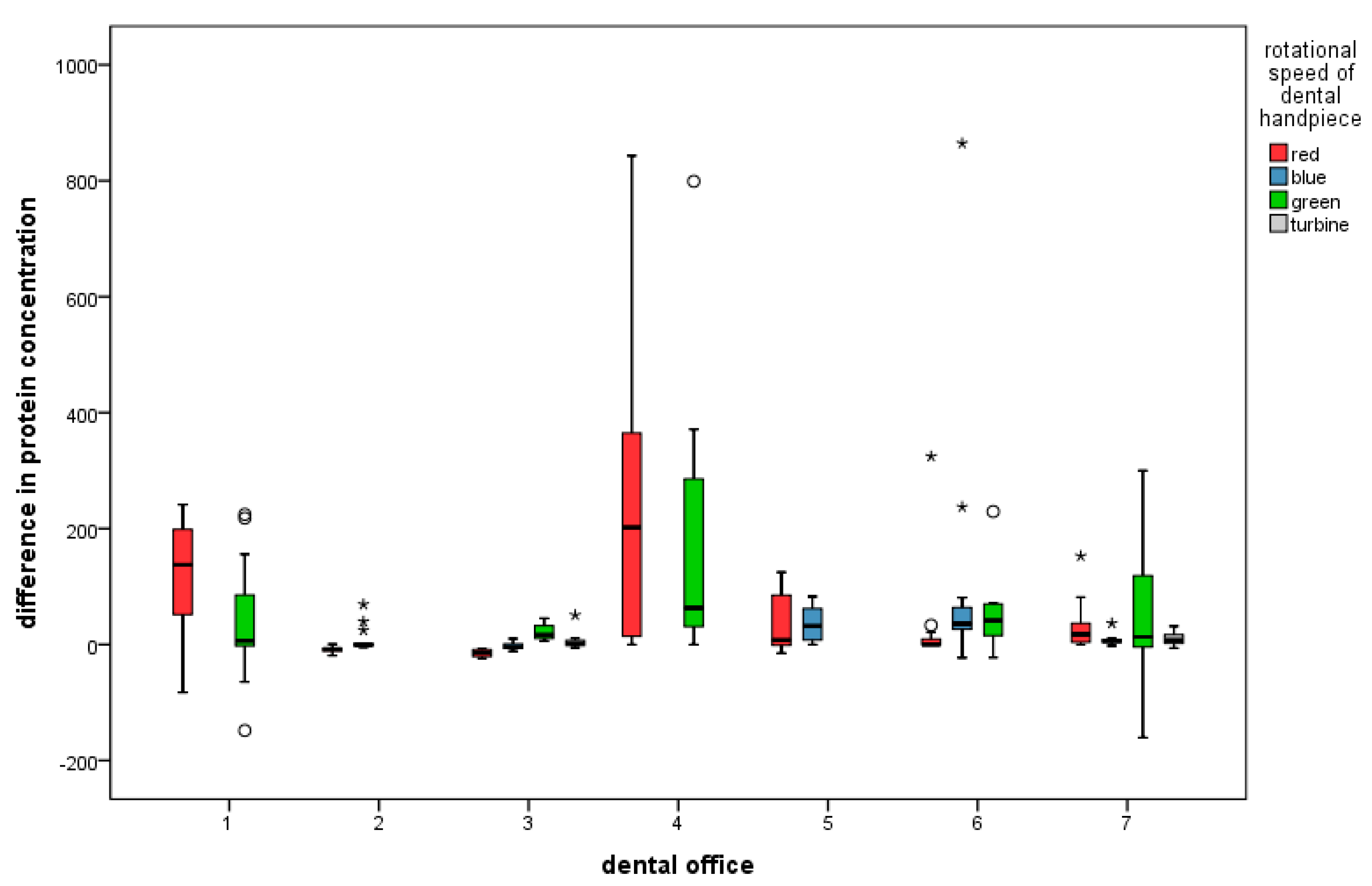
3.1. Descriptive Statistics for Protein Concentrations before and after Treatment, as Well as Difference (Increase or Decrease)
3.2. Final Statistics—Combined Influence of Parameters on Protein Concentration after Treatment and Difference (Increase or Decrease)
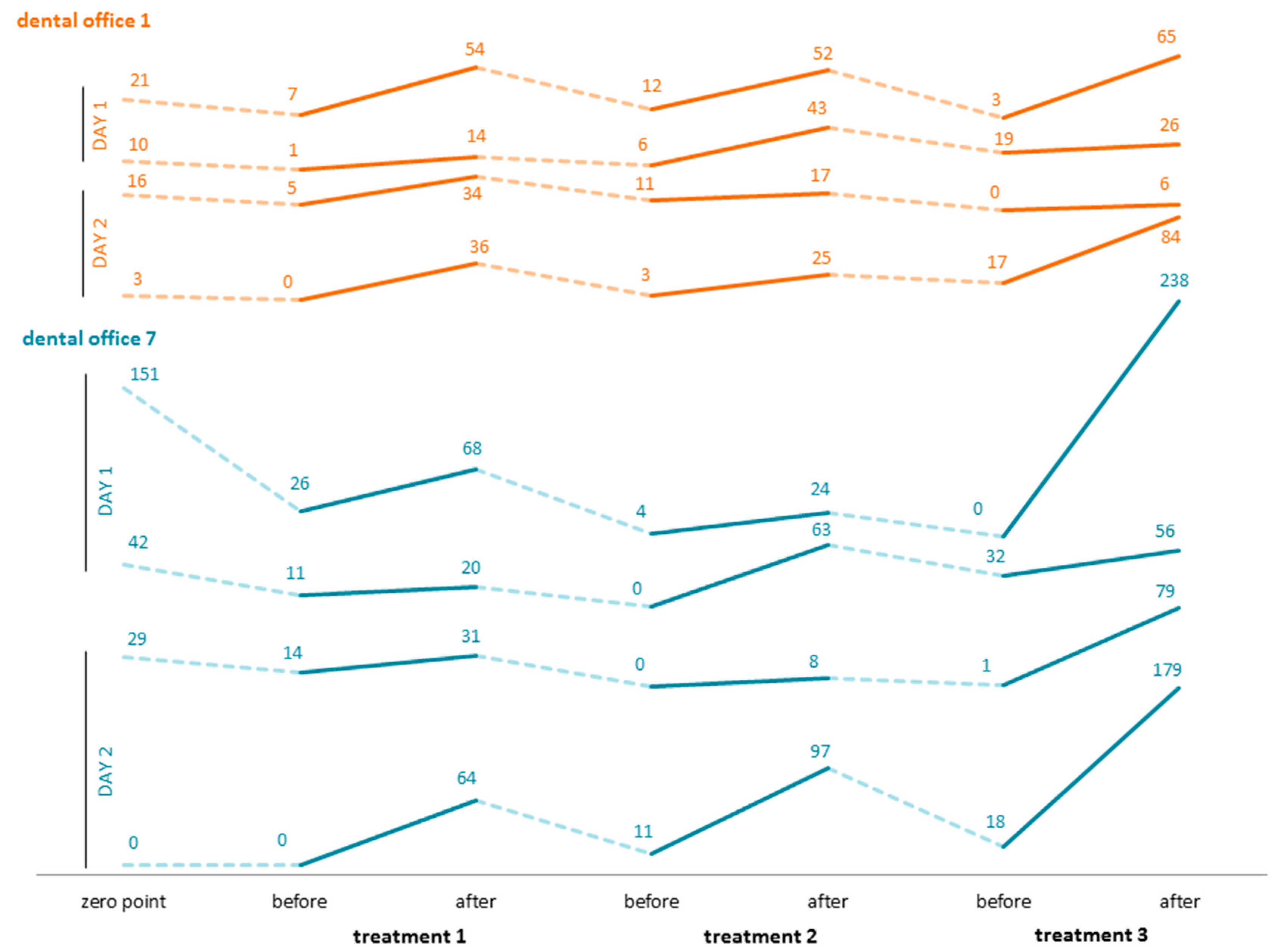
3.3. Three Consecutive Treatments per Day over the Course of Two Days in Two Dental Offices
4. Discussion
4.1. Outcome
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cafruny, W.A.; Brunick, A.; Nelson, D.M.; Nelson, R.F. Effectiveness of ultrasonic cleaning of dental instruments. Am. J. Dent. 1995, 8, 152–156. [Google Scholar] [PubMed]
- Rabenau, H.F.; Nentwig, G.H.; Doerr, H.W. Application of automated thermal disinfection instead of sterilisation procedures for treatment of rotating dental instruments: Efficacy against viruses? Zentralbl. Hyg. Umweltmed. 1997, 200, 197–215. [Google Scholar] [PubMed]
- Santiago, J.I.; Huntington, M.K.; Johnston, A.M.; Quinn, R.S.; Williams, J.F. Microbial contamination of dental unit waterlines: Short- and long-term effects of flushing. Gen. Dent. 1994, 42, 528–535. [Google Scholar] [PubMed]
- Gräf, W.; Kunz, B.; Loisl, B. Hygienic processing of dental transmission instruments (handpieces and instruments, turbines) in dental practice. Zentralbl. Hyg. Umweltmed. 1995, 198, 72–83. [Google Scholar]
- Simonetti D’Arca, A.S.; Petti, S.; Polimeni, A. A new device for the disinfection of handpieces and turbines. Minerva Stomatol. 1995, 44, 369–375. [Google Scholar]
