

Effectiveness and Evidence Level of Dance on Functioning of Children and Adolescents with Neuromotor Impairments: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Identification and Selection of Studies
2.3. Population
2.4. Intervention
2.5. Comparators
2.6. Outcome Measures
2.7. Study Type
2.8. Data Extraction
2.9. Methodological Quality Assessment
2.10. Evidence Synthesis
3. Results
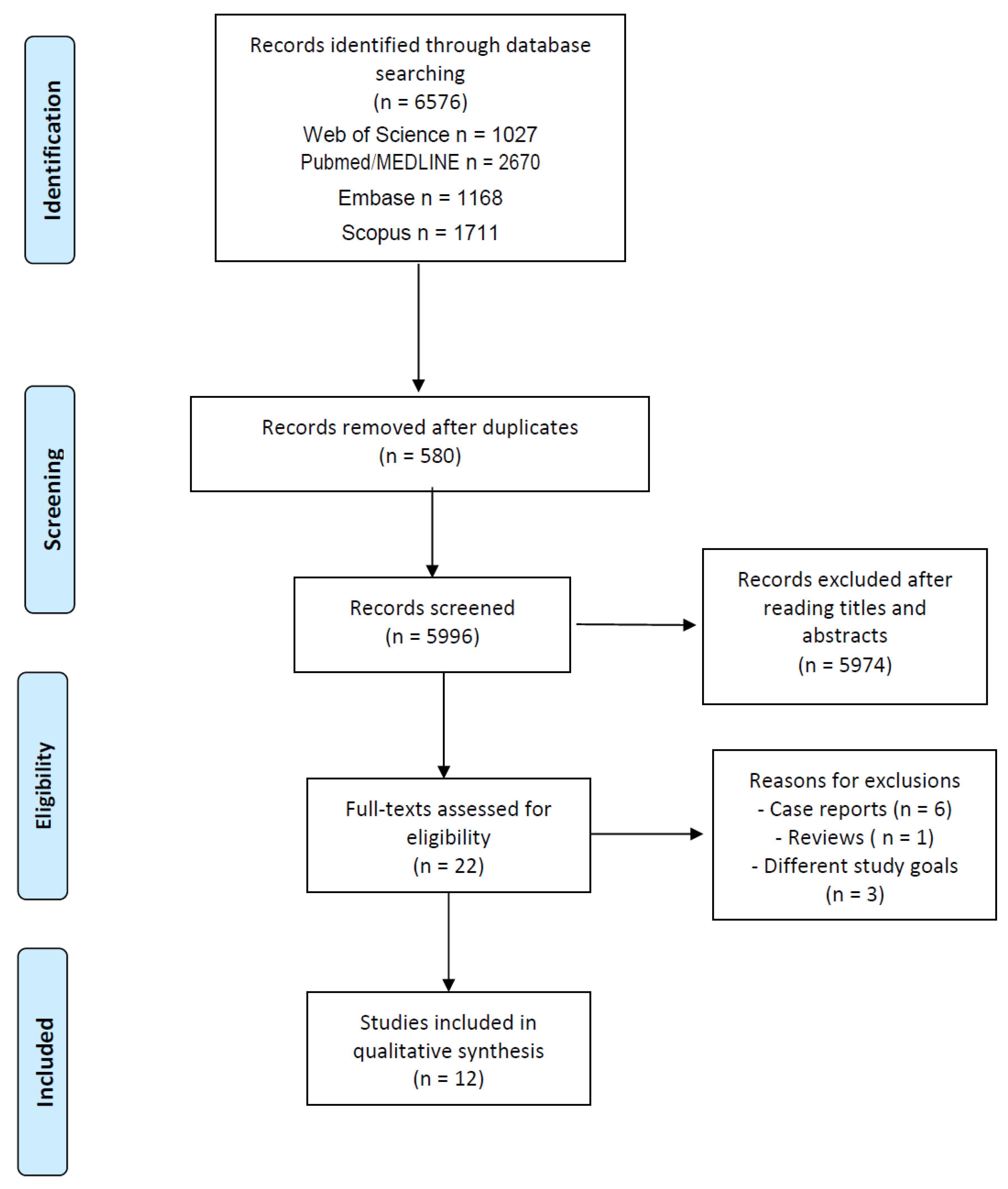
3.1. Search Strategy
3.2. Participants and Intervention Characteristics
3.3. Outcome Measures According to ICF Domains
Effectiveness of Dance Intervention
3.4. Methodological Quality Assessment
3.5. Evidence Synthesis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Field, D.A.; Roxborough, L. Validation of the relation between the type and amount of seating support provided and Level of Sitting Scale (LSS) scores for children with neuromotor disorders. Dev. Neurorehabilit. 2012, 15, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Field, D.A.; Roxborough, L.A. Responsiveness of the Seated Postural Control Measure and the Level of Sitting Scale in children with neuromotor disorders. Disabil. Rehabil. Assist. Technol. 2011, 6, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Levac, D.; Rivard, L.; Missiuna, C. Defining the active ingredients of interactive computer play interventions for children with neuromotor impairments: A scoping review. Res. Dev. Disabil. 2012, 33, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Brazil Ministry of Health; Secretary of Health Care; Department of Strategic Programmatic Actions. Care Guidelines for People with Cerebral Palsy. 2014. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes_atencao_pessoa_paralisia_cerebral.pdf (accessed on 31 January 2022).
