
Breakfast Quality and Insulin Resistance in Spanish Schoolchildren: A Cross-Sectional Study
 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
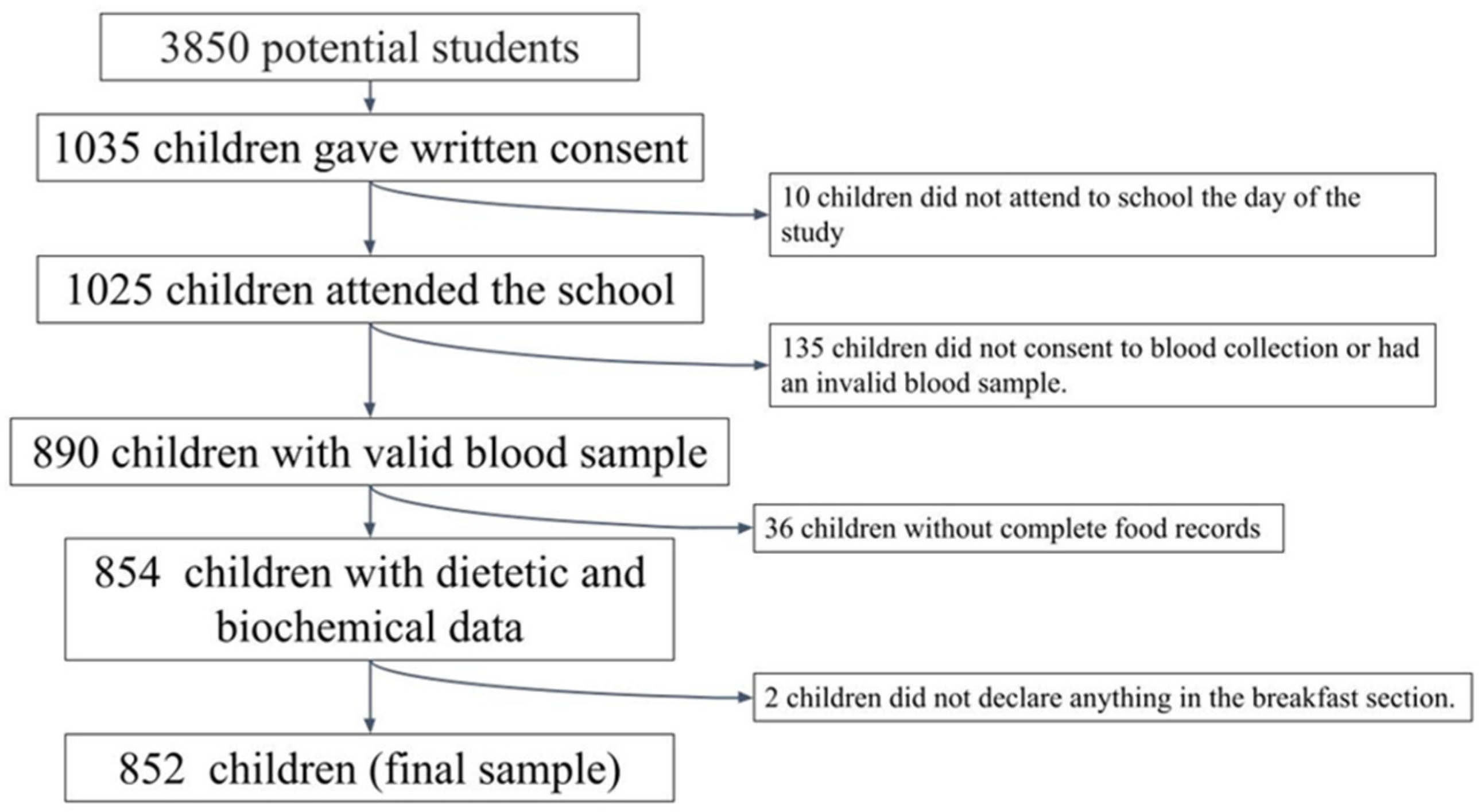
2.1. Study Sample
2.2. Socio-Demographic Data
2.3. Anthropometric Data
2.4. Physical Activity Data
2.5. Dietary Data
2.6. Definition of Breakfast
2.7. Breakfast Quality Index (BQI)
2.8. Biochemical Data
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Affenito, S.G. Breakfast: A Missed Opportunity. J. Am. Diet. Assoc. 2007, 107, 565–569. [Google Scholar] [CrossRef]
- Vereecken, C.; Dupuy, M.; Rasmussen, M.; Kelly, C.; Nansel, T.R.; Al Sabbah, H.; Baldassari, D.; Jordan, M.D.; Maes, L.; Niclasen, B.V.L.; et al. Breakfast Consumption and Its Socio-Demographic and Lifestyle Correlates in Schoolchildren in 41 Countries Participating in the HBSC Study. Int. J. Public Health 2009, 54 (Suppl. S2), 180–190. [Google Scholar] [CrossRef] [Green Version]
- Hallström, L.; Labayen, I.; Ruiz, J.R.; Patterson, E.; Vereecken, C.A.; Breidenassel, C.; Gottrand, F.; Huybrechts, I.; Manios, Y.; Mistura, L.; et al. Breakfast Consumption and CVD Risk Factors in European Adolescents: The HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutr. 2013, 16, 1296–1305. [Google Scholar] [CrossRef] [Green Version]
- Monzani, A.; Ricotti, R.; Caputo, M.; Solito, A.; Archero, F.; Bellone, S.; Prodam, F. A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future? Nutrients 2019, 11, 387. [Google Scholar] [CrossRef] [Green Version]
- Aesan-Agencia Española de Seguridad Alimentaria y Nutrición. Available online: https://www.aesan.gob.es/AECOSAN/web/nutricion/detalle/aladino_2019.htm (accessed on 7 October 2022).