- Noopan, S.; Unchui, P.; Techotinnakorn, S.; Ampornaramveth, R.S. Plasma Sterilization Effectively Reduces Bacterial Contamination in Dental Unit Waterlines. Int. J. Dent. 2019, 30, 5720204. [Google Scholar] [CrossRef] [Green Version]
- Alkhulaifi, M.M.; Alotaibi, D.H.; Alajlan, H.; Binshoail, T. Assessment of nosocomial bacterial contamination in dental unit waterlines: Impact of flushing. Saudi Dent. J. 2020, 32, 68–73. [Google Scholar] [CrossRef]
- Dang, Y.; Zhang, Q.; Wang, J.; Wang, Q.; Han, M.; Niu, Y.; Li, H.; Li, X. Assessment of microbiota diversity in dental unit waterline contamination. PeerJ 2022, 10, e12723. [Google Scholar] [CrossRef]
- Claesson, R.; Edwardsson, S.; Bäckman, N. Microbial contamination of dental unit water lines—A matter of following instructions. J. Hosp. Infect. 2021, 113, 187–188. [Google Scholar] [CrossRef]
- Omran, E.A.H.; Abbass, A.A.G.; Abaza, A.F.; Elzouki, E.M. Study of some risk factors for fungal contamination of dental unit waterlines in Alexandria, Egypt. J. Infect. Dev. Ctries. 2021, 15, 1197–1204. [Google Scholar] [CrossRef]
- Wu, M.; Shi, Z.; Yu, X.; Xu, Y.; Jin, X.; Zhang, L.; Fu, B. Disinfection methods of dental unit waterlines contamination: A systematic review. J. Med. Microbiol. 2022, 71, 001540. [Google Scholar] [CrossRef] [PubMed]
- Pagano, S.; Coniglio, M.; Valenti, C.; Federici, M.I.; Lombardo, G.; Cianetti, S.; Marinucci, L. Biological effects of Cannabidiol on normal human healthy cell populations: Systematic review of the literature. Biomed. Pharmacother. 2020, 132, 110728. [Google Scholar] [CrossRef]