- Lakes, K.D.; Sharp, K.; Grant-Beuttler, M.; Neville, R.; Haddad, F.; Sunico, R.; Ho, D.; Schneider, M.; Sawitz, S.; Paulsen, J.; et al. A Six Week Therapeutic Ballet Intervention Improved Gait and Inhibitory Control in Children With Cerebral Palsy—A Pilot Study. Front. Public Health 2019, 7, 137. [Google Scholar] [CrossRef] [PubMed]
- Pena, G.M.; Pavão, S.L.; Oliveira, M.F.; de Campos, A.C.; Rocha, N.A. Dual-task effects in children with neuromotor dysfunction: A systematic review. Eur. J. Phys. Rehabil. Med. 2019, 55, 281–290. [Google Scholar] [CrossRef]
- Brugnaro, B.H.; Oliveira, M.F.P.; de Campos, A.C.; Pavão, S.L.; Rocha, N.A.C.F. Postural control in Down syndrome and relationships with the dimensions of the International Classification of Functioning, Disability and Health—A systematic review. Disabil. Rehabil. 2022, 44, 2207–2222. [Google Scholar] [CrossRef]
- Novak, I.; McIntyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.-A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef]
- Withers, J.W.; Muzzolon, S.B.; Zonta, M.B. Influence of adapted hip-hop dancing on quality of life and social participation among children/adolescents with cerebral palsy. Arq. Neuro-Psiquiatr. 2019, 77, 712–722. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Stewart, D. The world health organization international classification of functioning, disability, and health: A model to guide clinical thinking, practice and research in the field of cerebral palsy. Semin. Pediatr. Neurol. 2004, 11, 5–10. [Google Scholar] [CrossRef]
- Imms, C.; Adair, B.; Keen, D.; Ullenhag, A.; Rosenbaum, P.; Granlund, M. ‘Participation’: A systematic review of language, definitions, and constructs used in intervention research with children with disabilities. Dev. Med. Child Neurol. 2016, 58, 29–38. [Google Scholar] [CrossRef]
- Mobbs, C.A.; Spittle, A.J.; Johnston, L.M. Participation Measures for Infants and Toddlers Aged Birth to 23 Months: A Systematic Review. Phys. Occup. Ther. Pediatr. 2021, 41, 567–589. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF. 2001. Available online: https://apps.who.int/iris/handle/10665/42407 (accessed on 31 January 2022).