- Moreno, E.R.; Valero Gaspar, T.; Alonso, P.R.; Díaz-Roncero González, A.; Carús, A.G.; Manuel, J.; Torres, Á.; Moreiras, G.V. Estado de Situación Sobre El Desayuno En España. 2008. Available online: https://pesquisa.bvsalud.org/portal/resource/pt/lis-46019 (accessed on 2 January 2023).
- Cuadrado-Soto, E.; López-Sobaler, A.M.; Jiménez-Ortega, A.I.; Bermejo, L.M.; Aparicio, A.; Ortega, R.M. Breakfast Habits of a Representative Sample of the Spanish Child and Adolescent Population (The ENALIA Study): Association with Diet Quality. Nutrients 2020, 12, 3772. [Google Scholar] [CrossRef]
- Coulthard, J.D.; Palla, L.; Pot, G.K. Breakfast Consumption and Nutrient Intakes in 4-18-Year-Olds: UK National Diet and Nutrition Survey Rolling Programme (2008–2012). Br. J. Nutr. 2017, 118, 280–290. [Google Scholar] [CrossRef] [Green Version]
- Szajewska, H.; Ruszczyński, M. Systematic Review Demonstrating That Breakfast Consumption Influences Body Weight Outcomes in Children and Adolescents in Europe. Crit. Rev. Food Sci. Nutr. 2010, 50, 113–119. [Google Scholar] [CrossRef]
- Rosato, V.; Edefonti, V.; Parpinel, M.; Milani, G.P.; Mazzocchi, A.; Decarli, A.; Agostoni, C.; Ferraroni, M. Energy Contribution and Nutrient Composition of Breakfast and Their Relations to Overweight in Free-Living Individuals: A Systematic Review. Adv. Nutr. 2016, 7, 455. [Google Scholar] [CrossRef] [Green Version]
- Adolphus, K.; Lawton, C.L.; Champ, C.L.; Dye, L. The Effects of Breakfast and Breakfast Composition on Cognition in Children and Adolescents: A Systematic Review. Adv. Nutr. 2016, 7, 590S–612S. [Google Scholar] [CrossRef] [Green Version]
- Ferrer-Cascales, R.; Sánchez-Sansegundo, M.; Ruiz-Robledillo, N.; Albaladejo-Blázquez, N.; Laguna-Pérez, A.; Zaragoza-Martí, A. Eat or Skip Breakfast? The Important Role of Breakfast Quality for Health-Related Quality of Life, Stress and Depression in Spanish Adolescents. Int. J. Environ. Res. Public Health 2018, 15, 1781. [Google Scholar] [CrossRef]
- O’Neil, C.E.; Byrd-Bredbenner, C.; Hayes, D.; Jana, L.; Klinger, S.E.; Stephenson-Martin, S. The Role of Breakfast in Health: Definition and Criteria for a Quality Breakfast. J. Acad. Nutr. Diet. 2014, 114, S8–S26. [Google Scholar] [CrossRef]
- Niemeier, H.M.; Raynor, H.A.; Lloyd-Richardson, E.E.; Rogers, M.L.; Wing, R.R. Fast Food Consumption and Breakfast Skipping: Predictors of Weight Gain from Adolescence to Adulthood in a Nationally Representative Sample. J. Adolesc. Health 2006, 39, 842–849. [Google Scholar] [CrossRef]
- Nicklas, T.A. Dietary Studies of Children and Young Adults (1973-1988): The Bogalusa Heart Study. Am. J. Med. Sci. 1995, 310 (Suppl. S1), S101–S108. [Google Scholar] [CrossRef]
- Tagi, V.M.; Giannini, C.; Chiarelli, F. Insulin Resistance in Children. Front. Endocrinol. 2019, 10, 342. [Google Scholar] [CrossRef] [Green Version]
- Levy-Marchal, C.; Arslanian, S.; Cutfield, W.; Sinaiko, A.; Druet, C.; Marcovecchio, M.L.; Chiarelli, F.; Amemiyia, S.; Berenson, G.; Caprio, S.; et al. Insulin Resistance in Children: Consensus, Perspective, and Future Directions. J. Clin. Endocrinol. Metab. 2010, 95, 5189. [Google Scholar] [CrossRef] [Green Version]
- Courtney, C.H.; Olefsky, J.M. Insulin Resistance. In Mechanisms of Insulin Action: Medical Intelligence Unit; Springer: New York, NY, USA, 2021; pp. 185–209. [Google Scholar] [CrossRef]
- Jurkovičová, J.; Hirošová, K.; Vondrová, D.; Samohýl, M.; Štefániková, Z.; Filová, A.; Kachútová, I.; Babjaková, J.; Argalášová, L. The Prevalence of Insulin Resistance and the Associated Risk Factors in a Sample of 14–18-Year-Old Slovak Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 909. [Google Scholar] [CrossRef]
- Gingras, V.; Rifas-Shiman, S.L.; Taveras, E.M.; Oken, E.; Hivert, M.F. Dietary Behaviors throughout Childhood Are Associated with Adiposity and Estimated Insulin Resistance in Early Adolescence: A Longitudinal Study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 129. [Google Scholar] [CrossRef]
- Werneck, A.O.; Agostinete, R.R.; Cayres, S.U.; Urban, J.B.; Wigna, A.; de Moraes Chagas, L.G.; Torres, W.; Fernandes, R.A. Association between Cluster of Lifestyle Behaviors and HOMA-IR among Adolescents: ABCD Growth Study. Medicina 2018, 54, 96. [Google Scholar] [CrossRef] [Green Version]
- Karatzi, K.; Moschonis, G.; Barouti, A.A.; Lionis, C.; Chrousos, G.P.; Manios, Y. Dietary Patterns and Breakfast Consumption in Relation to Insulin Resistance in Children. The Healthy Growth Study. Public Health Nutr. 2014, 17, 2790–2797. [Google Scholar] [CrossRef]