- Benett, A.M.; Fulford, M.V.; Walker, D.J.; Bradshaw, D.J.; Martin, M.V.; Marsh, P.D. Occupational health—Micorbial aerosols in general dental practice. Br. Dent. J. 2000, 189, 664–667. [Google Scholar] [CrossRef]
- Miller, R.L. Characteristics of blood-containing aerosols generated by common powered dental equipment. Am. Ind. Hyg. Assoc. J. 1995, 56, 670–676. [Google Scholar] [CrossRef]
- Epstein, J.B.; Rea, G.; Sibau, L.; Sherlock, C.H.; Le, N.D. Assessing viral retention and elimination in rotary dental instruments. JADA 1995, 126, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.L.; Arens, M.; Appleton, S.S.; Nakashima, K.; Ryu, J.; Boe, R.K.; Patrick, J.B.; Watanabe, D.T.; Suzuki, M. Cross-contamination potential with dental equipment. Lancet 1992, 340, 1252–1254. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.L.; Boe, R.K. Cross-Infection Risks associated with current procedures for using high-speed dental handpieces. JCM 1992, 30, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Pelzner, R.B.; Kempler, D.; Stark, M.M.; Barkin, P.R.; Graham, D.A. Laser evaluation of handpiece contamination. J. Dent. Res. 1977, 56, 1629–1634. [Google Scholar] [CrossRef]
- Scheid, R.C.; Kim, C.K.; Bright, J.S.; Whitely, M.S.; Rosen, S. Reduction of microbes in handpieces by flushing before use. JADA 1982, 105, 658–660. [Google Scholar] [CrossRef]
- Mills, S.E.; Kuehne, J.C.; Bradley, D.V. Bacteriological analysis of high-speed handpiece turbines. JADA 1993, 124, 59–62. [Google Scholar] [CrossRef]