- Dos Santos, A.N.; Pavão, S.L.; De Campos, A.C.; Rocha, N.A.C.F. International classification of functioning, disability and health in children with cerebral palsy. Disabil. Rehabil. 2011, 34, 1053–1058. [Google Scholar] [CrossRef] [PubMed]
- Ibragimova, N.; Granlund, M.; Björck-Äkesson, E. Field trial of ICF version for children and youth (ICF-CY) in Sweden: Logical coherence, developmental issues and clinical use. Dev. Neurorehabilit. 2009, 12, 3–11. [Google Scholar] [CrossRef]
- Farias, N.; Buchalla, C.M. A classificação internacional de funcionalidade, incapacidade e saúde da organização mundial da saúde: Conceitos, usos e perspectivas. Rev. Bras. De Epidemiol. 2005, 8, 187–193. [Google Scholar] [CrossRef]
- Teixeira-Machado, L.; Azevedo-Santos, I.; DeSantana, J.M. Dance Improves Functionality and Psychosocial Adjustment in Cerebral Palsy. Am. J. Phys. Med. Rehabil. 2017, 96, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, L.B.; Braga, D.M. Dança e fisioterapia em crianças e adolescentes com paralisia cerebral. Rev. Neurociência 2001, 18, 437–442. [Google Scholar] [CrossRef]
- Murphy, N.A.; Carbone, P.S.; Disabilities, A.T.C.O.C.W. Promoting the Participation of Children With Disabilities in Sports, Recreation, and Physical Activities. Pediatrics 2008, 121, 1057–1061. [Google Scholar] [CrossRef] [Green Version]
- Palisano, R.J.; Orlin, M.; Chiarello, L.A.; Oeffinger, D.; Polansky, M.; Maggs, J.; Gorton, G.; Bagley, A.; Tylkowski, C.; Vogel, L.; et al. Determinants of Intensity of Participation in Leisure and Recreational Activities by Youth With Cerebral Palsy. Arch. Phys. Med. Rehabil. 2011, 92, 1468–1476. [Google Scholar] [CrossRef] [PubMed]
- López-Ortiz, C.; Gaebler-Spira, D.J.; McKeeman, S.N.; McNish, R.N.; Green, D. Dance and rehabilitation in cerebral palsy: A systematic search and review. Dev. Med. Child Neurol. 2019, 61, 393–398. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Hernandes, E.; Zamboni, A.; Fabbri, S.; Di Thommazo, A. Using GQM and TAM to evaluate StArt—A tool that supports Systematic Review. CLEI Electron. J. 2012, 15, 3. [Google Scholar] [CrossRef]
- Arditi, C.; Burnand, B.; Peytremann-Bridevaux, I. Adding non-randomised studies to a Cochrane review brings complementary information for healthcare stakeholders: An augmented systematic review and meta-analysis. BMC Health Serv. Res. 2016, 16, 598. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Cherriere, C.; Martel, M.; Sarrasin, A.; Ballaz, L.; Tallet, J.; Lemay, M. Benefits of a Dance Intervention on Balance in Adolescents with Cerebral Palsy. Phys. Occup. Ther. Pediatr. 2020, 40, 518–533. [Google Scholar] [CrossRef]
- Joung, H.J.; Park, J.; Ahn, J.; Park, M.S.; Lee, Y. Effects of creative dance-based exercise on gait performance in adolescents with cerebral palsy. J. Exerc. Rehabil. 2020, 16, 332–343. [Google Scholar] [CrossRef] [PubMed]
- López-Ortiz, C.; Egan, T.; Gaebler-Spira, D. Pilot study of a targeted dance class for physical rehabilitation in children with cerebral palsy. SAGE Open Med. 2016, 4, 2050312116670926. [Google Scholar] [CrossRef]
- López-Ortiz, C.; Gladden, K.; Deon, L.; Schmidt, J.; Girolami, G.; Gaebler-Spira, D. Dance program for physical rehabilitation and participation in children with cerebral palsy. Arts Health 2012, 4, 39–54. [Google Scholar] [CrossRef]
- Cherriere, C.; Martel, M.; Fortin, S.; Raymond, M.-J.; Veilleux, L.N.; Lemay, M. An adapted dance program for children with Charcot-Marie-Tooth disease: An exploratory study. J. Bodyw. Mov. Ther. 2020, 24, 85–91. [Google Scholar] [CrossRef]
- Takahashi, H.; Seki, M.; Matsumura, T.; An, M.; Sasai, T.; Ogawa, Y.; Matsushima, K.; Tabata, A.; Kato, T. The Effectiveness of Dance/Movement Therapy in Children with Williams Syndrome: A Pilot Study. Am. J. Danc. Ther. 2020, 42, 33–60. [Google Scholar] [CrossRef]
- McGuire, M.; Long, J.; Esbensen, A.J.; Bailes, A.F. Adapted Dance Improves Motor Abilities and Participation in Children With Down Syndrome: A Pilot Study. Pediatr. Phys. Ther. 2019, 31, 76–82. [Google Scholar] [CrossRef]