- Marlatt, K.L.; Farbakhsh, K.; Dengel, D.R.; Lytle, L.A. Breakfast and Fast Food Consumption Are Associated with Selected Biomarkers in Adolescents. Prev. Med. Rep. 2016, 3, 49. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, J.P.; Cardel, M.I.; Cellini, J.; Hu, F.B.; Guasch-Ferré, M. Breakfast Skipping, Body Composition, and Cardiometabolic Risk: A Systematic Review and Meta-Analysis of Randomized Trials. Obesity 2020, 28, 1098–1109. [Google Scholar] [CrossRef]
- Joo, H.J.; Kim, G.R.; Park, E.C.; Jang, S.I. Association between Frequency of Breakfast Consumption and Insulin Resistance Using Triglyceride-Glucose Index: A Cross-Sectional Study of the Korea National Health and Nutrition Examination Survey (2016–2018). Int. J. Environ. Res. Public Health 2020, 17, 3322. [Google Scholar] [CrossRef]
- Apergi, K.; Karatzi, K.; Reppas, K.; Karaglani, E.; Usheva, N.; Giménez-Legarre, N.; Moreno, L.A.; Dimova, R.; Antal, E.; Jemina, K.; et al. Association of Breakfast Consumption Frequency with Fasting Glucose and Insulin Sensitivity/b Cells Function (HOMA-IR) in Adults from High-Risk Families for Type 2 Diabetes in Europe: The Feel4Diabetes Study. Eur. J. Clin. Nutr. 2022, 76, 1600–1610. [Google Scholar] [CrossRef]
- Arenaza, L.; Muñoz-Hernández, V.; Medrano, M.; Oses, M.; Amasene, M.; Merchán-Ramírez, E.; Cadenas-Sanchez, C.; Ortega, F.B.; Ruiz, J.R.; Labayen, I. Association of Breakfast Quality and Energy Density with Cardiometabolic Risk Factors in Overweight/Obese Children: Role of Physical Activity. Nutrients 2018, 10, 1066. [Google Scholar] [CrossRef] [Green Version]
- López-Sobaler, A.M.; Cuadrado-Soto, E.; Peral-Suárez, Á.; Aparicio, A.; Ortega, R.M. Importance of Breakfast in the Nutritional and Health Improvement of the Population. Nutr. Hosp. 2018, 35, 3–6. [Google Scholar] [CrossRef]
- Blasco, M.M. Breakfast Food Advertisements in Mediterranean Countries: Products’ Sugar Content in the Adverts from 2015 to 2019. Children 2021, 8, 14. [Google Scholar] [CrossRef]
- Jeans, M.R.; Asigbee, F.M.; Landry, M.J.; Vandyousefi, S.; Ghaddar, R.; Leidy, H.J.; Davis, J.N. Breakfast Consumption in Low-Income Hispanic Elementary School-Aged Children: Associations with Anthropometric, Metabolic, and Dietary Parameters. Nutrients 2020, 12, 2038. [Google Scholar] [CrossRef]
- Leidy, H.J.; Gwin, J.A.; Roenfeldt, C.A.; Zino, A.Z.; Shafer, R.S. Evaluating the Intervention-Based Evidence Surrounding the Causal Role of Breakfast on Markers of Weight Management, with Specific Focus on Breakfast Composition and Size. Adv. Nutr. 2016, 7, 563S–575S. [Google Scholar] [CrossRef] [Green Version]
- Gwin, J.A.; Leidy, H.J. Breakfast Consumption Augments Appetite, Eating Behavior, and Exploratory Markers of Sleep Quality Compared with Skipping Breakfast in Healthy Young Adults. Curr. Dev. Nutr. 2018, 2, nzy074. [Google Scholar] [CrossRef] [Green Version]
- Leidy, H.J.; Ortinau, L.C.; Douglas, S.M.; Hoertel, H.A. Beneficial effects of a higher-protein breakfast on the appetitive, hormonal, and neural signals controlling energy intake regulation in overweight/obese, “breakfast-skipping”, late-adolescent girls. Am. J. Clin. Nutr. 2013, 97, 677–688. [Google Scholar] [CrossRef] [Green Version]
- Douglas, S.M.; Byers, A.W.; Leidy, H.J. Habitual Breakfast Patterns Do Not Influence Appetite and Satiety Responses in Normal vs. High-Protein Breakfasts in Overweight Adolescent Girls. Nutrients 2019, 11, 1223. [Google Scholar] [CrossRef] [Green Version]
- Pereira, M.A.; Erickson, E.; McKee, P.; Schrankler, K.; Raatz, S.K.; Lytle, L.A.; Pellegrini, A.D. Breakfast Frequency and Quality May Affect Glycemia and Appetite in Adults and Children. J. Nutr. 2011, 141, 163–168. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, F.; Martins-Bock, P.; Trotte-Motta, M.; Helal, L. Biochemical and Molecular Mechanisms of Glucose Uptake Stimulated by Physical Exercise in Insulin Resistance State: Role of Inflammation. Arq. Bras. Cardiol. 2019, 113, 1139–1148. [Google Scholar] [CrossRef]
- Scheithauer, T.P.M.; Rampanelli, E.; Nieuwdorp, M.; Vallance, B.A.; Verchere, B.; van Raalte, D.H.; Herrema, H. Gut Microbiota as a Trigger for Metabolic Inflammation in Obesity and Type 2 Diabetes. Front. Immunol. 2020, 11, 571731. [Google Scholar] [CrossRef]
- Aznar, L.A.M.; Carou, M.D.C.V.; Sobaler, A.M.L.; Moreiras, G.V.; Villares, J.M.M. Role of Breakfast and Its Quality in the Health of Children and Adolescents in Spain. Nutr. Hosp. 2021, 38, 396–409. [Google Scholar] [CrossRef]
- Giovannini, M.; Verduci, E.; Scaglioni, S.; Salvatici, E.; Bonza, M.; Riva, E.; Agostoni, C. Breakfast: A Good Habit, Not a Repetitive Custom. J. Int. Med. Res. 2008, 36, 613–624. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, K.; Schwingshackl, L.; Gottschald, M.; Knüppel, S.; Stelmach-Mardas, M.; Aleksandrova, K.; Boeing, H. Breakfast Quality and Cardiometabolic Risk Profiles in an Upper Middle-Aged German Population. Eur. J. Clin. Nutr. 2017, 71, 1312. [Google Scholar] [CrossRef] [Green Version]