- Ishihama, K.; Koizumi, H.; Wada, T.; Iida, S.; Tanaka, S.; Yamanishi, T.; Enomoto, A.; Kogo, M. Evidence of aerosolised floating blood mist during oral surgery. J. Hosp. Infect. 2009, 71, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Mills, S.E. The dental unit waterline controversy: Defusing the myths, defining the solution. J. Am. Dent. Assoc. 2000, 131, 1427–1441. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, A.M.; Sartini, M.; Cristina, M.L. Microbial Contamination of Dental Unit Waterlines and Potential Risk of Infection: A Narrative Review. Pathogens 2020, 9, 651. [Google Scholar] [CrossRef]
- Zemouri, C.; Volgenant, C.M.C.; Buijs, M.J.; Crielaard, W.; Rosema, N.A.M.; Brandt, B.W.; Laheij, A.M.G.A.; De Soet, J.J. Dental aerosols: Microbial composition and spatial distribution. J. Oral Microbiol. 2020, 12, 1762040. [Google Scholar] [CrossRef]
- Carli, E.; Pasini, M.; Lardani, L.; Giuca, G.; Miceli, M. Impact of self-ligating orthodontic brackets on dental biofilm and periodontal pathogens in adolescents. J. Biol. Regul. Homeost. Agents 2021, 35 (Suppl. 1), 107–115. [Google Scholar] [CrossRef]
- Gu, S.; Chen, Z.; Wang, F.; Wang, X. Characterization and inhibition of four fungi producing citrinin in various culture media. Biotechnol. Lett. 2021, 43, 701–710. [Google Scholar] [CrossRef]
- Schalli, M.; Inwinkl, S.M.; Platzer, S.; Baumert, R.; Reinthaler, F.F.; Ofner-Kopeinig, P.; Haas, D. Cefsulodin and Vancomycin: A Supplement for Chromogenic Coliform Agar for Detection of Escherichia coli and Coliform Bacteria from Different Water Sources. Microorganisms 2022, 10, 2499. [Google Scholar] [CrossRef]
- ÖNORM EN ISO 11731; Wasserbeschaffenheit—Zählung von Legionellen. Austrian Standards International: Vienna, Austria, 2018.