- Cameron, K.L.; Allison, K.; McGinley, J.L.; Fini, N.A.; Cheong, J.L.; Spittle, A.J. Feasibility of a Dance PaRticipation intervention for Extremely prEterm children with Motor Impairment at prEschool age (Dance PREEMIE). Early Hum. Dev. 2021, 163, 105482. [Google Scholar] [CrossRef] [PubMed]
- Raghupathy, M.K.; Divya, M.; Karthikbabu, S. Effects of Traditional Indian Dance on Motor Skills and Balance in Children with Down syndrome. J. Mot. Behav. 2022, 54, 212–221. [Google Scholar] [CrossRef]
- Dickinson, H.; Rapp, M.; Arnaud, C.; Carlsson, M.; Colver, A.F.; Fauconnier, J.; Lyons, A.; Marcelli, M.; I Michelsen, S.; Parkes, J.; et al. Predictors of drop-out in a multi-centre longitudinal study of participation and quality of life of children with cerebral palsy. BMC Res. Notes 2012, 5, 300. [Google Scholar] [CrossRef] [Green Version]
- Van der Heide, J.C.; Begeer, C.; Fock, J.M.; Otten, B.; Stremmelaar, E.; A van Eykern, L.; Hadders-Algra, M. Postural control during reaching in preterm children with cerebral palsy. Dev. Med. Child Neurol. 2004, 46, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Woollacott, M.; Shumway-Cook, A.; Hutchinson, S.; Ciol, M.; Price, R.; Kartin, D. Effect of balance training on muscle activity used in recovery of stability in children with cerebral palsy: A pilot study. Dev. Med. Child Neurol. 2005, 47, 455–461. [Google Scholar] [CrossRef]
- Assis, G.S.; Schlichting, T.; Mateus, B.R.; Lemos, A.G.; dos Santos, A.N. Physical therapy with hippotherapy compared to physical therapy alone in children with cerebral palsy: Systematic review and meta-analysis. Dev. Med. Child Neurol. 2022, 64, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.M.; Cavagnino, D.T.; Bhat, A.N. Effects of Equine Therapy on Individuals with Autism Spectrum Disorder: A Systematic Review. Rev. J. Autism Dev. Disord. 2018, 5, 156–175. [Google Scholar] [CrossRef]
- Peters, B.C.M.; Wood, W. Autism and Equine-Assisted Interventions: A Systematic Mapping Review. J. Autism Dev. Disord. 2017, 47, 3220–3242. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Gorter, J.W. The ‘F-words’ in childhood disability: I swear this is how we should think! Child Care Health Dev. 2012, 38, 457–463. [Google Scholar] [CrossRef]


{kind=link}
| Study | Study Design | Participants | Intervention | Duration | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N (IG+CG) | Age Range | Health Condition | Classification Health Condtion | Session | Frequency (Days/Week) | Protocol | Follow Up | Comparators | |||
| [33] | Case series design | N = 10 IG = 10 CG = 0 | 0–3 years | extremely preterm and extremely low birth weight expressing motor impairments at 3 years’ corrected age | MABC-2 scored ≤16th | Dance PREEMIE | 30–60 min | 1×/week | 8 weeks | - | - |
| [34] | Randomised controlled, double-arm trial | N = 36 IG = 18 CG = 18 | 6–10 years | Down syndrome | <5 Beighton’s hypermobility test | Indian classical dance | 60 min | 3×/week | 6 weeks | - | Conventional therapy |
| [26] | Non-randomized controlled clinical trial | N = 9 IG = 5 CG = 4 | 7–12 years | CMT | - | Adapted dance program | 60 min | 2×/week | 10 weeks | - | Regular care |
| [30] | Case series design | N = 10 IG = 10 CG = 0 | 10–17 years | CP | GMFCS I a III Spastic N = 6 Ataxic N = 1 Dyscinetic N = 1 Spastic dyscinect N = 1 | Dance intervention. | 60 a 90 min | 2×/week | 10 weeks | - | - |
| [27] | Single-group cohort study | N = 13 IG = 13 CG = 0 | 13–20 years | CP | GMFCS I N = 3 GMFCS II N = 7 | Let’s Be Creative Dance Exercise program | 120 min | 2×/week | 12 weeks | - | - |
| [9] | Non-randomized controlled clinical trial | N = 18 IG = 9 CG = 9 | 10–13 years | CP | GMFCS I GMFCS II | Adapted hip-hop dancing | 60 min | 1×/week | 20 months | - | Conventional therapy |
| [31] | Case series design | N = 4 IG = 4 CG = 0 | 5–10 years | Willians syndrome | - | Dance/ movement therapy (DMT) | 60 min | 1×/week | 10 sessions | - | - |
| [28] | Non-randomized controlled clinical trial | N = 12 IG = 6 CG = 6 | 7–15 years | CP | GMFCS II N = 6 GMFCS III N = 3 GMFCS IV N = 2 | Targeted dance class, utilizing classical ballet principles for rehabilitation | 60 min | 3×/week | 4 weeks | After 1 month | Conventional therapy |