- Sámano, R.; Hernández-Chávez, C.; Chico-Barba, G.; Córdova-Barrios, A.; Morales-Del-olmo, M.; Sordo-Figuero, H.; Hernández, M.; Merino-Palacios, C.; Cervantes-Zamora, L.; Martínez-Rojano, H. Breakfast Nutritional Quality and Cognitive Interference in University Students from Mexico City. Int. J. Environ. Res. Public Health 2019, 16, 2671. [Google Scholar] [CrossRef] [Green Version]
- Monteagudo, C.; Palacín-Arce, A.; del Mar Bibiloni, M.; Pons, A.; Tur, J.A.; Olea-Serrano, F.; Mariscal-Arcas, M. Proposal for a Breakfast Quality Index (BQI) for Children and Adolescents. Public Health Nutr. 2012, 16, 639–644. [Google Scholar] [CrossRef]
- Pereira, J.L.; de Castro, M.A.; Hopkins, S.; Gugger, C.; Fisberg, R.M.; Fisberg, M. Proposal for a Breakfast Quality Index for Brazilian Population: Rationale and Application in the Brazilian National Dietary Survey. Appetite 2017, 111, 12–22. [Google Scholar] [CrossRef]
- Félix, P.V.; Pereira, J.L.; Leme, A.C.B.; de Castro, M.A.; Fisberg, R.M. Nutritional Breakfast Quality and Cardiometabolic Risk Factors: Health Survey of São Paulo, a Population-Based Study. Public Health Nutr. 2021, 24, 4102–4112. [Google Scholar] [CrossRef]
- Monteagudo, C.; Téllez, F.; Heras-González, L.; Ibañez-Peinado, D.; Mariscal-Arcas, M.; Olea-Serrano, F. School dietary habits and incidence of dental caries. Nutr. Hosp. 2015, 32, 383–388. [Google Scholar] [CrossRef]
- Rodríguez-Rodríguez, E.; Salas-González, M.D.; Ortega, R.M.; López-Sobaler, A.M. Leukocytes and Neutrophil–Lymphocyte Ratio as Indicators of Insulin Resistance in Overweight/Obese School-Children. Front. Nutr. 2022, 8, 1318. [Google Scholar] [CrossRef]
- Salas-González, M.D.; Aparicio, A.; Loria-Kohen, V.; Ortega, R.M.; López-Sobaler, A.M. Association of Healthy Eating Index-2015 and Dietary Approaches to Stop Hypertension Patterns with Insulin Resistance in Schoolchildren. Nutrients 2022, 14, 4232. [Google Scholar] [CrossRef]
- World Health Organization. World Health Organization Physical Status: The Use and Interpretation of Anthropometry; Report of the WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995; p. 543. [Google Scholar]
- WHO. Body Mass Index. Kans Nurse 2004, 79, 9. [Google Scholar]
- Onis, M.; Onyango, A.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; de Ridder, H. International Protocol for Anthropometric Assessment; Hutt, L., Ed.; International Society for the Advancement of Kinanthropometry: Glasgow, UK, 2011. [Google Scholar]
- Dezenberg, C.; Nagy, T.; Gower, B.; Johnson, R.; Goran, M. Predicting body composition from anthropometry in pre-adolescent children. Int. J. Obes. 1999, 23, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Ortega, R.M.; Requejo, A.M.; López-Sobaler, A.M. Activity Questionnaire. In Nutriguía. Manual of Clinical Nutrition in Primary Care; Ortega, R.M., Requejo, A.M., Eds.; Editorial Médica Panamericana: Madrid, Spain, 2015; Available online: https://www.ucm.es/idinutricion/file/cuestionario-de-actividad-escolares?ver (accessed on 2 January 2023).
- Peral-Suárez, Á.; Cuadrado-Soto, E.; Perea, J.M.; Navia, B.; López-Sobaler, A.M.; Ortega, R.M. Physical Activity Practice and Sports Preferences in a Group of Spanish Schoolchildren Depending on Sex and Parental Care: A Gender Perspective. BMC Pediatr. 2020, 20, 337. [Google Scholar] [CrossRef]
- González-Rodríguez, L.G.; Aparicio, A.; López-Sobaler, A.M.; Ortega, R.M. Omega 3 and Omega 6 Fatty Acids Intake and Dietary Sources in a Representative Sample of Spanish Adults. Int. J. Vitam. Nutr. Res. 2013, 83, 36–47. [Google Scholar] [CrossRef]
- Ortega, R.M.; Requejo, A.M.; Quintas, E.; Sánchez-Quiles, B.; López-Sobaler, A.M.; Andrés, P. Estimated Energy Balance in Female University Students: Differences with Respect to Body Mass Index and Concern about Body Weight. Int. J. Obes. 1996, 20, 1127–1129. [Google Scholar]
- WHO. Energy and Protein Requirements: Report of a Joint FAO/WHO/UNU Expert Consultation; WHO: Geneva, Switzerland, 1985. [Google Scholar]
- IOM. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids (Macronutrients); National Academies Press: Washington, DC, USA, 2005; ISBN 030908525X. [Google Scholar]
- Ortega, R.M.; Requejo, A.M.; Lopez-Sobaler, A.M. Weighed Food and Drinks Record. In Nutriguía. Manual of Clinical Nutrition in Primary Care; Ortega, R.M., Requejo, A.M., Eds.; Editorial Médica Panamericana: Madrid, Spain, 2015; Available online: https://www.ucm.es/data/cont/docs/980-2014-10-17-registro%203%20d%C3%ADas.pdf (accessed on 2 January 2023).