- Smith, A.; Smith, G.; Lappin, D.F.; Baxter, H.C.; Jones, A.; Baxter, R.L. Dental handpiece contamination: A proteomics and surface analysis approach. Biofouling 2014, 30, 29–39. [Google Scholar] [CrossRef]
- Büchter, A.; Kruse-Loesler, B. Development of a validated process for manual preparation of dental transmission instruments. Clin. Oral Investig. 2011, 15, 605–608. [Google Scholar] [CrossRef]
- DIN EN 15883-1; Washer-disinfectors—Part 1: General requirements, terms and definitions and tests. Beuth Verlag GmbH: Berlin, Germany, 2006.
- Gazzola, D.; Vincenzi, S.; Pasini, G.; Lomolino, G.; Curioni, A. Advantages of the KDS/BCA Assay over the Bradford Assay for Protein Quantification in White Wine and Grape Juice. Am. J. Enol. Vitic. 2014, 66, 227–233. [Google Scholar] [CrossRef]
- Smith, P.K.; Krohn, R.I.; Hermanson, G.T.; Mallia, A.K.; Gartner, F.H.; Provenzano, M.D.; Fujimoto, E.K.; Goeke, N.M.; Olson, B.J.; Klenk, D.C. Measurement of protein using bicinchoninic acid. Anal. Biochem. 1985, 150, 76–85. [Google Scholar] [CrossRef]
- Schwirzer, S. Entwicklung Eines Biologischen Verfahrens zur Bestimmung von 2,3,7,8-TCDD Äquivalenzwerten in Umweltrelevanten Matrizes unter Einbeziehung chemischer Clean-Up Schritte; Herbert Utz Verlag: Munich, Germany, 1998. [Google Scholar]
- Goldring, J.P.D. Measuring Protein Concentration with Absorbance, Lowry, Bradford Coomassie Blue, or the Smith Bicinchoninic Acid Assay Before Electrophoresis. Methods Mol. Biol. 2019, 1855, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Molinari, J.A. Infection control—Its evolution to the current standard precautions. JADA 2003, 134, 569–574. [Google Scholar] [PubMed]
- Neugeboren, N.; Nisengard, R.J.; Beutner, E.H.; Ferguson, G.W. Control of cross-contamination. JADA 1972, 85, 123–127. [Google Scholar] [CrossRef]
- Allison, J.R.; Edwards, D.C.; Bowes, C.; Pickering, K.; Dowson, C.; Stone, S.J.; Lumb, J.; Durham, J.; Jakubovics, N.; Holliday, R. The effect of high-speed dental handpiece coolant delivery and design on aerosol and droplet production. J. Dent. 2021, 112, 103746. [Google Scholar] [CrossRef] [PubMed]
- Bhandary, N.; Desai, A.; Shetty, Y.B. High speed handpieces. J. Int. Oral Health 2014, 6, 130–132. [Google Scholar] [PubMed]
- Hauman, C.H. Cross-infection risks associated with high-speed dental handpieces. J. Dent. Assoc. S. Afr. 1993, 48, 389–391. [Google Scholar] [PubMed]
- Pantanella, F.; Schippa, S.; Solimini, A.; Rosa, L.; Bettucci, A.; Berlutti, F. Efficacy of acoustic waves in preventing Streptococcus mutans adhesion on dental unit water line. Ann. Ig 2019, 31, 109–116. [Google Scholar] [CrossRef]
- Michels, W.; Schulze-Fincke, D. Kontamination und Aufbereitung zahnärztlicher Übertragungsinstrumente sowie rotierender Instrumente. Aseptica—Fachmag. Krankenh. Prax. 2009, 15, 3–6. [Google Scholar]
- Matys, J.; Grzech-Leśniak, K. Dental Aerosol as a Hazard Risk for Dental Workers. Materials 2020, 13, 5109. [Google Scholar] [CrossRef]
- Senpuku, H.; Fukumoto, M.; Uchiyama, T.; Taguchi, C.; Suzuki, I.; Arikawa, K. Effects of Extraoral Suction on Droplets and Aerosols for Infection Control Practices. Dent. J. 2021, 9, 80. [Google Scholar] [CrossRef] [PubMed]