| [29] | Single-group cohort study | N = 16 IG = 16 CG = 0 | - | CP | GMFCS I e II GMFCS III e IV | Classical ballet program | - | 1×/week | 5 a 8 weeks | - | - |
| [32] | Single-group cohort study | N = 14 IG = 14 CG = 0 | 4–13 years | Down syndrome | - | Adapted dance program | 60 min | 1×/week | 20 weeks | - | - |
| [5] | Single-group cohort study | N = 8 IG = 8 CG = 0 | 9–14 years | CP | - | Therapeutic Ballet | 60 min | 3×/week | 6 weeks | After 4–5 weeks. | - |
| [17] | Randomized controlled clinical trial | N = 26 IG= 13 CG= 13 | 15–29 years | CP | GMFCS II N= 9 GMFCS III N= 8 GMFCS IV N= 7 GMFCS V N= 2 | Dance class | 60 min | 2×/week | 12 weeks | - | Conventional therapy |
| Study | Body Structure and Function | Activity | Participation | Contextual Factors | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Evaluation Tool | Evaluated Task | Task Manipulation | Instruments | Evaluated Components | Instruments | Personal | Environmental | Instruments | |
| [33] | - Motor impairment | - MABC-2 | - Parents set goals for the children with a focus on motor and cognitive activity components | - COPM | - Parents set goals for children with a focus on participation | - COPM | - Enjoyment of dance classes | - | - Smiley face scale | |
| - Sedentay behavior and physical activity time | - Pre-PAQ | |||||||||
| [34] | - | - | - Agility and coordination on gait, control of object manipulation, grasping, visual-motor integration skills - dynamic balance and motor planning - functional balance | - TGMD-2 - FSST - PBS | - | - | - | - | - | |
| [26] | - Pain | - EVA | - Stay in orthostatism | - Eyes opened, eyes closed, and dual-task condition | - Subtest of Mira Stamback - Score! and Score DT - (Tea-Ch) | - | - | - | - | - |
| - Level of incapacity | - CMTPedS | |||||||||
| - ROM (knee extensors; ankle dorsiflexors) | - Goniomery | - Cognitive task and rhythm | ||||||||
| - Strength measures hip, knee - And ankle muscles - Muscle Power - AP and ML amplitude, velocity of CoP sway | - Lafayette Force platform | - Simple and divided sustained | ||||||||
| - Memory short term and working memory - Task memory | - WISC-IV | - Task attention | ||||||||
| [30] | - AP and ML amplitude and velocity of CoP sway | - Force platform | - Functional balance - Manual reaching - Gait - Rithimic tasks - Attention | - Simple, sustained, divided sustained | - PBS - PRT - 10 min walking test - Subtest of Mira Stamback - TEA-Ch (Score! and Score DT (Tea-Ch) | - | - | - | - | - |
| [27] | - Hip, knee, and ankle ROM in sagital plane | - Vicon Motion System | - Gait - Gross motor function | - | - Velocity; cadence; step length; support time uni/bipodal - GMFM-88 | - | - | - Body image | - | - BCS |
| [9] | - Pain and comfort level | - PODCI | - Upper extremity and physical function - Transfer and basic mobility—Sporting and physical function - Global function | - | - PODCI | - | - | - Happiness level - Sociability and emotional and behavior problems - Concentration, self-confidence, and aptitude | - | - Parents self-applicable questionnaire - PODCI - CBCL - Instructor’s perspective |
| [31] | - AP/ML amplitude and of sway of CoP - Strength of knee extens/flexors, ankle dorsiflexors/plantar flexors | - Force platform - Handheld dynamometers | - Static stance maintenance - Functional mobility | - Eyes open/eyes closed | - TUG | - | - | - Sociability and emotional and behavior problems | - | - CBCL |
| [28] | - | - | - Functional balance. - Quality of movement upper extremities | - PBS - QUEST | - | - | - | - | - | |
| [29] | - | - | - | - | - | - Parental participation and perception of dance therapeutic benefits | - Specific questionnaires for parents, children, and therapists, based on the LIFE-H | - | - | |
| [32] | - | - | - Gross motor function - Motor performance | - | - GMFM-88 - COPM | - Performance, satisfaction with individualized participation goals | - COPM | - | - | - |
| [5] | - BMI - Percent body fat and bone density - Hand Grip Strength | - Stadiometer - Densitometer - Handgrip dynamometer | - Selective voluntary motor control - Gait - Executive function - Habitual activity level | - | - ESCALE - GAITRite - Hearts and Flowers EF tasks - Activity monitors | - | - | - | - | - |