- Ortega, R.M.; López-Sobaler, A.M.; Andrés, P.; Requejo, A.M.; Aparicio, A. DIAL Software for Assessing Diets and Food Calculations (for Windows, Version 3.0.0.5); Department of Nutrition (UCM) & Alceingeniería, S.A.: Madrid, Spain, 2013; Available online: https://www.alceingenieria.net/infodial.htm (accessed on 2 January 2023).
- Ortega, R.M.; López-Sobaler, A.M.; Andrés, P.; Aparicio, A. Food Nutritional Composition. A Tool for the Design and Evaluation of Food and Diets; Department of Nutrition and Food Science, Complutense University of Madrid: Madrid, Spain, 2021; Available online: https://www.ucm.es/idinutricion/file/tca-2021?ver (accessed on 2 January 2023).
- Ortega, R.M.; Perez-Rodrigo, C.; Lopez-Sobaler, A.M. Métodos de Evaluación de La Ingesta Actual: Registro o Diario Dietético. Nutr. Hosp. 2015, 31, 38–45. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.R.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority. Dietary Reference Values for Nutrients Summary Report; EFSA Supporting Publications; European Food Safety Authority: Parma, Italy, 2017; Volume 14, p. e15121E. [Google Scholar] [CrossRef] [Green Version]
- Reese, J.W.; Duncan, P.; Bayse, D. Development and Evaluation of a Hexokinase/Glucose-6-Phosphate Dehydrogenase Procedure for Use as a National Glucose Reference Method; US GPO: Washington, DC, USA, 1977. [Google Scholar]
- el Kenz, H.; Bergmann, P. Evaluation of Immunochemiluminometric Assays for the Measurement of Insulin and C-Peptide Using the ADVIA Centaur®. Clin. Lab. 2004, 50, 171–174. [Google Scholar]
- Tripathy, D.; Carlsson, M.; Almgren, P.; Isomaa, B.; Taskinen, M.R.; Tuomi, T.; Groop, L.C. Insulin Secretion and Insulin Sensitivity in Relation to Glucose Tolerance: Lessons from the Botnia Study. Diabetes 2000, 49, 975–980. [Google Scholar] [CrossRef] [Green Version]
- Albareda, M.; Rodríguez-Espinosa, J.; Murugo, M.; de Leiva, A.; Corcoy, R. Assessment of Insulin Sensitivity and Beta-Cell Function from Measurements in the Fasting State and during an Oral Glucose Tolerance Test. Diabetologia 2000, 43, 1507–1511. [Google Scholar] [CrossRef] [Green Version]
- Keskin, M.; Kurtoglu, S.; Kendirci, M.; Atabek, M.E.; Yazici, C. Homeostasis Model Assessment Is More Reliable than the Fasting Glucose/Insulin Ratio and Quantitative Insulin Sensitivity Check Index for Assessing Insulin Resistance among Obese Children and Adolescents. Pediatrics 2005, 115, e500. [Google Scholar] [CrossRef] [Green Version]
- Manios, Y.; Moschonis, G.; Kourlaba, G.; Bouloubasi, Z.; Grammatikaki, E.; Spyridaki, A.; Hatzis, C.; Kafatos, A.; Fragiadakis, G.A. Prevalence and Independent Predictors of Insulin Resistance in Children from Crete, Greece: The Children Study. Diabet. Med. 2008, 25, 65–72. [Google Scholar] [CrossRef]
- Barbosa-Cortes, L.; Villasis-Keever, M.A.; del Prado-Manriquez, M.; Lopez-Alarcon, M. Adiposity and Insulin Resistance in Children from a Rural Community in Mexico. Arch. Med. Res. 2015, 46, 214–220. [Google Scholar] [CrossRef]
- Das, R.R.; Mangaraj, M.; Nayak, S.; Satapathy, A.K.; Mahapatro, S.; Goyal, J.P. Prevalence of Insulin Resistance in Urban Indian School Children Who Are Overweight/Obese: A Cross-Sectional Study. Front. Med. 2021, 8, 613594. [Google Scholar] [CrossRef]
- Rahimi, H.; Yuzbashian, E.; Zareie, R.; Asghari, G.; Djazayery, A.; Movahedi, A.; Mirmiran, P. Dietary Approaches to Stop Hypertension (DASH) Score and Obesity Phenotypes in Children and Adolescents. Nutr. J. 2020, 19, 112. [Google Scholar] [CrossRef]
- Evia-Viscarra, M.L.; Guardado-Mendoza, R. Comparison between Metabolically Healthy Obesity and Metabolically Unhealthy Obesity by Different Definitions among Mexican Children. J. Pediatr. Endocrinol. Metab. 2020, 33, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast Habits, Nutritional Status, Body Weight, and Academic Performance in Children and Adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [CrossRef]