- Han, P.; Li, H.; Walsh, L.J.; Ivanovski, S. Splatters and Aerosols Contamination in Dental Aerosol Generating Procedures. Appl. Sci. 2021, 11, 1914. [Google Scholar] [CrossRef]
- Rosa, V.; Agarwalla, S.V.; Tan, B.L.; Choo, S.Y.; Sim, Y.F.; Boey, F.Y.C.; Anantharaman, S.; Duggal, M.S.; Tan, K.S. Pandemic Preparedness and Response: A Foldable Tent to Safely Remove Contaminated Dental Aerosols—Clinical Study and Patient Experience. Appl. Sci. 2022, 12, 7409. [Google Scholar] [CrossRef]
- Engsomboon, N.; Pachimsawat, P.; Thanathornwong, B. Comparative Dissemination of Aerosol and Splatter Using Suction Device during Ultrasonic Scaling: A Pilot Study. Dent. J. 2022, 10, 142. [Google Scholar] [CrossRef]
- Innes, N.; Johnson, I.G.; Al-Yaseen, W.; Harris, R.; Jones, R.; Kc, S.; McGregor, S.; Robertson, M.; Wade, W.G.; Gallagher, J.E. A systematic review of droplet and aerosol generation in dentistry. J. Dent. 2021, 105, 103556. [Google Scholar] [CrossRef]
- Takenaka, S.; Sotozono, M.; Yashiro, A.; Saito, R.; Kornsombut, N.; Naksagoon, T.; Nagata, R.; Ida, T.; Edanami, N.; Noiri, Y. Efficacy of Combining an Extraoral High-Volume Evacuator with Preprocedural Mouth Rinsing in Reducing Aerosol Contamination Produced by Ultrasonic Scaling. Int. J. Environ. Res. Public Health 2022, 19, 6048. [Google Scholar] [CrossRef]
- Farah, R.I.; Althunayyan, A.A.; Al-Haj Ali, S.N.; Farah, A.I. Reduction of aerosols and splatter generated during ultrasonic scaling by adding food-grade thickeners to coolants: An in-vitro study. Clin. Oral Investig. 2022, 26, 2863–2872. [Google Scholar] [CrossRef]
- Michels, W.; Pieper, M. Eigenschaften von Blut und Einfluss auf die Reinigung. Zentralsterilisation 2004, 12, 324–330. [Google Scholar]
- Sasaki, J.I.; Imazato, S. Autoclave sterilization of dental handpieces: A literature review. J. Prosthodont Res. 2020, 64, 239–242. [Google Scholar] [CrossRef]
- Smith, A.J. The devil is in the validation and design; managing the risk from opportunistic pathogens in the dental unit. J. Hosp. Infect. 2021, 114, 61–62. [Google Scholar] [CrossRef]
- Leonard, D.L.; Charlton, D.G. Performance of high-speed dental handpieces subjected to simulated clinical use in sterilization. ADA 1999, 130, 1301–1311. [Google Scholar] [CrossRef] [PubMed]
- Weightman, N.C.; Lines, L.D. Problems with the decontamination of dental handpieces and other intra-oral dental equipment in hospitals. J. Hosp. Infect. 2004, 56, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Liu, J.; Chen, L.; Gan, N.; Yang, D. The Oral Microbiome in the Elderly With Dental Caries and Health. Front. Cell. Infect. Microbiol. 2019, 8, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zlatanović, L.; van der Hoek, J.P.; Vreeburg, J.H.G. An experimental study on the influence of water stagnation and temperature change on water quality in a full-scale domestic drinking water system. Water Res. 2017, 123, 761–772. [Google Scholar] [CrossRef]