| [17] | - | - | - Funtional activity - Functional independence | - | - WHODAS - FIM | - | - | - | - | - |
| Study | Main Results | ||||
|---|---|---|---|---|---|
| Body Structure and Functions | Activity | Participation | Contextual Factors (Personal) | Contextual Factors (Environmental) | |
| [33] | Pre- and post-intervention using the MABC-2 were not compared. | In the COPM performance score, score, each child had at least one goal with clinically significant improvement (median of 2 goals achieved, range 1–4). Four children achieved both participation and activity goals, three children achieved goals classified as activity, while one child achieved a participation goal. | In the COPM performance score, one child achieved the goals classified as participation. Not able to compare pre- and post-intervention using the Pré-PAQ. | In the COPM performance score, all children achieved the goals classified as satisfaction. | |
| [34] | - | The traditional Indian dance improved the locomotor skills, objective control, dynamic balance, and motor planning of children with Down syndrome more than that of neuromuscular exercises. Both the dance and neuromuscular training equally impacted the balance capacity. | - | - | - |
| [26] | Improvements on hip extensors, knee flexors and ankle dorsiflexor muscle strenght. Pain levels during physucal activity decreased following the protocol. | Improvements in cognitive features (attention and rithmic tasks). | |||
| [30] | No significant change was observed following protocol on the center of force amplitudes and speeds in the AP and ML axis for the static balance test. | PBS and PRT scores increased following dance protocol. PRT increased during first month of intervention, then remaining constant. There were increases in rhythm production. | |||
| [27] | Hip and ankle range of movement during walking increased in sagittal plane. | Significative improvements in GMFM scores dimensions D and E, walking velocity and cadence, step and stride length. The time of opposite foot off and first double-limb support decreased, whereas percentage of single-limb support time increased following protocol. | Scores of body cathexis scale increased. | ||
| [9] | Reduction of somatic complaints following dance intervention. | Improvements in transfer and basic mobility domains from pediatric outcomes data collection instrument, as well increase in sporting and physical function and global function following dance intervention. | Reduction in emotional and behavioral problems and an increase in social competence in the biopsychosocial profile. | ||
| [31] | Participants showed decreased postural sway in static stance with eyes open and with eyes closed following intervention. There were improvements in knee extensors and flexors and in hip extensors muscles. Ankle plantar flexors strength increased in half of the participants. | Most of the participants showed reduction smaller than 1s in Timed up and Go test (only one reduced 1.5s). | There were no differences in the emotional and behavioral tests. | ||
| [28] | Participants showed significant improvements in PBS scores following dance protocol. There were not significant differences in quality of upper extremity skills test. | ||||
| [29] | Children reported high enjoyment level and desire for more classes. Parents reported perceived therapeutic benefits and therapist viewed the classes as a positive adjunct to therapy | ||||
| [32] | Significative improvements in GMFM scores dimensions D and E. | Although caregiver reported physical, cognitive, and emotional improvements following dance protocol, and COPM did not show significant changes. | |||
| [5] | No significant changes we found for body composition, bony density, and hand muscle strength. | No significant changes we found for habitual physical activity and selective motor control of lower extremity, Time of ambulation decreased following dance protocol. There were significant differences in step length on right and stride length on left. There was improvement in inhibitory control with large individual response primarily among those above the mean at baseline. | |||