- Ramsay, S.A.; Bloch, T.D.; Marriage, B.; Shriver, L.H.; Spees, C.K.; Taylor, C.A. Skipping Breakfast Is Associated with Lower Diet Quality in Young US Children. Eur. J. Clin. Nutr. 2018, 72, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Wennberg, M.; Gustafsson, P.E.; Wennberg, P.; Hammarström, A. Poor Breakfast Habits in Adolescence Predict the Metabolic Syndrome in Adulthood. Public Health Nutr. 2015, 18, 122–129. [Google Scholar] [CrossRef] [Green Version]
- Sochol, K.M.; Johns, T.S.; Buttar, R.S.; Randhawa, L.; Sanchez, E.; Gal, M.; Lestrade, K.; Merzkani, M.; Abramowitz, M.K.; Mossavar-Rahmani, Y.; et al. The Effects of Dairy Intake on Insulin Resistance: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Nutrients 2019, 11, 2237. [Google Scholar] [CrossRef] [Green Version]
- Boon, N.; Hul, G.B.J.; Stegen, J.H.C.H.; Sluijsmans, W.E.M.; Valle, C.; Langin, D.; Viguerie, N.; Saris, W.H.M. An Intervention Study of the Effects of Calcium Intake on Faecal Fat Excretion, Energy Metabolism and Adipose Tissue MRNA Expression of Lipid-Metabolism Related Proteins. Int. J. Obes. 2007, 31, 1704–1712. [Google Scholar] [CrossRef] [Green Version]
- Adeva-Andany, M.M.; Martínez-Rodríguez, J.; González-Lucán, M.; Fernández-Fernández, C.; Castro-Quintela, E. Insulin Resistance Is a Cardiovascular Risk Factor in Humans. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 1449–1455. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.P.; Willett, W.C.; Hu, F.B. Sugar-Sweetened Beverages and Risk of Metabolic Syndrome and Type 2 DiabetesA Meta-Analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [Green Version]
- Motallaei, M.; Ramezani-Jolfaie, N.; Mohammadi, M.; Shams-Rad, S.; Jahanlou, A.S.; Salehi-Abargouei, A. Effects of Orange Juice Intake on Cardiovascular Risk Factors: A Systematic Review and Meta-Analysis of Randomized Controlled Clinical Trials. Phytother. Res. 2021, 35, 5427–5439. [Google Scholar] [CrossRef]
- Wang, B.; Liu, K.; Mi, M.; Wang, J. Effect of Fruit Juice on Glucose Control and Insulin Sensitivity in Adults: A Meta-Analysis of 12 Randomized Controlled Trials. PLoS ONE 2014, 9, e95323. [Google Scholar] [CrossRef] [Green Version]
- Alhabeeb, H.; Sohouli, M.H.; Lari, A.; Fatahi, S.; Shidfar, F.; Alomar, O.; Salem, H.; Al-Badawi, I.A.; Abu-Zaid, A. Impact of Orange Juice Consumption on Cardiovascular Disease Risk Factors: A Systematic Review and Meta-Analysis of Randomized-Controlled Trials. Crit. Rev. Food Sci. Nutr. 2022, 62, 3389–3402. [Google Scholar] [CrossRef]
- Shefferly, A.; Scharf, R.J.; Deboer, M.D. Longitudinal Evaluation of 100% Fruit Juice Consumption on BMI Status in 2–5-Year-Old Children. Pediatr. Obes. 2016, 11, 221–227. [Google Scholar] [CrossRef] [Green Version]
- Dubois, L.; Farmer, A.; Girard, M.; Peterson, K. Regular Sugar-Sweetened Beverage Consumption between Meals Increases Risk of Overweight among Preschool-Aged Children. J. Am. Diet. Assoc. 2007, 107, 924–934. [Google Scholar] [CrossRef]
- O’Connor, T.M.; Yang, S.J.; Nicklas, T.A. Beverage Intake among Preschool Children and Its Effect on Weight Status. Pediatrics 2006, 118, e1010–e1018. [Google Scholar] [CrossRef]
- O’neil, C.E.; Nicklas, T.A. A Review of the Relationship Between 100% Fruit Juice Consumption and Weight in Children and Adolescents. Am. J. Lifestyle Med. 2008, 2, 315–354. [Google Scholar] [CrossRef]
- Akhtar-Danesh, N.; Dehghan, M. Association between Fruit Juice Consumption and Self-Reported Body Mass Index among Adult Canadians. J. Hum. Nutr. Diet. 2010, 23, 162–168. [Google Scholar] [CrossRef]
- Beck, A.L.; Tschann, J.; Butte, N.F.; Penilla, C.; Greenspan, L.C. Association of Beverage Consumption with Obesity in Mexican American Children. Public Health Nutr. 2014, 17, 338–344. [Google Scholar] [CrossRef] [Green Version]
- Maki, K.C.; Phillips-Eakley, A.K.; Smith, K.N. The Effects of Breakfast Consumption and Composition on Metabolic Wellness with a Focus on Carbohydrate Metabolism. Adv. Nutr. 2016, 7, 613S. [Google Scholar] [CrossRef]


{kind=link}
| Total (n = 852) | Girls (n = 440) | Boys (n = 412) | |