- Bédard, E.; Laferrière, C.; Déziel, E.; Prévost, M. Impact of stagnation and sampling volume on water microbial quality monitoring in large buildings. PLoS ONE 2018, 13, e0199429. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, J.I.; Dignum, M.; Liu, G.; Medema, G.; van der Hoek, J.P. Changes in biofilm composition and microbial water quality in drinking water distribution systems by temperature increase induced through thermal energy recovery. Environ. Res. 2021, 194, 110648. [Google Scholar] [CrossRef]
- Iwawaki, Y.; Matsuda, T.; Kurahashi, K.; Honda, T.; Goto, T.; Ichikawa, T. Effect of water temperature during ultrasonic denture cleaning. J. Oral Sci. 2019, 61, 140–145. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Gunawan, C.; Barraud, N.; Rice, S.A.; Harry, E.J.; Amal, R. Understanding, Monitoring, and Controlling Biofilm Growth in Drinking Water Distribution Systems. Environ. Sci. Technol. 2016, 50, 8954–8976. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vial | Volume of Diluent (µL) | Volume and Source of BSA | Final BSA Concentration (µg/mL) |
|---|---|---|---|
| A | 0 | 300 of Stock | 2000 |
| B | 125 | 375 of Stock | 1500 |
| C | 325 | 325 of Stock | 1000 |
| D | 175 | 175 of vial b | 750 |
| E | 325 | 325 of vial c | 500 |
| F | 325 | 325 of vial e | 250 |
| G | 325 | 325 of vial f | 125 |
| H | 400 | 100 of vial g | 25 |
| I | 400 | 0 | 0 |
| Vial | Volume of Diluent (µL) | Volume and Source of BSA | Final BSA Concentration (µg/mL) |
|---|---|---|---|
| J | 700 | 100 of Stock | 2000 |
| K | 400 | 400 of vial j | 1500 |
| L | 450 | 300 of vial k | 1000 |
| M | 400 | 400 of vial l | 750 |
| N | 400 | 100 of vial m | 500 |
| O | 400 | 0 | 250 |
| Office | 4 × 105 rpm | 2 × 105 rpm | 4 × 104 rpm | 2 × 104 rpm |
|---|---|---|---|---|
| 1 | x 1 | x | ||
| 2 | x | x | ||
| 3 | x | x | x | x |
| 4 | x | x | ||
| 5 | x | x | ||
| 6 | x | x | x | |
| 7 | x | x | x | x |
| Wipe Disinfection, | Wipe Disinfection, | Wipe Disinfection | |
|---|---|---|---|
| Mech. Cleansing | Mech. Cleansing | ||
| Office | Mech. Disinfection/Sterilization | ||
| 1 | x 2 | ||
| 2 | x | ||
| 3 | x | ||
| 4 | x | ||
| 5 | x | ||
| 6 | x | ||
| 7 | x |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schalli, M.; Kogler, B.; Miorini, T.; Gehrer, M.; Reinthaler, F.F. High-Speed Dental Instruments: An Investigation of Protein-Contaminated Dental Handpieces with the Bicinchoninic Acid Assay in Dental Offices in Styria, Austria. Int. J. Environ. Res. Public Health 2023, 20, 1670. https://doi.org/10.3390/ijerph20031670
Schalli M, Kogler B, Miorini T, Gehrer M, Reinthaler FF. High-Speed Dental Instruments: An Investigation of Protein-Contaminated Dental Handpieces with the Bicinchoninic Acid Assay in Dental Offices in Styria, Austria. International Journal of Environmental Research and Public Health. 2023; 20(3):1670. https://doi.org/10.3390/ijerph20031670
Chicago/Turabian StyleSchalli, Michael, Birgit Kogler, Tillo Miorini, Michael Gehrer, and Franz F. Reinthaler. 2023. "High-Speed Dental Instruments: An Investigation of Protein-Contaminated Dental Handpieces with the Bicinchoninic Acid Assay in Dental Offices in Styria, Austria" International Journal of Environmental Research and Public Health 20, no. 3: 1670. https://doi.org/10.3390/ijerph20031670