| [17] | Significant improvements in domains of independence function, mainly mobility and communication in FIM. Improvements in body function, activity, and participation in WHODAS. | ||||
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | Classification |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [33] | NA | NA | NA | NA | − | − | + | − | − | ? | − | ? | High risk of bias |
| [34] | + | + | + | − | + | + | NA | NA | + | − | + | ? | High risk of bias |
| [26] | − | − | + | − | + | − | NA | NA | + | − | + | ? | High risk of bias |
| [30] | NA | NA | NA | NA | − | + | + | − | + | − | + | ? | High risk of bias |
| [27] | NA | NA | NA | NA | − | − | + | − | + | − | − | ? | High risk of bias |
| [31] | NA | NA | NA | NA | − | − | + | − | + | − | + | ? | High risk of bias |
| [9] | − | − | + | − | − | − | NA | NA | + | − | ? | ? | High risk of bias |
| [28] | − | − | + | ? | − | − | NA | NA | + | ? | + | ? | High risk of bias |
| [29] | NA | NA | NA | NA | − | − | + | − | + | − | ? | ? | High risk of bias |
| [32] | NA | NA | NA | NA | − | − | + | − | + | − | − | ? | High risk of bias |
| [5] | NA | NA | NA | NA | − | + | + | + | + | ? | + | ? | High risk of bias |
| [17] | + | + | + | − | + | + | NA | NA | + | ? | − | ? | High risk of bias |
| Question: Dance Should Be Used in the Rehabilitation of Children and Adolescents with Neuromotor Disability? | |||||||
|---|---|---|---|---|---|---|---|
| Body Structure and Function Outcomes | Sample Size | Risk of Bias | Inconsistency | Indirecteness | Imprecision | Publication Bias | Overall Certainty of Evidence |
| Postural sway [26,30,31] | 23 | Very serious a,b,c,d | Not Serious | Serious e | Very serious g | Very serious h | ⨁◯◯◯ VERY LOW |
| Range of movement lower limbs [26,27] | 23 | Very serious a,b,c,d | Not serious | Serious e | Very serious g | None | ⨁◯◯◯ VERY LOW |
| Pain [9,26] | 27 | Very serious a,b,c,d | Not serious | Very serious e | Very serious g | None | ⨁◯◯◯ VERY LOW |
| Muscle strength lower limbs [26,31] | 13 | Very serious a,b,c,d | Not serious | Serious e | Very serious g | None | ⨁◯◯◯ VERY LOW |
| Activity Outcomes | Sample Size | Risk of Bias | Inconsistency | Indirectenes | Imprecision | Publication Bias | Overall Certainty of Evidence |
| Rhythm [26,30] | 19 | Very serious a,b,c,d | Not serious | Not serious | Very serious v | Very serious h | ⨁◯◯◯VERY LOW |
| Gait [5,26,26] | 31 | Very serious a,c,d | Not Serious | Serious e,f | Very serious g | None | ⨁◯◯◯ VERY LOW |
| Attention [26,30] | 19 | Very serious a,b,c,d | Not serious | Not serious | Very serious g | Very serious h | ⨁◯◯◯ VERY LOW |
| Gross motor function [17,26,32,34] | 53 | Very serious a,b,c,d | Not serious | Very serious e | Very serious g | None | ⨁◯◯◯ VERY LOW |
| Funcional balance [28,30,34] | 22 | Very serious a,b,c,d | Not serious | Serious e | Very serious g | None | ⨁◯◯◯ VERY LOW |
| Contextual Factors (Personal) | Sample Size | Risk of Bias | Inconsistency | Indirecteness | Imprecision | Publication Bias | Overall Certainty of Evidence |
| [9,33] | 28 | Very serious a,b,c,d | Not serious | Serious f | Very serious g | None | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lima, E.F.; Brugnaro, B.H.; Rocha, N.A.C.F.; Pavão, S.L. Effectiveness and Evidence Level of Dance on Functioning of Children and Adolescents with Neuromotor Impairments: A Systematic Review. Int. J. Environ. Res. Public Health 2023, 20, 1501. https://doi.org/10.3390/ijerph20021501
Lima EF, Brugnaro BH, Rocha NACF, Pavão SL. Effectiveness and Evidence Level of Dance on Functioning of Children and Adolescents with Neuromotor Impairments: A Systematic Review. International Journal of Environmental Research and Public Health. 2023; 20(2):1501. https://doi.org/10.3390/ijerph20021501
Chicago/Turabian StyleLima, Elisangela F., Beatriz H. Brugnaro, Nelci Adriana C. F. Rocha, and Silvia L. Pavão. 2023. "Effectiveness and Evidence Level of Dance on Functioning of Children and Adolescents with Neuromotor Impairments: A Systematic Review" International Journal of Environmental Research and Public Health 20, no. 2: 1501. https://doi.org/10.3390/ijerph20021501