|---|---|---|---|
| Father’s highest level of education [% (n)] | |||
| No schooling or primary education | 24.6 (210) | 23.2 (102) | 26.2 (108) |
| Secondary Education | 34.6 (295) | 34.8 (153) | 34.5 (142) |
| University studies | 29.7 (253) | 28.0 (123) | 31.6 (130) |
| Not determined | 11.0 (94) | 14.1 (62) | 7.8 (32) * |
| Mother’s highest level of education [% (n)] | |||
| No schooling or primary education | 20.9 (178) | 21.1 (93) | 20.6 (85) |
| Secondary Education | 39.6 (337) | 38.4 (169) | 40.8 (168) |
| University studies | 33.1 (282) | 32.5 (143) | 33.7 (139) |
| Not determined | 6.5 (55) | 8.0 (35) | 4.9 (20) |
| Age and anthropometric data-X ± SD | |||
| Age (years) | 10.1 ± 0.9 | 10.1 ± 0.9 | 10.1 ± 1.0 |
| Weight (kg) | 39.4 ± 9.2 | 39.6 ± 9.2 | 39.1 ± 9.3 |
| Height (m) | 143.4 ± 8.6 | 144.1 ± 9.1 | 142.7 ± 8.0 * |
| Body fat (%) # | 27.6 ± 5.7 | 29.3 ± 4.7 | 25.8 ± 6.1 * |
| BMI (kg/m2) | 19.0 ± 3.1 | 18.9 ± 3.0 | 19.0 ± 3.3 |
| zBMI # | 0.68 ± 1.13 | 0.57 ± 1.04 | 0.80 ± 1.20 * |
| Nutritional status by BMI [% (n)] | |||
| Underweight | 0.8 (7) | 0.7 (3) | 1.0 (4) |
| Normal weight | 59.4 (506) | 63.2 (278) | 55.3 (228) * |
| Overweight | 27.5 (234) | 29.1 (128) | 25.7 (106) |
| Obesity | 12.3 (105) | 7.0 (31) | 18.0 (74) * |
| Physical Activity | |||
| Activity coefficient [X ± SD] | 1.53 ± 0.11 | 1.52 ± 0.11 | 1.53 ± 0.11 |
| MVPA ≥1 h/day [% (n)] | 31.8 (262) | 23.2 (98) | 40.9 (164) * |
| Biochemical data-X ± SD | |||
| Glucose (mg/dL) | 84.4 ± 9.7 | 83.4 ± 10.0 | 85.5 ± 9.2 * |
| Insulin (μU/mL) | 6.3 ± 4.4 | 7.1 ± 4.8 | 5.5 ± 3.6 * |
| HOMA-IR | 1.33 ± 0.97 | 1.48 ± 1.08 | 1.17 ± 0.80 * |
| Insulin resistance [% (n)] | 5.2 (44) | 7.0 (31) | 3.2 (13) * |
| Total (n = 852) | Girls (n = 440) | Boys (n = 412) | |
|---|---|---|---|
| BQI (score) (0–10), X ± SD | 4.50 ± 1.25 | 4.58 ± 1.25 | 4.41 ± 1.25 * |
| Item BQI [% (n)] | |||
| Fruits and/or juice consumption | 29.6 (252) | 33.6 (148) | 25.2 (104) * |
| Dairy products consumption | 97.8 (833) | 98.0 (431) | 97.6 (402) |
| Cereals and derivate consumption | 61.3 (522) | 65.2 (287) | 57.0 (235) * |
| Fruits, cereals, and dairy product in the breakfast | 14.8 (126) | 18.0 (79) | 11.4 (47) * |
| Include olive oil | 16.2 (138) | 16.4 (72) | 16.0 (66) |
| Absence of butter or margarine | 29.3 (250) | 30.5 (134) | 28.2 (116) |
| Calcium (>20% PRI) | 91.3 (778) | 90.7 (399) | 92.0 (379) |
| Simple sugar (<5% kcal/day) | 46.6 (397) | 43.4 (191) | 50.0 (206) |
| MUFA/SFA ratio (≥2:1) | 0.47 (4) | 0.45 (2) | 0.49 (2) |
| Energy intake from breakfast (20–25% kcal/day) | 21.0 (179) | 22.3 (98) | 19.7 (81) |
| Total | Girls | Boys | ||||
|---|---|---|---|---|---|---|
| HOMA-IR ≤3.16 (n = 808) | HOMA-IR >3.16 (n = 44) | HOMA-IR ≤3.16 (n = 409) | HOMA-IR >3.16 (n = 31) | HOMA-IR ≤3.16 (n = 399) | HOMA-IR >3.16 (n = 13) | |
| BQI (score) (0–10), X ± SD | 4.50 ± 1.24 | 4.50 ± 1.34 | 4.56 ± 1.24 | 4.71 ± 1.30 | 4.43 ± 1.24 | 4.00 ± 1.35 * |
| Item BQI [% (n)] | ||||||
| Fruits and/or juice consumption | 28.8 (233) | 43.2 (19) * | 32.3 (132) | 51.61 (16) * | 25.3 (101) | 23.1 (3) |
| Dairy products consumption | 97.7 (789) | 100.0 (44) | 97.8 (400) | 100.0 (31) | 97.5 (389) | 100.0 (13) |
| Cereals and derivate consumption | 61.0 (493) | 65.9 (29) | 65.3 (267) | 64.5 (20) | 56.6 (226) | 69.2 (9) |
| Fruits, cereals, and dairy product in the breakfast | 14.4 (116) | 22.7 (10) | 17.1 (70) | 29.0 (9) | 11.5 (46) | 7.7 (1) |
| Include olive oil | 16.0 (129) | 20.5 (9) | 15.9 (65) | 22.6 (7) | 16.0 (64) | 15.4 (2) |
| Absence of butter or margarine | 28.6 (231) | 43.2 (19) * | 29.6 (121) | 41.9 (13) | 27.6 (110) | 46.2 (6) |
| Calcium (>20% PRI) | 91.7 (741) | 84.1 (37) | 91.4 (374) | 80.7 (25) * | 92.0 (367) | 92.3 (12) |
| Simple sugar (<5% kcal/day) | 47.3 (382) | 34.1 (15) | 44.3 (181) | 32.3 (10) | 50.4 (201) | 38.5 (5) |
| MUFA/SFA ratio (≥2:1) | 0.37 (3) | 2.27 (1) | 0.24 (1) | 3.23 (1) * | 0.50 (2) | 0.00 (0) |
| Energy intake from breakfast (20–25% kcal/day) | 21.0 (170) | 20.5 (9) | 21.8 (89) | 29.0 (9) | 20.3 (81) | 0.0 (0) |
| Total (n = 852) | Girls (n = 440) | Boys (n = 412) | ||||
|---|---|---|---|---|---|---|
| Model 1 OR 95% CI | Model 2 OR 95% CI | Model 1 OR 95% CI | Model 2 OR 95% CI | Model 1 OR 95% CI | Model 2 OR 95% CI | |
| BQI | ||||||
| T1 (BQI < 4 points) | 1 | 1 | 1 | 1 | 1 | 1 |
| T2 (BQI = 4 points) | 0.965 (0.427–2.184) | 0.995 (0.408–2.427) | 1.911 (0.528–6.915) | 1.855 (0.491–7.015) | 0.473 (0.148–1.513) | 0.478 (0.128–1.780) |
| T3 (BQI > 4 points) | 0.856 (0.373–1.964) | 0.843 (0.338–2.098) | 1.994 (0.560–7.100) | 2.094 (0.565–7.761) | 0.172 (0.034–0.872) * | 0.104 (0.014–0.772) * |
| Item BQI | ||||||
| Fruits and/or juice consumption | 1.876 (1.013–3.471) * | 2.203 (1.124–4.314) * | 2.238 (1.074–4.665) * | 3.202 (1.408–7.281) * | 0.885 (0.239–3.280) | 0.926 (0.235–3.652) |
| Dairy products consumption (≥0.5 portion) | 1.305 (0.394–4.321) | 2.249 (0.510–9.917) | 1.611 (0.371–6.999) | 1.788 (0.387–8.264) | 0.981 (0.124–7.775) | 2.163 (0.191–24.499) |
| Cereals and derivate consumption | 1.162 (0.621–2.174) | 1.296 (0.651–2.579) | 0.974 (0.454–2.089) | 1.100 (0.480–2.520) | 1.378 (0.454–4.185) | 1.589 (0.445–5.667) |
| Fruits. cereals. and dairy product in the breakfast | 1.755 (0.844–3.648) | 1.838 (0.820–4.120) | 1.981 (0.875–4.485) | 2.407 (0.971–5.963) | 0.639 (0.081–5.033) | 0.620 (0.073–5.240) |
| Include olive oil | 1.353 (0.635–2.884) | 1.453 (0.653–3.231) | 1.544 (0.639–3.731) | 1.818 (0.710–4.654) | 0.952 (0.206–4.396) | 0.882 (0.177–4.408) |
| Include butter or margarine | 1.898 (1.026–3.514) * | 1.888 (0.976–3.655) | 1.719 (0.817–3.618) | 1.659 (0.742–3.712) | 2.252 (0.740–6.849) | 2.712 (0.823–8.935) |
| Calcium (>20% PRI) | 0.478 (0.205–1.113) | 0.584 (0.238–1.434) | 0.390 (0.150–1.014) | 0.467 (0.168–1.293) | 1.046 (0.132–8.306) | 1.540 (0.179–13.209) |
| Simple sugar (<5% kcal/day) | 0.577 (0.305–1.092) | 0.522 (0.263–1.036) | 0.600 (0.276–1.306) | 0.537 (0.233–1.236) | 0.616 (0.198–1.914) | 0.459 (0.131–1.602) |
| MUFA/SFA ratio (≥2:1) | 6.240 (0.636–61.246) | 11.702 (0.902–151.810) | 13.600 (0.830–222.865) | 16.079 (0.872–296.573) | - | - |
| Energy intake from breakfast (20–25% kcal/day) | 0.940 (0.444–1.989) | 0.769 (0.339–1.746) | 1.475 (0.656–3.318) | 1.368 (0.565–3.314) | - | - |
| Item—Fruits and/or juice consumption divided | ||||||
| Consume whole fruit 1 | 0.831 (0.320–2.155) | 0.836 (0.304–2.296) | 0.862 (0.291–2.551) | 1.153 (0.356–3.731) | 0.609 (0.077–4.792) | 0.393 (0.046–3.322) |
| Consume natural juice 2 | 2.232 (1.168–4.267) * | 2.572 (1.255–5.271) * | 2.713 (1.279–5.754) * | 3.147 (1.370–7.231) * | 0.917 (0.199–4.235) | 1.517 (0.302–7.620) |
| Item—Include butter or margarine divided | ||||||
| Include butter 3 | 2.296 (1.213–4.346) * | 2.387 (1.184–4.812) * | 2.297 (1.058–4.990) * | 2.170 (0.921–5.109) | 2.416 (0.770–7.581) | 2.907 (0.843–10.028) |
| Include Margarine 4 | 0.977 (0.340–2.807) | 1.169 (0.386–3.540) | 0.572 (0.132–2.480) | 0.680 (0.148–3.124) | 2.158 (0.458–10.175) | 2.762 (0.511–14.920) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salas-González, M.D.; Lozano-Estevan, M.d.C.; Aparicio, A.; Bermejo, L.M.; Loria-Kohen, V.; Ortega, R.M.; López-Sobaler, A.M. Breakfast Quality and Insulin Resistance in Spanish Schoolchildren: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 1181. https://doi.org/10.3390/ijerph20021181
Salas-González MD, Lozano-Estevan MdC, Aparicio A, Bermejo LM, Loria-Kohen V, Ortega RM, López-Sobaler AM. Breakfast Quality and Insulin Resistance in Spanish Schoolchildren: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(2):1181. https://doi.org/10.3390/ijerph20021181
Chicago/Turabian StyleSalas-González, María Dolores, María del Carmen Lozano-Estevan, Aránzazu Aparicio, Laura M. Bermejo, Viviana Loria-Kohen, Rosa M. Ortega, and Ana M. López-Sobaler. 2023. "Breakfast Quality and Insulin Resistance in Spanish Schoolchildren: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 2: 1181. https://doi.org/10.3390/ijerph20021181